
Vol. 24 - Num. 95
Originales
Sensibilidad del test de diagnóstico rápido SARS-CoV-2 Panbio en Atención Primaria
Ana M.ª Alonso Rubioa, Mercedes Garrido Redondob, M.ª Rosario Bachiller Luquec, M.ª Luisa Vega Gutiérrezc, Cristina García de Riverad, Beatriz Liras Muñoze, Teresa Palencia Ercillaf, Mónica Sanz Fernándezg, M.ª Jesús Alonso Ballesterosh, M.ª Fe Muñoz Morenoi, Paula Borregón Garridoj
aPediatra. CS Covaresa-Parque Alameda. Valladolid. España.
bPediatra. CS La Tórtola. Valladolid. España.
cPediatra. CS Pilarica. Valladolid. España.
dPediatra. CS Rondilla. Valladolid. España.
ePediatra. CS Cuéllar. Cuellar. Segovia. España.
fPediatra. CS Cuellar. Cuellar. Segovia. España.
gPediatra. CS Pisuerga. Arroyo de la Encomienda. Valladolid. España.
hPediatra. CS Medina del Campo. Valladolid. España.
iPediatra. Unidad de Apoyo a la Investigación. Hospital Clínico Universitario. Valladolid. España.
jEstudiante de Medicina. Facultad de Medicina. Universidad de Valladolid. Valladollid. España.
Correspondencia: AM Alonso . Correo electrónico: alonsoam04@hotmail.com
Cómo citar este artículo: Alonso Rubio AM, Garrido Redondo M, Bachiller Luque MR, Vega Gutiérrez ML, García de Rivera C, Liras Muñoz B, et al. Sensibilidad del test de diagnóstico rápido SARS-CoV-2 Panbio en Atención Primaria . Rev Pediatr Aten Primaria. 2022;24:e283-e289.
Publicado en Internet: 21-09-2022 - Número de visitas: 12222
Resumen
Introducción y objetivos: los pediatras de Atención Primaria necesitamos técnicas de diagnóstico rápido (TDR) fiables para prevenir la propagación de la enfermedad COVID-19 mediante un cribado temprano y eficaz a la espera de una vacuna. El objetivo de este trabajo fue evaluar como novedad en Atención Primaria, tanto en adultos como niños, sintomáticos y contactos asintomáticos, la sensibilidad (S) de los test de antígeno SARS-CoV-2 Panbio del laboratorio Abbott respecto a la reacción en cadena de la polimerasa (PCR).
Pacientes y métodos: se incluyeron 591 pacientes (222 menores de 14 años) (249 sintomáticos y 342 contactos). Se calculó la sensibilidad (S) y la especificidad (E) junto con sus intervalos de confianza (IC) del 95%. La independencia de los dos resultados ha sido analizada mediante el test de McNemar.
Resultados: la S del test en adultos fue del 81% (IC 95%: 66,16-96,34) y en niños del 80% (IC 95%: 34,94-100) dentro de los 5 primeros días. En contactos se evaluó la S en los cinco primeros días, en adultos (68%; IC 95%: 51,13-86,37), del 5.º al 9.º día (85%) y en niños (66%; IC 95%: 30,31-100). El tipo de contacto más frecuente fue domiciliario en un 52% de los casos. La E fue 100% en todos los casos.
Conclusiones: el test rápido de antígeno SARS-CoV-2 Panbio puede ser útil para diagnóstico de adultos y niños los primeros cinco días de inicio de síntomas, así como entre el 5.º y 9.º día tras el contacto con positivo COVID-19 confirmado, pendiente de interpretar en futuros estudios.
Palabras clave
● Atención Primaria ● COVID-19 ● Diagnóstico en el punto de atención ● SARS-CoV-2INTRODUCCIÓN
La importancia de un diagnóstico precoz de la enfermedad COVID-19 en Atención Primaria radica en evitar la propagación del virus SARS-CoV-2 mediante un cribado temprano y eficaz para proceder a un aislamiento casi inmediato. Para ello son necesarias técnicas de diagnóstico rápido (TDR) que sean fiables1-4. El objetivo de este trabajo fue evaluar la sensibilidad (S) del uso de los primeros test inmunocromatográficos de antígeno Panbio COVID-19 (Abbott Diagnostic GmbH, Jena, Alemania) en los centros de salud, respecto de la reacción en cadena de la polimerasa (PCR) hospitalaria, a lo largo de los primeros días tras el inicio de los síntomas o contacto con positivo, tanto en niños como en adultos. Varios estudios demuestran que la detección del antígeno tiene mayor correlación que la PCR con el cultivo del virus, lo que podría hacer más probable el contagio5,6.
