
Vol. 24 - Num. 95
Notas clínicas
Eructo, un síntoma que debemos tomar en serio
Miguel Ángel Carro Rodrígueza, Yoko Oyakawa Barcellib, Lucía Marcela Figueroa Ospinab, Miriam Melissa Mendoza Chávezb, Roi Piñeiro Pérezb
aUnidad de Gastroenterología Pediátrica. Servicio de Pediatría. Hospital General de Villalba. Collado Villalba. Madrid. España.
bServicio de Pediatría. Hospital General de Villalba. Madrid. España.
Correspondencia: MA Carro. Correo electrónico: miguel.carro@hgvillalba.es
Cómo citar este artículo: Carro Rodríguez MA, Oyakawa Barcelli Y, Figueroa Ospina LM, Mendoza Chávez MM, Piñeiro Pérez R. Eructo, un síntoma que debemos tomar en serio . Rev Pediatr Aten Primaria. 2022;24:e319-e322.
Publicado en Internet: 11-10-2022 - Número de visitas: 185567
Resumen
El eructo es un síntoma frecuente en Pediatría que socialmente está mal considerado y puede tener consecuencias negativas en la calidad de vida del paciente. No obstante, no son muchas las publicaciones pediátricas al respecto. Según su origen, se pueden clasificar como eructos supragástricos o gástricos, con una fisiología distinta y que pueden ser síntomas de patologías subyacentes tanto físicas como psicológicas. Se revisa la fisiología del eructo y el diagnóstico diferencial a propósito de dos casos diagnosticados de eructos supragástricos.
Caso clínico 1: varón de 14 años con cuadro de 15 días de eructos hasta 20-30 por minuto, sensación de imputación esofágica y dolor abdominal. El dolor mejora con omeprazol, pero los eructos persisten; se realiza endoscopia y tránsito esofágico superior que resultan normales. Mejora tras logopedia e inicio de técnicas de relajación.
Caso clínico 2: varón de 10 años con cuadro de 19 días de eructos de más de 15 por minuto, sin otros síntomas digestivos, pero con sintomatología ansiosa. Mejoría tras tratamiento psicológico.
Ambos tipos de eructo presentan una fisiología distinta, de manera que en el eructo supragástrico el aire no proviene del estómago. El esfínter esofágico inferior permanece cerrado. Los dos tipos son distinguibles mediante pH-impedanciometría. Conclusión: una cuidadosa anamnesis puede establecer el diagnóstico de sospecha del origen del eructo antes de recurrir a pruebas complementarias y permite orientar el tratamiento más adecuado para cada paciente.
Palabras clave
● Aerofagia ● Enfermedades del esófago ● Eructo ● Reflujo gastroesofágicoINTRODUCCIÓN
El eructo es un síntoma frecuente en Pediatría que socialmente está mal considerado y puede tener consecuencias negativas en la calidad de vida del paciente. No obstante, no son muchas las publicaciones pediátricas al respecto. Según su origen, se pueden clasificar como eructos supragástricos o gástricos. La realización de un diagnóstico adecuado es importante para excluir posibles causas secundarias tratables. Se revisa la fisiología del eructo y el diagnóstico diferencial a propósito de dos casos.
CASO CLÍNICO 1
Varón de 14 años, remitido a urgencias por cuadro de 15 días de evolución de eructos y dolor abdominal. Además, refiere sensación de impactación diaria en tercio medio esofágico que mejora al beber agua, con algún vómito ocasional y sin presentar pérdida de peso ni apetito. El dolor mejoró tras inicio de omeprazol, almagato y domperidona, persistiendo los eructos, que se producen durante todo el día, de forma continua, aunque mejoran durante el sueño.
No presenta asma ni dermatitis atópica, no tiene otros antecedentes personales de interés. La exploración física completa por aparatos es normal, pero presenta eructos continuos a un ritmo de unos 20-30 por minuto. Se realiza hemograma y perfil hepatorrenal en urgencias sin hallazgos. Se solicita tránsito esofágico superior ambulatorio que resulta normal, sin presentar alteraciones anatómicas ni signos de reflujo gastroesofágico. Es reevaluado a los 20 días de evolución en consultas de Gastroenterología pediátrica, con diagnóstico inicial de eructos supragástricos. Se pauta metoclopramida, pero dada la sensación de impactación que comenta el paciente se solicita endoscopia digestiva superior. El esófago, estómago y duodeno observados son normales endoscópica e histológicamente. Es valorado por Psicología y Rehabilitación, iniciando técnicas de relajación y rehabilitación logofonatoria, de manera que el cuadro se resuelve a los dos meses del inicio sin recaídas en los cuatro años siguientes.
