
Vol. 25 - Num. 98
Originales
Tiroiditis de Hashimoto: manifestaciones clínicas, bioquímicas y su asociación con enfermedades autoinmunes y no autoinmunes
Ana Laura Bahena Garcíaa, Sofía Elizondo Benetb, Héctor Eliud Arriaga Cázaresc, Samantha Garza Fuentesa
aDepartamento de Endocrinología Pediátrica. Unidad Médica de Alta Especialidad #25. Nuevo León. México.
bDepartamento de Pediatría. Unidad Médica de Alta Especialidad #25. Nuevo León. México.
cDepartamento de Investigación. Unidad Médica de Alta Especialidad #21. Nuevo León. México.
Correspondencia: S Elizondo. Correo electrónico: sofia.elizondob@gmail.com
Cómo citar este artículo: Bahena García AL, Elizondo Benet S, Arriaga Cázares HE, Garza Fuentes S. Tiroiditis de Hashimoto: manifestaciones clínicas, bioquímicas y su asociación con enfermedades autoinmunes y no autoinmunes . Rev Pediatr Aten Primaria. 2023;25:137-44.
Publicado en Internet: 12-06-2023 - Número de visitas: 50983
Resumen
Introducción: la tiroiditis de Hashimoto es la causa más frecuente de disfunción tiroidea en niños, con una incidencia del 1 al 2%. Esta enfermedad autoinmune suele estar relacionada con otras patologías. El objetivo es determinar si existen asociaciones en pacientes pediátricos con tiroiditis de Hashimoto tanto clínicas, como bioquímicas, con otras enfermedades para establecer directrices para su detección y tratamiento oportuno.
Material y métodos: estudio observacional descriptivo y transversal en un periodo de 15 años de pacientes con diagnóstico de tiroiditis de Hashimoto menores de 15 años que llevaron seguimiento en la Unidad Médica de Alta Especialidad #25 de Monterrey, Nuevo León, México. Se analizaron variables como antecedentes heredofamiliares de enfermedad tiroidea, autoinmune o neoplásica, sexo, edad, motivo de consulta, función tiroidea en el momento del diagnóstico y la presencia de comorbilidades autoinmunes y no autoinmunes.
Resultados: se analizaron 110 pacientes. El motivo de consulta más frecuente en el momento del diagnóstico fue una detección casual de hormona estimulante de la glándula tiroides (TSH) elevada. El 80% debutó con un hipotiroidismo franco bioquímico. El 26% de los pacientes presentó una segunda enfermedad autoinmune no tiroidea, donde predominó la diabetes mellitus tipo 1 en un 18% y, con menor frecuencia, otras como vitíligo, lupus eritematoso sistémico y enfermedad de Addison. La obesidad fue la comorbilidad no autoinmune más frecuente.
Conclusiones: los pacientes pediátricos con tiroiditis de Hashimoto tienen alto riesgo de presentar una enfermedad autoinmune no tiroidea, principalmente diabetes mellitus tipo 1. Se encontró que los pacientes en edad pediátrica de sexo masculino con tiroiditis de Hashimoto tienen alto riesgo de desarrollar una enfermedad autoinmune no tiroidea.
Palabras clave
● Adolescente ● Hipotiroidismo ● Niño ● Tiroiditis autoinmune ● Tiroiditis de Hashimoto ● Tiroiditis linfocítica crónicaINTRODUCCIÓN
La tiroiditis de Hashimoto, también conocida bajo los nombres de tiroiditis crónica autoinmune (TCA) o tiroiditis linfocítica crónica, es la causa más común de hipotiroidismo adquirido y de bocio en niños y adolescentes. Se presenta en el 1 al 2% de los niños, siendo más frecuente en el sexo femenino y en la etapa puberal1.
El término tiroiditis se define como evidencia de “infiltración linfocítica intratiroidea” con o sin daño folicular. Dos tipos de TCA son causas de hipotiroidismo persistente: la enfermedad de Hashimoto (forma con bocio) y la tiroiditis atrófica (forma sin bocio). Ambas se caracterizan por autoanticuerpos antitiroideos circulantes y diversos grados de disfunción tiroidea, diferenciándose únicamente por la presencia o ausencia de bocio2. La TCA suele sospecharse en presencia de bocio, incluso en ausencia de signos y síntomas de disfunción tiroidea. De entre los sintomáticos, la manifestación clínica más frecuente es el bocio y el retraso del crecimiento3. También se puede diagnosticar incidentalmente durante los chequeos médicos o el seguimiento de niños con enfermedades asociadas autoinmunes: diabetes tipo 14,5, enfermedad celiaca6 y vitíligo7,8. Puede presentarse también en cromosomopatías como: síndromes de Turner, Down y Klinefelter, en enfermedades reumatológicas, como el lupus eritematoso sistémico9,10, y en enfermedades metabólicas11, como diabetes tipo 212, entre otras.
