
Vol. 24 - Num. 94
Originales
Utilización de antibióticos en la población menor de 14 años
Juan Ríos Laordena, Carlos Marcilla Vázquezb, Ángeles Lloret Callejoc, Francisco Tejada Cifuentesc, M.ª José Tirado Peláezc
aPediatra. CS Zona VI. Gerencia de Atención Integrada de Albacete. Albacete. España.
bServicio de Pediatría. Complejo Hospitalario Universitario. Gerencia de Atención Integrada de Albacete. Albacete. España.
cFarmacéutico de Atención Primaria. Gerencia de Atención Integrada de Albacete. Albacete. España.
Cómo citar este artículo: Ríos Laorden J, Marcilla Vázquez C, Lloret Callejo A, Tejada Cifuentes F, Tirado Peláez MJ. Utilización de antibióticos en la población menor de 14 años. Rev Pediatr Aten Primaria. 2022;24:137-47.
Publicado en Internet: 15-06-2022 - Número de visitas: 21014
Resumen
Objetivo: obtener un mapa de prescripción de antibióticos por edades en procesos infecciosos, en el ámbito de la atención primaria en menores de 14 años.
Material y métodos: estudio observacional, descriptivo, de utilización de medicamentos, realizado sobre la prescripción de antibióticos. La muestra del estudio son todos los niños del área que, durante el periodo del estudio (enero de 2017 a diciembre de 2019), han recibido la prescripción de un antibiótico. Se ha calculado el valor de los indicadores descritos en el programa de optimización de uso de antibióticos.
Resultados: durante el 2017 el número total de antibióticos prescritos fue 28 030, un 12% y 14% más que en 2018 y 2019, respectivamente. En el año 2018 un 31,4% de la población estudiada recibió al menos la prescripción de un antibiótico al año, mientras que en el 2019 este valor fue 35,8%. En el caso de dos prescripciones al año, el valor fue 15,4% en 2018 y 14,4% en 2019. La prescripción del grupo de penicilinas sensibles a betalactamasas ha pasado de 1,7% en 2017 a 7,7% en 2019, mientras que en el grupo de los macrólidos ha sido a la inversa, pasando de 19,6% en 2017 a 14,9% en 2019.
Conclusión: en este estudio se obtienen por primera vez indicadores cuantitativos y cualitativos de uso de antibióticos en edad pediátrica, en patología infecciosa prevalente. Se confirma el elevado consumo de antibióticos, especialmente en el grupo de 0-4 años, así como la mala selección de determinados grupos de antibióticos, como macrólidos y cefalosporinas, en patologías en las que no son de primera elección.
Palabras clave
● Adecuación ● Antibióticos ● Indicadores ● Población pediátricaINTRODUCCIÓN
En la población pediátrica española se produce un alto consumo de antibióticos de uso sistémico a nivel comunitario1. De hecho, en 2019 ocupábamos el quinto lugar en mayor consumo de antibióticos entre los países europeos, teniendo en cuenta solo los datos relativos a consumo obtenidos con receta oficial financiada por el Sistema Nacional de Salud, dejando fuera otras tres fuentes importantes como la automedicación, la prescripción privada y el consumo hospitalario2. Este excesivo consumo no es exclusivo de ningún grupo etario, siendo el consumo en la población pediátrica también elevado3. Datos recientes del European Centre for disease Prevention and control (ECDC) afirman que, según los datos disponibles de los sistemas de vigilancia españoles, la situación de microorganismos resistentes a antibióticos en España plantea una amenaza de salud pública importante para el país, siendo muy elevados los niveles actuales de Staphylococcus aureus resistente a meticilina, enterobacterias productoras de betalactamasas de espectro extendido4,5 y Acinetobacter baumannii, estando por encima de la media de la Unión Europea (UE). Además, el rápido aumento en los últimos cinco años de enterobacterias productoras de carbapenemasas representa una nueva amenaza para la seguridad de los pacientes en todos los ámbitos de la atención sanitaria. Todo ello, unido al elevado consumo de antibióticos, no representa las condiciones óptimas para el control de estos organismos multirresistentes6.
El aumento de los niveles de resistencias bacterianas en los últimos años hace inaplazable la implantación de actividades programadas, dirigidas a la prevención y control de dichas resistencias. Estos programas se deben encaminar fundamentalmente a prevenir la transmisión de infecciones y a fomentar un uso adecuado de los antimicrobianos7.
En diciembre de 2014 se aprobó la puesta en marcha de Programas de Optimización de Uso de Antibióticos (PROA) en el ámbito hospitalario y de Atención Primaria (AP), a través del Plan Nacional frente a la resistencia a los antibióticos (PRAN), que tuvo cinco años de vigencia (2014-2018). Posteriormente, en el año 2019, se ha aprobado el PRAN para los años 2019-2021, que continúa avanzando sobre la base construida con el trabajo desarrollado entre 2014 y 2018, con el objetivo general de reducir o, al menos, frenar el crecimiento de la resistencia a los antibióticos y su impacto en la salud de toda la población. Para ello, se plantean dos estrategias generales: reducir el consumo de antibióticos y disminuir la necesidad de utilizar antibióticos en medicina humana y veterinaria8. La optimización de la prescripción de los antibióticos debe ser entendida como un proceso de cambio de hábitos de prescripción, cuyos objetivos finales son obtener los mejores resultados clínicos en pacientes con infecciones y minimizar los efectos adversos de los antibióticos, fundamentalmente la aparición, el desarrollo y la diseminación de resistencias a los antimicrobianos.
El proceso de toma de decisiones para la indicación de antibióticos está influenciado por condicionantes internos y externos, de tal manera que en los distintos ámbitos asistenciales es conocido que el 35-50% de los tratamientos antibióticos es optimizable9.
