

Educación en el asma. Evaluación de los conocimientos sobre asma infantil en consultas de Atención Primaria
María Vegas Carróna, M.ª Teresa Asensi Monzób
aPediatra. CS Carranque. Málaga. España.
bPediatra. CS Serrería 1. Valencia. España.
Correspondencia: M Vegas. Correo electrónico: mvegas_91@hotmail.com
Cómo citar este artículo: Vegas Carrón M, Asensi Monzó MT. Educación en el asma. Evaluación de los conocimientos sobre asma infantil en consultas de Atención Primaria. Rev Pediatr Aten Primaria. 2022;24:e93-e105.
Publicado en Internet: 12-04-2022 - Número de visitas: 16502
Resumen
Objetivos: determinar el nivel de conocimiento sobre asma de los familiares de niños asmáticos seguidos en consultas de Atención Primaria.
Material y métodos: estudio descriptivo y transversal realizado mediante encuestas de conocimientos sobre asma usando el Newcastle Asthma Knowledge Questionnaire (NAQK), cumplimentadas por familiares de niños/as asmáticos seguidos en consultas de pediatría de Atención Primaria, realizadas entre noviembre de 2020 y marzo de 2021.
Resultados: se encuestó a 97 familiares (edad media de 39,73 años, 81,4% madres). La puntuación media obtenida en el NAQK fue 19,97/31. No se encontró ninguna relación significativa entre la puntuación NAQK obtenida y la edad de progenitores, el número de hijos asmáticos, el uso de tratamiento preventivo, las hospitalizaciones previas, la necesidad de visitas a urgencias o centro de salud ante crisis asmáticas, la vacunación antigripal previa de los hijos asmáticos o el hecho de conocer cuáles son los grupos de riesgo para dicha vacunación. Sin embargo, sí se encontró una relación estadísticamente significativa entre la puntuación NAQK y el nivel de estudios de progenitores (p = 0,002 <0,05), así como el grado de parentesco (madre o padre) con el paciente (p = 0,002 <0,05).
Conclusiones: nuestros encuestados tienen un nivel de conocimiento sobre asma mayor comparado con otros estudios realizados en ámbito escolar u hospitalario. Sin embargo, se detectan aspectos deficitarios que podrían mejorarse mediante la implantación de programas educativos en Atención Primaria, lo que supondría un aumento de los conocimientos sobre asma de nuestros encuestados y, por tanto, una mejora en su calidad de vida.
Palabras clave
● Asma ● Atención Primaria de Salud ● Conocimiento de asma ● Cuestionario The Newcastle Asthma Knowledge Questionnaire ● EducaciónINTRODUCCIÓN
El asma es la enfermedad crónica pediátrica más frecuente en países desarrollados, ocasionando una elevada repercusión individual, familiar y socioeconómica. Es motivo de gran absentismo escolar, siendo además una de las principales causas de ingreso hospitalario en los niños1.
Los médicos somos cada vez más conscientes de la importancia de evaluar el nivel de conocimientos que poseen los pacientes sobre sus enfermedades, particularmente en el caso de patologías crónicas, que requieren la participación del enfermo y sus familias en el tratamiento. Por este motivo, en los últimos años se están dirigiendo muchos esfuerzos hacia la educación de los niños asmáticos y sus familias2.
La mayoría de los estudios demuestran que las intervenciones educativas añadidas al tratamiento médico del asma son beneficiosas, ya que mejoran la sintomatología, aumentan el grado de conocimiento sobre la enfermedad, conducen a la adquisición de habilidades y promueven la participación familiar en el manejo de la enfermedad, favoreciendo así el cumplimiento terapéutico2. Por ello, las principales guías de manejo del asma actuales recomiendan la intervención educativa como un pilar básico del tratamiento de asma3. Sin embargo, todo esto no asegura una disminución de la morbilidad o una mejoría en la calidad de vida de los pacientes asmáticos si no va acompañado de planes de acción individualizados, revisiones periódicas y aprendizaje del automanejo del asma4.
Se considera que la evaluación del nivel de conocimientos sobre asma y su progresión (conocido como “diagnóstico educativo”) es una parte primordial en el proceso educativo de dicha patología. Para ello, disponemos de varios cuestionarios, traducidos y validados al castellano, entre los que figura el Newcastle Asthma Knowledge Questionnaire (NAQK), el cual ha demostrado ser un instrumento válido para la evaluación de los conocimientos sobre asma de pacientes y cuidadores2. Su versión española es aceptable y equivalente culturalmente a la versión original y tiene un buen grado de fiabilidad, validez y reproductibilidad4.
El objetivo de este estudio es determinar el nivel de conocimiento sobre asma y su manejo entre familiares de niños asmáticos seguidos en nuestra consulta de Atención Primaria (AP), utilizando para ello una encuesta elaborada y validada con dicho fin.
De manera secundaria, se pretende determinar si existe relación entre el conocimiento de familiares y el uso de tratamiento preventivo, las hospitalizaciones previas, las visitas a urgencias o al centro de salud por exacerbaciones asmáticas y su relación con vacunación antigripal anual.
MATERIAL Y MÉTODOS
Estudio observacional descriptivo y transversal mediante encuestas auto cumplimentadas, sobre los conocimientos de asma infantil y su manejo. Se enviaron mediante correo electrónico dichos cuestionarios (a través de Google Forms) a los familiares de niños/as asmáticos seguidos en nuestra consulta de AP en los centros de salud de Carranque y las Delicias (Málaga, España). Las encuestas fueron realizadas durante el período comprendido entre el 23 de noviembre de 2020 y el 7 de marzo de 2021.
En dichas encuestas, los conocimientos sobre asma fueron evaluados usando el NAQK traducido al castellano y validado por Praena, et al.4. Además, se recogieron una serie de ítems para valorar la situación clínica y familiar del paciente: edad y sexo del paciente y familiar, nivel de estudios del familiar, número de hijos con asma, necesidad de ingreso hospitalario, visitas a urgencias o al centro de salud por exacerbaciones asmáticas previas, tratamiento preventivo que usaba el paciente y vacunación antigripal en la campaña previa o actual.
Cada pregunta del cuestionario NAQK se puntúa con 0 (incorrecta) o 1 (correcta), siguiendo la sistemática de corrección de Praena, et al.4. La puntuación total se obtiene sumando la puntuación asignada a cada una de las 31 preguntas de las que se compone el cuestionario. Por tanto, la puntuación final podrá variar entre 0 y 31 puntos, y a mayor puntuación obtenida mayor será el grado de conocimiento sobre asma y su manejo.
Se consideraron elegibles para este estudio los familiares de pacientes menores de 14 años, con diagnóstico médico previo de asma, que consultaban de manera presencial o telefónica (debido a la situación de pandemia causada por COVID-19), por sintomatología respiratoria o de otro tipo durante el citado periodo de estudio, cuando alguno de los investigadores estuviese presente. Los criterios de inclusión fueron: familiares mayores de edad, con adecuado dominio del castellano y consentimiento verbal previo a participar en el estudio, capaces de comprender y rellenar el cuestionario. Se excluyeron a familiares que no cumplieran todos los criterios de inclusión citados. A todos ellos se les solicitó su correo electrónico personal para el envío de la encuesta mediante Google Forms, siempre y cuando hubiesen dado previamente su consentimiento verbal para la utilización de los datos.
Se realizó un análisis descriptivo de las variables estudiadas y los valores se expresaron como porcentaje respecto al total. Además, para las variables numéricas se calculó su media, mediana, desviación típica y rango.