Su causa es multifactorial, interviniendo factores genéticos, ambientales y endógenos para el desarrollo de autoinmunidad. Hasta el 30% de los casos puede tener antecedentes familiares de enfermedad tiroidea autoinmune, por lo que se ha establecido la importancia de la susceptibilidad genética de la enfermedad, sobre todo en la edad pediátrica, pudiendo atribuírsele hasta el 80% de los casos13. Entre los factores ambientales se encuentran la ingesta inadecuada de iodo, la deficiencia de selenio, la exposición al humo de tabaco u otros contaminantes, las enfermedades infecciosas, el estrés, entre otros. Se ha sugerido el nivel de TSH como un marcador de riesgo cardiometabólico14.
Es bien conocida la asociación entre la inflamación crónica y la formación de cáncer. Ante la presencia de nódulos tiroideos, es necesaria su evaluación para descartar malignidades. La tiroiditis linfocítica crónica puede dificultar el adecuado diagnóstico, ya que comparten características citológicas que pueden dar lugar a diagnósticos indeterminados o contradictorios15. Es importante reconocer el cambio general en el espectro de histotipos y las alteraciones moleculares subyacentes comunes en el cáncer de tiroides pediátrico, ya que puede influir directamente en la selección de pruebas diagnósticas y las recomendaciones terapéuticas16.
El objetivo de nuestro estudio es identificar las comorbilidades más frecuentes que se presentan en los pacientes pediátricos con diagnóstico de tiroiditis de Hashimoto y determinar su asociación con otras enfermedades autoinmunes y no autoinmunes para en un futuro establecer pautas para su diagnóstico temprano.
MATERIAL Y MÉTODOS
Estudio observacional descriptivo y transversal de pacientes con diagnóstico de tiroiditis de Hashimoto menores de 15 años que llevaron seguimiento en la Unidad Médica de Alta Especialidad #25 de Monterrey, Nuevo León, México, durante el periodo 2006-2021. Este estudio fue aprobado por el Comité Local de Investigación en Salud.
Se obtuvo la muestra con casos consecutivos, incluyendo a todos los sujetos disponibles. Se extrajo la información de expedientes de pacientes menores de 15 años con diagnóstico de tiroiditis de Hashimoto que contaban con expediente clínico completo y determinación de anticuerpos antiperoxidasa tiroideos positivos. Se excluyeron pacientes con pérdida de seguimiento o que tuvieran el diagnóstico de alguna cromosomopatía. Se analizaron diferentes variables como el sexo, la edad, el motivo de consulta y la función tiroidea en el momento del diagnóstico, la presencia de comorbilidades y los antecedentes heredofamiliares de enfermedad tiroidea, autoinmune o neoplásica y de otras enfermedades autoinmunes.
Se utilizaron medidas de tendencia central como medianas para variables cualitativas y medias para las cuantitativas. Para el análisis inferencial en variables categóricas se utilizó la prueba de Chi cuadrado y la prueba exacta de Fisher, considerando significancia estadística con una p ≤0,05. Posteriormente, se obtuvo la razón de momios (RM, [odds ratio]).
RESULTADOS
Se analizaron 123 expedientes clínicos, de los cuales 110 cumplieron con los criterios de inclusión (Tabla 1). De ellos, 84 (77%) pacientes fueron de sexo femenino. La mediana de edad al momento del diagnóstico fue de 10 años. Y 60 (55%) tuvieron un rango de edad entre 4 a 10 años. El motivo de consulta más frecuente fue una detección casual de TSH elevada, seguido por manifestaciones de enfermedad tiroidea, como aumento de peso, retraso en el crecimiento o pubertad, fatiga y/o estreñimiento en el 31% de los pacientes.