En el PRAN de la Agencia Española del Medicamento y Productos Sanitarios (AEMPS), en su línea estratégica I, se establece la vigilancia del consumo y de la resistencia a los antibióticos. En concreto, indica la necesidad de monitorizar el consumo de antibióticos como medida indispensable para conocer la presión que el uso de los mismos ejerce en la aparición de resistencias, estableciéndose dos acciones: mejorar la obtención de datos del consumo de antibióticos en la comunidad y en los hospitales, asegurar la explotación y análisis de los datos a nivel local, regional y nacional, y el retorno de información, así como facilitar la accesibilidad a la información a través de una plataforma pública (mapas de consumo) donde puedan consultarse datos nacionales y en la que, a día de hoy, estos datos no se muestran estratificados por edades ni grupos de población10.
Del mismo modo, en la línea estratégica II del PRAN, se establecen como objetivos prioritarios de mejora en pediatría de AP disminuir la cantidad global de prescripción, disminuir la prescripción en procesos no bacterianos y mejorar la adecuación en procesos concretos11.
A nivel europeo, los países del sur son más consumidores de antibióticos que los del norte, llegando a triplicar a los que menos consumen (Países Bajos y países nórdicos). Este patrón norte-sur es patente tanto en consumo de antibióticos como en resistencias a los mismos, siendo más evidente en AP y observando un consumo más homogéneo entre los distintos países a nivel hospitalario12. La comparación del consumo antibiótico en edad pediátrica entre diferentes países europeos pone de manifiesto la amplia variabilidad de patrones de prescripción de antibióticos, sugiriendo que una gran parte de los antimicrobianos se utilizan de forma inapropiada, fundamentalmente en el tratamiento de infecciones respiratorias13-15.
Desde hace años, los sistemas de salud vienen monitorizando la prescripción de antibióticos de los profesionales médicos, especialmente en AP. Esta monitorización en nuestro sistema de salud ha estado basada principalmente en el cálculo de la dosis diaria definida por 1000 habitantes/día (DHD) de antiinfecciosos de uso sistémico, cefalosporinas y macrólidos, y de antiinfecciosos sistémicos de segunda línea (fluorquinolonas y cefalosporinas de 3.ª y 4.ª generación). En el Plan Nacional se han establecido indicadores de población total y de pediatría, aunque los datos publicados de los mismos son generales y no estratificados por edades16.
El objetivo de este trabajo es realizar un análisis del consumo y de la adecuación de la prescripción de antibióticos en la población pediátrica de la Gerencia de Atención Integrada de Albacete, en los procesos infecciosos más prevalentes, y proponer un catálogo de indicadores generales y específicos de uso de antibióticos para pediatría. Además, se van a presentar los resultados estratificados por grupos de población (estratificación por edades).
Asimismo, y siguiendo las recomendaciones del PRAN, se está realizando un feedback de información-formación a los facultativos sanitarios, con la finalidad de disminuir el consumo y mejorar la utilización de los antibióticos en población pediátrica, en el contexto de un programa de optimización de uso de antimicrobianos.
MATERIAL Y MÉTODOS
Estudio observacional, descriptivo, de utilización de medicamentos, realizado sobre la prescripción de antibióticos en la población pediátrica de la Gerencia de Atención Integrada de Albacete (España), seguido de una intervención de tipo formativo realizada sobre los profesionales sanitarios del área.
La muestra del estudio está formada por todos los niños del área de ambos sexos (0-14 años), que durante el periodo del estudio (enero de 2017 a diciembre de 2019), han recibido la prescripción de al menos un antibiótico. A continuación, se describen las variables que se han recogido para la realización del estudio, obtenidas del sistema de Información de AP (Turriano) del Servicio de Salud de Castilla-La Mancha (SESCAM). Todos los datos se han codificado de forma anonimizada: día de la semana de prescripción; mes de la prescripción; sexo; diagnóstico: se utilizó la codificación del Código Internacional de Enfermedades 9.ª edición (CIE-9-MC) y de la Clasificación Internacional de AP (CIAP) (Tabla 1); antibiótico: se utilizó el Sistema de Clasificación Anatómica Terapéutica; química (ATC) del subgrupo farmacológico J01; fecha de nacimiento del paciente; centro salud.
| Tabla 1. Codificación de la patología infecciosa pediátrica. Indicadores de adecuación de la prescripción | ||
|---|---|---|
| Faringoamigdalitis aguda (FAA) | Indicadores | |
| CIE - 462 | Faringitis aguda |
% pacientes tratados con antibiótico (J01) % pacientes menores de 3 años con antibiótico (J01) % pacientes tratados con penicilinas sensibles a betalactamasas o amoxicilina (J01CE + J01CA04) % pacientes tratados con amoxicilina-clavulánico (J01CR2) % pacientes tratados con macrólidos (J01FA) % recetas amoxicilina/recetas (amoxicilina+ amoxicilina-clavulánico) (J01CA04 + J01CR2) |
| CIE - 463 | Amigdalitis aguda | |
| CIE - 034 | Amigdalitis estreptocócica | |
| CIAP - R76 | Amigdalitis | |
| CIAP - R72 | Faringoamigdalitis estreptocócica | |
| Resfriado común | Indicadores | |
| CIE - 460 | Resfriado común | % pacientes tratados con antibiótico (J01) |
| CIAP - R74 | Infección respiratoria superior | |
| Otitis media aguda (OMA) | Indicadores | |
| CIE - 381 | Otitis media aguda no supurada |
% pacientes tratados con antibiótico (J01) % pacientes tratados con amoxicilina (J01CA04) % pacientes tratados con macrólidos % pacientes tratados con amoxicilina-clavulánico % recetas amoxicilina/recetas (amoxicilina+amoxicilina-clavulánico) |
| CIE - 382 | Otitis media aguda supurada | |
| CIAP - H71 | Otitis media/miringitis aguda | |
| Bronquiolitis aguda | Indicadores | |
| CIE - 466 | Bronquitis aguda | % pacientes tratados con antibiótico (J01) |
| CIAP - R78 | Bronquitis/bronquiolitis aguda | |
| Neumonía aguda adquirida en la comunidad (NAC) | Indicadores | |
| CIE - 486 | Neumonía no especificada | % pacientes tratados con ATB (J01) |
| CIAP - R88 | Neumonía | |
| Infección del tracto urinario (ITU) | Indicadores | |
| CIE - 595 | Cistitis |
% pacientes tratados con ATB (J01) % procesos tratados con ATB (J01)
|
| CIE - 590 | Infecciones renales | |
| CIE - 599 | Otras alteraciones de la uretra y las vías urinarias | |
| CIAP - U71 | Cistitis y otras infecciones urinarias | |
| CIAP - U70 | Pielitis/pielonefritis | |
| CIAP - U99 | Otros problemas renales | |

Teniendo en cuenta que la dosificación realizada en pacientes pediátricos no está estandarizada, sino calculada en función del peso del paciente, en este estudio se ha utilizado como unidad de medida el número de días de tratamiento (DOT). Su cálculo presenta gran dificultad y variabilidad debido a la cumplimentación heterogénea de la receta médica, en la cual no queda recogido de modo fiable el apartado de la duración del tratamiento. Por ello, para obtener la DOT, nos hemos basado en la utilización teórica de cada antibiótico para cada una de las patologías prevalentes analizadas en nuestro estudio, teniendo en cuenta la duración de cada uno de ellos según las guías de consenso españolas y cómo la edad afecta a la duración en algunas de estas patologías, por ejemplo, en la otitis media aguda17,18.