El análisis estadístico se realizó con el programa informático SPSS versión 25.0. Se consideraron las diferencias estadísticamente significativas con un valor p <0,05. Se emplearon diferentes pruebas para demostrar la asociación estadística entre la variable cuantitativa puntuación de la prueba NAQK y el resto de las variables: el coeficiente de correlación de Pearson para las variables cuantitativas, la prueba de la T de Student (dos categorías) y el análisis de la varianza (varias categorías) para las variables cualitativas. Como test no paramétricos (los cuales no precisan condición previa de normalidad) se empleó la prueba de U de Mann-Whitney.
RESULTADOS
ANÁLISIS DESCRIPTIVO
Se enviaron 164 cuestionarios, de los cuales fueron contestados 97, obteniéndose una participación del 59,1%. Los pacientes fueron 53 niños (54,6%) y 44 niñas (45,4%) con una edad media de 6,8 años (desviación estándar [DE] = 3,48; rango 2-14).
El 81,4% de los cuestionarios fueron cumplimentados por la madre, seguido de un 11,3% por el padre, un 5,2% por ambos y solo un 2,1% por otro tipo de familiar (en su mayoría abuelos). La edad media de los encuestados fue de 39,73 años (DE = 6,11; rango 24-63). El nivel de estudios predominante entre los encuestados fueron los estudios universitarios (35,1%), seguido de formación profesional (22,7%) y enseñanza obligatoria (16,5%). El 82,5% de los encuestados tenían solo un hijo con asma, y un 15,5% tenían más de un hijo con dicha patología, siendo el número medio de hijos asmáticos de 1,21 (DE = 0,46; rango 1-5).
Un 13,4% de los pacientes habían ingresado previamente por exacerbación asmática, de estos el 69,2% lo hicieron solo en una ocasión, mientras que el 30,8% lo habían hecho dos o más veces.
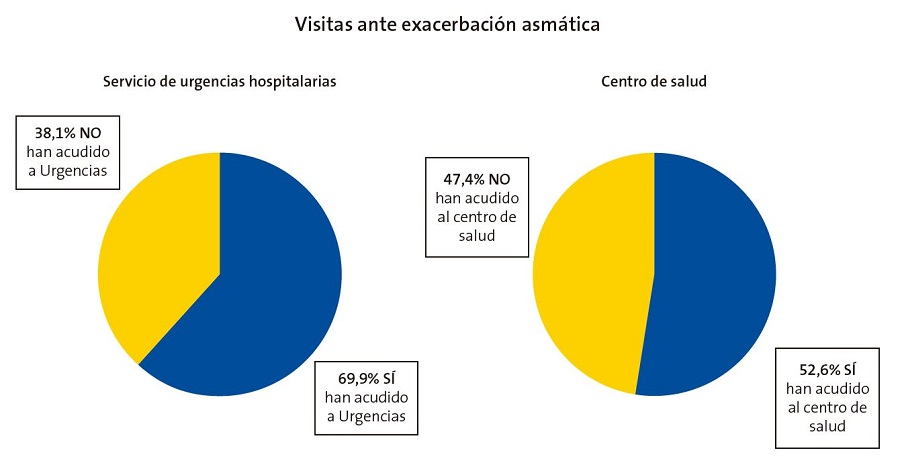
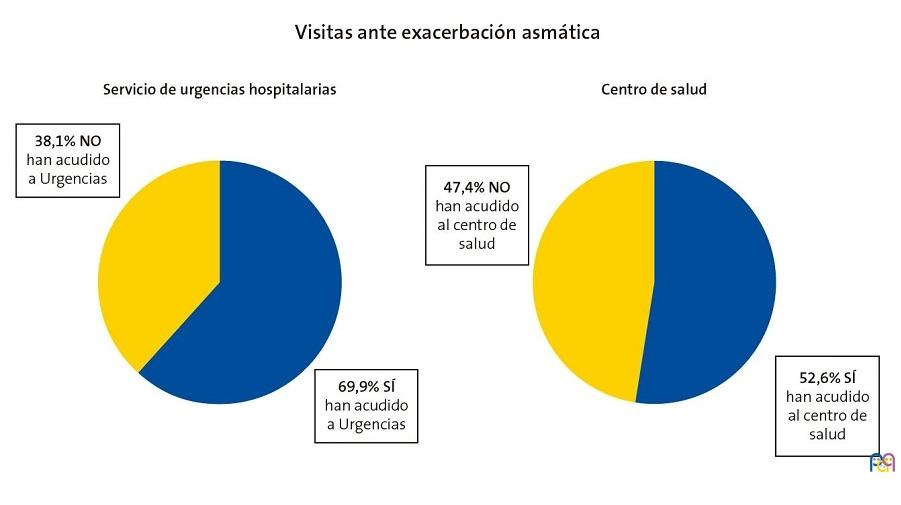
Un 61,9% de los encuestados habían acudido alguna vez a un servicio de urgencias por crisis asmática, siendo el número medio de visitas a dicho servicio de 2,74 (DE = 3,12; rango 1-15). Por otro lado, un 52,6% de los pacientes habían acudido de urgencias a un centro de salud por crisis asmática. De ellos, solo un 10% afirma haber acudido en una ocasión, frente al 90% que han acudido dos o más veces por dicho motivo. Por tanto, se evidencia por parte de estos encuestados mayor asistencia a los servicios de urgencias con respecto a los centros de salud ante una exacerbación asmática de sus hijos (Fig. 1).
| Figura 1. Gráfico de sectores comparativo de las visitas de los encuestados con sus hijos a los servicios de urgencias hospitalarias y centro de salud ante una exacerbación asmática desde el diagnóstico de asma |
|---|
 |
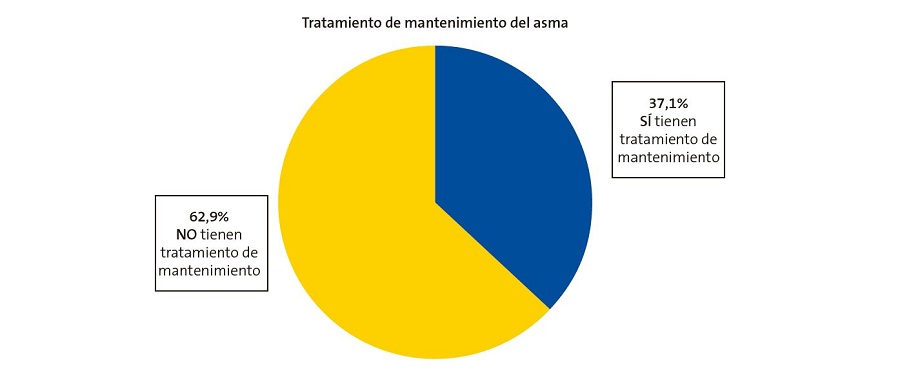
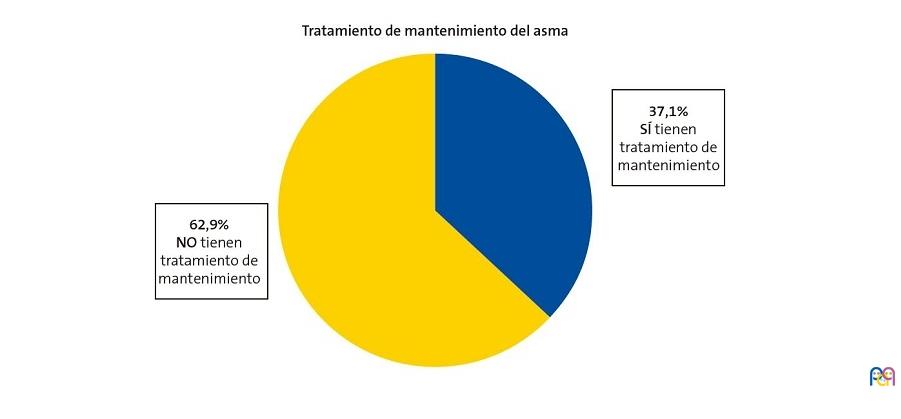
El 62,9% de los pacientes no tenían prescrito tratamiento de mantenimiento del asma, mientras que un 37,1% sí que lo tenían (Fig. 2), principalmente corticoides inhalados (43,9%) seguido de la combinación de broncodilatadores de acción prolongada con corticoides inhalados (22%), antileucotrienos (17,1%) y la combinación de antileucotrienos y corticoides inhalados (17,1%).