MATERIAL Y MÉTODOS
Participantes
Participaron en el estudio 7 centros de Atención Primaria de las provincias de Valladolid y Segovia (España) entre los meses de octubre y noviembre de 2020. Se incluyeron pacientes con síntomas COVID-19 y contactos asintomáticos en los que se solicitó prueba de PCR. Se excluyeron aquellas muestras con resultado dudoso, toma dificultosa o que tenían PCR positiva previa conocida (2%) o con test de anticuerpos positivos para IgG (7,8%). De un total de 591 pacientes incluidos, 249 presentaban síntomas compatibles con enfermedad COVID-19 y 342 eran contactos asintomáticos con positivo.
El 55,9% fueron mujeres y 222 eran menores de 14 años (media 6,69 años, DE [desviación estándar] 3,9).
Tanto pediatras como personal de enfermería entrenados hicieron dos tomas de frotis nasofaríngeo a cada paciente. Con la primera muestra se realizó el test de antígeno Panbio COVID-19 Abbott con lectura a los 15 minutos in situ según las instrucciones del fabricante; mientras el segundo hisopo de muestra se introdujo en medio de transporte universal para virus (Deltalab, MDD, CE 0318, España) para análisis en las posteriores 24 horas de PCR (prueba Cobas® SARS-CoV-2 para su uso en los sistemas Cobas® 6800/8800 Systems) en el servicio de Microbiología del Hospital de referencia (Hospital Clínico de Valladolid, Hospital del Río Hortega, Hospital de Segovia).
El proyecto fue aprobado por el Comité de Ética e Investigaciones Científicas de la Gerencia Regional de Salud. Todos los pacientes a los que se propuso participar aceptaron voluntariamente el consentimiento informado y, en el caso de menores, a través de su progenitor o tutor legal.
Los reactivos fueron proporcionados por la Gerencia Regional de Salud de Castilla y León. No existe conflicto de intereses con la industria farmacéutica.
Análisis estadístico
Las variables cuantitativas se presentan con la media y la desviación típica y las cualitativas según su distribución de frecuencias.
A partir de las respuestas del test y las obtenidas en la PCR se ha calculado la S y la especificidad (E) junto con sus intervalos de confianza del 95%. La independencia de los dos resultados ha sido analizada mediante el test de McNemar.
Los datos se han obtenido con el programa estadístico IBM SPSS Statistics versión 24.0 para Windows y con el programa Epidat versión 3.1. Aquellos valores de p <0,05 han sido considerados estadísticamente significativos.
RESULTADOS
De la población total analizada (n = 591), se obtuvieron 59 test de antígeno positivos (10%) y 89 PCR positivas (15%), cuando la prevalencia de enfermedad COVID-19 en la población de Castilla y León era de un 10%.
Estudio de pacientes sintomáticos
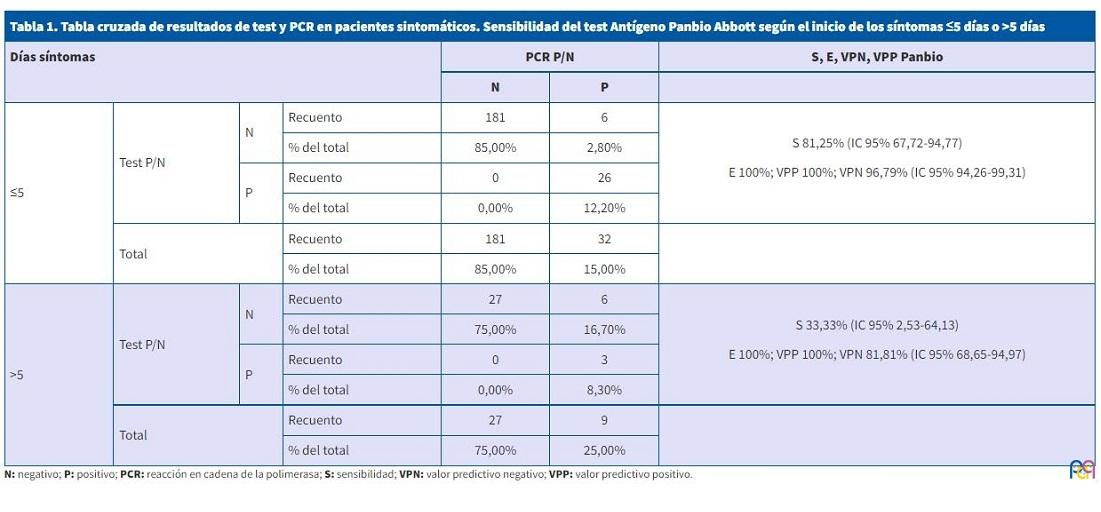
Se analizaron 249 pacientes con síntomas compatibles con COVID-19. La S y E global en este grupo con su intervalo de confianza (IC) fueron: S = 68% (IC 95%: 53,28-83,08), E = 100%. Sin embargo, cuando analizamos los pacientes con síntomas de comienzo en los cinco días previos al test (n = 213), S = 81% (IC 95%: 66,16-96,34) y E = 100% y en aquellos con más de cinco días de evolución de síntomas (n = 36) la S baja a 33% (IC 95%: 0,00-69,69), manteniendo una E de 100% (Tabla 1).
