
Vol. 24 - Num. 93
Originales
Utilidad de la telemedicina en la atención pediátrica urgente durante la pandemia por COVID-19
Adrián García Rona, Eva Arias Vivasa, Carmen Martínez del Ríob, Rosa M.ª González Tobosoc, Deborah Forrester Zapatad, Patricia Fernández Garcíab, Marta Bote Gascóna
aUnidad de Neuropediatría. Instituto del Niño y del Adolescente. Hospital Clínico San Carlos. Madrid. España.
bServicio de Pediatría. Instituto del Niño y del Adolescente. Hospital Clínico San Carlos. Madrid. España.
cPediatra. CS Ciudad de los Periodistas. Madrid. España.
dPediatra. CS Guzmán el Bueno. Instituto del Niño y del Adolescente. Hospital Clínico San Carlos. Madrid. España.
Correspondencia: A García. Correo electrónico: drgarciaron@gmail.com
Cómo citar este artículo: García Ron A, Arias Vivas E, Martínez del Río C, González Toboso RM, Forrester Zapata D, Fernández García P, et al. Utilidad de la telemedicina en la atención pediátrica urgente durante la pandemia por COVID-19. Rev Pediatr Aten Primaria. 2022;24:23-9.
Publicado en Internet: 25-01-2022 - Número de visitas: 13150
Resumen
Introducción: nuestro sistema sanitario ha sufrido una reorganización sin precedentes priorizando la atención de los pacientes con sintomatología COVID-19. El uso de telemedicina se presenta como una alternativa útil en la era pos-COVID. El objetivo del estudio fue valorar la utilidad del servicio de mensajería de Twitter como herramienta de telemedicina para el cribado de patología urgente.
Material y métodos: estudio descriptivo, retrospectivo y transversal de un programa de telemedicina desarrollado por un equipo de especialistas en Pediatría y sus Áreas Específicas durante el estado de alarma. Se recogieron datos demográficos, número y motivos de consultas según signos, síntomas y su forma de presentación (texto, foto o vídeo). Se analizó el número de consultas resueltas, derivaciones y el grado de satisfacción.
Resultados: se atendió un total de 182 consultas realizadas en su mayoría por mujeres (71%), durante las primeras semanas del confinamiento (70%). El 100% fueron mensajes de texto, acompañados casi en un tercio de los casos de material audiovisual (27,2% fotos, 4,6% vídeos). La edad media de los pacientes atendidos fue de 2,72 ± 2,74 y los principales motivos de consulta: fiebre, exantemas y dificultad respiratoria. El 18,13% tuvo relación con la COVID-19, y solamente el 8,24% fue derivado.
Conclusiones: aunque la telemedicina no puede reemplazar la valoración presencial y todavía existen limitaciones técnicas y legales, nuestros resultados sugieren que podría ser una alternativa prometedora para mejorar el acceso, reducir los tiempos de triaje, coordinar los recursos disponibles, y disminuir el riesgo de contagio y saturación de las instalaciones sanitarias.
Palabras clave
● COVID-19 ● Pandemia ● TelemedicinaINTRODUCCIÓN
Desde que la Organización Mundial de la Salud declaró la pandemia por el coronavirus SARS-CoV-2 (COVID-19) en marzo de 2020, su evolución y extensión a nivel mundial ha puesto a prueba la capacidad del sistema sanitario de decenas de países.
Para evitar el colapso y dar respuesta al incremento exponencial de casos, nuestro sistema sanitario ha sufrido una reorganización sin precedentes, priorizando la atención de los pacientes con sintomatología COVID-19 y limitando la asistencia hospitalaria no urgente para minimizar el riesgo de infección. En caso concreto de los pacientes pediátricos, en la Comunidad de Madrid se centralizó la atención pediátrica en dos hospitales. Esta redistribución ha tenido como consecuencia directa una reducción extraordinaria en la disponibilidad de atención médica, y ha obligado al personal sanitario a enfrentarse a nuevos desafíos éticos.
En este contexto, profesionales, centros sanitarios y sociedades científicas han dado un paso adelante en la comunicación con la población, aumentando de forma considerable su presencia en redes sociales (RR. SS.) y generalizando el uso de las tecnologías de información y comunicación para superar las barreras existentes en la atención de pacientes durante la crisis sanitaria.