| Tabla 1. Descripción general de 110 pacientes diagnosticados con tiroiditis de Hashimoto en el periodo de 15 años | |
|---|---|
| Variable | Frecuencia, n (%) |
|
Edad media Mediana de edad |
9,9 años 10 años |
|
Sexo Femenino Masculino |
85 (77) 25 (23) |
|
Motivo de consulta Detección casual de TSH elevada Bocio Talla baja Otras manifestaciones de enfermedad tiroidea |
41 (37) 26 (24) 9 (8) 34 (31) |
|
Estado del perfil tiroideo al diagnóstico Eutiroidismo Hipotiroidismo subclínico Hipotiroidismo franco Hipertiroidismo |
15 (14) 19 (17) 75 (68) 1 (1) |
|
Comorbilidades autoinmunes Ninguna DM tipo 1 LES Vitíligo Enfermedad de Addison |
82 (74) 20 (18) 1 (1) 6 (5) 2 (2) |
|
Comorbilidades no autoinmunes Ninguna Obesidad Cáncer tiroideo Síndrome metabólico |
79 (72) 17 (15) 9 (8) 5 (5) |
|
Antecedentes heredofamiliares Ninguno Patología tiroidea autoinmune Otras enfermedades tiroideas Cáncer tiroideo Otra enfermedad autoinmune |
86 (78) 4 (4) 15 (13) 3 (3) 2 (2) |
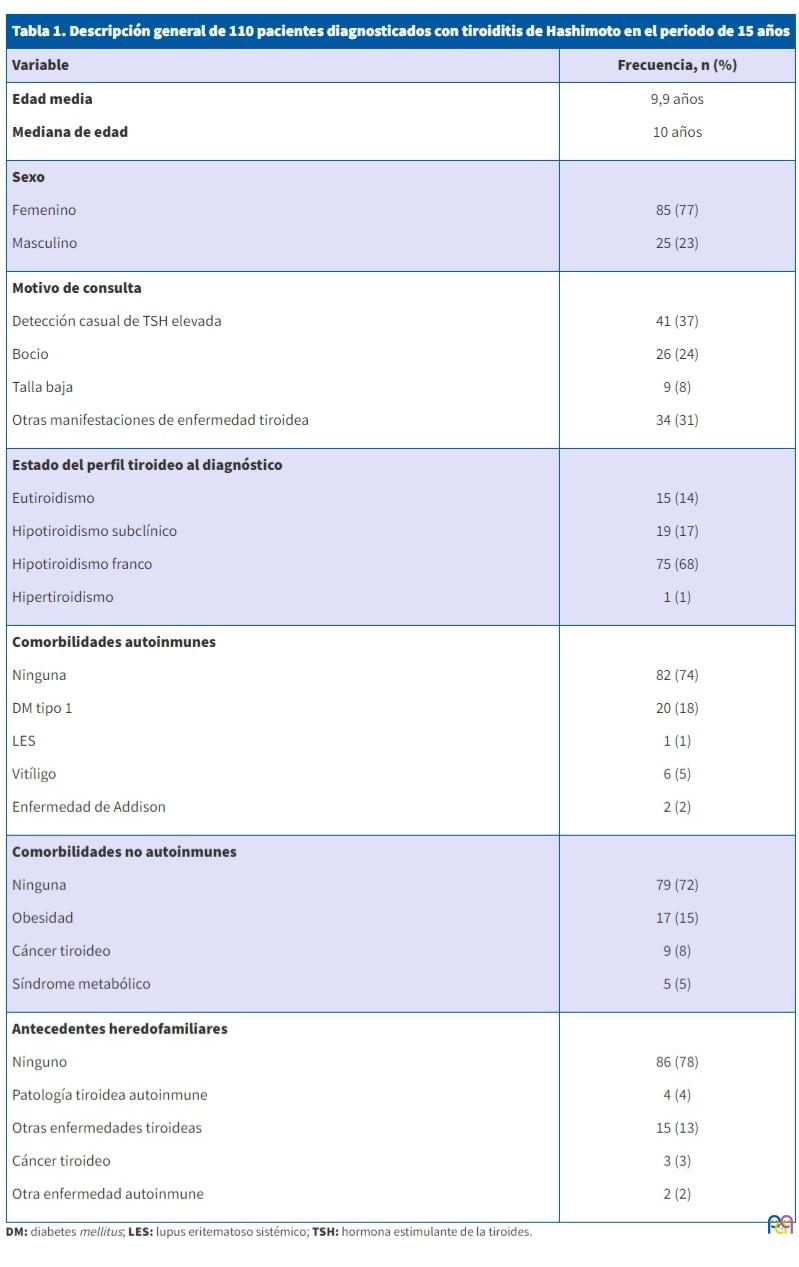
El estado bioquímico del perfil tiroideo inicial en su mayoría se presentó con un hipotiroidismo franco, encontrándose en 75 (68%) de ellos, seguido de hipotiroidismo subclínico en el 17%. Únicamente se presentó hipertiroidismo bioquímico en un paciente. En la mayoría de los pacientes no había antecedentes heredofamiliares conocidos relevantes. El 13% contaba con antecedente en familiares directos de enfermedad tiroidea no autoinmune; el 4%, de patología tiroidea de etiología autoinmune; y el 2%, de enfermedades autoinmunes no tiroideas. En el 3% se reportó antecedente de cáncer tiroideo.