CASO CLÍNICO 2
Varón de 10 años remitido a consulta de Gastroenterología por cuadro de 19 días caracterizado por episodios de eructos con un ritmo de más de 15 veces por minuto, coincidiendo con más nerviosismo, ocurriéndole a diario, más por la noche antes acostarse. Refiere que tiene un inicio voluntario, pero que una vez que comienza no puede frenarlo. No presenta dolor abdominal, pirosis, impactación ni atragantamiento, se acompaña de escaso apetito y saciedad precoz sin pérdida de peso. Hábito intestinal caracterizado por una deposición cada 24-48 horas sin dolor con la defecación. No presenta distensión abdominal acompañante.
Refiere mal rendimiento escolar, motivo por el cual comienza apoyo extraescolar y castigos sin videoconsola, mostrando datos de ansiedad e irritabilidad. Vive en el seno de una familia monoparental con escaso contacto con el padre. El paciente es derivado a Psicología, con mejoría a los cinco meses de terapia sin recaídas en los seis meses posteriores.
DISCUSIÓN
El eructo gástrico es un mecanismo de defensa frente a una dilatación gástrica excesiva por el gas ingerido. Ante una dilatación del estómago proximal, se produce un estímulo de los receptores de la pared gástrica que desencadenan un reflejo vagal, a través del cual se produce una relajación del esfínter esofágico inferior y de la crura diafragmática y, finalmente, la salida del aire en dirección proximal. Sin embargo, los eructos supragástricos se producen bien por una inyección de aire de origen proximal al esófago o bien por una succión mediante contracción diafragmática, causando una dilatación del esófago, con relajación de esfínter esofágico superior y expulsión del aire hacia la boca1. En ambos casos el esfínter esofágico inferior permanece cerrado y el aire no entra al estómago. Una vez conocida la fisiopatología y el recorrido aéreo en cada uno de los tipos de eructo, es comprensible que el ritmo de los eructos supragástricos pueda ser tan alto como en los casos presentados.
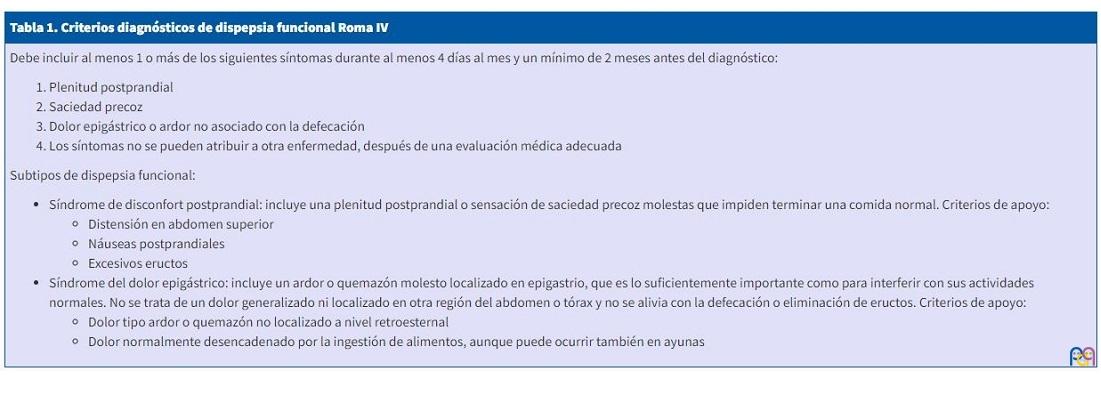
De forma fisiológica, se producen unos 30 eructos gástricos cada día2. Sin embargo, pueden aparecer como síntomas de múltiples patologías digestivas, como la enfermedad por reflujo gastroesofágico (ERGE), donde no necesariamente se producen de forma simultánea con los episodios de reflujo. Se ha observado que adultos con ERGE tienen una burbuja gástrica mayor y mayor ingesta de aire, posiblemente relacionada con las molestias digestivas, dado que la ingesta de aire en estos pacientes disminuye con inhibidores de la bomba de protones3. También es frecuente la presencia excesiva de eructos gástricos en pacientes con dispepsia funcional, considerándose en los criterios Roma IV como un criterio de apoyo para el diagnóstico de dispepsia funcional tipo disconfort posprandial4 (Tabla 1). El tratamiento de los eructos gástricos será, por tanto, de la patología subyacente.