La salud digital (eSalud, e-Health) supone un concepto amplio que incluye entre otros servicios de telesalud, la telemedicina (atención directa a pacientes con fines diagnósticos y tratamiento), el telediagnóstico y la teleducación.
El uso de telemedicina para dar cobertura a los pacientes pediátricos se presenta como una alternativa útil en la era pos-COVID. La teleconsulta permite el acceso a la sanidad de niños desatendidos desde el punto de vista médico de una forma rápida, precisa y segura, disminuyendo el riesgo de transmisión y contagio de enfermedades infecciosas1-5. Aunque existen algunas dudas relacionadas con la privacidad y confidencialidad,, cada vez hay mayor evidencia respecto a la efectividad de la intervención médica basada en vídeo o audioconsulta para una gran variedad de urgencias pediátricas2.
Tanto los pacientes como sus familias han comprendido la necesidad de realizar gran parte de sus consultas médicas de forma remota (mensajes de texto, videoconferencias o llamadas telefónicas). Sin embargo, salvo por algunas recomendaciones, no ha existido un protocolo unificado de comunicación con los pacientes durante la pandemia, y cada centro o profesional lo ha realizado según los recursos disponibles.
El servicio de mensajería de Twitter es rápido, fiable, barato, y permite la comunicación directa desde diversos dispositivos, sin necesidad de respuesta inmediata y con posibilidad de intercambiar mensajes, adjuntar archivos, hacer una llamada o establecer una videoconferencia, con un nivel aceptable de calidad y seguridad.
El objetivo del presente estudio es describir la utilidad del servicio de mensajería de Twitter en el triaje pediátrico telemático para evitar visitas innecesarias a los centros hospitalarios y solucionar problemas de salud menores en niños que no precisan atención médica presencial, durante el periodo de tiempo que ha durado el estado de alarma y la reorganización de la atención urgente en la Comunidad de Madrid.
MATERIAL Y MÉTODOS
Estudio descriptivo, retrospectivo y transversal sobre la utilidad del servicio de mensajería de Twitter, como herramienta de telemedicina para el cribado de patología urgente en Pediatría durante los meses en los que se ha mantenido el estado de alarma en España para afrontar la situación de emergencia sanitaria provocada por la COVID-19.
Diseño del Programa de Telemedicina
Reclutamos un equipo constituido por facultativos especialistas y residentes en Pediatría y sus áreas específicas de un hospital terciario y de dos centros de Atención Primaria de la Comunidad de Madrid.
Todos los miembros del equipo fueron entrenados mediante simulación, para familiarizarse con el uso de la red social y realizar interacciones virtuales con posibles pacientes. El proceso de formación incluyó la revisión de diversos aspectos legales relacionados con la asistencia, confidencialidad y privacidad del paciente, insistiendo en la necesidad de responder exclusivamente a los mensajes privados. Esta forma de interacción requiere que el potencial paciente/representante legal solicite tu contacto y aprobación para el envío de información, lo cual, desde el punto de vista legal, podría entenderse como un consentimiento expreso e interesado, al enviar voluntariamente sus datos para obtener una orientación profesional. Además, permite la posibilidad de enviar archivos multimedia (fotos y vídeos) y mejorar la toma de decisiones.
Se diseñó un cuadrante de turnos que permitiera la atención de las consultas en el menor tiempo posible durante 24 horas, y un grupo de WhatsApp con todos los miembros del equipo para interconsultar dudas sobre alguna subespecialidad concreta.
Se establecieron tres turnos al día, en cada uno de los cuales había un residente que filtraba las preguntas y un especialista que supervisaba todos los casos atendidos.
Difusión del Programa de Telemedicina
Se creó una cuenta en Twitter seleccionando como nombre Equipo Pediatría HCSC (@EquipoHCSC), y creamos un perfil dirigido a que los usuarios de esta red social conocieran el objetivo de la cuenta y las condiciones, antes de acceder de forma espontánea y voluntaria al servicio de telemedicina. Reflejamos en la biografía el propósito fundamental de la cuenta: “Resolvemos tus dudas por mensaje privado para evitar visitas innecesarias a urgencias mientras dure el estado de alarma por COVID-19”, y fijamos un tuit explicativo para que los pacientes supieran que las consultas debían realizarse mediante mensajes privados.