| Figura 2. Gráfico de sectores sobre la prescripción de tratamiento de mantenimiento del asma |
|---|
 |
CUESTIONARIO NAQK
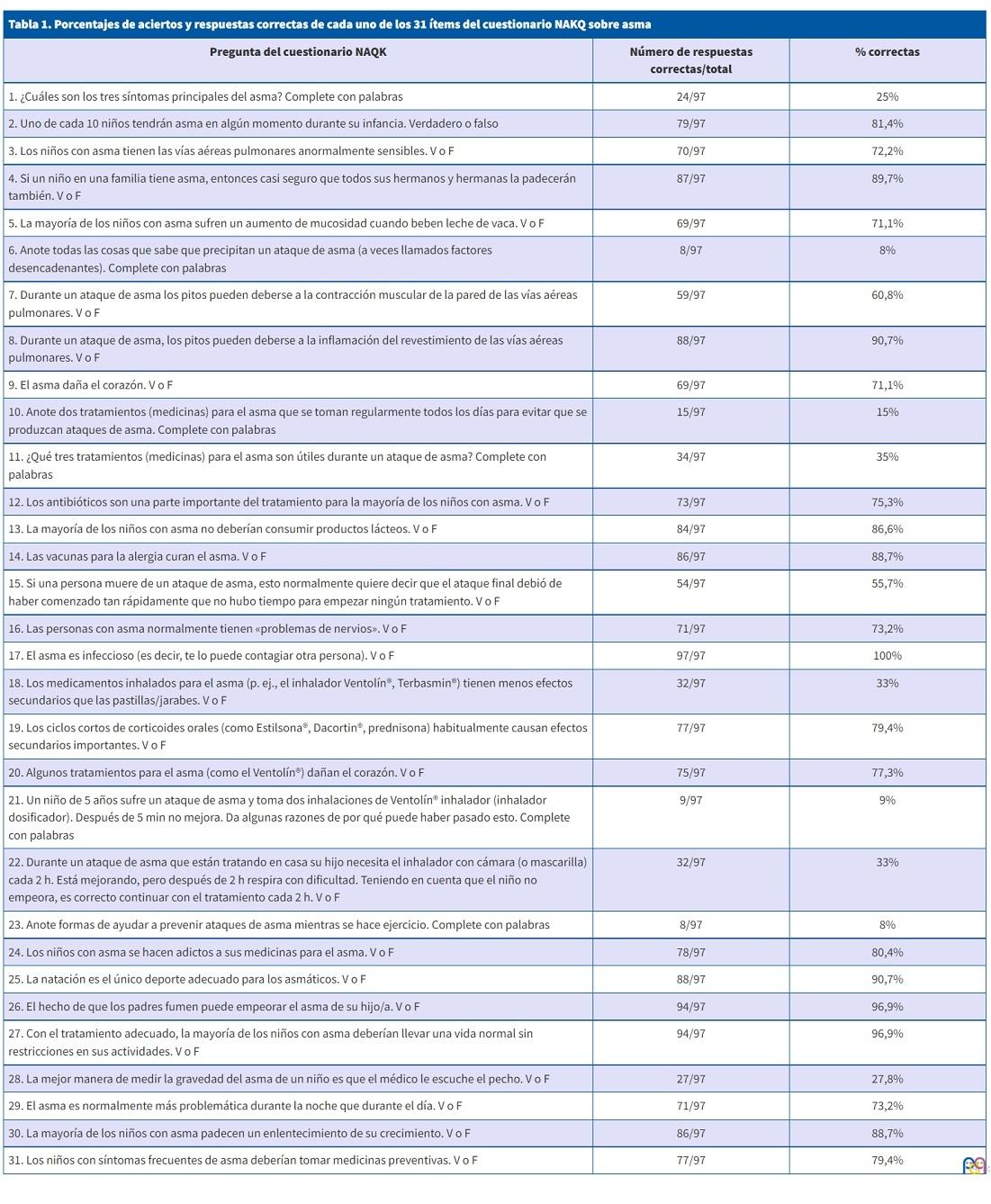
La puntuación media obtenida en el NAQK fue de 19,97 (DE 2,66; rango 13-28). En la Tabla 1, se muestra el porcentaje de aciertos de cada uno de los 31 ítems del cuestionario NAQK.
| Tabla 1. Porcentajes de aciertos y respuestas correctas de cada uno de los 31 ítems del cuestionario NAKQ sobre asma | ||
|---|---|---|
| Pregunta del cuestionario NAQK | Número de respuestas correctas/total | % correctas |
| 1. ¿Cuáles son los tres síntomas principales del asma? Complete con palabras | 24/97 | 25% |
| 2. Uno de cada 10 niños tendrán asma en algún momento durante su infancia. Verdadero o falso | 79/97 | 81,4% |
| 3. Los niños con asma tienen las vías aéreas pulmonares anormalmente sensibles. V o F | 70/97 | 72,2% |
| 4. Si un niño en una familia tiene asma, entonces casi seguro que todos sus hermanos y hermanas la padecerán también. V o F | 87/97 | 89,7% |
| 5. La mayoría de los niños con asma sufren un aumento de mucosidad cuando beben leche de vaca. V o F | 69/97 | 71,1% |
| 6. Anote todas las cosas que sabe que precipitan un ataque de asma (a veces llamados factores desencadenantes). Complete con palabras | 8/97 | 8% |
| 7. Durante un ataque de asma los pitos pueden deberse a la contracción muscular de la pared de las vías aéreas pulmonares. V o F | 59/97 | 60,8% |
| 8. Durante un ataque de asma, los pitos pueden deberse a la inflamación del revestimiento de las vías aéreas pulmonares. V o F | 88/97 | 90,7% |
| 9. El asma daña el corazón. V o F | 69/97 | 71,1% |
| 10. Anote dos tratamientos (medicinas) para el asma que se toman regularmente todos los días para evitar que se produzcan ataques de asma. Complete con palabras | 15/97 | 15% |
| 11. ¿Qué tres tratamientos (medicinas) para el asma son útiles durante un ataque de asma? Complete con palabras | 34/97 | 35% |
| 12. Los antibióticos son una parte importante del tratamiento para la mayoría de los niños con asma. V o F | 73/97 | 75,3% |
| 13. La mayoría de los niños con asma no deberían consumir productos lácteos. V o F | 84/97 | 86,6% |
| 14. Las vacunas para la alergia curan el asma. V o F | 86/97 | 88,7% |
| 15. Si una persona muere de un ataque de asma, esto normalmente quiere decir que el ataque final debió de haber comenzado tan rápidamente que no hubo tiempo para empezar ningún tratamiento. V o F | 54/97 | 55,7% |
| 16. Las personas con asma normalmente tienen «problemas de nervios». V o F | 71/97 | 73,2% |
| 17. El asma es infeccioso (es decir, te lo puede contagiar otra persona). V o F | 97/97 | 100% |
| 18. Los medicamentos inhalados para el asma (p. ej., el inhalador Ventolín®, Terbasmin®) tienen menos efectos secundarios que las pastillas/jarabes. V o F | 32/97 | 33% |
| 19. Los ciclos cortos de corticoides orales (como Estilsona®, Dacortin®, prednisona) habitualmente causan efectos secundarios importantes. V o F | 77/97 | 79,4% |
| 20. Algunos tratamientos para el asma (como el Ventolín®) dañan el corazón. V o F | 75/97 | 77,3% |
| 21. Un niño de 5 años sufre un ataque de asma y toma dos inhalaciones de Ventolín® inhalador (inhalador dosificador). Después de 5 min no mejora. Da algunas razones de por qué puede haber pasado esto. Complete con palabras | 9/97 | 9% |
| 22. Durante un ataque de asma que están tratando en casa su hijo necesita el inhalador con cámara (o mascarilla) cada 2 h. Está mejorando, pero después de 2 h respira con dificultad. Teniendo en cuenta que el niño no empeora, es correcto continuar con el tratamiento cada 2 h. V o F | 32/97 | 33% |
| 23. Anote formas de ayudar a prevenir ataques de asma mientras se hace ejercicio. Complete con palabras | 8/97 | 8% |
| 24. Los niños con asma se hacen adictos a sus medicinas para el asma. V o F | 78/97 | 80,4% |
| 25. La natación es el único deporte adecuado para los asmáticos. V o F | 88/97 | 90,7% |
| 26. El hecho de que los padres fumen puede empeorar el asma de su hijo/a. V o F | 94/97 | 96,9% |
| 27. Con el tratamiento adecuado, la mayoría de los niños con asma deberían llevar una vida normal sin restricciones en sus actividades. V o F | 94/97 | 96,9% |
| 28. La mejor manera de medir la gravedad del asma de un niño es que el médico le escuche el pecho. V o F | 27/97 | 27,8% |
| 29. El asma es normalmente más problemática durante la noche que durante el día. V o F | 71/97 | 73,2% |