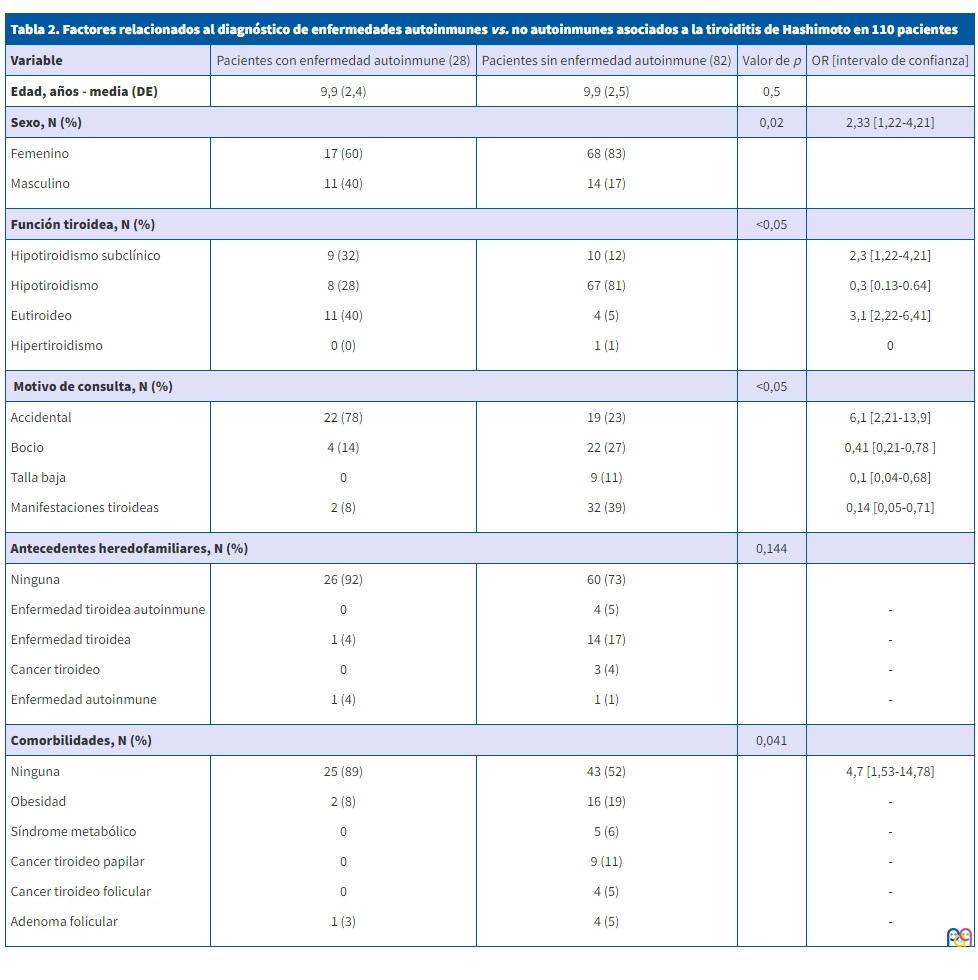
En cuanto a las comorbilidades autoinmunes en los pacientes con tiroiditis de Hashimoto estudiados, encontramos que 28 (26%) presentaban otra patología autoinmune. La más prevalente fue diabetes mellitus tipo 1 en 20 (18%) sujetos. En referencia a las comorbilidades no autoinmunes, la obesidad fue la más frecuente en el 15%, mientras que el 8% presentó cáncer tiroideo. Los pacientes fueron divididos en dos grupos: los que presentaron alguna comorbilidad autoinmune y los que no; se exponen los resultados en la Tabla 2. De los pacientes analizados, no se encontró diferencia significativa en cuanto a la edad entre quienes presentaron o no presentaron comorbilidades autoinmunes, con una edad media de 9,9. En cuanto al sexo, de los 85 pacientes de sexo femenino, el 20% presentaba una segunda enfermedad autoinmune, mientras que de los 25 de sexo masculino, el 44% presentó alguna comorbilidad autoinmune (p = 0,02). En el 81% de los pacientes del grupo que no presentó comorbilidad autoinmune, se reportó hipotiroidismo franco en el perfil tiroideo al diagnóstico (p <0,05). Mientras que en el 40% del grupo de quienes la presentaron se reportó eutiroideo (p <0,001).