| Tabla 1. Tabla cruzada de resultados de test y PCR en pacientes sintomáticos. Sensibilidad del test Antígeno Panbio Abbott según el inicio de los síntomas ≤5 días o >5 días | ||||||
|---|---|---|---|---|---|---|
| Días síntomas | PCR P/N | S, E, VPN, VPP Panbio | ||||
| N | P | |||||
| ≤5 | Test P/N | N | Recuento | 181 | 6 |
S 81,25% (IC 95% 67,72-94,77) E 100%; VPP 100%; VPN 96,79% (IC 95% 94,26-99,31) |
| % del total | 85,00% | 2,80% | ||||
| P | Recuento | 0 | 26 | |||
| % del total | 0,00% | 12,20% | ||||
| Total | Recuento | 181 | 32 | |||
| % del total | 85,00% | 15,00% | ||||
| >5 | Test P/N | N | Recuento | 27 | 6 |
S 33,33% (IC 95% 2,53-64,13) E 100%; VPP 100%; VPN 81,81% (IC 95% 68,65-94,97) |
| % del total | 75,00% | 16,70% | ||||
| P | Recuento | 0 | 3 | |||
| % del total | 0,00% | 8,30% | ||||
| Total | Recuento | 27 | 9 | |||
| % del total | 75,00% | 25,00% | ||||
Estudio de contactos
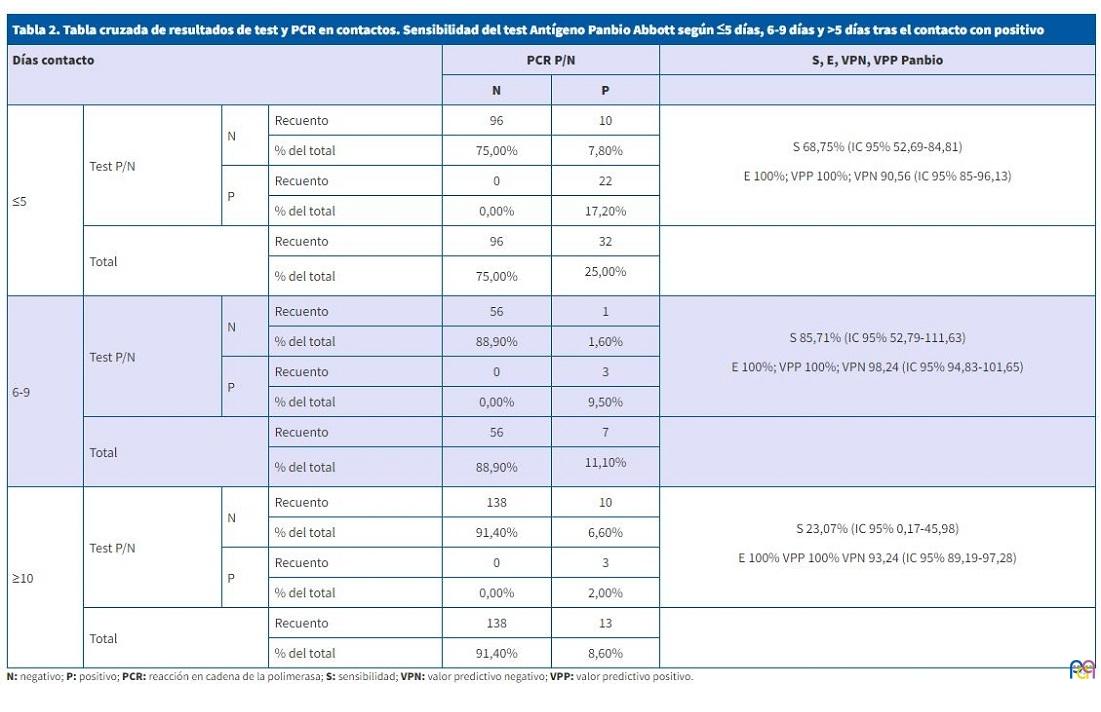
En cuanto al estudio en contactos (n = 342), la S global del test de antígeno es de 60% (IC 95%: 46,40-75,16); E = 100%, mientras que si analizamos esta entre el 6.º y 9.º día desde el último contacto con positivo sube a S = 85% (IC 95%: 52,65-100,00), E = 100% y dentro de los 5 primeros días es de S = 68% (IC 95%: 51,13-86,37); E = 100% (Tabla 2).