Se ha realizado un análisis descriptivo de las variables, analizando tanto el consumo como la indicación del antibiótico. Se han calculado como variables de resultados todos los indicadores descritos en el PROA en AP para población pediátrica. Los indicadores de consumo se han calculado en los tres años del estudio y por tramos de población de 0 a 4 años, de 5 a 9 y de 10 a 14 años: tasa de consumo de antibióticos de uso sistémico; prevalencia de uso de antibióticos o porcentaje de población pediátrica que consume antibióticos en un año; porcentaje de consumo de penicilinas sensibles a betalactamasas en pediatría; porcentaje de consumo de amoxicilina respecto al total; porcentaje de consumo de amoxicilina/clavulánico respecto al total; porcentaje del consumo de amoxicilina sin clavulánico; porcentaje de consumo de macrólidos respecto al total y porcentaje de consumo de cefalosporinas de 3.ª generación respecto al total (Tabla 1). La adecuación de la prescripción de antibióticos se ha obtenido mediante el cálculo de todos los indicadores cualitativos, más otros de elaboración propia para aquellos diagnósticos donde el PRAN no tiene indicadores.
El estudio se ha realizado con arreglo a los principios de la Declaración de Helsinki y de la Ley Orgánica de Protección de Datos de entrada en vigor el 25 de mayo de 2018. Este estudio fue aprobado por el Comité Ético de Investigación con Medicamentos (CEIM) del área.
RESULTADOS
La población a estudio no varió mucho a lo largo de los tres años, de 38 857 niños de 0-14 años en 2017 a 38 299 en 2019. Durante el primer año del estudio (2017), el número total de antibióticos del grupo J01 prescritos en niños de 0 a 14 años fue de 28 030, un 12% y 14% más que en 2018 (25 016) y 2019 (24 557). En los tres años analizados, la prescripción fue mayor en el sexo masculino y en el tramo de edad de 0 a 4 años, disminuyendo a medida que la edad aumentaba.
Para calcular la tasa de consumo se utilizó el resultado de la DOT teórica, obtenida para cada antibiótico en cada patología. La mayor adecuación en la prescripción se refleja en el descenso de la DOT obtenida a lo largo del periodo de estudio, pasando de 8,2 en el año 2017 a 7,7 en 2018 y 7,2 en 2019 (Tabla 2).
| Tabla 2. Datos poblacionales, consumo de antibióticos y número de días de tratamiento totales y por tramos de edad | |||
|---|---|---|---|
| 2017 | 2018 | 2019 | |
| Población por tramos de edad | |||
| Población 0-4 años | 11 529 | 11 074 | 11 103 |
| Población 5-9 años | 13 493 | 13 142 | 13 150 |
| Población 10-14 años | 13 835 | 14 087 | 14 046 |
| Población 0-14 años | 38 857 | 38 303 | 38 299 |
| Prevalencia uso ATB (%) por tramos de edad en un año | |||
| ATB 0-4 años | 13 387 (116,1%) | 12 271 (110,8%) | 11 777 (106,1%) |
| ATB 5-9 años | 9266 (68,7%) | 7940 (60,4%) | 7835 (59,6%) |
| ATB 10-14 años | 5377 (38,9%) | 4805 (34,1%) | 4945 (35,2%) |
| ATB 0-14 años | 28 030 | 25 016 | 24 557 |
| DOT por tramos de edad | |||
| DOT 0 - 4 años | 8,1 | 7,5 | 7 |
| DOT 5-9 años | 8,2 | 7,9 | 7,4 |
| DOT 10-14 años | 8,4 | 8 | 7,5 |
| DOT media | 8,2 | 7,7 | 7,2 |
| N.º procesos totales | 61 534 | 61 334 | 58 818 |

La tasa de consumo encontrada en el tramo de 0-4 años fue casi el doble que en el tramo de 10-14 años en todo el periodo (Tabla 3). Con respecto a la prevalencia de uso de antibióticos, es también más elevada en los primeros cuatro años de vida, disminuyendo a lo largo del periodo de estudio, pasando de un 116,1% en 2017 a un 106,1% en el 2019. La tasa de consumo fue superior en el ámbito rural (19,1% en el año 2018 y 18,6% en 2019), frente al 10,8% y 10,7% del área urbana.