| Tabla 2. Factores relacionados con el diagnóstico de enfermedades autoinmunes vs. no autoinmunes asociados a la tiroiditis de Hashimoto en 110 pacientes | ||||
|---|---|---|---|---|
| Variable | Pacientes con enfermedad autoinmune (28) | Pacientes sin enfermedad autoinmune (82) | Valor de p | OR [intervalo de confianza] |
| Edad, años - media (DE) | 9,9 (2,4) | 9,9 (2,5) | 0,5 | |
| Sexo, N (%) | 0,02 | 2,33 [1,22-4,21] | ||
|
Femenino Masculino |
17 (60) 11 (40) |
68 (83) 14 (17) |
||
| Función tiroidea, N (%) | <0,05 | |||
|
Hipotiroidismo subclínico Hipotiroidismo Eutiroideo Hipertiroidismo |
9 (32) 8 (28) 11 (40) 0 (0) |
10 (12) 67 (81) 4 (5) 1 (1) |
2,3 [1,22-4,21] 0,3 [0.13-0.64] 3,1 [2,22-6,41] 0 |
|
| Motivo de consulta, N (%) | <0,05 | |||
|
Accidental Bocio Talla baja Manifestaciones tiroideas |
22 (78) 4 (14) 0 2 (8) |
19 (23) 22 (27) 9 (11) 32 (39) |
6,1 [2,21-13,9] 0,41 [0,21-0,78 ] 0,1 [0,04-0,68] 0,14 [0,05-0,71] |
|
| Antecedentes heredofamiliares, N (%) | 0,144 | |||
|
Ninguna Enfermedad tiroidea autoinmune Enfermedad tiroidea Cancer tiroideo Enfermedad autoinmune |
26 (92) 0 1 (4) 0 1 (4) |
60 (73) 4 (5) 14 (17) 3 (4) 1 (1) |
- - - - |
|
| Comorbilidades, N (%) | 0,041 | |||
|
Ninguna Obesidad Síndrome metabólico Cancer tiroideo papilar Cancer tiroideo folicular Adenoma folicular |
25 (89) 2 (8) 0 0 0 1 (3) |
43 (52) 16 (19) 5 (6) 9 (11) 4 (5) 4 (5) |
4,7 [1,53-14,78] - - - - - |
|
DISCUSIÓN
Casi la mitad de las personas con tiroiditis de Hashimoto tiene antecedentes familiares de enfermedad tiroidea autoinmune, pero en nuestro trabajo esta relación se presentó solo en el 4% de los pacientes estudiados. Se encontró, en estudios realizados en Dinamarca, una concordancia del 55% en gemelos monocigóticos, en contraste con un 3% de gemelos dicigóticos17. Además, ha sido asociado con ciertas cromosomopatías, como el síndrome de Down y el síndrome de Turner. Por otro lado, también se consideran causantes de la enfermedad algunos factores ambientales, como la ingesta excesiva de iodo, infecciones virales, estrés, radiación previa y ciertos fármacos como la amiodarona, el litio y algunos antiepilépticos18.
Esta enfermedad es más común en el sexo femenino, con una relación sexo femenino-masculino aproximada de 2 a 10:1 y suele aparecer durante la pubertad. Sin embargo, aunque su incidencia es menor en la edad pediátrica, se considera la causa adquirida más común de hipotiroidismo en niños y adolescentes, con una prevalencia del 1-2%19. La prevalencia de tiroiditis de Hashimoto se encuentra incrementada en pacientes con diabetes mellitus tipo 1, el 20% de los cuales tiene anticuerpos antitiroideos positivos y el 5%, TSH elevada. Además, puede estar presente como parte de los síndromes autoinmunes poliglandulares: en el 10% de los pacientes del tipo 1, asociada a candidiasis mucocutánea, hipoparatiroidismo e insuficiencia suprarrenal como resultado de una mutación en el gen AIRE (regulador autoinmune), o en el tipo 2 (síndrome de Schmidt), donde suele presentarse en la adolescencia asociado a diabetes mellitus con o sin insuficiencia suprarrenal20.