| 30. La mayoría de los niños con asma padecen un enlentecimiento de su crecimiento. V o F | 86/97 | 88,7% |
| 31. Los niños con síntomas frecuentes de asma deberían tomar medicinas preventivas. V o F | 77/97 | 79,4% |
- Conocimientos generales
Tan solo un 25% de los encuestados fue capaz de enumerar correctamente los tres síntomas principales de una crisis asmática. En un porcentaje más elevado de casos, los encuestados enumeraron hasta dos síntomas (52%), pero las normas de corrección del NAQK indican que, para que la respuesta sea válida, se tienen que enumerar los tres síntomas.
El 81,4% conocía cuál es la prevalencia del asma, el 72,2% sabía que los niños con asma tienen las vías aéreas anormalmente sensibles y un 71,1% afirmó que el asma no daña el corazón. La mayoría de los encuestados (96,9%) sabía que ser fumadores puede empeorar el asma de sus hijos y un 73,2% conocía que el asma es más problemática por la noche que durante el día. Sin embargo, un 72,2% de los progenitores consideró que la mejor manera de medir la gravedad del asma es mediante la auscultación pulmonar del médico.
- Crisis aguda de asma
Solo un 8% de los encuestados identificó correctamente los tres principales factores desencadenantes de una crisis (ejercicio, alergia y resfriados), aunque un 47% identificó un factor y un 25% identificó dos factores. Un 60,8% indicó que los pitos pueden deberse a broncoconstricción, y el 90,7% respondió que se debían a la inflamación de la pared bronquial.
En cuanto al tratamiento de una crisis aguda, solo un 35% supo nombrar correctamente dos tratamientos útiles ante una exacerbación asmática y un 39% identificó de forma correcta un tratamiento, siendo uno de los errores más comunes indicar la budesónida como fármaco de este grupo. Además, solo un 8% conocía dos formas para prevenir un ataque de asma de esfuerzo ante la realización de ejercicio, mientras que la mitad de los encuestados (50%) no identificaron de manera correcta ninguna forma de prevención.
En cuanto a los efectos adversos de medicamentos, el 79,4% sabía que los ciclos cortos de corticoides orales no causan efectos secundarios importantes, el 77,3% sabía que el salbutamol no daña el corazón, pero solo un 33% supo que los medicamentos inhalados tienen menos efectos secundarios que los orales.
En cuanto a la pregunta de cómo manejar una crisis asmática que no mejora tras una dosis de salbutamol, solo el 9% supo identificar dos formas de actuación correcta, mientras que más de la mitad (un 59% de los casos), no supo acertar ninguna razón.
- Tratamiento de mantenimiento
La mayoría de los encuestados (75,3% de los casos) sabían que los antibióticos no son una parte fundamental del tratamiento y que las vacunas de la alergia no son un tratamiento definitivo para el asma (88,7% de los casos).
En las preguntas referentes al tratamiento de mantenimiento del asma, solo un 15% de los encuestados fueron capaces de identificar dos tipos de estos tratamientos, aunque más de la mitad (un 57%), supieron identificar al menos uno de ellos, aceptando como válidos tanto nombres genéricos como principios activos. A pesar de ello, un 79,4% de los encuestados consideraba que los niños con síntomas frecuentes de asma deben tomar tratamiento preventivo, y el 96,9% afirmaron que la mayoría de los niños pueden llevar una vida normal sin restricciones siguiendo un tratamiento adecuado.
- Falsas creencias
En cuanto a la relación del asma con la alergia a las proteínas de la leche de vaca, la mayoría de encuestados (71,1%) sabía que sus hijos no sufren un aumento de mucosidad cuando beben leche de vaca y, por tanto, un 86,6% de ellos asumían que pueden tomar productos lácteos.
Además, la totalidad de los encuestados (100%) afirmaban que el asma no se contagia y que los que la padecen no tienen problemas de “nervios”, acertando un 73,2% de los encuestados. El 80,4% conocía que estos niños no se hacen adictos a sus medicinas y el 88,9% afirmó que el asma no produce un enlentecimiento del crecimiento.
VACUNACIÓN ANTIGRIPAL
Al preguntar a los familiares acerca de sus conocimientos sobre la campaña de vacunación antigripal anual, el 78,4% afirmaba conocer que su hijo pertenecía a uno de los grupos de riesgo que deben recibir la vacuna financiada por el Sistema Nacional de Salud. Sin embargo, solo un 6% de los familiares fue capaz de identificar correctamente tres de los grupos de riesgo para la vacunación, mientras que un 12% identificaron dos grupos, un 34% un grupo y el 47% no fue capaz de identificar ningún grupo de riesgo.