| Tabla 3. Indicadores de consumo por tramos de edad en población pediátrica en el área de Albacete. Periodo 2017-2019 | ||||
|---|---|---|---|---|
| Tramos de edad | 2017 | 2018 | 2019 | |
| Tasa de consumo de antibióticos de uso sistémico (J01), DTD en menores de 14 años | Total | 16,2 | 13,8 | 12,7 |
| 0-4 años | 25,7 | 22,4 | 20,3 | |
| 5-9 años | 15,3 | 13 | 12,1 | |
| 10-14 años | 8,9 | 7,5 | 7,2 | |
| Prevalencia de uso de ATB o porcentaje de población PED que consume ATB en un año (%) | Total | 72,1 | 65,3 | 64,1 |
| 0-4 años | 116,1 | 110,8 | 106,1 | |
| 5-9 años | 68,7 | 60,4 | 59,6 | |
| 10-14 años | 38,9 | 34,1 | 35,2 | |
| Consumo de penicilinas sensibles a betalactamasas en PED (%) | Total | 1,7 | 5,6 | 7,7 |
| 0-4 años | 3,5 | 3,1 | 5 | |
| 5-9 años | 10,9 | 8,9 | 11,7 | |
| 10-14 años | 7,6 | 7 | 8 | |
| Consumo de amoxicilina respecto al total (%) | Total | 45,7 | 45,2 | 47,2 |
| 0-4 años | 53,3 | 52,1 | 54,5 | |
| 5-9 años | 39,9 | 40,2 | 41,9 | |
| 10-14 años | 36,7 | 35,8 | 38,5 | |
| Consumo de amoxicilina/ clavulánico respecto al total (%) | Total | 24,3 | 24,6 | 23,2 |
| 0-4 años | 19,8 | 19,6 | 19,1 | |
| 5-9 años | 26,8 | 28,4 | 25,9 | |
| 10-14 años | 31,2 | 31,2 | 28,7 | |
| Porcentaje del consumo de amoxicilina sin clavulánico (%) | Total | 65,3 | 64,7 | 67,1 |
| 0-4 años | 72,9 | 72,7 | 74,1 | |
| 5-9 años | 59,8 | 58,6 | 61,8 | |
| 10-14 años | 54 | 53,4 | 57,3 | |
| Porcentaje del consumo de macrólidos respecto al total (%) | Total | 19,6 | 18,6 | 14,9 |
| 0-4 años | 19,5 | 19 | 14,4 | |
| 5-9 años | 19,1 | 17,1 | 14,3 | |
| 10-14 años | 20,6 | 19,7 | 17,1 | |
| Porcentaje del consumo de cefalosporinas de 3.ª generación respecto al total (%) | Total | 1,1 | 2,8 | 3,5 |
| 0-4 años | 1,6 | 3,1 | 3,9 | |
| 5-9 años | 1,1 | 2,6 | 3,3 | |
| 10-14 años | 0,2 | 2,4 | 2,9 | |
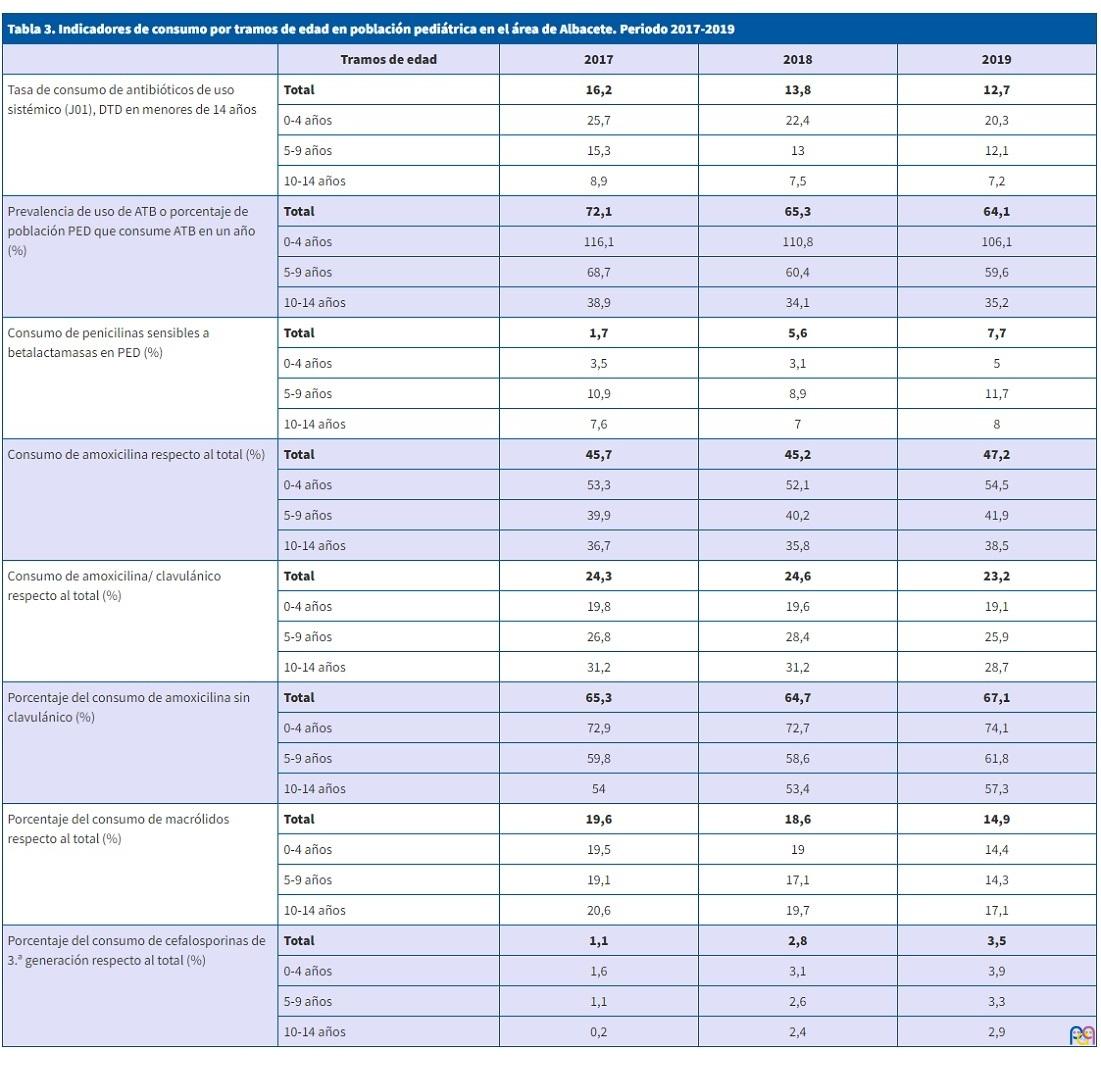
En el año 2017, un 39,4% de la población total recibió la prescripción de un antibiótico al año y un 16,6%, dos antibióticos al año, hasta el máximo de 18 prescripciones antibióticas realizadas a un paciente. En 2018, se pautó un antibiótico a un 31,4% de la población total y a un 15,4%, dos veces al año. Finalmente, en el año 2019, al 35,8% de la población total le prescribieron un antibiótico al año y al 14,4 % en dos ocasiones. En estos dos últimos años, el número máximo de prescripciones realizadas fue de 20, en ambos casos a un solo paciente.