| Tabla 2. Tabla cruzada de resultados de test y PCR en contactos. Sensibilidad del test Antígeno Panbio Abbott según ≤5 días, 6-9 días y >5 días tras el contacto con positivo | ||||||
|---|---|---|---|---|---|---|
| Días contacto | PCR P/N | S, E, VPN, VPP Panbio | ||||
| N | P | |||||
| ≤5 | Test P/N | N | Recuento | 96 | 10 |
S 68,75% (IC 95% 52,69-84,81) E 100%; VPP 100%; VPN 90,56 (IC 95% 85-96,13) |
| % del total | 75,00% | 7,80% | ||||
| P | Recuento | 0 | 22 | |||
| % del total | 0,00% | 17,20% | ||||
| Total | Recuento | 96 | 32 | |||
| % del total | 75,00% | 25,00%
|
||||
| 6-9 | Test P/N | N | Recuento | 56 | 1 |
S 85,71% (IC 95% 52,79-111,63) E 100%; VPP 100%; VPN 98,24 (IC 95% 94,83-101,65) |
| % del total | 88,90% | 1,60% | ||||
| P | Recuento | 0 | 3 | |||
| % del total | 0,00% | 9,50% | ||||
| Total | Recuento | 56 | 7 | |||
| % del total | 88,90% | 11,10%
|
||||
| ≥10 | Test P/N | N | Recuento | 138 | 10 |
S 23,07% (IC 95% 0,17-45,98) E 100% VPP 100% VPN 93,24 (IC 95% 89,19-97,28) |
| % del total | 91,40% | 6,60% | ||||
| P | Recuento | 0 | 3 | |||
| % del total | 0,00% | 2,00% | ||||
| Total | Recuento | 138 | 13 | |||
| % del total | 91,40% | 8,60% | ||||
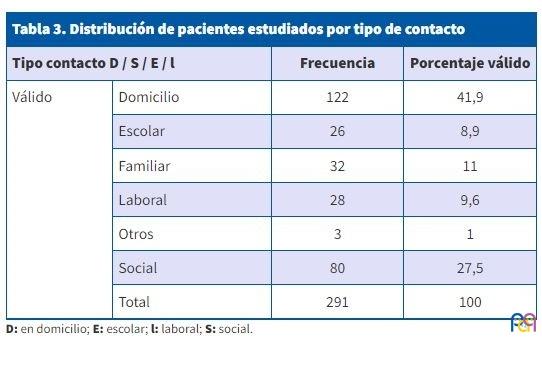
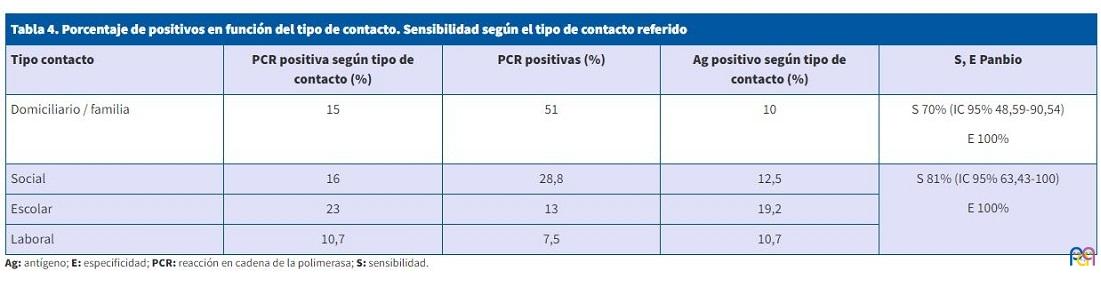
El mayor porcentaje de los contactos estudiados correspondían a exposiciones en ámbito domiciliario (n = 41,9%) seguido de otro tipo de contacto social (n = 27,5%) (Tabla 3). La S del test en los casos de contactos del ámbito familiar y domiciliario resultó ser del 70% (IC 95%: 48,59-90,54), E = 100% (Tabla 4).