Los síntomas más comunes del hipotiroidismo son: fatiga, intolerancia al frío, estreñimiento e irregularidades menstruales. Los niños pueden presentar retraso puberal o, en casos de hipotiroidismo grave de larga evolución, desarrollar pubertad precoz. Otros hallazgos son: bradicardia, reflejos retardados y mixedema de cara y extremidades. El hipotiroidismo causa un crecimiento lineal deficiente y, si no se diagnostica, puede comprometer la estatura adulta21. Sin embargo, el hipotiroidismo rara vez es la etiología del aumento de peso. De hecho, el aumento de peso excesivo se asocia con leve incremento de la tirotropina (entre 5 y 10 mUI/l), con normalización del nivel de la misma tras lograr la pérdida de peso22.
Los hallazgos de laboratorio incluyen niveles elevados de hormona estimulante del tiroides (TSH), niveles bajos de tiroxina libre (T4) y/o la presencia de autoanticuerpos contra la peroxidasa tiroidea (anti-TPO) o la tiroglobulina (anti-TG). Aunque una TSH elevada se considera diagnóstica de tiroiditis de Hashimoto, es importante señalar que este marcador puede elevarse secundariamente a otras condiciones, incluyendo obesidad, infección y exceso de ingesta de yodo. Además, ha habido informes de pacientes con enfermedad clínicamente evidente, pero serología negativa23. Por otro lado, entre el 10 y el 15% de la población general es positiva para anticuerpos anti-TPO sin síntomas clínicos. Debido a esta ambigüedad, a menudo se recurre a una evaluación adicional de la tiroides mediante ecografía en escala de grises. Históricamente, la ecografía ha revelado áreas de ecogenicidad hipoecoica y heterogénea. Sin embargo, este aspecto 'apolillado' solo está presente en aproximadamente un tercio de los niños24.
En nuestro estudio, comparado con lo establecido en la literatura, también fue predominante el sexo femenino, con una relación femenino-masculino 3,3:1. La edad media al diagnóstico fue de 9,9 años, una edad menor a la reportada en otros estudios. En un estudio realizado en Argentina, se encontró una relación 2:1 con edad promedio de 11 años, mientras que en Turquía la relación fue de 6:1, con edades más frecuentes al diagnóstico entre los 12-14 años25. El 37% de los pacientes fue diagnosticado incidentalmente por medio de medición de TSH elevada26, mientras que solo el 24% fue por la presencia de bocio, similar a lo reportado en otros estudios27,28.
En cuanto al perfil tiroideo inicial de nuestros pacientes, se reportó un hipotiroidismo franco en el 68% de los pacientes, porcentaje elevado al compararlo con otro estudio realizado en Argentina, donde se detectó hipotiroidismo subclínico en el 55% e hipotiroidismo franco en el 10,5%3. Esto pudiera estar relacionado con un diagnóstico más tardío en nuestro país, asociado a la falta de accesos a los servicios de salud de un gran porcentaje de la población. En México, alrededor de 33 millones de habitantes no se encuentran afiliados a algún sistema de salud29. Esto también pudiera estar relacionado con el bajo porcentaje de antecedentes heredofamiliares conocidos, en contraste con otros estudios3,20. Solamente se encontró hipertiroidismo en uno de los pacientes, en comparación con un estudio realizado en Costa Rica, donde el 42%, casi la mitad de sus pacientes pediátricos con tiroiditis de Hashimoto, tienen hipertiroidismo30. Encontramos que el perfil bioquímico más habitual en quienes se diagnosticó una enfermedad autoinmune no tiroidea fue de eutiroidismo: en el 40%, p <0,001, mientras que en quienes no la presentaron, se encontró un hipotiroidismo franco en el 80%. En un estudio que se llevó a cabo en Italia con más de 500 pacientes, el 69% de los pacientes que presentó como comorbilidad una enfermedad autoinmune no tiroidea se encontraba eutiroideo31.
En relación con las comorbilidades que presentaron los pacientes con tiroiditis linfocítica crónica, la diabetes mellitus tipo 1 fue la más frecuente, presente en el 18% de los pacientes, seguido por obesidad en el 15%, cáncer tiroideo en el 8% y vitíligo en el 5%. Aproximadamente el 45% del total de los pacientes no presentó ninguna comorbilidad, ya sea autoinmune o no autoinmune.