Una vez creado el perfil, se realizó una campaña de difusión audiovisual a través de RR. SS., categorizando el tema mediante diversos hashtags: “#COVID19”, “#QuedateEnCasa”, “#confinamiento”, “#telemedicina”, “#SomosClinico”, “#YoMeQuedoEnCasa”, etc., y mencionando a las principales sociedades científicas @aepediatria, @aepap, @SEPEAP, @lasecip…
Programa de Telemedicina
En cada una de las consultas se realizó en primer lugar un triaje telemático con preguntas estandarizadas relacionadas con el triángulo de evaluación pediátrica: estado general y aspecto, respiración y coloración de piel.
Según el motivo de consulta y el triaje:
- Si la consulta era de carácter clínico y se consideraba que no precisaba atención urgente, se respondía la duda y se daban indicaciones acerca de los signos de alarma a vigilar dejando claro que, si aparecían, debían volver a consultar o acudir directamente al servicio de urgencias para valoración presencial.
- Si la consulta era de carácter clínico y se consideraba la necesidad de atención urgente, se derivaba a los centros disponibles según la comunidad autónoma.
- Si el motivo de la consulta no tenía un carácter puramente clínico (puericultura o medidas de Salud Pública relacionadas con la pandemia), se intentó documentar y derivar a fuentes fiables (páginas web de sociedades científicas, blogs profesionales, etc.) donde conseguir información relacionada con su pregunta.
Valoración del Programa de Telemedicina
Desde el 14 de marzo de 2020 hasta la reanudación de asistencia pediátrica se recogieron todos los mensajes privados enviados al perfil @EquipoHCSC. Se recogieron datos demográficos del paciente y del familiar responsable del contacto, fecha y motivo de consulta, así como el número de veces que solicitaron el servicio.
Para el análisis de los datos se clasificaron en función de los signos y síntomas. También se tuvo en cuenta si se acompañaban o no de archivo multimedia (foto o vídeo), y si la consulta estaba relacionada con la COVID-19. Se analizó el número de consultas resueltas, y aquellas que precisaron derivación al servicio de urgencias para valoración presencial.
Finalmente se valoró el grado de satisfacción con la atención recibida mediante un cuestionario de satisfacción que establecía una puntuación entre 0 (mínimo grado de satisfacción) y 10 (máximo nivel de satisfacción), días después de la consulta.
RESULTADOS
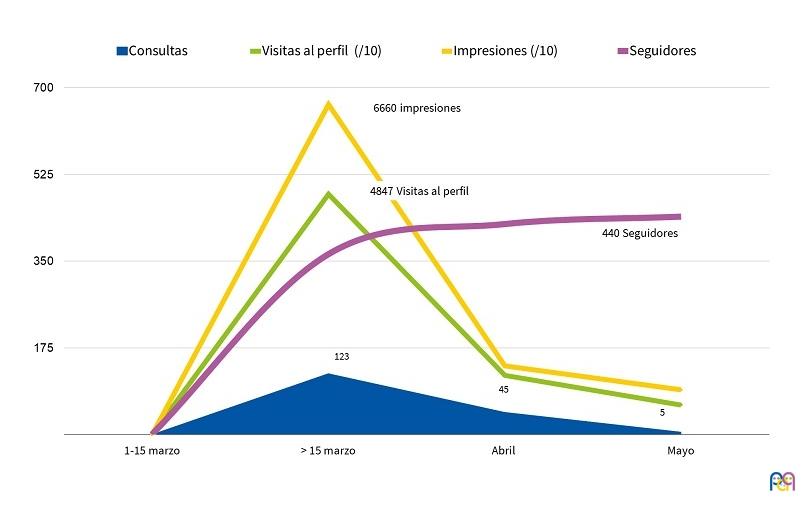
Durante el estado de alarma, @EquipoHCSC obtuvo más de 7000 visitas al perfil y estableció una red de contactos (“Siguiendo”) con las principales sociedades científicas pediátricas y los perfiles individuales relacionados con más “seguidores”, alcanzando un total de 443 seguidores al final del confinamiento.
Se atendieron un total de 182 consultas realizadas por 138 personas diferentes. Hasta 35 familias realizaron más de una consulta por diferentes motivos y en distintos momentos a lo largo del estudio.