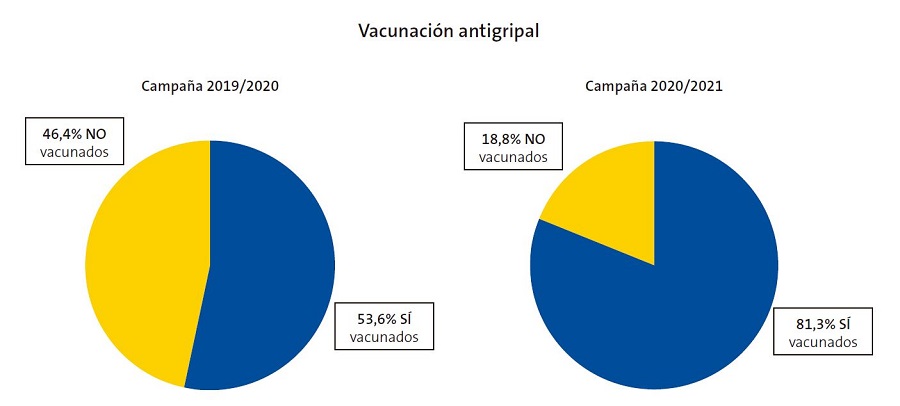
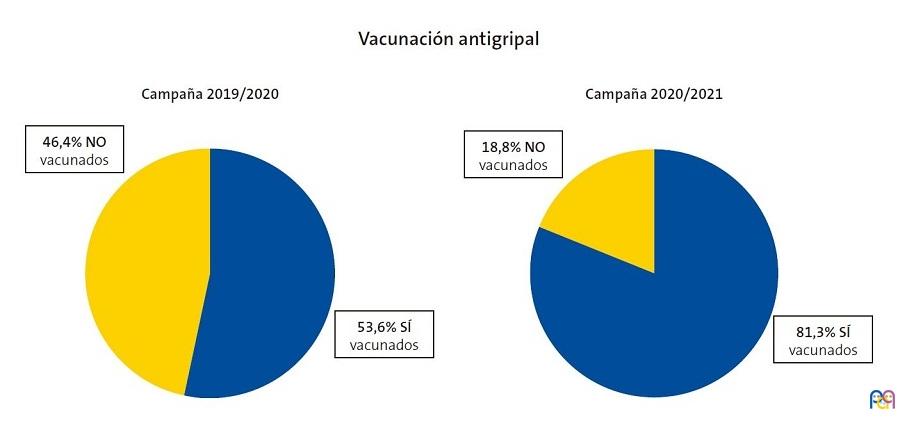
Un 81,3% de los niños asmáticos han recibido la vacuna antigripal durante esta campaña de vacunación (2020-2021), mientras que en la campaña del año pasado (2019-2020) solo lo hicieron un 53,6%, evidenciándose un incremento del 27,7% de los vacunados en la campaña actual con respecto a la anterior (Fig. 3).
| Figura 3. Gráfico de sectores comparativo de los niños asmáticos vacunados contra la gripe durante la campaña vacunal 2020/2021 con respecto a la campaña 2019/2020 |
|---|
 |
ANÁLISIS ESTADÍSTICO
En cuanto al estudio estadístico, no se encontraron diferencias significativas entre la puntuación NAQK obtenida y la edad de los progenitores (p = 0,995 >0,05) o el número de hijos asmáticos (p = 0,788 >0,05) mediante el análisis de correlación de Pearson.
Además, no se encontró relación significativa entre la puntuación NAQK y el uso de tratamiento preventivo (p = 0,381 >0,05), las hospitalizaciones previas (p = 0,055 >0,05), o la necesidad de visitas a urgencias (p = 0,436 >0,05) o centro de salud (p = 0,267 >0,05) ante una exacerbación asmática, empleando en todas ellas la prueba de la T de Student para muestras independientes.
Tampoco se encontraron diferencias estadísticamente significativas entre la calificación NAQK obtenida y la vacunación antigripal previa de los hijos asmáticos, tanto en la campaña vacunal de este año 2020-2021 (p = 0,161 >0,05) como en la del año pasado 2019-2020 (p = 0,105 >0,05), ni se encontró relación significativa entre la puntuación NAQK y el hecho de conocer cuáles son los grupos de riesgo que se benefician de la vacunación antigripal (p = 0,660 >0,05), utilizando para ello el test no paramétrico U de Mann-Whitney.
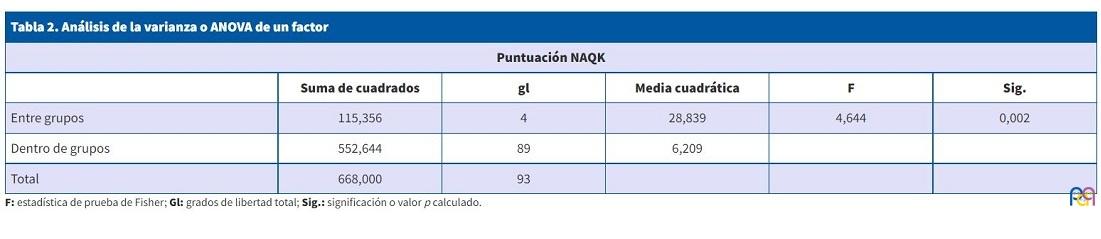
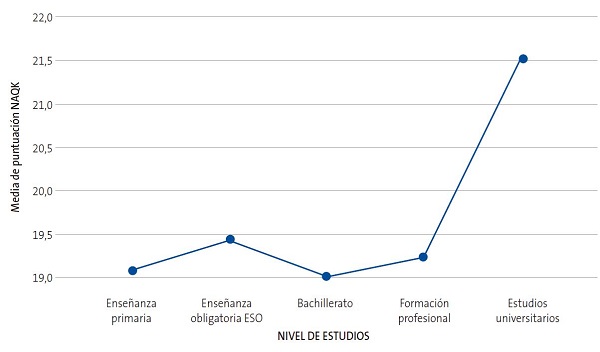
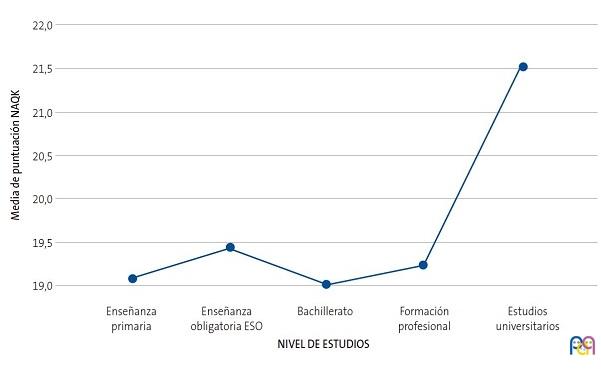
Sin embargo, sí se encontró una relación estadísticamente significativa (p = 0,002 <0,05) entre la puntuación NAQK obtenida y el nivel de estudios de familiares, mediante la prueba de análisis de la varianza o ANOVA de un factor (Tablas 2 y 3, Fig. 4).