| Tabla 3. Distribución de pacientes estudiados por tipo de contacto | |||
|---|---|---|---|
| Tipo contacto D / S / E / l | Frecuencia | Porcentaje válido | |
| Válido | Domicilio | 122 | 41,9 |
| Escolar | 26 | 8,9 | |
| Familiar | 32 | 11 | |
| Laboral | 28 | 9,6 | |
| Otros | 3 | 1 | |
| Social | 80 | 27,5 | |
| Total | 291 | 100 | |
| Tabla 4. Porcentaje de positivos en función del tipo de contacto. Sensibilidad según el tipo de contacto referido | ||||
|---|---|---|---|---|
| Tipo contacto | PCR positiva según tipo de contacto (%) | PCR positivas (%) | Ag positivo según tipo de contacto (%) | S, E Panbio |
| Domiciliario / familia | 15 | 51 | 10 |
S 70% (IC 95% 48,59-90,54) E 100% |
| Social | 16 | 28,8 | 12,5 |
S 81% (IC 95% 63,43-100) E 100% |
| Escolar | 23 | 13 | 19,2 | |
| Laboral | 10,7 | 7,5 | 10,7 | |
Estudio en menores de 14 años
De la muestra total (n = 591), 222 eran menores de 14 años con una media de edad x = 6,69 (DE 3,9) años, 54,5% mujeres, 122 sintomáticos y 100 contactos.
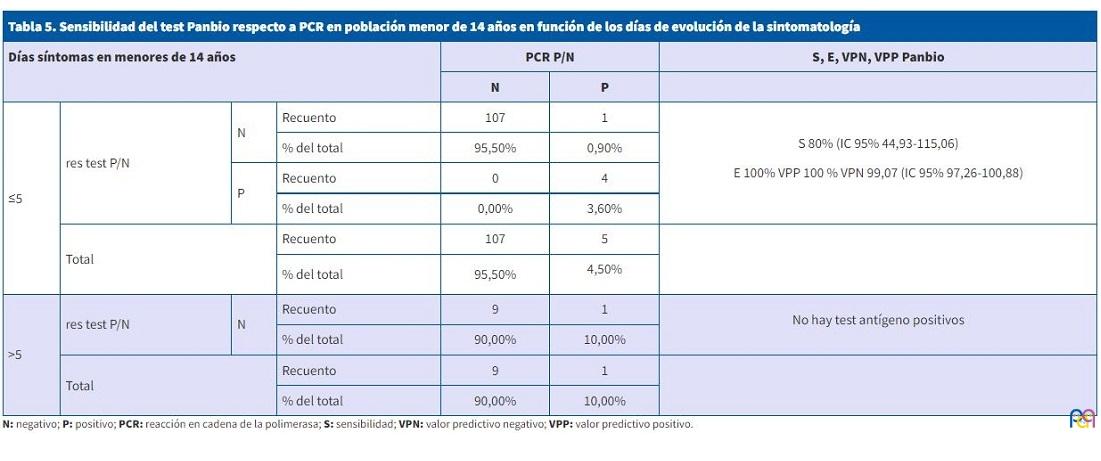
La S del test de antígeno Panbio en menores de 14 años, en los cinco primeros días de síntomas, es de 80% (IC 95%: 34,94-100), E 100%. Más allá de los cinco días, solo hay un niño con PCR positiva de 10 analizados cuyo resultado del test es negativo (Tabla 5).
| Tabla 5. Sensibilidad del test Panbio respecto a PCR en población menor de 14 años en función de los días de evolución de la sintomatología | ||||||
|---|---|---|---|---|---|---|
| Días síntomas en menores de 14 años | PCR P/N | S, E, VPN, VPP Panbio | ||||
| N | P | |||||
| ≤5 | res test P/N | N | Recuento | 107 | 1 |
S 80% (IC 95% 44,93-115,06) E 100% VPP 100 % VPN 99,07 (IC 95% 97,26-100,88) |
| % del total | 95,50% | 0,90% | ||||
| P | Recuento | 0 | 4 | |||
| % del total | 0,00% | 3,60% | ||||
| Total | Recuento | 107 | 5 | |||
| % del total | 95,50% | 4,50%
|
||||
| >5 | res test P/N | N | Recuento | 9 | 1 |
No hay test antígeno positivos |
| % del total | 90,00% | 10,00% | ||||
| Total | Recuento | 9 | 1 | |||
| % del total | 90,00% | 10,00% | ||||
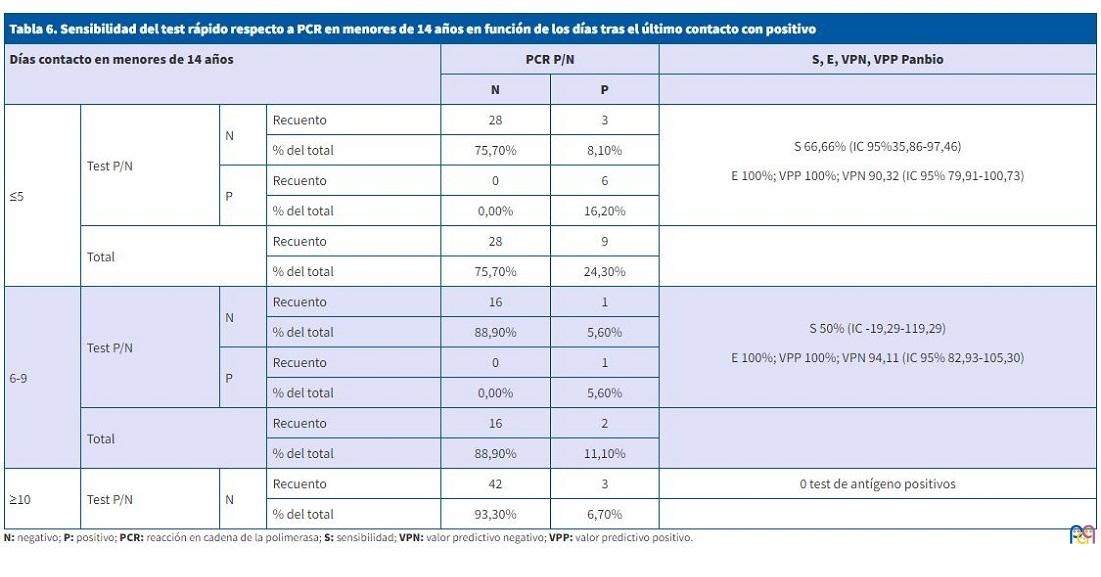