El 71% de los usuarios fueron mujeres, y en la mayoría de los casos, la madre del paciente. El 70% del total de las consultas se realizaron en los primeros 15 días de la creación del perfil. El 49% en la primera semana y el 18,8% durante la segunda, cayendo estas progresivamente a medida que mejoraba la situación. Las características y evolución del perfil durante la cuarentena se detallan en la Fig. 1.
| Figura 1. Características y evolución del perfil de Twitter durante la cuarentena |
|---|
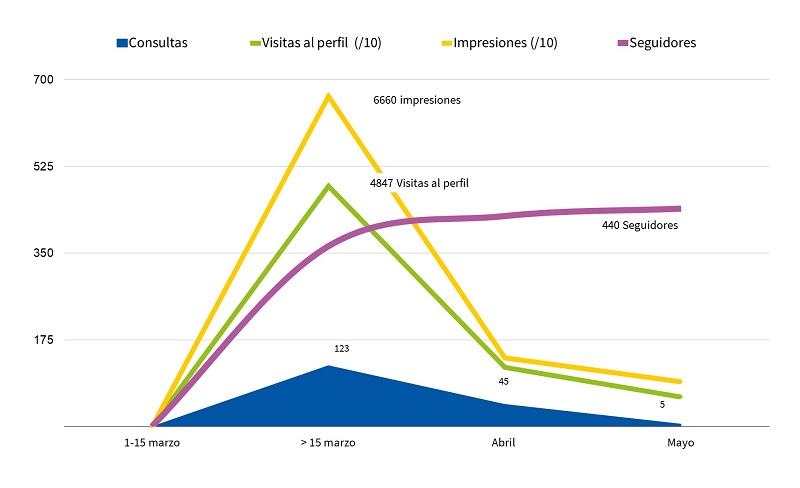 |
Desde el punto de vista clínico, se prestó asistencia sanitaria a 138 pacientes con edades comprendidas entre 2 días y 11 años, con una edad media de 2,72 ± 2,74 (rango intercuartílico: 3,58 años). El 31,8% completó la descripción de la semiología clínica con material audiovisual (27,2% foto, 4,6% vídeo).
Según el motivo de consulta y el triaje inicial, el 82,8% de las consultas realizadas tuvieron un perfil puramente clínico y el 17,2% restante fueron dudas de puericultura.
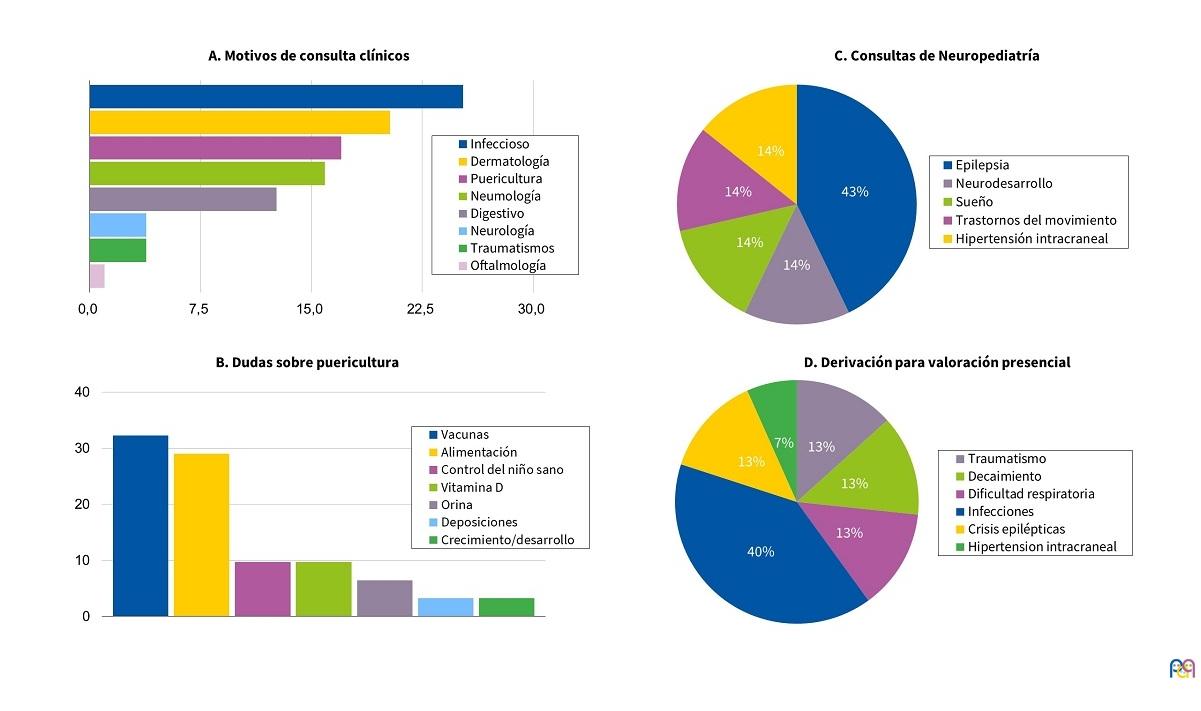
Al analizar los mensajes por grupos clínicos, los principales motivos de consulta estuvieron relacionados con enfermedades infecciosas (25,3%), problemas dermatológicos (20,3%), puericultura (17,0%), neumología (15,9%), digestivo (12,6%), neurología (3,8%), patología traumática (3,8%) y oftalmológica (1,0%).
