
Vol. 24 - Num. 95
Originales
Mycoplasma pneumoniae: características clínicas diferenciales y dificultades diagnósticas de las neumonías atípicas en niños
Mercedes Cemeli Canoa, Mónica López Camposb, Pilar Oliván Otalc, Eva M.ª Navarro Serranod, M.ª Isabel Lostal Graciab, César García Verae
aPediatra. CS Valdespartera. Zaragoza. España.
bPediatra. CS Actur Norte. Zaragoza. España.
cCS Canal Imperial. Zaragoza. España.
dPediatra. CS Alfajarín. Zaragoza. España.
ePediatra. CS José Ramon Muñoz Fernández. Zaragoza. España.
Correspondencia: M Cemeli. Correo electrónico: cano.mcemeli@salud.aragon.es
Cómo citar este artículo: Cemeli Cano M, López Campos M, Oliván Otal P, Navarro Serrano EM, Lostal Gracia MI, García Vera C. Mycoplasma pneumoniae: características clínicas diferenciales y dificultades diagnósticas de las neumonías atípicas en niños . Rev Pediatr Aten Primaria. 2022;24:273-84.
Publicado en Internet: 11-10-2022 - Número de visitas: 30175
Resumen
Este artículo ha sido corregido: ver la corrección en Rev Pediatr Aten Primaria. 2022; Vol. 24. N.º 96. Diciembre 2022.
Introducción: la neumonía por Mycoplasma pneumoniae continúa estando infradiagnosticada en las consultas de Pediatría de Atención Primaria, especialmente en los niños más pequeños.
Material y métodos: estudio prospectivo en 9 cupos pediátricos, sobre niños desde 1 mes a 14 años con neumonía diagnosticada mediante radiografía y clínica compatible. Diagnóstico etiológico mediante serología en la fase aguda. Se analiza la relación de diferentes variables con la etiología atípica y no atípica.
Resultados: de los 92 pacientes incluidos, un 30,4% fueron neumonías atípicas que, a pesar de no ser raras en menores de 2 años (26% del total a esta edad), predominaron en los mayores de 5 años (80,9%). La edad media en meses fue significativamente mayor en atípicas (74,2 ± 42,2), que en las no atípicas (35,9 ± 33,8; p <0,0001). La congestión nasal (42,8%; OR: 1,8; p <0,01) y la taquipnea (64,2%; OR: 2,4; p <0,014) fueron significativamente más frecuentes en las no atípicas y en las atípicas, respectivamente. El patrón alveolar se observó en el 53,6% de las neumonías atípicas, sin diferencias con las no atípicas. Solamente un 25% de las neumonías atípicas fueron correctamente tratadas inicialmente con macrólidos en monoterapia sin existir diferencias en cuanto a su evolución con respecto a la elección de un tipo u otro de terapia antibiótica. Las neumonías no atípicas precisaron antibioterapia intravenosa con una mayor frecuencia (15,6%) de forma no estadísticamente significativa.
Conclusión: las neumonías por gérmenes atípicos parecen más prevalentes en niños pequeños de lo previamente descrito, en ocasiones en coexistencia con virus. Su mejor diagnóstico y tratamiento continúan siendo un reto por resolver.
Palabras clave
● Mycoplasma pneumoniae ● Atención Primaria ● NeumoníaINTRODUCCIÓN
La neumonía adquirida en la comunidad (NAC) es una patología frecuente en la consulta de Atención Primaria, siendo en la mayoría de las ocasiones todo un reto diagnóstico en lo referente a su etiología1-3. En la última década, los cambios en las tendencias epidemiológicas demuestran que en la práctica diaria los patrones clínicos y radiológicos clásicamente descritos no siempre permiten el diagnóstico más exacto en pediatría, tal y como se corrobora en diferentes aportaciones en la bibliografía4-7. Incluso en el ámbito hospitalario, las pruebas microbiológicas no tienen la suficiente sensibilidad y especificidad, pudiéndose determinar la etiología de la neumonía en solo el 40-80% de los casos8.
Los principales agentes etiológicos se presuponen virus y neumococo, los primeros afectando fundamentalmente a menores de 5 años, y el segundo, a niños de cualquier edad. En los últimos 15 años se está observando un aumento de la incidencia de virus y gérmenes atípicos, pudiendo alcanzar el 30% de las causas de neumonía adquirida comunitaria. De este modo, según los signos y síntomas clínicos, sería difícil diferenciar entre neumonía típica y atípica.
De ahí la importancia de conocer los cambios epidemiológicos de nuestro entorno para revisar y mejorar las guías de actuación de las neumonías en la consulta de pediatría. En este trabajo se analizan las características de la etiología atípica en comparación al resto de neumonías, para orientar el abordaje de esta entidad en pediatría de Atención Primaria.
MATERIAL Y MÉTODOS
Estudio prospectivo observacional y analítico, en 9 cupos de pediatría de Atención Primaria de la provincia de Zaragoza, donde se incluyeron a lo largo de dos años naturales pacientes de 1 mes a 14 años con el diagnóstico clínico-radiológico de neumonía. Se consideró la radiografía de tórax anteroposterior como patrón oro para establecer el diagnóstico de NAC.
El caso de neumonía fue definido como la presencia en un paciente sano, de clínica respiratoria infecciosa compatible asociada a un patrón radiológico alveolar, intersticial, mixto o indefinido.
Se excluyeron: pacientes menores de 1 mes y mayores de 14 años; inmunodeficiencias primarias o secundarias; enfermedad neoplásica; patología pulmonar (fibrosis quística, asma mal controlado, secuestro pulmonar, bronquiectasia, displasia broncopulmonar); encefalopatías con posibilidad de broncoaspiración; pacientes positivos a la prueba de la tuberculina; neumonías en niños que habían sido hospitalizados en los 7-14 días previos al inicio de síntomas o cuando estos comenzaron en las primeras 48 horas de hospitalización; pacientes diagnosticados de neumonía por otro facultativo distinto al habitual en el estudio o diagnosticados en otro servicio en un periodo superior a 5 días; y pacientes en los que no se obtuvo el consentimiento informado.
Se recogió como variable principal el tipo de neumonía (atípica y no atípica -incluyendo entre estas las neumocócicas y víricas-), incluyendo otras variables secundarias de tipo: demográfico (edad, sexo), epidemiológico (antecedente de bronquitis y/o neumonías, vacunación), clínicas (temperatura, tos, frecuencia respiratoria (FR) según criterios de la OMS9, signos de dificultad respiratoria, saturación de oxígeno y otros síntomas extrapulmonares), radiológicas, analíticas (cifra absoluta de leucocitos, neutrófilos, proteína C reactiva (PCR), serología IgM de M. pneumoniae) y de tratamiento.
El diagnóstico de neumonía atípica se realizó mediante serología a M. pneumoniae (técnica ELISA basada en la reacción de los anticuerpos de la muestra con el antígeno unido a la superficie de poliestireno), que permite la cuantificación de IgM con una sensibilidad de 81-89% en niños10,11.
El diagnóstico de neumonía no atípica incluyó las de probable origen neumocócico (aquellas que no cumplían los requisitos del resto de los tipos de neumonías), mixta (determinación de más de dos gérmenes a la vez) y las de origen vírico diagnosticadas por positividad en el aspirado nasofaríngeo para virus (ANF) mediante inmunofluorescencia, que incluyó la determinación de: virus respiratorio sincitial (VRS), influenza A y B, parainfluenza 1,2,3, metapneumovirus y adenovirus.