| Tabla 2. Análisis de la varianza o ANOVA de un factor | |||||
|---|---|---|---|---|---|
| Puntuación NAQK | |||||
| Suma de cuadrados | gl | Media cuadrática | F | Sig. | |
| Entre grupos | 115,356 | 4 | 28,839 | 4,644 | 0,002 |
| Dentro de grupos | 552,644 | 89 | 6,209 | ||
| Total | 668,000 | 93 | |||
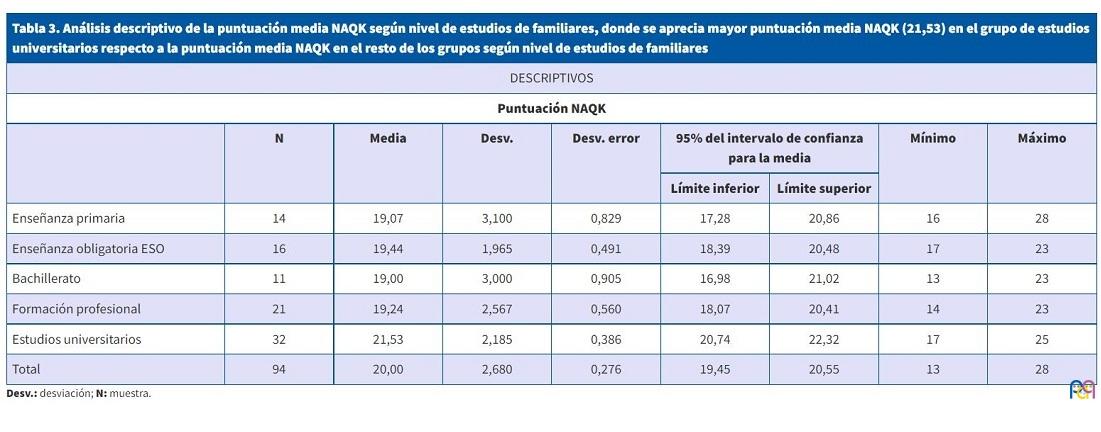
| Tabla 3. Análisis descriptivo de la puntuación media NAQK según nivel de estudios de familiares, donde se aprecia mayor puntuación media NAQK (21,53) en el grupo de estudios universitarios respecto a la puntuación media NAQK en el resto de los grupos según nivel de estudios de familiares | ||||||||
|---|---|---|---|---|---|---|---|---|
| DESCRIPTIVOS | ||||||||
| Puntuación NAQK | ||||||||
| N | Media | Desv. | Desv. error | 95% del intervalo de confianza para la media | Mínimo | Máximo | ||
| Límite inferior | Límite superior | |||||||
| Enseñanza primaria | 14 | 19,07 | 3,100 | 0,829 | 17,28 | 20,86 | 16 | 28 |
| Enseñanza obligatoria ESO | 16 | 19,44 | 1,965 | 0,491 | 18,39 | 20,48 | 17 | 23 |
| Bachillerato | 11 | 19,00 | 3,000 | 0,905 | 16,98 | 21,02 | 13 | 23 |
| Formación profesional | 21 | 19,24 | 2,567 | 0,560 | 18,07 | 20,41 | 14 | 23 |
| Estudios universitarios | 32 | 21,53 | 2,185 | 0,386 | 20,74 | 22,32 | 17 | 25 |
| Total | 94 | 20,00 | 2,680 | 0,276 | 19,45 | 20,55 | 13 | 28 |
| Figura 4. Gráfico de líneas comparativo de puntuaciones medias NAQK según nivel de estudios de familiares |
|---|
 |
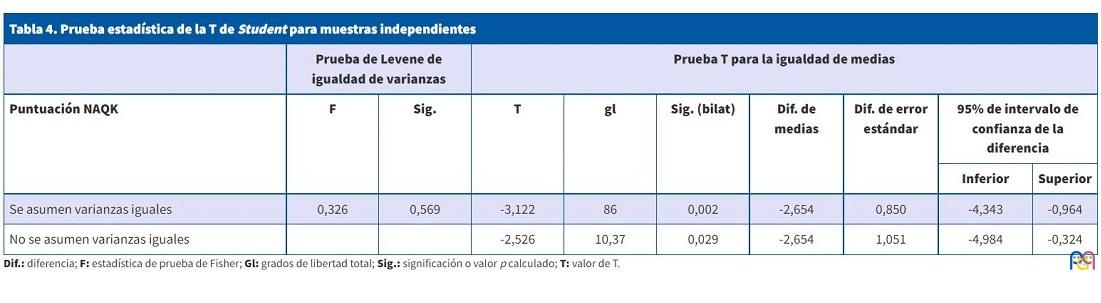
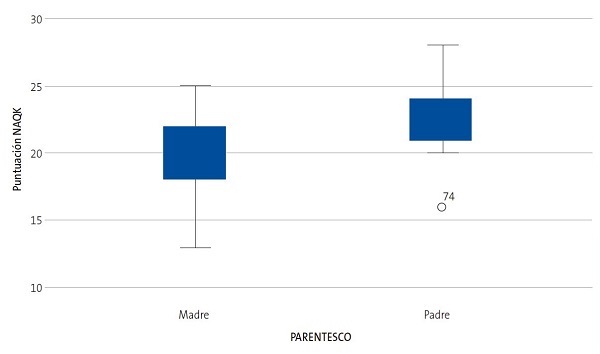
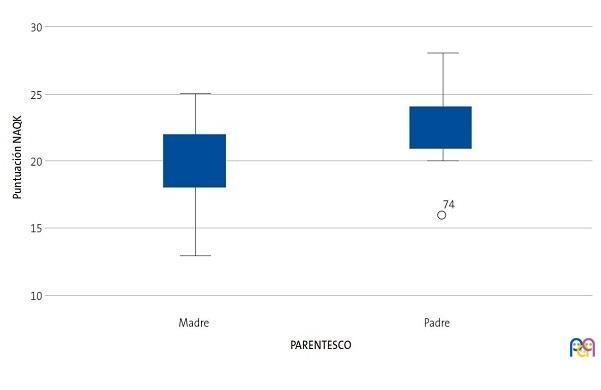
Además, se comprobó, mediante la prueba estadística de la T de Student para muestras independientes, que existían diferencias estadísticamente significativas (T = -3.12, p = 0,002 <0,05) en la puntuación de la prueba respecto al parentesco de madre o padre (Tablas 4 y 5, Fig. 5).
| Tabla 4. Prueba estadística de la T de Student para muestras independientes | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Prueba de Levene de igualdad de varianzas | Prueba T para la igualdad de medias | ||||||||
| Puntuación NAQK | F | Sig. | T | gl | Sig. (bilat) | Dif. de medias | Dif. de error estándar | 95% de intervalo de confianza de la diferencia | |
| Inferior | Superior | ||||||||
| Se asumen varianzas iguales | 0,326 | 0,569 | -3,122 | 86 | 0,002 | -2,654 | 0,850 | -4,343 | -0,964 |
| No se asumen varianzas iguales | -2,526 | 10,37 | 0,029 | -2,654 | 1,051 | -4,984 | -0,324 | ||
| Tabla 5. Análisis descriptivo de la puntuación media NAQK según tipo de parentesco, donde se comprueba que la puntuación media NAQK es mayor en el grupo de los padres (22,5) con respecto al grupo de las madres (19,50), teniendo siempre en cuenta la escasez del tamaño muestral del grupo de los padres (n = 10) | |||||
|---|---|---|---|---|---|
| Estadísticas de grupo | |||||
| Parentesco | N | Media | Desv. | Desv. error promedio | |
| Puntuación NAQK | Madre | 78 | 19,85 | 2,439 | 0,276 |
| Padre | 10 | 22,50 | 3,206 | 1,014 | |
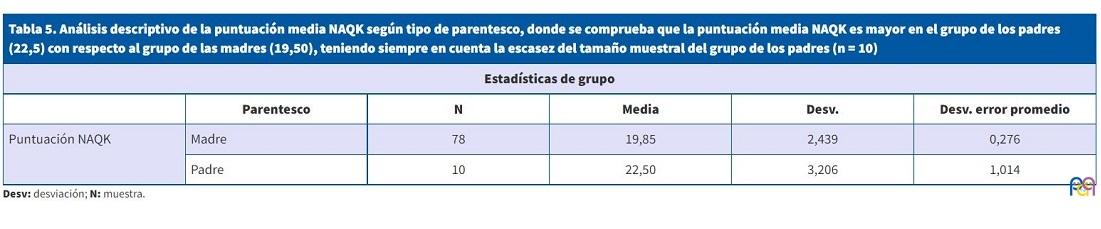
| Figura 5. Gráfico Box-Plot de comparativa de medianas de la puntuación NAQK según el tipo de parentesco |
|---|
 |
DISCUSIÓN
Existen varios estudios en España que utilizan el cuestionario NAQK traducido y adaptado al español por Praena, et al.4 para evaluar los conocimientos sobre asma en padres, profesores o adolescentes asmáticos2-9.