En nuestro estudio, casi la mitad de los pacientes de sexo masculino presentó una segunda enfermedad autoinmune, mientras que en el sexo femenino se reportó en un quinto de ellos, resultando estadísticamente significativo con una p = 0,02. Esto podría estar en relación con que en el grupo de escolares y adolescentes con enfermedades autoinmunes suele ser mayor la prevalencia del sexo masculino, al contrario de lo que sucede en la edad adulta31.
CONCLUSIONES
Los pacientes pediátricos con tiroiditis de Hashimoto tienen alto riesgo de presentar una enfermedad autoinmune no tiroidea, principalmente diabetes mellitus tipo 1. Es importante que el médico conozca estas enfermedades y las detecte en forma oportuna, ya que el tratamiento precoz de ambas enfermedades conducirá a un mejor control de la enfermedad y a una mejora de la salud. El perfil eutiroideo en el momento del diagnóstico de tiroiditis de Hashimoto fue el más frecuentemente encontrado en quienes presentaron una enfermedad autoinmune no tiroidea. Se encontró que en la edad pediátrica el sexo masculino tiene alto riesgo de desarrollar como comorbilidad una enfermedad autoinmune no tiroidea.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo. Este trabajo no ha recibido financiación.
RESPONSABILIDAD DE LOS AUTORES
Contribución de los autores: concepción y diseño del estudio (ALBG, HEAC), recogida de datos (ALBG), análisis e interpretación de resultados (ALBG, HEAC), preparación del borrador del manuscrito (ALBG, SEB, HEAC, SGF). Todos los autores revisaron los resultados y aprobaron la versión final del manuscrito.
ABREVIATURA
TCA: tiroiditis crónica autoinmune · TG: tiroglobulina · TPO: peroxidasa tiroidea · TSH: hormona estimulante de la glándula tiroides · T4: tiroxina libre.
BIBLIOGRAFÍA
- Hanley P, Lord K, Bauer AJ. Thyroid disorders in children and adolescents. JAMA Pediatr. 2016;170(10):1008-19.
- Cappa M, Bizzarri C, Crea F. Autoimmune thyroid diseases in children. J Thyroid Res. 2010;2011:675-703.
- Gómez E, Nso Roca AP, Juste M, Cortés E. Enfermedad de Hashimoto en una cohorte de 29 niños y adolescentes. Epidemiología, evolución y comorbilidad a corto y largo plazo. Arch Argent Pediatr. 2018;116(1):56-8.
- Korzeniowska K, Ramotowska A, Szypowska A, Szadkowska A, Fendler W, Kalina Faska B, et al. How does autoimmune thyroiditis in children with type 1 diabetes mellitus influence glycemic control, lipid profile and thyroid volume? J Pediatr Endocrinol Metab. 2015;28(3-4):275-8.
- Bárová H, Perusicová J, Hill M, Sterzl I, Vondra K, Masek Z. Anti-GAD-positive patients with type 1 diabetes mellitus have higher prevalence of autoimmune thyroiditis than anti-GAD-negative patients with type 1 and type 2 diabetes mellitus. Physiol Res. 2004;53(3):279-86.
- Husby S, Koletzko S, Korponay Szabó IR, Mearin ML. Phillips A, Shamir R. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. 2012;54(1):136-60.
- Fallahi P, Elia G, Ragusa F, Ruffilli I, Camastra S, Giusti C, et al. The aggregation between AITD with rheumatologic, or dermatologic, autoimmune diseases. Best Pract Res Clin Endocrinol Metab. 2019;33(6):101372.
- Liu M, Murphy E, Amerson EH. Rethinking screening for thyroid autoimmunity in vitiligo. J Am Acad Dermatol. 2016;75(6):1278-80.
- Merino Muñoz R, Remesal Camba A, Murias Loza S. Lupus eritematoso sistémico. An Pediatr Contin. 2013;11(2):89-97.
- Klionsky J, Antonelli M. Thyroid disease in lupus: an updated review. ACR Open Rheumatol. 2020;2(2):74-8.
- Brenta G, Fretes O. Dyslipidemias and hypothyroidism. Pediatr Endocrinol Rev. 2014;11(4):390-9.
- Nishi M. Diabetes mellitus and thyroid diseases. Diabetol Int. 2018;9(2):108-12.
- Saranac l, Zivanovic S, Bjelakovic B, Stamenkovic H, Novak M, Kamenov B. Why is the thyroid so prone to autoimmune disease? Horm Res Paediatr. 2011;75(3):157-65.