El motivo de consulta más frecuente fue la fiebre, seguido por la aparición brusca de exantemas cutáneos y dificultad respiratoria. Estos tres síntomas representaban además la mayoría de los motivos de consulta por causa infecciosa, dermatológica y respiratoria.
Los grupos clínicos con mayor variedad respecto a las consultas realizadas fueron la Pediatría general y la Neuropediatría. Solo el 18,1% de las consultas estuvieron relacionadas con la COVID-19.
De todos los pacientes atendidos, solo el 8,2% tuvieron que ser derivados para valoración presencial.
Las características clínicas de los mensajes recibidos se detallan en la Fig. 2.
| Figura 2. Características clínicas de las consultas y motivos principales para valoración presencial |
|---|
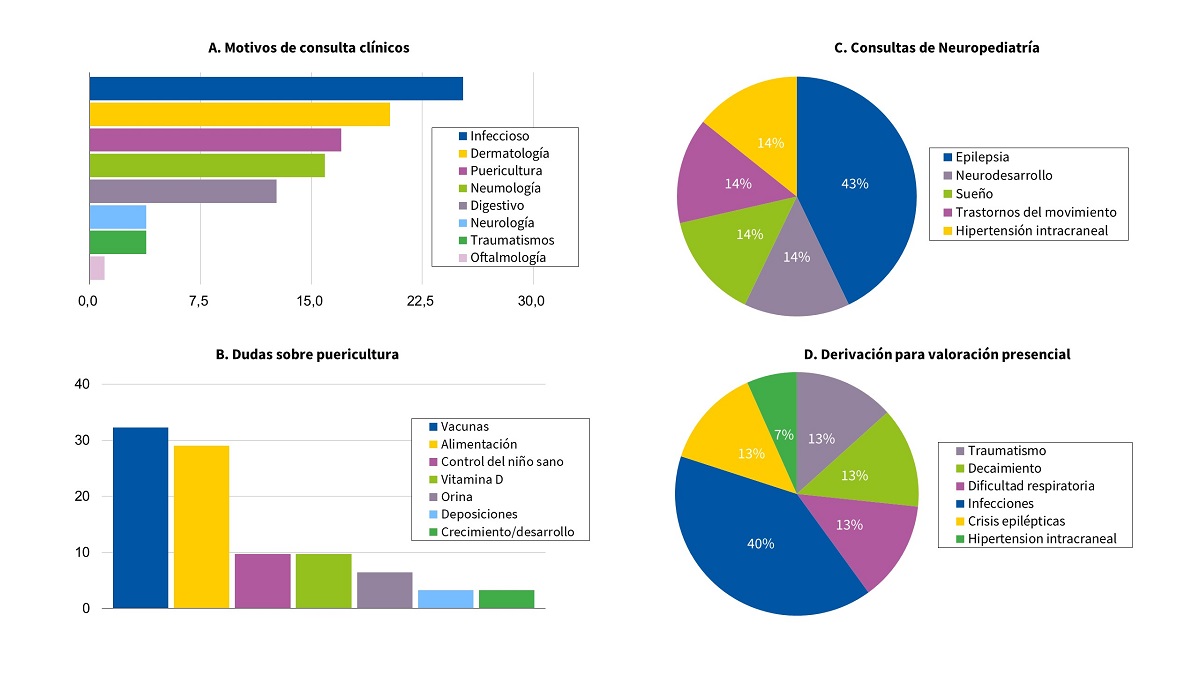 |
Todas las consultas fueron atendidas y resueltas mediante mensajes multimedia (texto, foto o vídeo), siendo muy variable el número de mensajes necesarios en cada conversación según el motivo de consulta, la descripción inicial del caso y el nivel de angustia familiar. El tiempo medio de respuesta fue de 9,9 minutos.