El nivel medio de conocimientos de la muestra de nuestro estudio puede ser considerado como intermedio, ya que la puntuación obtenida en el NAQK (19,97±2,66) es superior a la alcanzada por el grupo de personas sin relación alguna con el asma (16,84±2,56) del estudio de validación al castellano del cuestionario NAQK de Praena, et al4, pero inferior a la obtenida en el grupo de personas con gran conocimiento (23±2,94) de dicho estudio. Además, la puntuación NAQK de nuestro estudio también es superior a la alcanzada por el grupo de bajo conocimiento sobre asma (13,0) del estudio original de validación del cuestionario NAQK realizado en 1990 por Fitzclarence y Henry5, pero inferior a la obtenida por el grupo de alto conocimiento de dicho estudio (25,3).
En nuestro estudio realizado con familiares de niños asmáticos en consultas de AP, se observa que la puntuación NAQK es visiblemente superior a las alcanzadas en otros estudios realizados con padres de niños asmáticos a nivel hospitalario, como el elaborado por García-Luzardo, et al.2 en un servicio de urgencias pediátricas (con una puntuación NAQK de 16,14±2,92), y el realizado por Leonardo Cabello, et al.3 en las consultas de Neumología Pediátrica (con una puntuación NAQK de 18,5±3,7).
Se observa que nuestra puntuación NAQK también es superior a la obtenida por los profesores (17,90±3,1), los adolescentes asmáticos (17,24±2,7) y los adolescentes no asmáticos (16,23±2,8) del estudio sobre asma en varios centros escolares de Praena6 y, además, superior a la obtenida por los profesores del Estudio sobre Asma en los Centros Escolares Españoles (EACEE)7, de 16,0±4,8 puntos.
En cuanto a las puntuaciones NAQK obtenidas por los familiares de niños asmáticos ingresados en hospitales por reagudización de la enfermedad, también fueron menores, como se refleja en el estudio realizado en Australia por Henry, et al8, con una puntuación NAQK de 18,3 en el grupo de niños con varios ingresos previos, y 17,2 puntos en aquellos que ingresaban por primera vez. También se objetiva una puntuación NAQK menor (15,5 puntos) en el estudio realizado en Malasia por Fadzil y Norzila9 en 2002.
Por tanto, es destacable que nuestros encuestados de AP reflejen un mayor nivel de conocimiento (con puntuaciones NAQK mayores) con respecto a otros estudios realizados a nivel hospitalario con padres de niños asmáticos, ya que se sobreentiende a priori que estos pacientes hospitalarios presentan un mayor tiempo de evolución o gravedad de su patología asmática, lo cual debería justificar un mayor grado de conocimiento de la enfermedad. Este mayor nivel de conocimiento reflejado en las consultas de AP podría justificarse por un mayor grado de confianza y cercanía existente en la relación médico-paciente, lo que permitiría a los niños asmáticos y sus familias una mayor accesibilidad para exponer sus dudas sobre el asma y su manejo, siendo estas resueltas de forma rápida y eficaz en un ambiente más cómodo y familiar con respecto al que pudiera existir en un servicio de urgencias o consultas hospitalarias.
Existen diversas publicaciones previas a nuestro estudio donde también se encuentra una relación estadísticamente significativa entre el nivel de conocimientos de los padres sobre el asma y otras variables, como el nivel educativo de los progenitores. Es el caso del estudio ya citado de Fadzil y Norzila9, donde se concluye que el nivel de conocimientos sobre el asma es superior en el grupo de padres con mayor nivel socioeconómico, y lo relaciona probablemente con un mayor nivel de educación en dicho grupo. Además, en este mismo estudio, se obtuvo una relación estadísticamente significativa entre el nivel de conocimientos paternos de asma y el uso de esteroides como tratamiento de mantenimiento, especialmente en altas dosis (p = 0,03 <0,05), datos que no pudieron ser corroborados en nuestro estudio ya que la puntuación NAQK obtenida por los encuestados fue independiente del tratamiento de mantenimiento de sus hijos (p = 0,88 >0,05). De manera análoga a nuestro estudio, Fadzil y Norzila9 tampoco encontraron diferencias significativas en sus resultados en función de la edad paterna o la existencia de ingresos hospitalarios previos. En el estudio realizado en Australia por Henry, et al.8 también se concluye que el grado de conocimiento de los padres de hijos asmáticos es mayor en el grupo de alto nivel socioeconómico y en el de no fumadores, sin que la existencia de ingresos hospitalarios previos modificase el nivel de conocimientos. De la misma forma, en nuestra población estudiada tampoco se encuentra ninguna relación significativa entre el nivel de conocimientos sobre asma y la necesidad de ingreso hospitalario o visitas a Urgencias o AP ante una exacerbación.
Hay que destacar que existen estudios donde se objetiva que el número de visitas a Urgencias por exacerbaciones asmáticas puede reducirse mediante el aumento del grado de conocimientos de los progenitores a través de programas educativos, como sucede en el estudio elaborado por Wesseldine, et al.10, en el que mediante una intervención educativa para el asma se obtiene una reducción significativa tanto del número de reingresos hospitalarios como de las visitas a Urgencias o AP por exacerbación asmática. De la misma forma, en el metaanálisis realizado por Coffman, et al11 se concluye que proporcionar educación sobre el asma reduce las visitas al servicio de urgencias y el tiempo medio de hospitalización de pacientes asmáticos, aunque afirman que no afecta a la probabilidad de ingreso ni al número de visitas urgentes a su médico de AP.
Otro dato que cabe destacar en nuestro estudio es la relación estadísticamente significativa obtenida entre el nivel de conocimientos de asma y el tipo de parentesco de los encuestados (p = 0,02 <0,05), con una puntuación media NAQK visiblemente mayor en el grupo de los padres con respecto al grupo de las madres, dato que debería ser analizado teniendo en cuenta la escasez del tamaño muestral del grupo de los padres. Este dato no ha podido ser corroborado con otros estudios similares al no existir análisis estadísticos previos entre dichas variables.
Hay que tener en cuenta que en nuestro estudio existen algunos aspectos deficitarios sobre los conocimientos en asma de los encuestados, que podrían ser mejorables. Es destacable el resultado obtenido en la pregunta 10 acerca del tratamiento de mantenimiento de asma, donde solo un 15% de los encuestados supo identificar correctamente dos fármacos preventivos, cifra visiblemente inferior a la obtenida en el estudio de Urgencias de García Luzardo, et al.2 que fue de 26,6%, y en el de consultas de Neumología de Leonardo Cabello, et al.3 que fue del 43%. Aunque la educación en asma es competencia de todos los profesionales sanitarios de cualquier nivel asistencial y del medio escolar, teóricamente debería recaer principalmente sobre AP, dada su cercanía y accesibilidad. Sin embargo, los datos publicados demuestran que la educación realizada por los pediatras de AP es insuficiente12. A pesar de que la transmisión de información (conocimientos anatómicos-fisiológicos, factores desencadenantes, demostración de forma práctica de la técnica inhalatoria) se hace de forma frecuente, la entrega de un plan de acción por escrito y la educación en automanejo es deficiente12. Muchos de los pacientes son atendidos en la consulta a demanda, y no en una consulta programada, más adecuada para el desarrollo de un programa educativo. La enfermería, que debería tener un papel fundamental en las actividades educativas, trabajando coordinadamente con el resto de los profesionales, frecuentemente no participa en la atención del niño asmático12. Todo esto supone un déficit en aspectos organizativos como el tiempo, participación y coordinación entre profesionales, que origina una calidad asistencial insuficiente, donde no pueden desarrollarse programas educativos eficientes que permitan a los familiares aumentar su conocimiento acerca del control y tratamiento de mantenimiento del asma. De esta forma, se favorece en ocasiones el desconocimiento, incumplimiento o abandono de este tratamiento por parte de los niños asmáticos y sus familias, como se hace visible en la pregunta 10.