| Tabla 1. Criterios diagnósticos de dispepsia funcional Roma IV |
|---|
|
Debe incluir al menos 1 o más de los siguientes síntomas durante al menos 4 días al mes y un mínimo de 2 meses antes del diagnóstico:
Subtipos de dispepsia funcional:
|
Los eructos supragástricos no se producen de forma fisiológica. Se trata de un fenómeno conductual que puede ser controlado de forma voluntaria y, por lo general, disminuyen cuando se distrae al paciente y durante el sueño, y no se incrementan tras las comidas2. Sin embargo, en ocasiones se han visto asociados a procesos patológicos, como la ERGE, de manera que en pacientes con sintomatología refractaria a inhibidores de la bomba de protones podrían jugar un papel clínico relevante5. Se postula que también pueden aparecer como un intento de alivio de otras molestias digestivas, como en el caso de eructos persistentes en pacientes sometidos a una funduplicatura de Nissen que, aunque tienen reducida la capacidad de expulsar eructos gástricos, presentan un aumento posoperatorio de los eructos supragástricos3, si bien esto no está claro en niños6. El tratamiento médico generalmente no se recomienda en los eructos supragástricos; la terapia rehabilitadora logopédica sí se recomienda en estos pacientes, así como la valoración psicológica1.
Mención aparte merece el término aerofagia. Se trata de un trastorno gastrointestinal funcional con criterios diagnósticos propios (Tabla 2), por lo que hay que evitar utilizar este término si no cumple todos4. En la aerofagia hay una ocupación intestinal de aire deglutido; por tanto, también puede llenarse la cámara gástrica y provocar eructos gástricos, aunque pueden coexistir con eructos supragástricos. En el tratamiento se puede valorar la logopedia con el objetivo de disminuir la ingesta de aire y fármacos como la simeticona.
| Tabla 2. Criterios diagnósticos de aerofagia Roma IV |
|---|
|
Debe cumplir todos los criterios siguientes, como mínimo 2 meses antes del diagnóstico:
|

La pH-impedanciometría puede ser una herramienta útil para el diagnóstico diferencial entre eructos gástricos y supragástricos, de manera que en los primeros se observa el flujo retrógrado de aire desde estómago hacia esófago, mientras que en los segundos se observa el flujo anterógrado con un retorno rápido sin llegar a estómago7. Además, nos permite cuantificar el aire deglutido. Sin embargo, se trata de una prueba invasiva y no siempre accesible.
Conclusiones: es necesario conocer la fisiología del eructo para intentar establecer el origen gástrico o supragástrico. Una cuidadosa anamnesis puede establecer el diagnóstico de sospecha de dicho origen antes de recurrir a pruebas complementarias y permite orientar el tratamiento más adecuado a cada paciente.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
ERGE: enfermedad por reflujo gastroesofágico.
BIBLIOGRAFÍA
- Kessing BF, Bredenoord AJ, Smout AJ. The pathophysiology, diagnosis and treatment of excessive belching symptoms. Am J Gastroenterol. 2014;109:1196-203.
- Bredenoord AJ, Smout AJ. Physiologic and pathologic belching. Clin Gastroenterol Hepatol. 2007;5:772-5.
- Hemmink G J, Weusten B l, Bredenoord A J, Timmer R, Smout A J. Increased swallowing frequency in GORD is likely to be caused by perception of reflux episodes. Neurogastroenterol Motil. 2009;21:143-8.
- Drossman DA, Hasler WL. Rome IV - Functional GI disorders: disorders of gut-brain interaction. Gastroenterology. 2016;150:1257-492.
- Ong AM, Chua LT, Khor CJ, Asokkumar R, Namasivayam V, Wang YT. Diaphragmatic Breathing Reduces Belching and Proton Pump Inhibitor Refractory Gastroesophageal Reflux Symptoms. Clin Gastroenterol Hepatol. 2018;16:407-16.
- Rinsma NF, Mauritz FA, van Heurn LW, Sloots CE, Siersema PD, Houwen RH, et al. Impact of laparoscopic antireflux surgery on belching in pediatric GERD patients. Neurogastroenterol Motil. 2016;28:1525-32.
- Woodley FW, Ciciora SL, Vaz K, Williams K, Di Lorenzo C, Jadcherla S. Novel Use of Impedance Technology Shows That Esophageal Air Events Can Be Temporally Associated With Gastroesophageal Reflux Disease-like Symptoms. J Pediatr Gastroenterol Nutr. 2020;70:e7-e11.