La S del test en estudio de contactos, en niños, los 5 primeros días tras el último contacto (37%) fue del 66% (IC 95%: 30,3-100) E 100%. En los contactos entre el 6.º al 9.º día (17%) bajó al 50% E 100% y más allá de 10 días (45%) el test de antígeno no detectó ninguno de los 3 positivos que detecta la PCR (Tabla 6).
| Tabla 6. Sensibilidad del test rápido respecto a PCR en menores de 14 años en función de los días tras el último contacto con positivo | ||||||
|---|---|---|---|---|---|---|
| Días contacto en menores de 14 años | PCR P/N | S, E, VPN, VPP Panbio | ||||
| N | P | |||||
| ≤5 | Test P/N | N | Recuento | 28 | 3 |
S 66,66% (IC 955,86-97,46) E 100%; VPP 100%; VPN 90,32 (IC 95% 79,91-100,73) |
| % del total | 75,70% | 8,10% | ||||
| P | Recuento | 0 | 6 | |||
| % del total | 0,00% | 16,20% | ||||
| Total | Recuento | 28 | 9 | |||
| % del total | 75,70% | 24,30% | ||||
| 6-9 | Test P/N | N | Recuento | 16 | 1 |
S 50% (IC -19,29-119,29) E 100%; VPP 100%; VPN 94,11 (IC 95% 82,93-105,30) |
| % del total | 88,90% | 5,60% | ||||
| P | Recuento | 0 | 1 | |||
| % del total | 0,00% | 5,60% | ||||
| Total | Recuento | 16 | 2 | |||
| % del total | 88,90% | 11,10% | ||||
| ≥10 | Test P/N | N | Recuento | 42 | 3 | 0 test de antígeno positivos |
| % del total | 93,30% | 6,70% | ||||
Un 44,2% de los contagios en niños fueron en el ámbito domiciliario y un 30% en reuniones sociales.
DISCUSIÓN
El empleo de las TDR ya generalizadas en nuestro entorno supone una oportunidad a nuestro alcance para contener la propagación del virus. Los resultados de nuestro estudio en Castilla y León sobre la S del antígeno rápido Panbio COVID-19 en torno a un 81% en sintomáticos coinciden con otros trabajos a nivel nacional aconsejando su empleo durante los primeros cinco días tras el inicio de los síntomas2,5,6.
Hasta la fecha de realización de este estudio, la mayoría de los trabajos se habían realizado en pacientes hospitalizados o atendidos en servicios de urgencias7-9, donde la tasa de positividad era mayor. Sin embargo, los pediatras de atención primaria que lo diseñamos creímos que es en nuestro nivel asistencial donde una TDR puede ser más útil si es eficaz y eficiente.