Toda la información recogida se trató conforme a lo establecido en la Ley Orgánica 15/99, de Protección de Datos de Carácter Personal. En la base de datos del estudio no se incluyeron datos personales ni ningún dato que permitiera identificarlos. Se les asignó un código que solo el equipo investigador conocía. El proyecto fue aprobado por el Comité de Ética de Investigación de la comunidad de Aragón (CEICA) con fecha 17 febrero de 2017, expediente C.P.C.I. PI17/0000, Acta n.º 02/2017.
Análisis estadístico
Para el análisis descriptivo, se calcularon para las variables cuantitativas las medidas de tendencia central y de dispersión (media, mediana y desviación estándar) y para las cualitativas, las frecuencias absolutas y los porcentajes con sus respectivos intervalos de confianza al 95% (IC 95%). Para el estudio analítico, las relaciones entre variables se exploraron mediante el cálculo de la odds ratio (OR) y de la diferencia de medias (DM) con sus IC 95%. La significación estadística fue calculada mediante Chi cuadrado con corrección de Yates o la prueba exacta de Fisher y t-Student. Si en la comparación de medias alguna de las distribuciones no cumplía los criterios de normalidad, se utilizó la prueba no paramétrica U de Mann-Whitney. La relación entre las variables clínicas, analíticas y radiológicas con la posible etiología se evaluó mediante análisis univariante. Se diseñó también un modelo multivariante de regresión logística para predecir el tipo de neumonía según las diferentes variables, incluyendo aquellas que podrían relacionarse con el tipo de neumonía según el análisis univariante (valor de p <0,10), o también con criterios de plausibilidad biológica. Para todas las comparaciones, como umbral de significación estadística se tomó un valor de p ≤0,05.
Finalmente, se estudió la concordancia entre el diagnóstico inicial de sospecha realizado por cada colaborador de neumonía atípica basado en las características clínico-radiológicas y el diagnóstico de neumonía atípica con base en la serología positiva. No se incluyeron diagnósticos iniciales de neumonía no clasificable y neumonías mixtas para facilitar el análisis de concordancia.
RESULTADOS
Se incluyeron un total de 92 pacientes, un 30,4% (IC 95%: 21,9 a 40,5%) fueron diagnosticadas como neumonías atípicas por M. pneumoniae y un 69,6% como no atípicas. Entre los pacientes con neumonía atípica, el 64,3% (IC 95%: 45,8 a 79,3%) fueron mujeres, siendo en las no atípicas el 48,4% (IC 95%: 36,6 a 60,4%) sin diferencias estadísticas.
Se pudo extraer muestra para determinación serológica a M. pneumoniae en 81 pacientes. Se detectaron títulos elevados de Ig M frente a M. pneumoniae en un 39,5%. De los cuales, el 14,2% fueron infecciones mixtas de M. pneumoniae y virus (especialmente VRS). En el estudio serológico de gérmenes atípicos, hubo un paciente en el que se encontró una infección mixta de M. pneumoniae y Ch. pneumoniae, así como otra paciente con positividad triple para M. pneumoniae, citomegalovirus y parvovirus B19.
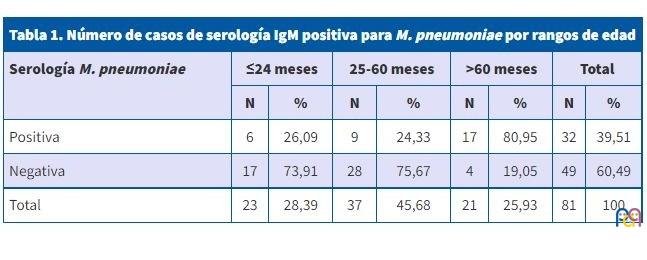
Dicha serología fue positiva fundamentalmente en los mayores de 5 años (80,9%; IC 95%: 60 a 92,3%), alcanzando el 26% (IC 95%: 12,5 a 46,5%) en menores de 2 años (Tabla 1).
| Tabla 1. Número de casos de serología IgM positiva para M. pneumoniae por rangos de edad | ||||||||
|---|---|---|---|---|---|---|---|---|
| Serología M. pneumoniae | ≤24 meses | 25-60 meses | >60 meses | Total | ||||
| N | % | N | % | N | % | N | % | |
| Positiva | 6 | 26,09 | 9 | 24,33 | 17 | 80,95 | 32 | 39,51 |
| Negativa | 17 | 73,91 | 28 | 75,67 | 4 | 19,05 | 49 | 60,49 |
| Total | 23 | 28,39 | 37 | 45,68 | 21 | 25,93 | 81 | 100 |
La edad media en meses fue significativamente mayor en las neumonías atípicas (74,2 ± 42,2 meses) que en el resto (35,9 ± 33,8 meses); DM: 38,32 (IC 95%: 20,11 a 56,54; p <0,001).
Noviembre y abril (con el 17,5% de neumonías atípicas detectadas cada uno) fueron los meses en los que se detectaron un mayor número de neumonías atípicas sin diferencias significativas respecto al resto de meses.
Destacó el antecedente de bronquitis previas, que fue mayor en el caso de las neumonías no atípicas (26,56%) que en las atípicas (17,8 %), sin que la diferencia fuera significativa, al igual que sucedió al valorar el antecedente de neumonías.
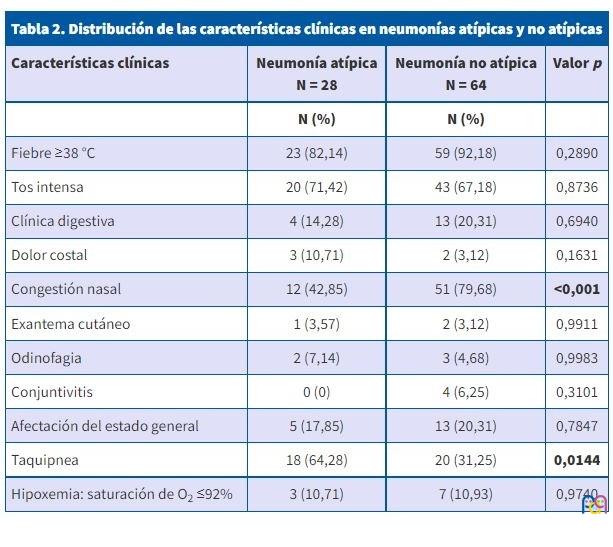
Tal y como se muestra en la Tabla 2, no existieron diferencias significativas en cuanto a la presentación clínica entre neumonías atípicas y no atípicas, así como en determinados signos exploratorios. La fiebre superior a 38 °C se dio en menor frecuencia en neumonías atípicas; sin embargo, del grupo de pacientes con ausencia de fiebre (n = 5), un 60% eran neumonías atípicas. La tos intensa se dio en mayor proporción en pacientes con neumonía atípica; sin embargo, estuvo ausente en el 3,6% de las neumonías atípicas. Otros síntomas que no se relacionaron de forma significativa con neumonías atípicas fueron la clínica digestiva, la conjuntivitis, la afectación del estado general, el dolor costal (la odinofagia, el exantema cutáneo y la hipoxemia Sat O2 <92%) a pesar de darse en menor proporción que en las neumonías no atípicas. En cambio, la congestión nasal (42,8%; OR: 1,8; p <0,01) y la taquipnea (64,2%; OR: 2,4; p <0,014) fueron significativamente más frecuentes en las no atípicas y en las atípicas, respectivamente. La mayoría de los pacientes no mostró signos de dificultad respiratoria, estando únicamente presente en el 7,1% en las neumonías por M. pneumoniae. Hay que destacar que los pacientes con dolor costal, se diagnosticaron como neumonía atípica en el 60% de los casos, siendo el resto, 40%, neumonías no atípicas.