El mayor aumento de consumo de antibióticos durante este periodo se ha dado en el grupo de las penicilinas sensibles a betalactamasas (pasando de un 1,7% en 2017, a un 5,6% en 2018 y un 7,7% en 2019), seguido por las cefalosporinas de tercera generación (1,1% en el año 2017, 2,8% en 2018 y 3,5% en 2019). Por el contrario, el mayor descenso ha estado en el indicador de consumo de macrólidos, que pasó de un 19,6% en 2017 a un 18,6% en 2018 y un descenso más marcado en 2019 hasta el 14,9%, siendo proporcional en cada tramo de edad.
En niños de 0-4 años se registraron un total de 61 534 procesos de patología infecciosa durante el año 2017 y 61 334 en el año 2018; cifra superior al total de procesos de 2019, siendo de 58 818. De estos procesos, más de un 85% corresponde a patología respiratoria, como resfriado común o faringoamigdalitis aguda (FAA).
Un 37,7% de la población pediátrica en 2017 fue tratada con un antibiótico para un proceso de FAA, descendido en los años posteriores a un 27,3% en 2018 y un 27,3% en 2019 (Tabla 4). Del total de procesos codificados como FAA, se trataron con antibióticos el 68,6% en 2017, 58,6% en 2018 y 57,4% en el año 2019. En menores de tres años la cifra de población tratada fue disminuyendo a lo largo del estudio (41,3% en 2017, 33% en 2018 y 23,8% en 2019). Respecto a la selección del antibiótico para el tratamiento de FAA, se produjo un aumento del tratamiento con penicilinas sensibles a betalactamasas (de 60,3% en 2017 y 60,9 % en 2018 a 66,8% en 2019). Por el contrario, los procesos de FAA tratados con macrólidos mostraron un descenso importante (de 20,7% en 2017 y 19,6% en el año 2018 al 14,3% del año 2019). Menor fue la disminución de los procesos tratados con amoxicilina-clavulánico, que pasaron de un 12,5% en 2017 a un 10,4 % en el año 2018 y un 9,5% en 2019.
| Tabla 4. Indicadores de adecuación en los procesos infecciosos más prevalentes en población pediátrica en el área de Albacete. Periodo 2017-2019 | ||||
|---|---|---|---|---|
| Proceso Infeccioso | Indicador | Valor 2017 | Valor 2018 | Valor 2019 |
| Faringoamigdalitis aguda (FAA) | % pacientes tratados con antibiótico (J01) | 37,6% | 27,3% | 27,3% |
| % pacientes menores de 3 años con antibiótico (J01) | 41,3% | 33% | 23,8% | |
| % pacientes tratados con penicilinas sensibles a betalactamasas o amoxicilina (J01CE + J01CA04) | 60,3% | 60,9% | 66,8% | |
| % pacientes tratados con amoxicilina-clavulánico (J01CR2) | 18,2% | 17,7% | 16,6% | |
| % pacientes tratados con macrólidos (J01FA) | 14,2% | 11,5% | 8,2% | |
| % recetas amoxicilina/recetas (amoxicilina+ amoxicilina-clavulánico) (J01CA04 + J01CR2) | 73,1% | 73,1% | 74,9% | |
| Resfriado común | % pacientes tratados con antibiótico (J01) | 8,6% | 5,5% | 4,1% |
| Otitis media aguda (OMA) | % pacientes tratados con antibiótico (J01) | 15,7% | 15,3% | 15,1% |
| % pacientes tratados con amoxicilina (J01CA04) | 42,2% | 44,9% | 45,7% | |
| % pacientes tratados con macrólidos | 8,1% | 5,5% | 4,9% | |
| % pacientes tratados con amoxicilina-clavulánico | 19,7% | 22,9% | 21,7% | |
| % recetas amoxicilina/recetas (amoxicilina+amoxicilina-clavulánico) | 68,2% | 66,3% | 67,8% | |
| Bronquiolitis aguda | % pacientes tratados con antibiótico (J01) | 3,1% | 2,6% | 2,2% |
| Neumonía aguda adquirida en la comunidad (NAC) | % pacientes tratados con ATB (J01) | 0,3% | 0,8% | 0,8% |
| Infección del tracto urinario (ITU) | % pacientes tratados con ATB (J01) | 0,7% | 1,7% | 1,7% |