Respecto al nivel de satisfacción, el 87,6% de los usuarios mostraron activamente su satisfacción con la iniciativa y atención recibida, obteniendo una puntuación media de 7,8 ± 1,7 puntos sobre 10.
DISCUSIÓN
España dispone de un Sistema Nacional de Salud (SNS) formado por un conjunto de prestaciones sanitarias públicas que garantizan el acceso universal a la atención sanitaria urgente de todos los habitantes.
En el SNS, los usuarios pueden acceder de manera libre y voluntaria a los servicios de urgencias tanto en Atención Primaria como hospitales, garantizando su igualdad. Sin embargo, puede favorecer el hecho de que en muchas ocasiones se realice un mal uso de estos servicios, saturándolos por motivos banales de consulta6,7.
En el caso de la asistencia pediátrica urgente, los padres eligen con frecuencia los servicios de urgencias, ya sea por motivos laborales, libertad de horarios o simplemente por comodidad. Se estima que una gran parte de estas visitas son evitables.
Durante la pandemia por coronavirus nuestro sistema sanitario ha sufrido una reorganización sin precedentes, priorizando la atención de los pacientes con sintomatología COVID-19 y limitando la asistencia hospitalaria no urgente para minimizar el riesgo adicional de infección5.
En este contexto, la telemedicina se ha posicionado como una herramienta de primera línea para salvar las barreras existentes en la atención urgente, descongestionar el sistema de salud, facilitar el acercamiento de los pacientes a los profesionales y disminuir la propagación del virus con visitas innecesarias al hospital8.
Los resultados clínicos publicados muestran la utilidad de la telemedicina para el diagnóstico de enfermedades agudas pediátricas comunes, en relación con la reproducibilidad del diagnóstico respecto a las consultas presenciales, el índice de satisfacción del paciente, así como en una posible reducción de los costos de la atención3,4,9. En nuestro estudio, utilizamos Twitter por ser una red social extendida que dispone de un servicio de mensajería que nos permitía la interacción directa con otros usuarios de forma rápida, privada y con un nivel bastante aceptable de calidad y seguridad.
Las interacciones con el perfil fueron rápidas. En los primeros 15 días del estado de alarma se produjo un incremento exponencial en el número de seguidores y se realizaron la mayor parte de las consultas. Esta buena respuesta posiblemente fue debida a que coincidió con el periodo de tiempo de mayor incertidumbre y miedo a la situación epidemiológica, y con la reestructuración de la atención urgente en Pediatría en la Comunidad de Madrid.
De forma similar a lo descrito en la bibliografía, los procesos infecciosos fueron el motivo de consulta más frecuente, seguidos por consultas relacionadas con problemas cutáneos y puericultura10. Cabe destacar que casi un tercio de los pacientes (31,8%) envió de forma espontánea archivos de imagen o vídeo para completar la información clínica.
Aunque por los resultados y el nivel de satisfacción obtenidos (el 87,6% de los consultores mostró activamente su satisfacción) consideramos que las decisiones clínicas fueron acertadas, el porcentaje de pacientes derivados a los servicios de urgencias para valoración presencial fue mucho menor de lo descrito en la literatura científica (20-30% descrito frente a nuestro 8%)9. Estos resultados podrían estar justificados por el breve periodo de tiempo y contexto epidemiológico en el que se realizó el estudio.
Aunque consideramos que los resultados respaldan la utilidad de la telemedicina en el triaje de pacientes pediátricos, los resultados deben interpretarse con cautela por varios motivos y limitaciones. En primer lugar, el estudio se realizó durante el peor momento de la pandemia, lo cual pudo favorecer la aceptación de un Programa de Telemedicina realizado a través de RR. SS. Además, no pudimos evaluar la gravedad comparativa de la enfermedad entre las consultas telemáticas frente a las presenciales. Esto podría sesgar los resultados, ya que la gravedad de la enfermedad puede afectar la decisión de utilizar o no la telemedicina. Los pacientes que presentan sintomatología leve podrían considerar innecesaria la consulta, mientras que aquellos con patologías graves o inestables podrían recurrir directamente a los servicios hospitalarios. Por último, aunque no existe una regulación específica y suficientemente detallada en nuestro ordenamiento jurídico, no podemos obviar diversos aspectos éticos o legales de nuestro estudio, ni las dificultades del sistema utilizado para la protección de datos11-13.