| Tabla 2. Distribución de las características clínicas en neumonías atípicas y no atípicas | |||
|---|---|---|---|
| Características clínicas | Neumonía atípica N = 28 |
Neumonía no atípica N = 64 |
Valor p |
| N (%) | N (%) | ||
| Fiebre ≥38 °C | 23 (82,14) | 59 (92,18) | 0,2890 |
| Tos intensa | 20 (71,42) | 43 (67,18) | 0,8736 |
| Clínica digestiva | 4 (14,28) | 13 (20,31) | 0,6940 |
| Dolor costal | 3 (10,71) | 2 (3,12) | 0,1631 |
| Congestión nasal | 12 (42,85) | 51 (79,68) | <0,001 |
| Exantema cutáneo | 1 (3,57) | 2 (3,12) | 0,9911 |
| Odinofagia | 2 (7,14) | 3 (4,68) | 0,9983 |
| Conjuntivitis | 0 (0) | 4 (6,25) | 0,3101 |
| Afectación del estado general | 5 (17,85) | 13 (20,31) | 0,7847 |
| Taquipnea | 18 (64,28) | 20 (31,25) | 0,0144 |
| Hipoxemia: saturación de O2 ≤92% | 3 (10,71) | 7 (10,93) | 0,9740 |
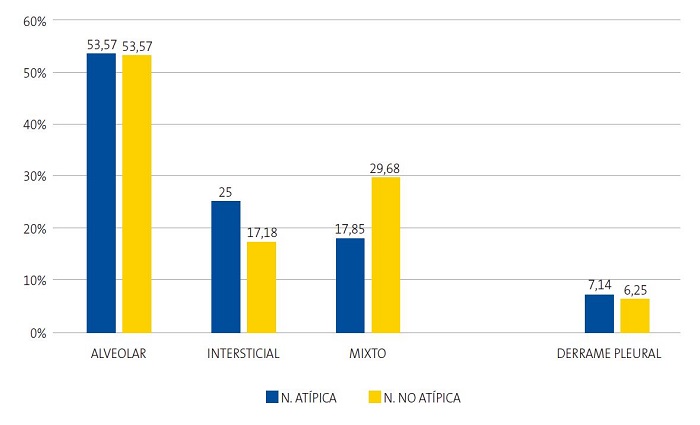
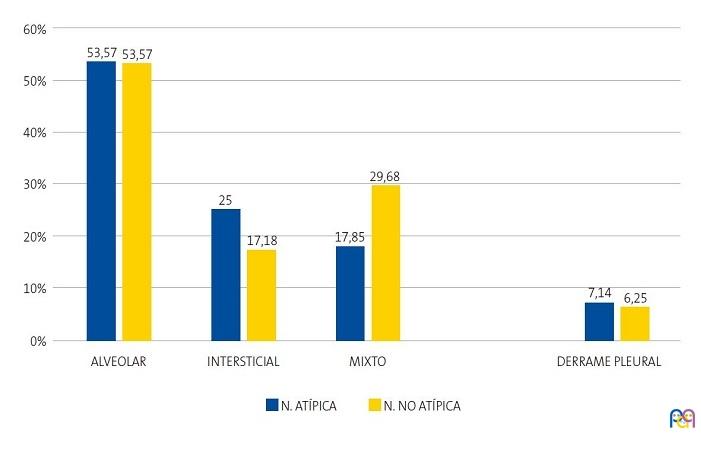
La Figura 1 muestra la ausencia de diferencias significativas entre los tipos de neumonía con los diferentes perfiles radiológicos anteriormente descritos y la existencia de derrame pleural. Un único caso de neumonía por M. pneumoniae no pudo ser clasificado en ningún patrón radiológico por el investigador. De esta forma, destaca que el patrón alveolar se observó en un porcentaje muy similar al otro grupo; sin embargo, el patrón intersticial fue más frecuente en neumonías atípicas que en las no atípicas sin diferencias significativas (p = 0,5042). El derrame pleural fue discretamente más frecuente en neumonías atípicas que en las no atípicas (p = 0,9890) de forma no significativa.
| Figura 1. Distribución (%) de los patrones radiológicos y derrame pleural en neumonías atípicas y no atípicas (n = 91) |
|---|
 |
La Tabla 3 muestra los valores y comparaciones estadísticas de los parámetros de laboratorio. Las cifras de leucocitos y neutrófilos fueron discretamente más elevadas en las neumonías no atípicas, pero sin diferencia estadísticamente significativa. Ninguna neumonía por M. pneumoniae mostró valores de PCR >6 mg/dl. Las cifras de PCR fueron mayores en el grupo de las neumonías no atípicas (6,6 ± 10,7 mg/dl) frente a las atípicas (1,7 ± 1,7 mg/dl), DM: -4,8 (IC 95%: -7,6 a -1,9; p = 0,0612).
| Tabla 3. Distribución de los valores analíticos en neumonías atípicas y no atípicas. Las variables cuantitativas con distribución normal (leucocitos) se expresan como media ± desviación estándar y las variables sin distribución normal (neutrófilos y PCR), como mediana y rango intercuartílico | ||||
|---|---|---|---|---|
| Neumonía atípica | Neumonía no atípica | DM; IC 95% y significación estadística | ||
| N.º de leucocitos x 1000 | N = 28 | N = 60 | ||
| Media | 10 817 | 12 013 | -1196; -3590 a 1199 (p = 0,3220) | |
| Desviación estándar | 5015 | 5662 | ||
| Mediana | 9500 | 10 800 | ||
| Rango intercuartílico | 7400-13 575 | 7875-15 225 | ||
| Moda | 5800 | 10 900 | ||
| N.º de neutrófilos x 1000 | N = 28 | N = 60 | ||
| Media | 5260 | 6376 | -1116; -3150 a 918 (U de Mann Whitney, p = 0,4965)* | |
| Desviación estándar | 3992 | 5311 | ||
| Mediana | 4600 | 4150 | ||
| Rango intercuartílico | 2450-5975 | 2700-8750 | ||
| Moda | 4800 | 2700 | ||
| PCR (mg/dl) | N = 24 | N = 60 | ||
| Media | 1,79 | 6,59 | -4,80; -7,65 a -1,95 (U de Mann Whitney, p = 0,0612)* | |
| Desviación estándar | 1,71 | 10,72 | ||
| Mediana | 0,92 | 2,40 | ||
| Rango intercuartílico | 0,38-2,33 | 0,46-6,28 | ||
| Moda | 0 | 0 | ||

Los ingresos en el caso de las no atípicas (27,2 %; IC 95: 21,2 a 43,4%) fueron significativamente más frecuentes que en las atípicas (7,1%; IC 95: 1,9 a 22,6%) (OR: 1,4; IC 95: 1,1 a 1,7; p = 0,0490), sin encontrarse diferencias con respecto a los diferentes motivos de ingreso.