| % procesos tratados con ATB (J01) | 31% | 80,2% | 69,8% | |
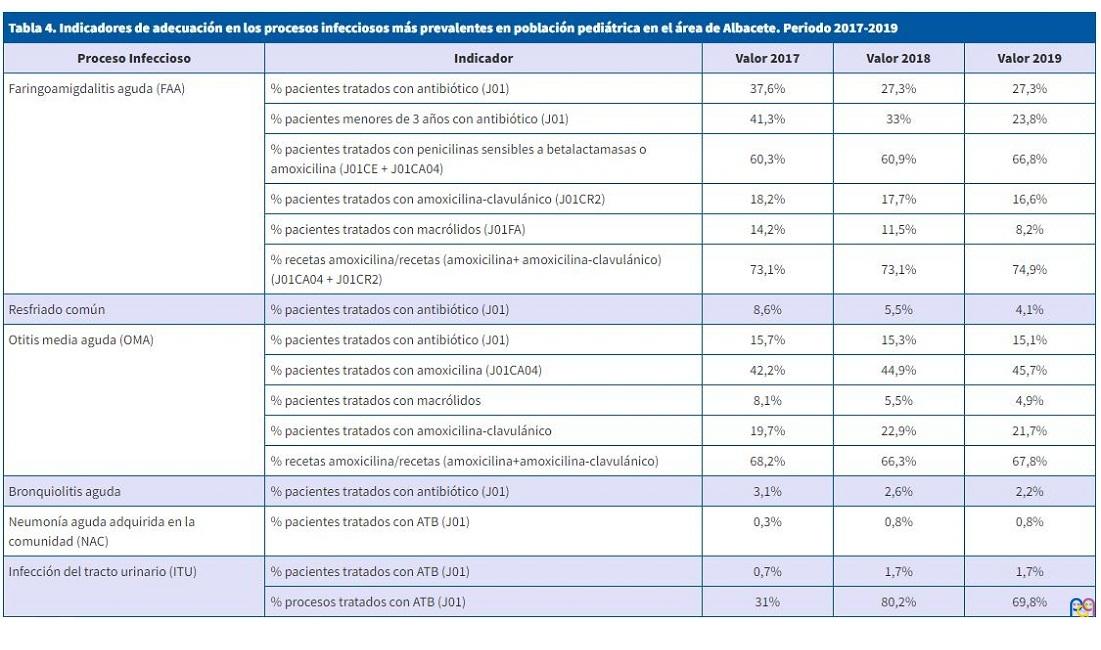
En el diagnóstico de resfriado común hubo una disminución de pacientes tratados con antibióticos: 8,6% en 2017, 5,5% en 2018 y 4,1% en 2019. Mucho más marcado fue el descenso en menores de 3 años, pasando del 16,6% en el año 2017 a un 13,8% en 2018 y un 9% en 2019.
Respecto a la otitis media aguda (OMA), la población pediátrica tratada con antibióticos fue muy similar a lo largo del estudio: 15,7% en 2017, 15,2% en 2018 y 15,1% en 2019. Del total de procesos codificados como OMA, se trataron con antibióticos aproximadamente las tres cuartas partes de los mismos: 73,1% en 2017, 76,8% en 2018 y 76,6 % en 2019. Casi la mitad de los casos de OMA fueron tratados con amoxicilina (42,2% en 2017, 44,9 % en 2018 y 45,7% en 2019). Un porcentaje no desdeñable (19,7% en 2017, 22,9 % en 2018 y 21,7% en 2019) se trataron con amoxicilina-ácido clavulánico, siendo también significativos los casos tratados con macrólidos (8,1% en 2017, con un descenso significativo en los años posteriores a 5,5% en 2018 y 4,9% en 2019).
DISCUSIÓN
La población pediátrica de nuestro estudio ha permanecido estable a lo largo de los tres años, así como la tendencia en la reducción anual del consumo de antibióticos. Se han obtenido por primera vez datos cuantitativos estratificados en nuestro ámbito, clasificándose por grupos de edad de 0 a 4, 5 a 9 y 10 a 14 años, a diferencia de lo que aparece en la mayoría de los estudios que publican datos referentes a población global19-21, al igual que en el PRAN8.
La utilización de la DOT para calcular las tasas de consumo globales ha permitido que los resultados obtenidos reflejaran mejor la selección de los diferentes grupos de antibióticos. Las tasas de consumo de nuestro estudio han disminuido progresivamente (2017-2019), si bien han sido más elevadas en los primeros años de vida, al contrario de lo que debería ocurrir si consideramos que en este grupo de edad el número de infecciones víricas es mayor y, por tanto, un tratamiento antibiótico estaría menos frecuentemente indicado.
A medida que avanza el estudio se ha constatado una mayor utilización de penicilinas sensibles a betalactamasas y un descenso en el empleo de macrólidos, si bien estos resultados siguen siendo insuficientes, pues las penicilinas sensibles a betalactamasas son el tratamiento de elección para la FAA y deberíamos acercarnos a un uso de amoxicilina-ácido clavulánico y de macrólidos exclusivamente ceñido a criterios de consenso 22.
Uno de los principales puntos de inadecuación en la prescripción de antibióticos es la sobreutilización de macrólidos: demasiado elevada respecto a las recomendaciones nacionales e internacionales para este grupo de antibióticos, quizás motivada por la falsa seguridad que les atribuye su amplio espectro y por su facilidad de administración (bajo número de dosis, volúmenes y duración). Se han obtenido en nuestro estudio consumos cercanos al 15% para este subgrupo, con una distribución similar en los tres grupos de edad estudiados. Si consideramos, por ejemplo, el caso de la FAA, los procesos tratados con macrólidos fueron un 20,7% en 2017, 19,6% en el año 2018 y 14,3% en 2019, cifras muy superiores a las que se deberían obtener, considerando que en esta patología la indicación de macrólidos se limita a pacientes con alergia anafiláctica a penicilina, y la prevalencia de esta en niños es de 1,7-5,2%23.