No ocurre lo mismo en relación con el tratamiento de una exacerbación asmática (pregunta 11), donde un 35% de los encuestados supo identificar correctamente dos fármacos empleados en una crisis aguda de asma, porcentaje solo levemente inferior al obtenido en el de consultas de Neumología de Leonardo Cabello, et al 3 que fue del 39,2%, pero ligeramente superior al del estudio de Urgencias de García Luzardo, et al.2, que fue de 31,9%. Esto puede deberse a la accesibilidad y cercanía de la AP, que hace que muchos padres y familiares acudan en numerosas ocasiones a los centros de salud ante las crisis asmáticas de sus hijos, para confirmar el diagnóstico y asegurarse de estar realizando el tratamiento correctamente. Por ello, la implantación de mejoras en los programas educativos (como el refuerzo de los planes de acción por escrito) generaría beneficios evidentes a largo plazo en nuestros pacientes, así como una mejora en su calidad de vida.
Por último, en relación con la vacunación antigripal, cabe destacar el incremento del número de niños asmáticos vacunados de la gripe durante la campaña 2020-2021 con respecto a la campaña anterior. Este aumento podría relacionarse con la existencia de la pandemia causada por COVID-19 en este último año, ya que la preocupación y la incertidumbre en la población de que ambos virus respiratorios pudiesen desencadenar un mayor número de crisis asmáticas o agravarlas, ha provocado en las familias de niños asmáticos una gran sensibilización acerca de la importancia de la vacunación antigripal en dicho colectivo.
En cuanto a las limitaciones de nuestro estudio, hay que señalar que el hecho de que se haya desarrollado durante la pandemia por COVID-19 y su confinamiento, ha supuesto una mayor dificultad para la obtención de la muestra, al disminuir tanto la incidencia de patología asmática como el número de visitas presenciales por dicho motivo en AP. Además, hemos encontrado por parte de algunas familias problemas para el manejo de aplicaciones por internet y, por tanto, para cumplimentar las encuestas enviadas mediante correo electrónico, lo que ha causado una pérdida de muestra bastante significativa. Todo ello, ha dificultado el desarrollo de un programa educativo posterior con nuestros pacientes asmáticos y familiares que pudiera mejorar sus resultados en el cuestionario NAQK y, por tanto, sus conocimientos acerca del asma.
CONCLUSIONES
Nos parece interesante aportar a la literatura los resultados obtenidos con el cuestionario NAQK sobre conocimiento de asma, en una muestra amplia de familiares de niños asmáticos que consultan de forma exclusiva en AP, pues en España el cuestionario NAQK ha sido utilizado sobre todo para evaluar conocimientos en personal docente1,6,7, así como en Servicios de Urgencias2 o consultas hospitalarias de Neumología3, existiendo solo algunos estudios a nivel internacional10,11 que emplean muestra de familiares de niños asmáticos que acuden a consultas de AP y a servicios de Atención Hospitalaria (Urgencias y hospitalización).
Nuestra conclusión principal en este estudio es que, en comparación con otros estudios realizados en el ámbito escolar u hospitalario, nuestros encuestados tienen mayor nivel de conocimiento sobre el asma (reflejado en una puntuación NAQK superior).
Reconocemos que en nuestra población estudiada existen numerosos aspectos deficitarios que habría que mejorar a través de la implantación de programas educativos de calidad en AP, como consultas programadas y específicas de asma para cada paciente o charlas de educación grupal para varias familias.
Además, el uso de nuevas tecnologías durante la pandemia provocada por COVID-19, nos hace replantearnos nuevas formas de educar a los pacientes asmáticos y sus familias mediante recursos y materiales online, como por ejemplo vídeos didácticos sobre los principales aspectos de la enfermedad que pudiesen ser enviados mediante correo electrónico a cada una de estas familias.
Nuestra hipótesis es que esta intervención educativa posterior no solo supondría un aumento de la puntuación NAQK y de los conocimientos sobre asma de nuestros encuestados en futuros estudios, sino que, a largo plazo, permitiría una reducción tanto del número de visitas urgentes como del consumo de recursos sanitarios directos e indirectos que ello conlleva, además de una mejora en el automanejo del asma y, por tanto, de la calidad de vida de nuestros pacientes.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflicto de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
AP: Atención Primaria · DE: desviación estándar · EACEE: Estudio sobre Asma en los Centros Escolares Españoles · NAQK: Newcastle Asthma Knowledge Questionnaire.
BIBLIOGRAFÍA
- Fierro Urturi A, Acebes Puertas R, Córdoba Romero A, del Amo Ramos S, Sanz Fernández M. Impacto de una intervención educativa sobre asma en los profesores de Educación Infantil y Primaria de una zona básica de salud. Rev Pediatr Aten Primaria. 2020; 22:353-60.
- García Luzardo MR, Aguilar Fernández AJ, Rodríguez Calcines N, Pavlovic Nesic S. Conocimientos acerca del asma de los padres de niños asmáticos que acuden a un servicio de urgencias. Acta Pediatr Esp .2012;70:196-203.
- Leonardo Cabello MT, Oceja-Setien E, García Higuera l, Cabero MJ, Pérez Belmonte E, Gómez-Acebo I. Evaluación de los conocimientos paternos sobre asma con el Newcastle Asthma Knowledge Questionnaire. Rev Pediatr Aten Primaria. 2013;15:117-26.
- Praena Crespo M, Lora Espinosa A, Aquino Llinares N, Sánchez Sánchez AM, Jiménez Cortés A. Versión española del NAKQ. Adaptación transcultural y análisis de fiabilidad y validez. An Pediatr. 2009;70:209-17.
- Fitzclarence CA, Henry RL. Validation of an asthma knowledge questionnaire. J Paediatr Child Health. 1990;26:200-4.
- Praena Crespo M, Fernández Truan JC, Aquino Llinares N, Murillo Fuentes A, Sánchez Sánchez A, Gálvez González J, et al. Situación de los conocimientos, las actitudes y la calidad de vida en asma de adolescentes y profesorado. Necesidad de educar en los centros de enseñanza. An Pediatr. 2012;77:226-35.
- López-Silvarrey Varela A. Estudio sobre el asma en los centros escolares españoles (EACEE) 2009-2010. A Coruña. En: Fundación María José Jove; 2011 [en línea] [consultado el 18/04/2021]. Disponible en: www.fundacionmariajosejove.org/media/upload/files/Maqueta_final_publicacin_resultados_Estudio_Asma_Nacional_FMJJ_FBBVA_en_11.pdf
- Henry RL, Cooper DM, Halliday JA. Parental asthma knowledge: its association with readmission of children to hospital. J Paediatr Child Health. 1995;31:95-8.
- Fadzil A, Norzila MZ. Parental asthma knowledge. Med J Malaysia. 2002;57:474-81.
- Wesseldine L, McCarthy P, Silverman M. Structured discharge procedure for children admitted to hospital with acute asthma: a randomised controlled trial of nursing practice. Arch Dis Child. 1999;80:110-14.
- Coffman JM, Cabana MD, Halpin HA, Yelin EH. Effects of asthma education on children’s use of acute care services: a meta-analysis. Pediatrics. 2008;121:575-86.
- Rueda Esteban S. Asma en el niño y adolescente (controversias): Atención Primaria versus Atención Hospitalaria. A favor del manejo en el hospital. Rev Pediatr Aten Primaria. 2014;16:17-27.