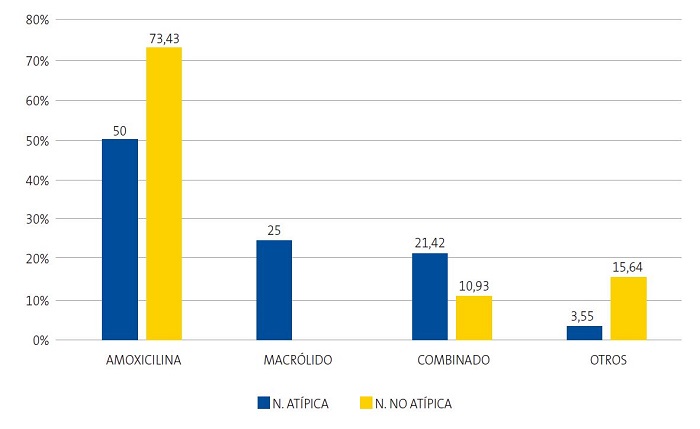
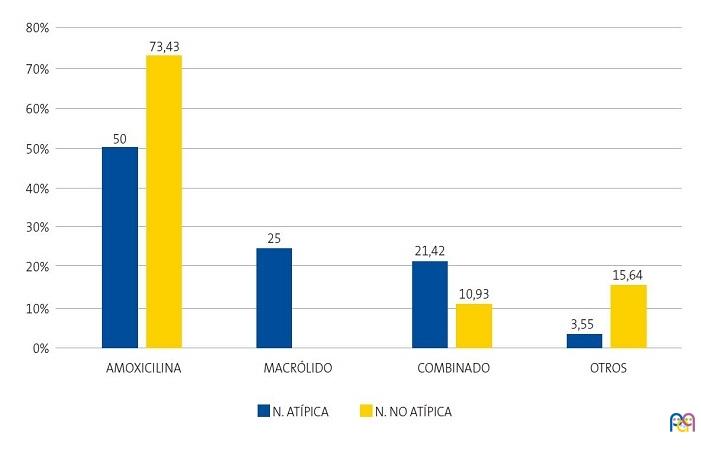
Se constataron diferencias significativas en el uso de amoxicilina (OR: 2,7; IC 95%: 1,1 a 6,9; p = 0,0286) en neumonías no atípicas frente a atípicas y de azitromicina (RP: 4,1; IC 95%: 2,7 a 5,8; p = 0,0002) en el grupo de neumonías atípicas frente al resto; sin embargo, no existieron en cuanto al tratamiento combinado de ambos, siendo muy similar en ambos tipos (OR: 0,4; IC 95%: 0,1 a 1,4; p = 0,3154). De este modo, vemos en la Figura 2 cómo una cuarta parte de las neumonías atípicas fueron tratadas correctamente con azitromicina en monoterapia y un 21,42% en combinación con amoxicilina y azitromicina, sin existir diferencias significativas en la elección de un tipo u otro de terapia antibiótica (OR: 2,2; IC 95%: 0,6 a 7,3; p = 0,3154). El tratamiento antibiótico intravenoso se precisó fundamentalmente en las neumonías no atípicas de forma no estadísticamente significativa.
| Figura 2. Distribución (%) de los principales antibióticos utilizados en neumonías atípicas y no atípicas (n = 92) |
|---|
 |
Con respecto a la evolución clínica, la duración de la fiebre más de 48 horas fue mayor en el grupo de neumonías no atípicas (25%) que en las atípicas (11,1%), sin existir diferencias estadísticamente significativas. En cambio, al mes de tratamiento, la tos persistió más frecuentemente en las neumonías atípicas (11,1%; IC 95%: 3,8 a 28,1 %; p = 0,3153) pero con una auscultación cardiopulmonar normalizada más rápidamente (88,9%; IC 95%: 71,9 a 96,1 %; p = 0,2172).
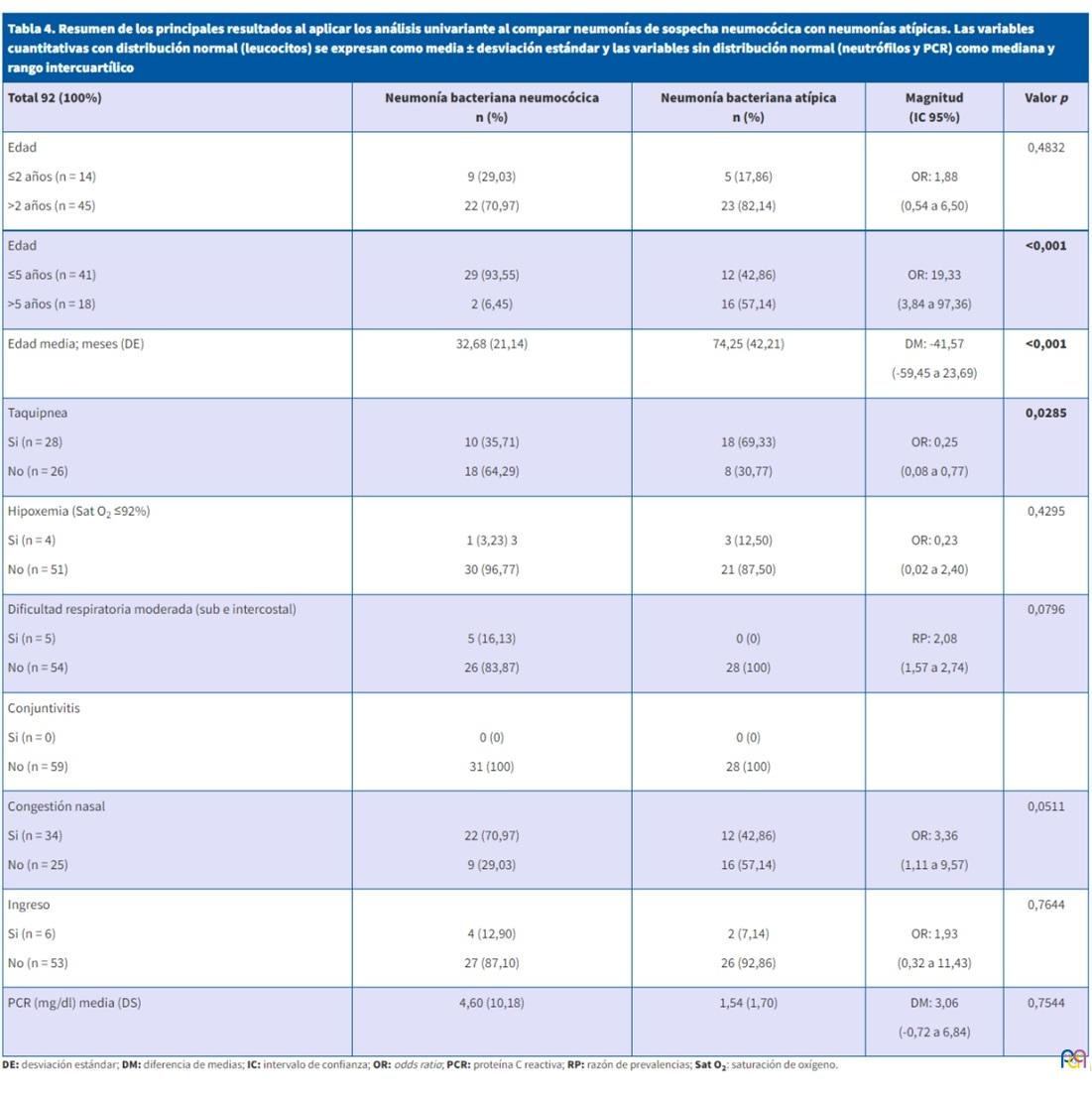
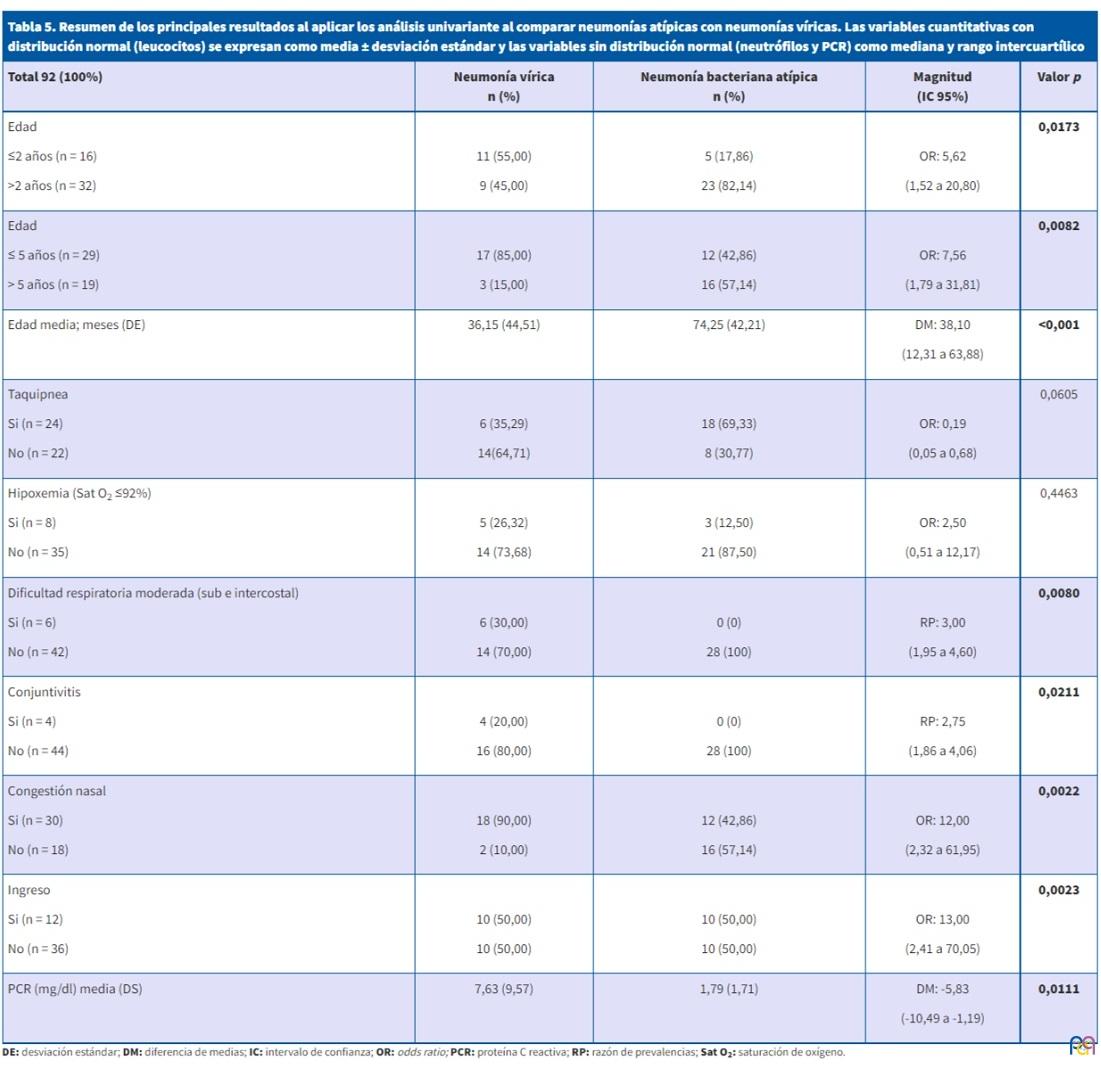
Las variables relacionadas significativamente con el tipo de neumonía quedan reflejadas en las Tablas 4 y 5. A su vez, se realizó un estudio multivariante comparando los tres tipos principales de neumonía (bacteriana de sospecha neumocócica, bacteriana atípica y vírica). La edad media fue significativamente mayor en las neumonías atípicas frente a las de sospecha neumocócica. Además, se obtuvieron unas menores tasas de hipoxemia y de ingreso en neumonías atípicas frente al resto. Los valores de PCR se mostraron únicamente más elevados en neumonías víricas frente a neumonías atípicas.
| Tabla 4. Resumen de los principales resultados al aplicar los análisis univariante al comparar neumonías de sospecha neumocócica con neumonías atípicas. Las variables cuantitativas con distribución normal (leucocitos) se expresan como media ± desviación estándar y las variables sin distribución normal (neutrófilos y PCR) como mediana y rango intercuartílico | ||||
|---|---|---|---|---|
| Total 92 (100%) | Neumonía bacteriana neumocócica n (%) |
Neumonía bacteriana atípica n (%) |
Magnitud (IC 95%) |
Valor p |
|
Edad ≤2 años (n = 14) >2 años (n = 45) |
9 (29,03) 22 (70,97) |
5 (17,86) 23 (82,14) |
OR: 1,88 (0,54 a 6,50) |
0,4832 |
|
Edad ≤5 años (n = 41) >5 años (n = 18) |
29 (93,55) 2 (6,45) |
12 (42,86) 16 (57,14) |
OR: 19,33 (3,84 a 97,36) |
<0,001 |
|
Edad media; meses (DE) |
32,68 (21,14) |
74,25 (42,21) |