La obtención de indicadores específicos de consumo ligados a diagnósticos en cualquier grupo de población es compleja, quizás más en pediatría, donde el déficit en el registro o la complejidad en la codificación pueden alterar los resultados. Sin embargo, la automatización en los archivos de registros de las historias clínicas electrónicas está siendo decisiva y favorecedora24. En nuestro estudio se ha logrado obtener, por primera vez para población pediátrica, todos los indicadores específicos, utilizando para ello unas poblaciones, tanto de pacientes como de prescriptores, muy estables.
Si analizamos estos indicadores, en el tratamiento del segundo proceso infeccioso más prevalente en población pediátrica, la FAA, se ha producido una disminución de los pacientes totales tratados con antibióticos (sobre todo en los menores de 3 años) y un aumento en la prescripción de penicilinas sensibles a betalactamasas, lo cual refleja una mayor adecuación en la selección del antibiótico17. En esta patología también se observó una disminución en la prescripción de macrólidos (indicado principalmente en pacientes alérgicos a penicilinas) y de amoxicilina-clavulánico, indicado en niños con FAA por estreptococo betahemolítico del grupo A (EBHGA) que hubieran presentado un fracaso terapéutico o un estado de portador de este germen17.
Los datos de nuestro estudio muestran que se consolida la tendencia a no prescribir antibióticos en proceso víricos no complicados, como el resfriado común, persistiendo todavía un 4% de niños tratados con antibióticos de manera innecesaria, siendo todavía mayor este porcentaje en menores de 3 años.
En la otitis media aguda un alto porcentaje de pacientes fueron tratados con antibióticos (73,1% en 2017, 76,8% en 2018 y 76,6% en 2019), cifra muy elevada, teniendo en cuenta que aproximadamente el 90% de los casos de OMA pueden considerarse como una enfermedad autolimitada, con adecuada evolución con analgesia pautada18. Si bien es cierto que la utilización de antibióticos previene complicaciones como la mastoiditis aguda, no se trata de una complicación frecuente y es necesario tratar a más de cuatro mil pacientes con OMA para prevenir un caso de mastoiditis18,25. Quizás la selección del antibiótico no podemos considerarla inapropiada, pues prácticamente la mitad fueron tratados con amoxicilina y una quinta parte con amoxicilina-ácido clavulánico, siendo estos datos entendibles si consideramos los fracasos terapéuticos con amoxicilina, los niños menores de seis meses o los menores de dos años con clínica grave18. En el caso de los macrólidost, existe una mayor adecuación que en la FAA, pues en el último año solo un 4,9% recibieron tratamiento con este grupo terapéutico23. Aunque en España del 30 al 50% de los neumococos son resistentes a macrólidos, este grupo es de elección en pacientes con alergia grave con reacción anafiláctica a la penicilina18,26. En esta patología faltaría seguir promoviendo estrategias destinadas a enfocar tratamientos diferidos y criterios clínicos que nos adecúen un tratamiento empírico antibiótico con pautas cortas de cinco días27.
En nuestra área, con mayoritaria población urbana, se ha encontrado mayor consumo antibiótico en población rural, explicable posiblemente por la existencia de menor plantilla de pediatras en zonas rurales.
Con nuestro estudio se demuestra que sigue siendo importante la formación y evaluación continua, con obtención de datos de consumo y la retroalimentación de estos a los profesionales prescriptores. Se corrobora la necesidad de establecer un PROA en nuestro ámbito de AP, con la implicación y el trabajo multidisciplinar de todos los profesionales sanitarios.
CONFLICTO DE INTERESES
Este trabajo no ha recibido ningún tipo de financiación económica. Los autores declaran no tener ningún conflicto de intereses.
ABREVIATURAS
AEMPS: Agencia Española del Medicamento y Productos Sanitarios · AP: Atención Primaria · ATC: Sistema de Clasificación Anatómica Terapéutica; química · CEIM: Comité Ético de Investigación con medicamentos · CIAP: Clasificación Internacional de AP · CIE-9: Código Internacional de Enfermedades 9.ª edición · DHD: dosis diaria definida por 1000 habitantes/día · DOT: número de días de tratamiento · EBHGA: estreptococo betahemolítico del grupo A · ECDC: European Centre for disease Prevention and control · FAA: faringoamigdalitis aguda · OMA: otitis media aguda · PRAN: Plan Nacional frente a la resistencia a los antibióticos · PROA: Programas de Optimización de Uso de Antibióticos · SESCAM: Servicio de Salud de Castilla La Mancha. UE: Unión Europea.
BIBLIOGRAFÍA
- Albañil Ballesteros MR. Plan Nacional de Resistencia a Antibióticos. Form Act Pediatr Aten Prim. 2016;9;56-9.
- Antimicrobial consumption in the EU/EEA, annual epidemiological report for 2019. En: European Centre for Disease Prevention and Control. Stockholm: ECDC; 2020: 4-9 [en línea] [consultado el 16/02/2021]. Disponible en http://ecdc.europa.eu/en
- Malo S, Bjerrum l, Feja C, Lallana MJ, Poncel A, Rabanaque MJ. Prescripción antibiótica en infecciones respiratorias agudas en Atención primaria. An Pediatr. 2014; 82: 412-16.
- Canton R, Loza E, Aznar J, Barrón-Adúriz R, Calvo J, Castillo FJ, et al. Antimicrobial susceptibility trends and evolution of isolates with extended spectrum beta-lactamases among Gram-negative organisms recovered during the SMART study in Spain (2011-2015). Rev Esp Quimioter 2018; 31:136-45.
- Díaz MA, Hernández JR, Martínez-Martínez l, Rodríguez Baño J, Pascual A, Grupo de Estudio de Infección Hospitalaria (GEIH). Escherichia coli y Klebsiella pneumoniae productoras de betalactamasas de espectro extendido en hospitales españoles: segundo estudio multicéntrico (proyecto GEIH-BLEE 2006). Enferm Infecc Microbiol Clin 2009; 27:503-10.