- Chang YC, Hua SC, Chang CH, Kao WY, Lee HL, Chuang LM, et al. High TSH level within Normal Range Is Associated with Obesity, Dyslipidemia, Hypertension, Inflammation, hypercoagulability, and the metabolic syndrome: a novel cardiometabolic marker. J Clin Med. 2019;8(6):817.
- Silva de Morais N, Stuart J, Guan H, Wang Z, Cibas ES, Frates MC, et al. The mpact of Hashimoto Thyroiditis on thyroid nodule cytology and risk of thyroid cancer. J Endocr Soc. 2019;3(4):791-800.
- Paulson V, Rudzinski ER, Hawkins DS. Thyroid cancer in the pediatric population. Genes (Basel). 2018;10(9):723.
- Brix TH, Hegedüs l, Gardas A, Banga JP, Nielsen CH. Monozygotic twin pairs discordant for Hashimoto's thyroiditis share a high proportion of thyroid peroxidase autoantibodies to the immunodominant region A. Further evidence for genetic transmission of epitopic 'fingerprints'. Autoimmunity. 2011;44(3):188-94.
- Duntas LH. Environmental factors and autoimmune thyroiditis. Nat Clin Pract Endocrinol Metab. 2008;4:454-60.
- Casto C, Pepe G, Li Pomi A, Corica D, Aversa T, Wasniewska M. Hashimoto's thyroiditis and Graves' disease in genetic syndromes in pediatric age. Genes (Basel). 2021;12(2):222.
- Núñez Almache O, Del Aguila Villar C, Chávez E, Espinoza O, Pinto P, Calagua M, et al. Progresión clínica de la tiroiditis autoinmune en niños y adolescentes atendidos en el Instituto Nacional de Salud del Niño. An Fac Med. 2015;76(4):325-31.
- Hanley P, Lord K, Bauer AJ. Thyroid disorders in children and adolescents: a review. JAMA Pediatr. 2016;170(10):1008-19.
- Pacifico l, Anania C, Ferraro F, Andreoli GM, Chiesa C. Thyroid function in childhood obesity and metabolic comorbidity. Clin Chim Acta. 2012;413(3- 4):396-405.
- Mincer DL, Jialal I: Hashimoto thyroiditis. In: StatPearls. Treasure Island, FL; 2023 [en línea] [consultado el 11/04/2023]. Disponible en www.ncbi.nlm.nih.gov/books/NBK459262/
- Decker T, Schnittka E, Stolzenberg l, Yalowitz J. Shear-Wave Elastography for the Diagnosis of Pediatric Hashimoto's Thyroiditis: A systematic review and meta-analysis. Cureus. 2023;15(2):e35490.
- Dündar B, Boyaci A, Sangün O, Dündar N. Hashimoto thyroiditis in children and adolescents: evaluation of clinical and laboratory findings. Turk Arch Ped. 2011;46:309-13.
- Crisafulli G, Gallizzi R, Aversa T, Salzano G, Valenzise M, Wasniewska M, et al. Thyroid function test evolution in children with Hashimoto's thyroiditis is closely conditioned by the biochemical picture at diagnosis. Ital J Pediatr. 2018;44(1):22.
- De Luca F, Santucci S, Corica D, Pitrolo E, Romeo M, Aversa T. Hashimoto's thyroiditis in childhood: presentation modes and evolution over time. Ital J Pediatr. 2013;39:8.
- Tang S, Yang M, Zhang D, Tong YJ, Xin Y. Clinical characteristics and follow-up of 19 children with Hashimoto's thyroiditis aged below 3 years: a single-center retrospective analysis. Front Endocrinol (Lausanne). 2021;12:737527.
- INEGI. Censo de Población y Vivienda. 2020 [en línea] [consultado el 11/04/2023]. Disponible en www.inegi.org.mx/contenidos/programas/ccpv/2020/doc/Censo2020_Principales_resultados_EUM.pdf
- Acevedo G, Mejía J, Gil M, Astudillo E, Gómez J, Valencia A, et al. Características clínicas y paraclínicas de pacientes pediátricos con tiroiditis autoinmune en una institución especializada de Cali, Colombia. Rev Méd Univ Costa Rica. 2020;14(2):13-22.
- Ruggeri RM, Trimarchi F, Giuffrida G, Certo R, Cama E, Campennì A, et al. Autoimmune comorbidities in Hashimoto’s thyroiditis: different patterns of association in adulthood and childhood/adolescence. Eur J Endocrinol. 2017;176(2):133-41.