DM: -41,57 (-59,45 a 23,69) |
<0,001 |
|
Taquipnea Sí (n = 28) No (n = 26) |
10 (35,71) 18 (64,29) |
18 (69,33) 8 (30,77) |
OR: 0,25 (0,08 a 0,77) |
0,0285 |
|
Hipoxemia (Sat O2 ≤92%) Sí (n = 4) No (n = 51) |
1 (3,23) 3 30 (96,77) |
3 (12,50) 21 (87,50) |
OR: 0,23 (0,02 a 2,40) |
0,4295 |
|
Dificultad respiratoria moderada (sub e intercostal) Sí (n = 5) No (n = 54) |
5 (16,13) 26 (83,87) |
0 (0) 28 (100) |
RP: 2,08 (1,57 a 2,74) |
0,0796 |
|
Conjuntivitis Sí (n = 0) No (n = 59) |
0 (0) 31 (100) |
0 (0) 28 (100) |
|
|
|
Congestión nasal Sí (n = 34) No (n = 25) |
22 (70,97) 9 (29,03) |
12 (42,86) 16 (57,14) |
OR: 3,36 (1,11 a 9,57) |
0,0511 |
|
Ingreso Sí (n = 6) No (n = 53) |
4 (12,90) 27 (87,10) |
2 (7,14) 26 (92,86) |
OR: 1,93 (0,32 a 11,43) |
0,7644 |
|
PCR (mg/dl) media (DS)
|
4,60 (10,18) |
1,54 (1,70) |
DM: 3,06 (-0,72 a 6,84) |
0,7544 |
| Tabla 5. Resumen de los principales resultados al aplicar los análisis univariante al comparar neumonías atípicas con neumonías víricas. Las variables cuantitativas con distribución normal (leucocitos) se expresan como media ± desviación estándar y las variables sin distribución normal (neutrófilos y PCR) como mediana y rango intercuartílico | ||||
|---|---|---|---|---|
| Total 92 (100%) | Neumonía vírica n (%) |
Neumonía bacteriana atípica n (%) |
Magnitud (IC 95%) |
Valor p |
|
Edad ≤2 años (n = 16) >2 años (n = 32) |
11 (55,00) 9 (45,00) |
5 (17,86) 23 (82,14) |
OR: 5,62 (1,52 a 20,80) |
0,0173 |
|
Edad ≤ 5 años (n = 29) > 5 años (n = 19) |
17 (85,00) 3 (15,00) |
12 (42,86) 16 (57,14) |
OR: 7,56 (1,79 a 31,81) |
0,0082 |
|
Edad media; meses (DE) |
36,15 (44,51) |
74,25 (42,21) |
DM: 38,10 (12,31 a 63,88) |
<0,001 |
|
Taquipnea Si (n = 24) No (n = 22) |
6 (35,29) 14(64,71) |
18 (69,33) 8 (30,77) |
OR: 0,19 (0,05 a 0,68) |
0,0605 |
|
Hipoxemia (Sat O2 ≤92%) Si (n = 8) No (n = 35) |
5 (26,32) 14 (73,68) |
3 (12,50) 21 (87,50) |
OR: 2,50 (0,51 a 12,17) |
0,4463 |
|
Dificultad respiratoria moderada (sub e intercostal) Si (n = 6) No (n = 42) |
6 (30,00) 14 (70,00) |
0 (0) 28 (100) |
RP: 3,00 (1,95 a 4,60) |
0,0080 |
|
Conjuntivitis Si (n = 4) No (n = 44) |
4 (20,00) 16 (80,00) |
0 (0) 28 (100) |
RP: 2,75 (1,86 a 4,06) |
0,0211 |
|
Congestión nasal Si (n = 30) No (n = 18) |
18 (90,00) 2 (10,00) |
12 (42,86) 16 (57,14) |
OR: 12,00 (2,32 a 61,95) |
0,0022 |
|
Ingreso Si (n = 12) No (n = 36) |
10 (50,00) 10 (50,00) |
10 (50,00) 10 (50,00) |
OR: 13,00 (2,41 a 70,05) |
0,0023 |
|
PCR (mg/dl) media (DS) |
7,63 (9,57) |
1,79 (1,71) |
DM: -5,83 (-10,49 a -1,19) |
0,0111 |
Finalmente, en el estudio la concordancia entre el diagnóstico inicial de sospecha de neumonía atípica y el diagnóstico final de neumonía atípica con base en la serología positiva, se encontró un coeficiente de kappa 0,26 que, según la clasificación de Freiss, es una correlación débil (Tabla 6).
| Tabla 6. Número de casos del resultado de la serología para M. pneumoniae y el diagnóstico de sospecha de neumonía | |||
|---|---|---|---|
| Serología positiva | Serología negativa | Total | |
| Neumonía atípica | 6 | 10 | |