La S del test Panbio COVID-19 en nuestro estudio de contactos asintomáticos es del 68% en los primeros cinco días tras el último contacto, menor a otros estudios10. Sin embargo, sorprende que entre el 6.º y 9.º día sube a un 85%, que podría estar relacionado con una replicación viral más alta en esos días. De hecho, Gremmels11 y Van der Moeren12 demuestran una correlación negativa entre la carga viral y los ciclos de PCR necesarios para la detección del virus, lo que podría explicar que a partir del décimo día apenas se detectan antígenos positivos mientras la PCR es positiva. Albert y Torres13 y Pekosz14 observan que cuando el test rápido es negativo, el virus SARS-CoV-2 tampoco crece en medio de cultivo específico. Esto explicaría que, a pesar de la baja sensibilidad del test a partir del décimo día (S 65%) y coincidiendo con el estudio de una segunda PCR en contactos asintomáticos, los falsos negativos quizás no posean una carga viral suficiente y seamos capaces de frenar la propagación detectando solo aquellos realmente contagiosos.
En pacientes diagnosticados previamente de COVID-19, parece que ningún estudio detectó virus con capacidad para crecer en medio de cultivo después del día 9 de la enfermedad, a pesar de las cargas virales persistentemente altas15. De hecho, parece que aquellos individuos positivos pero asintomáticos tienen una eliminación viral más rápida, lo que supone un periodo infeccioso más corto. En este sentido, deberíamos plantearnos si fuera necesario realizar un test de antígeno a aquellos positivos tras los 10 días de aislamiento para asegurarnos de que no contagian al alta. Así, podría sustituir el test rápido antigénico a la PCR que de rutina se solicita al personal de residencias y sanitarios o profesores, previa a incorporarse al trabajo.
En cuanto al tipo de contacto, en nuestro trabajo la mitad de los asintomáticos positivos derivaban del ámbito familiar, siendo la mayor fuente de contagios seguido del ámbito social y menos del escolar (13%) como refieren otros16,17. La edad media de los contactos escolares fue de 16 meses, por lo que parece que podría corresponder con guarderías y no tanto con colegios.
En niños y según nuestros resultados, parece útil la realización del test en sintomáticos durante los primeros cinco días de evolución de la enfermedad (S = 80%). En cuanto al estudio de contactos, habría que valorar si la sensibilidad del 66% de los primeros cinco días tras el último contacto con positivo permite usar el test con la premisa de que tienen menos carga viral18, sin querer decir con ello que no contagien. Sin embargo, podría explicar menor contagiosidad en niños sin restar importancia a las medidas de seguridad que se han llevado a cabo en los colegios.
Sería interesante diferenciar dentro del mismo estudio los contactos asintomáticos de los que ya han comenzado con síntomas que en un principio pueden pasar desapercibidos, así como analizar los resultados en función de la prevalencia de la enfermedad en cada área de salud donde puede influir en la cantidad de test solicitados con más o menos síntomas o tras consultas diferidas en el tiempo por mayor presión asistencial.
A lo largo de las diferentes olas de pandemia, hemos aprendido que cuando la incidencia ha sido menor, hemos recurrido a test más sensible como la PCR para intentar no perder casos.
En un futuro próximo se deberían definir mejor los síntomas más frecuentes en positivos con base en los datos recogidos por los rastreadores en las guías asistenciales. Por supuesto, el análisis de marcadores inflamatorios en la respuesta inmune tanto en enfermos, contactos asintomáticos e inmunodeprimidos y en función de los días de evolución podría dar explicación a la pobre expresividad de la enfermedad COVID-19 en niños o la susceptibilidad de aquellos que desarrollan un síndrome inflamatorio multisistémico poscovid.
CONCLUSIONES
El test rápido de antígeno SARS-CoV-2 puede ser útil para detectar sintomáticos positivos los primeros cinco días tras el inicio de los síntomas, tanto en adultos como en niños. Los primeros cinco y hasta diez días tras el contacto podría ser útil en adultos asintomáticos.
El test es útil para detectar contactos familiares domiciliarios, que son los más frecuentes.
La disminución de la sensibilidad del test respecto a la PCR a partir del décimo día debería interpretarse en función de los estudios que analizan la correlación con cargas virales y capacidad de infección.
ABREVIATURAS
DE: desviación estándar · E: especificidad · IC: intervalo de confianza · PCR: reacción en cadena de la polimerasa · S: sensibilidad · TDR: técnicas de diagnóstico rápido.
CONFLICTOS DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
BIBLIOGRAFÍA
- Harrington A, Cox B, Snowdon J, Bakst J, Ley E, Grajales P, et al. Comparison of Abbott ID Now and Abbott m2000 methods for the detection of SARS-CoV-2 from nasopharyngeal and nasal swabs from symptomatic patients. J Clin Microbiol. 2020;58:e00798.
- Porte l, Legarraga P, Vollrath V, Aguilera X, Munita JM, Araos R, et al. Evaluation of a novel antigen-based rapid detection test for the diagnosis of SARS-CoV-2 in respiratory samples. Int J Infect Dis. 2020;99:328-33.