Sin embargo, consideramos que la telemedicina era una alternativa razonable en la situación de excepcionalidad que estábamos viviendo. Además, al utilizar un servicio de mensajería privada, podría entenderse que hay un consentimiento del interesado y por tanto expreso de la persona que consulta.
A pesar de todo y teniendo en cuenta que la telemedicina va a suponer más de la mitad de nuestras consultas en los próximos meses, se deberían considerar los desafíos de esta herramienta desde el punto de vista técnico y ético, tanto para los pacientes (seguridad, privacidad y confidencialidad), como para los profesionales médicos responsables de la asistencia.
Nuestros resultados sugieren que la telemedicina podría ser una prometedora alternativa para mejorar el acceso a la sanidad, reducir los tiempos de triaje, coordinar los recursos sanitarios disponibles e incluso, realizar el seguimiento del paciente desde su domicilio evitando desplazamientos innecesarios, disminuyendo el riesgo de contagio y la saturación de las instalaciones sanitarias8,14.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
SS.: redes sociales · SNS: Sistema Nacional de Salud.
BIBLIOGRAFÍA
- Burke BL Jr, Hall RW. Telemedicine: Pediatric Applications. Pediatrics. 2015;136:293-308.
- Mehrotra A. The convenience revolution for treatment of low-acuity conditions. JAMA. 2013;310:35-6.
- McConnochie KM, Conners GP, Brayer AF, Goepp J, Herendeen NE, Wood NE, et al. Differences in diagnosis and treatment using telemedicine versus in-person evaluation of acute illness. Ambul Pediatr. 2006;6:187-95.
- Ray KN, Shi Z, Gidengil CA, Poon SJ, Uscher-Pines l, Mehrotra A. Antibiotic Prescribing During Pediatric Direct-to-Consumer Telemedicine Visits. Pediatrics. 2019;143:e20182491.
- Bloem BR, Dorsey ER, Okun MS. The Coronavirus Disease 2019 Crisis as Catalyst for Telemedicine for Chronic Neurological Disorders. JAMA Neurol. 2020;77:927-8.
- Hostetler MA, Mace S, Brown K, Finkler J, Hernández D, Krug SE, et al. Emergency department overcrowding and children. Pediatr Emerg Care. 2007;23:507-15.
- García de Ribera MC, Bachiller Luque MR, Vázquez Fernández M, Barrio Alonso MP, Hernández Velázquez P, Hernández Vázquez AM. Triaje de urgencias pediátricas en Atención Primaria española mediante teléfono móvil. Análisis de un modelo en un área de salud. Rev Calid Asist. 2013;28:174-80.
- Santos-Peyret A, Durón RM, Sebastián-Díaz MA, Crail-Meléndez D, Gómez-Ventura S, Briceño-González E, et al. E-health tools to overcome the gap in epilepsy care before, during and after COVID-19 pandemics. Rev Neurol. 2020;70:323‐8.
- Harvey JB, Yeager BE, Cramer C, Wheeler D, McSwain SD. The Impact of Telemedicine on Pediatric Critical Care Triage. Pediatr Crit Care Med. 2017;18:555-60.
- Crane JD, Benjamin JT. Pediatric residents’ telephone triage experience: do parents really follow telephone advice? Arch Pediatr Adolesc Med. 2000;154:71-4.
- Recomendaciones del ICOMEM sobre Telemedicina ante la crisis sanitaria. En: Ilustre Colegio Oficial de Médicos de Madrid [en línea] [consultado el 20/01/2022]. Disponible en https://fundadeps.org/wp-content/uploads/2020/04/icomem-telemedicina.pdf
- Muñoz Fernández l, Díaz García E, Gallego Riestra S. Las responsabilidades derivadas del uso de las tecnologías de la información y comunicación en el ejercicio de las profesiones sanitarias. An Ped (Barc). 2020;92:307.
- Bravo Acuña J, Merino Moína M. Uso de nuevas tecnologías en la comunicación con los pacientes, su utilidad y sus riesgos. An Pediatr (Barc). 2020;92:251-2.
- Vidal-Alaball J, Acosta-Roja R, Pastor N, Sánchez U, Morrison D, Narejos S, et al. Telemedicine in the face of the COVID-19 pandemic. Aten Primaria. 2020;52:418-22.