| Neumonía no atípica | 22 | 44 | 66 |
| Total | 28 | 48 | 76 |
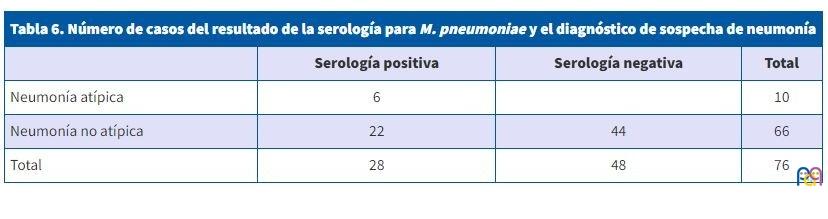
De este modo, el diagnóstico de sospecha de neumonía atípica fue confirmado únicamente en 6 de 28 casos (21,4%). Sin embargo, el diagnóstico de neumonía no atípica fue correcto en el 91,6% (44 casos de 48). El VPP de la sospecha clínico-radiológica fue de 60% (IC 95%: 29,6 a 90,3%) y el VPN de 66,6% (IC 95%: 55,3 a 78,1%). La sensibilidad del diagnóstico clínico de neumonía atípica fue del 21,4% (IC 95%: 6,2 a 36,6%), la especificidad del 91,6% (IC 95%: 83,85% a 99,4%), la PFP (probabilidad de falsos positivos) 8,3%, PFN (probabilidad de falsos negativos) 78,5% y con CP+ (coeficiente de probabilidad positiva) de 2,5 (IC 95%: 0,8 a 8,3) y CP- (coeficiente de probabilidad negativa) de 0,8 (IC 95%: 0,6 a 1,1). Estos coeficientes de probabilidades (según el Evidence-Based Medicine Working Group) indican que generan cambios pequeños (en ocasiones importantes) de la probabilidad.
DISCUSIÓN
Nuestro estudio recoge un total de 92 pacientes, de los cuales 28 fueron neumonías por M. pneumoniae diagnosticadas preferentemente desde AP y en su mayoría con buena evolución tras el tratamiento antibiótico empírico.
En nuestra serie, se estableció el diagnóstico de neumonía atípica en el 30% de los pacientes y el de neumonía mixta en el 4%, al asociarse con otro germen, generalmente con virus. Por otro lado, el 80% de estas serologías positivas fueron encontradas en pacientes con edad superior a 5 años; sin embargo, en el resto de los rangos de edad, llegó a alcanzar el 30%, cifra a tener en cuenta a la hora de la sospecha de gérmenes atípicos en el resto de las edades12-15. Estos resultados concuerdan con los presentados en otros estudios, con incidencias de gérmenes atípicos entre el 30-40%16-18. Sin embargo, no hay acuerdo sobre el papel de la coinfección de M. pneumoniae con virus, en cuanto a pronóstico y evolución, ni se puede precisar si los agentes son concomitantes en el tiempo o agravantes evolutivos19,20.
De esta forma, hemos podido determinar la incidencia aproximada de los gérmenes atípicos en nuestra población de referencia. Entre los casos existe un alto porcentaje de infectados menores de 5 años, con una edad promedio por debajo de lo establecido clásicamente. Este alto porcentaje puede deberse a la escolarización precoz y, con ello, una sensibilización que predispone a que nuevos contactos con el microorganismo determine infecciones más graves, de forma más temprana. Pero también podría ser atribuible a una limitación del estudio que utilizó Ig M para el diagnóstico y esta no aumenta en las reinfecciones, sino que se produce una respuesta rápida de Ig G e Ig A, que en estos pacientes no se estudiaron, por lo que no se detectaron algunos casos que podrían haber ocurrido en escolares y adolescentes. Además, estudios hospitalarios como el de Wood et al.17, reportaron un 56% de niños sanos con colonización por M. pneumoniae mediante técnicas PCR a partir de muestras nasofaríngeas y de técnicas serológicas (Ig M e Ig G).