- Calderaro A, De Conto F, Buttrini M, Piccolo G, Montecchini S, Maccari C, et al. Human respiratory viruses, including SARS-CoV-2, circulating in the winter season 2019-2020 in Parma, Northern Italy. Int J Infect Dis. 2021;102:79-84.
- CDC COVID-19 Response Team, CDC COVID-19 Response Team, Bialek S, Gierke R, Hughes M, McNamara LA, et al. Coronavirus Disease 2019 in Children - United States, February 12-April 2, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:422-6.
- Candel FJ, Barreiro P, San Román J, Abanades JC, Barba R, Barberán J, et al. Recommendations for use of antigenic tests in the diagnosis of acute SARS-CoV-2 infection in the second pandemic wave: attitude in different clinical settings. Rev Esp Quimioter. 2020;33:466-84.
- Linares M, Pérez Tanoira R, Romanyk J, Pérez García F, Gómez-Herruz P, Arroyo T, et al. Panbio antigen rapid test is reliable to diagnose SARS-CoV-2 infection in the first 7 days after the onset of symptoms. J Clin Virol. 2020;133:104659.
- Young S, Taylor SN, Cammarata CL, Varnado KG, Roger-Dalbert C, Montano A, et al. Clinical Evaluation of BD Veritor SARS-CoV-2 Point-of-Care Test Performance Compared to PCR-Based Testing and versus the Sofia 2 SARS Antigen Point-of-Care Test. J Clin Microbiol. 2020;59:e02338-20.
- Scohy A, Anantharajah A, Bodéus M, Kabamba-Mukadi B, Verroken A, Rodriguez-Villalobos H. Low performance of rapid antigen detection test as frontline testing for COVID-19 diagnosis. J Clin Virol. 2020;129:104455.
- Lambert-Niclot S, Cuffel A, Le Pape S, Vauloup-Fellous C, Morand-Joubert l, Roque-Afonso A-M, et al. Evaluation of a Rapid Diagnostic Assay for Detection of SARS-CoV-2 Antigen in Nasopharyngeal Swabs. J Clin Microbiol. 2020;58:e00977.
- Alemany A, Baro B, Ouchi D, Ubals M, Corbacho-Monné M, Vergara-Alert J, et al. Analytical and Clinical Performance of the Panbio COVID-19 Antigen-Detecting Rapid Diagnostic Test. J Infect. 2021;82:186-230.
- Gremmels H, Winkel BMF, Schuurman R, Rosingh A, Rigter NAM, Rodriguez O, et al. Real-life validation of the Panbio COVID-19 Antigen Rapid Test (Abbott) in community-dwelling subjects with symptoms of potential SARS-CoV-2 infection. Eclinical Med. 2021;31:100677.
- Van der Moeren N, Zwart VF, Lodder EB, Van den Bijllaardt W, Van Esch HRJM, Stohr JJJM, et al. Evaluation of the test accuracy of a SARS-CoV-2 rapid antigen test in symptomatic community dwelling individuals in the Netherlands. PLos One. 2021;16:e0250886.
- Albert E, Torres I, Bueno F, Huntley D, Molla E, Fernández-Fuentes MÁ, et al. Field evaluation of a rapid antigen test (Panbio COVID-19 Ag Rapid Test Device) for the diagnosis of COVID-19 in primary healthcare centers. Clin Microbiol Infect. 2021;27:472.e7-472.e10.
- Pekosz A, Cooper CK, Parvu V, Li M, Andrews JC, Manabe YC, et al. Antigen-based testing but not real-time PCR correlates with SARS-CoV-2 virus culture. Clin Infect Dis. 2021;73(9):e2861-e2866.
- Cevik M, Tate M, Lloyd O, Maraolo AE, Schafers J, Ho A. SARS-CoV-2, SARS-CoV, and MERS-CoV viral load dynamics, duration of viral shedding, and infectiousness: a systematic review and meta-analysis. The Lancet Microbe. 2021;2:e13-e22.
- Melé M, Henares D, Pino R, Asenjo S, Matamoros R, Fumadó V, et al. Low impact of SARS-CoV-2 infection among paediatric acute respiratory disease hospitalizations. J Infect. 2021;82:414-51.
- Ríos-Barnés M, Lanaspa M, Noguera-Julian A, Baleta l, De Sevilla MF, Ferri D, et al. The Spectrum of COVID-19 Disease in Adolescents. Arch Bronconeumol. 2021;57:84-5.
- Kociolek LK, Muller WJ, Yee R, Dien Bard J, Brown CA, Revell P, et al. Comparison of upper respiratory viral load distributions in asymptomatic and symptomatic children diagnosed with SARS-CoV-2 infection in pediatric hospital testing programs. J Clin Microbiol. 2020;59:e02593-20.