- European Centre for Disease Prevention and Control. ECDC country visit to Spain to discuss antimicrobial resistance issues. Stockholm: ECDC; 2018.
- Fernández-Urrusuno R, Flores-Dorado M, Moreno-Campoy E, Montero-Balosa MC. Selección de indicadores para la monitorización continua del impacto de programas de optimización de uso de antimicrobianos en Atención Primaria. Enferm Infecc Microbiol Clin. 2015 May;33:311-9.
- Plan Nacional frente a la Resistencia de Antibióticos 2019-2021. En: Ministerio de Sanidad, Agencia Española de Medicamentos y Productos Sanitarios. 2019 [en línea] [consultado el 01/12/2020]. Disponible en www.resistenciaantibioticos.es
- Hulscher MEJL, Grol RPTM, van der Meer JWM. Antibiotic prescribing in hospitals: a social and behavioural scientific approach. Lancet Infect Dis. 2010; 10:167-75.
- Plan estratégico y de riesgo para reducir el riesgo de selección y diseminación de la resistencia a los antibióticos. AEMPS. En: Ministerio de Sanidad, Servicios Sociales e Igualdad. 2015 [en línea] [consultado el 09/06/2022] Disponible en www.aemps.gob.es/publicaciones/publica/plan-estrategico-antibioticos/v2/docs/plan-estrategico-antimicrobianos-AEMPS.pdf
- Objetivos de mejora prioritarios en Atención Primaria (Pediatría). AEMPS. En: Ministerio de Sanidad, Servicios Sociales e Igualdad. 2017 [en línea] [consultado el 09/06/2022] Disponible en www.resistenciaantibioticos.es/es/publicaciones/objetivos-de-mejora-prioritarios-en-atencion-primaria-pediatria
- Ashiru-Oredope D, Hopkins S J. Antimicrobial stewardship: English Surveillance Programme for Antimicrobial Utilization and Resistance (ESPAUR). Antimicrob Chemother 2013; 68:2421-23.
- Holstiege J, Schink T, Molokhia M, Mazzaglia G, Innocenti F, Oteri A, et al. Systemic antibiotic prescribing to paediatric outpatients in 5 European countries: a population-based cohort study. BMC Pediatr. 2014; 14:11-14.
- Holstiege J, Garbe E. Systemic antibiotic use among children and adolescents in Germany: a population-based study. European Journal of pediatrics. 2013;172:787-95.
- Youngster I, Avorn J, Belleudi V, Cantarutti A, Díez-Domingo J, Kirchmayer U, et al. Antibiotic Use in Children. A Cross-National Analysis of six Countries. J Pediatr. 2017; 182:239-44.
- Informe anual PRAN. Junio 2019-Junio 2020. En: Ministerio de Sanidad, Agencia Española de Medicamentos y Productos Sanitarios. 2021 [en línea] [consultado el 01/03/2021]. Disponible en www.resistenciaantibioticos.es
- Piñeiro Pérez R, Álvez González F, Baquero-Artigao F, Cruz Cañete M, de la Flor i Bru J, Fernández Landaluce A y Grupo Colaborador de Faringoamigdalitis Aguda en Pediatría. Actualización del documento de consenso sobre el diagnóstico y tratamiento de la faringoamigdalitis aguda. An Pediatr. 2020; 3:206.e1-206.e8
- Del Castillo Martín F, Baquero Artigao F, de la Calle Cabrera T, López Robles M, Ruiz Canela J, Alfayate Miguelez S, et al. Documento de consenso sobre etiología, diagnóstico y tratamiento de la otitis media aguda. An Pediatr (Barc): 2012; 77: 345.e1-345.e8
- Tyrstrup M, Beckman A, Mölstad S, Engström S, Lannering C, Melander E, et al. Reduction in antibiotic prescribing for respiratory tract infections in swedish primary care, a retrospective study of electronic patient records. BMC Infectious Diseases. 2016; 16:709.
- Lampi E, Carlsson F, Sundvall PD, Torres MJ, Ulleryd P, Åhrén C, et al. Interventions for prudent antibiotic use in primary healthcare: an econometric analysis. BMC Health Serv Res. 2020; 20: 895.
- García Vera C, Albañil Ballesteros R. Prescripción de antibióticos en pediatría de atención primaria: una responsabilidad compartida. An Pediatr. 2018; 89:195-6.
- Holten KB, Onusko EM. Appropriate prescribing of oral beta-lactam antibiotics. Am Fam Physician. 2000; 62:611-20.
- Baquero Artigao F, Michavila A, Suárez-Rodríguez A, Hernández A, Martínez-Campos l, Calvo C, et al. Documento de consenso de la Sociedad Española de Infectología Pediátrica, Sociedad Española de Inmunología Clínica y Alergia Pediátricas, Asociación Española de Pediatría de Atención Primaria y Sociedad Española de Pediatría Extrahospitalaria y Atención Primaria sobre antibioterapia en alergia a penicilina o Amoxicilina. An Pediatr (Barc) 2017; 86:99.e1-99.e9
- Ewald D, Huss G, Auras S, Cáceres JR, Hadjipanayis A, Geraedts M. Development of a core set of quality indicators for paediatric primary care practices in Europe, COSI-PPC-EU. Eur J Pediatr. 2018; 177:921-33.
- Thompson PL, Gilbert RE, Long PF, Saxena S, Sharland M, Wong IC. Effect of antibiotics for otitis media on mastoiditis in children: a retrospective cohort study. Pediatrics. 2009; 123:424-30.
- Pérez E, Martín J, Mazón A, García C, Robles P, Iriarte V, et al. Antimicrobial resistance among respiratory pathogens in Spain: latest data and changes over 11 years (1996-1997 to 2006-2007). Antimicrobial Agents Chemother. 2010; 54:2953-59.
- Spurling G, del Mar C, Dooley l, Foxlee R, Farley R. Delayed antibiotic prescriptions for respiratory infections. Cochrane Database Syst Rev. 2017; 9.