No obstante, la proporción de neumonías atípicas en el estudio es relevante y en concordancia con las publicaciones más recientes2,5,26, lo que apunta a la posibilidad de que estén infradiagnosticadas en la población infantil, con una incidencia real desconocida.
La edad fue una de las principales variables estudiadas y, coincidiendo con lo descrito, resultaron más prevalentes las neumonías atípicas en mayores de 60 meses. Hasta hace poco, la edad era considerada como el principal factor predictivo del tipo de neumonía21-24. Coincidiendo con la mayoría de las series, en las atípicas23,24,27,28, la media de edad fue significativamente mayor, en comparación al resto de neumonías.
Entre las manifestaciones clínicas más frecuentes en neumonías por M. pneumoniae, destacaron: la fiebre, tos, congestión nasal, afectación del estado general, clínica digestiva y taquipnea, siendo este último el que alcanzó la diferencia significativa frente al grupo de no atípicas, especialmente frente a las de sospecha neumocócica. Este dato se ha analizado en pocos estudios29, siendo un hallazgo interesante al tratarse de neumonías con clínica más larvada cuyo diagnóstico podría demorarse en el tiempo. Algunos de estos estudios encontraron únicamente pacientes con taquipnea en el caso de que la neumonía por M. pneumoniae se asociara a infección con un virus29. En esta misma línea, y en contra del patrón clínico más larvado de este tipo de neumonías, Søndergaard et al.29 publicaron una incidencia del 100% de tos asociada al signo de taquipnea en neumonías atípicas.
Por otro lado, destaca que el dolor costal fue 3 veces más prevalente en las neumonías atípicas que en el resto, posiblemente influenciado por una edad mayor de los niños, capaces de referir verbalmente síntomas tan subjetivos como es el dolor.
Dentro del patrón alveolar fue similar la proporción de neumonías atípicas y no atípicas, en contra de los patrones descritos1,10 y en la misma dirección de los últimos trabajos publicados, en los que ningún patrón se muestra como exclusivo de una etiología concreta5,6,22,30. La condensación lobar ya no puede considerarse un hallazgo patognomónico de la etiología bacteriana típica, dada la elevada proporción en la que se encuentra en los pacientes con neumonía atípica, aumentando si existe coinfección con virus23,29,30.
Otro dato que destacar fue que el porcentaje de neumonías por M. pneumoniae que asociaron derrame pleural fue muy similar a las no atípicas, similar a recientes trabajos que alcanzan proporciones de hasta un 18%29 en asociación con virus. Generalmente, hacen referencia a pequeños derrames pleurales, con poca expresión clínica.
Por otro lado, se muestra cómo los parámetros de laboratorio no son específicos de la etiología bacteriana, ofreciendo únicamente información adicional al diagnóstico, tal y como demuestran otros autores31,32. Además, la eficacia de la serología como método aislado es especialmente controvertida en el caso de M. pneumoniae, habiéndose demostrado más eficaz el uso conjunto con la reacción en cadena de la polimerasa (PCR) para detectar el ADN del germen. Serán necesarios más avances en este campo para poder obtener resultados fiables de una forma rápida que facilite la toma de decisiones en la consulta de AP.
La mayoría de las pacientes en nuestra serie recibieron como tratamiento amoxicilina por vía oral, utilizándose correctamente en monoterapia en el 80% de las neumonías no atípicas, pero también se prescribió en la mitad de las atípicas, siendo favorable la evolución. Solamente una cuarta parte de las neumonías atípicas fueron tratadas con macrólidos considerando el diagnóstico de presunción, sin evidenciar diferencias en la evolución respecto a las tratadas con beta-lactámicos, hallazgo compartido por alguna revisión sistemática18,33. Es interesante destacar la resolución clínica de la neumonía con la utilización de amoxicilina, sin necesidad de utilizar macrólido, a pesar de la positividad para M. pneumoniae. Los beneficios del tratamiento antibiótico con M. pneumoniae en niños no ha sido estudiado adecuadamente33. Existen varias revisiones sistemáticas18,33,34 que muestran resultados similares, donde el beneficio de tratamiento con macrólidos en neumonías por M. pneumoniae es incierto en niños. Por ello, algunos autores han considerado innecesaria la terapia antibiótica de estas infecciones respiratorias atípicas por tratarse, la mayoría de las veces, de una infección autolimitada, aunque la antibioterapia reduciría la duración de los síntomas y la transmisión. De ahí, la importancia de la necesidad de mejora en el diagnóstico inicial etiológico.
Una de las principales limitaciones de nuestro estudio afecta a la potencia estadística derivada del tamaño muestral (n = 92) y puede determinar resultados estadísticamente no significativos que podrían cambiar la tendencia con un mayor número de casos incluidos. Se ha considerado una clasificación del tipo de neumonía que podría ser aplicable teniendo en cuenta las limitaciones y la falta de disponibilidad de las técnicas de diagnóstico etiológico en las consultas de AP. Por eso, la asunción en este estudio obliga a interpretar los datos con cautela.
Debido a la limitación de las técnicas de diagnóstico etiológico disponibles en AP, se asumió como válida la positividad en la primera semana de diagnóstico, de Ig M para M. pneumoniae, mediante técnicas cualitativas (ELISA). Se sabe que no existen pruebas lo suficientemente sensibles que permitan un diagnóstico rápido y fiable de infección por M. pneumoniae. La guía de manejo de la IDSA recomienda la realización de serología (en fase inicial y de convalecencia) o PCR de secreciones nasofaríngeas (más rápida y elevada especificidad). Sin embargo, el aumento del coste de recursos que suponía en nuestra área de AP impidió que dichas técnicas se llevaran a cabo.
Finalmente, este trabajo aporta datos que muestran pocos rasgos epidemiológicos, clínicos o radiológicos diferenciales de los tipos de neumonía entre los considerados hasta la actualidad, para orientar en el diagnóstico etiológico, especialmente en lo referente a gérmenes atípicos.
ABREVIATURAS
ANF: aspirado nasofaríngeo para virus · CP-: coeficiente de probabilidad negativa · CP+: coeficiente de probabilidad positiva · FR: frecuencia respiratoria · IC 95%: intervalos de confianza al 95% · NAC: neumonía adquirida en la comunidad · PCR: proteína C reactiva · PFN: probabilidad de falsos negativos · PFP: probabilidad de falsos positivos · VPN: valor predictivo negativo · VPP: valor predictivo positivo · VRS: virus respiratorio sincitial.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
El proyecto de investigación fue financiado parcialmente con la beca José María Mengual Mur de la Fundación para el progreso de la Pediatría del año 2018.
BIBLIOGRAFÍA
- Andrés Martín A, Moreno-Pérez D, Alfayate Miguélez S, Couceiro Gianzo JA, García García ML, Korta Murua J, et al. Etiología y diagnóstico de la neumonía adquirida en la comunidad y sus formas complicadas. An Pediatr (Barc). 2012;76:162.e1-162.e18.
- Honkinen M, Lahti E, Osterback R, Ruuskanen O,Waris M. Viruses and bacteria in sputum samples of children with community-acquired pneumonia. Clin Microbiol Infect. 2012;18:300-7.
- Infants and Children: Acute Management of Community Acquired Pneumonia. En: NSW Health. Guideline. Agency for Clinical Innovation; 2018 [en línea] [consultado el 15/09/2022]. Disponible en https://www1.health.nsw.gov.au/pds/ActivePDSDocuments/GL2018_007.pdf
- Aguilera-Alonso D, Illán-Ramos M, Daoud Z, Guinea V, Culebras E, Ramos JT. Análisis del impacto de los test de diagnóstico virológico en el consumo de antibióticos en pacientes pediátricos ingresados por neumonía adquirida en la comunidad. Enferm Infecc Microbiol Clin. 2020;38:230-3.
- Nelson KA, Morrow C, Wingerter SL, Bachur RG, Neuman MI. Impact of chest radiography on antibiotic treatment for children with suspected pneumonia. Pediatr Emerg Care. 2016;32:514-9.
- Neuman MI, Graham D, Bachur R. Variation in the use of chest radiography for pneumonia in pediatric emergency departments. Pediatr Emerg Care. 2011;27:606-10.
- Clark JE, Hammal D, Hamptom F, Spencer D, Parker l. Epidemiology of community-acquired pneumonia in children seen in hospital. Epidemiol Infect. 2007;135:262-9.
- Heiskanen-Kosma T, Korppi M, Jokinen C, Kurki S, Heiskanen l, Juvonen H, et al. Etiology of childhood pneumonia: Serologic results of a prospective, population-based study. Pediatr Infect Dis J. 1998;17:986-91.
- The Management of acute respiratory infections in children: practical guidelines for outpatient care. En: World Health Organization; 1995 [en línea] [consultado el 15/09/2022]. Disponible en https://apps.who.int/iris/handle/10665/41803
- Giménez Sánchez F, Sánchez Marenco A, Battles Garrido JM, López Soler JA, Sánchez-Solís Querol M. Características clínico-epidemiológicas de la neumonía adquirida en la comunidad en niños menores de 6 años. An Pediatr (Barc). 2007;66:578-84.
- Rudan I, O’Brien KL, Nair H, Liu l, Theodoratou E, Qazi S, et al. Epidemiology and etiology of childhood pneumonia in 2010: estimates of incidence, severe morbidity, mortality, underlying risk factors and causative pathogens for 192 countries. J Glob Health. 2013;3:010401.
- Korppi M, Heiskanen-Kosma T, Kleemola M. Incidence of community-acquired pneumonia in children caused by pneumoniae: serological results of a prospective, population-based study in primary health care. Respirology. 2004;9:109-14.
- Layani-Milon MP, Gras I, Valette M, Luciani J, Stagnara J, Aymard M, et al. Incidence of upper respiratory tract pneumoniae infections among outpatients in Rhone-Alpes, France, during five successive winter periods. J Clin Microbiol. 1996;34:447-9.
- Rasmussen JN, Voldstedlund M, Andersen RL, Ellermann-Eriksen S, Jensen TG, Johansen HK, et al. Increased incidence of pneumoniae infections detected by laboratory-based surveillance in Denmark in 2010. Euro Surveill. 2010;15:19708.
- Jacobs E. Pneumoniae disease manifestations and epidemiology. En: Razin S, Herrman R, editores. Molecular biology and pathogenicity of mycoplasmas. Kluwer New York: Academic/Plenum Publishers; 2002. p. 519-30.
- Baer G, Engelcke G, Abele-Horn M, Schaad UB, Heininger U. Role of Chl. pneumoniae and pneumoniae as causative agents of community-acquired pneumonia in hospitalised children and adolescents. Eur J Clin Microbiol Infect Dis. 2003;22:742-5.
- Wood PR, Hill VL, Burks ML, Peters JI, Singh H, Kannan TR, et al. Mycoplasma pneumoniae in children with acute and refractory asthma. Ann Allergy Asthma Immunol. 2013;110:328-34.
- Mulholland S, Gavranich JB, Gillies MB, Chang AB. Antibiotics for community acquired lower respiratory tract infections secondary to pneumoniae in children. The Cochrane Database of Systematic Reviews 2012;9:CD004875.
- Cimolai N, Wensley D, Seear M. Mycoplasma pneumoniae as a cofactor in severe respiratory infections. Clin Infect Dis. 1995;21:1182-5.
- Cemeli Cano M, Laliena Aznar S, Beltrán García S, Sáez de Adana Pérez ME y García Vera C. Neumonía muy atípica en paciente de dos años. Rev Pediatr Aten Primaria. 2019:21:61-4.
- Harris M, Clark J, Coote N, Fletcher P, Harnden A, McKean M, Thomson A. British Thoracic Society guidelines for the management of community acquired pneumonia in children. Thorax. 2011;66:1-23
- Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, et al. The management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011;53:25-76.
- Úbeda Sansano MI, Murcia García J, Asensi Monzó MT y Grupo de Vías Respiratorias. Neumonía adquirida en la comunidad. El pediatra de Atención Primaria y la Neumonía. Protocolo del GVR (publicación P-GVR-8) [en línea] [consultado el 15/09/2022]. Disponible en www.aepap.org/sites/default/files/documento/archivos-adjuntos/protocolo-neumonia-2017.pdf
- Byington CL, Bradley JS. Pediatric community-acquired pneumonia. In: Feigin and Cherry’s Textbook of Pediatric Infectious Diseases, 7th ed, Cherry JD, Harrison GJ, Kaplan SL, Steinbach W, Hotez P (Eds), Elsevier Saunders, Philadelphia 2014; 283.
- Clark JE, Hammal D, Spencer D, Hampton F. Children with pneumonia: how do they present and how are they managed? Arch Dis Child. 2007;92:394-8.
- Jain S, Williams DJ, Arnold SR, Ampofo K, Bramley AM, Reed C, et al. Community-acquired pneumonia requiring hospitalization among U.S. children. N Engl J Med. 2015;372:835-45.
- Garcés-Sánchez MD, Díez-Domingo J, Ballester Sanz A, Peidro Boronat C, García López M, Antón Crespo V, et al. Epidemiología de la neumonía adquirida en la comunidad en menores de 5 años en la Comunidad Valenciana. An Pediatr (Barc). 2005;63:125-30.
- Jiang W, Wu M, Zhou J, Wang Y, Hao C, Ji W, et al. Etiologic spectrum and occurrence of coinfections in children hospitalized with community-acquired pneumonia. BMC Infectious Diseases. 2017;17:787-95.
- Søndergaard MJ, Friis MB, Hansen DS, Jørgensen IM. Clinical manifestations in infants and children with pneumoniae infection. PLoS One 2018 Apr 26;13(4):e0195288.
- Finnegan OC, Fowles SJ, White RJ. Radiographic appearances of pneumoniae. Thorax. 1981;36:469-72.
- Summah H, Qu JM. Biomarkers: A definite plus in pneumonia. Mediators Inflamm. 2009;6753-62.
- Peltola V, Mertsola J, Ruuskanen O. Comparison of total white blood cell count and serum C reactive protein levels in confirmed bacterial and viral infections. J Pediatr. 2006;149:721-4.
- Biondi E, McCulloh R, Alverson B, Klein A, Dixon A, Ralston S. Treatment of pneumoniae: A systematic review. Pediatrics. 2014;133:1081-90.
- Gardiner SJ, Gavranich JB, Chang AB. Antibiotics for community-acquired lower respiratory tract infections secondary to pneumoniae in children. Cochrane Database Syst Rev. 2015; 1:CD004875.