
Vol. 22 - Num. 88
Originales
Alteraciones del metabolismo de los hidratos de carbono en pacientes pediátricos con obesidad
José M.ª Basain Valdésa, M.ª Carmen Valdés Alonsoa, Margarita Pérez Martínezb, Miriam Álvarez Viltresc, Silvia M.ª Marín Juliád
aServicio de Endocrinología. Hospital Pediátrico Docente Juan Manuel Márquez. La Habana. Cuba.
bGinecóloga. Grupo Básico de Trabajo 2. Policlínico Universitario Carlos Manuel Portuondo Lambert. La Habana. Cuba .
cMédico General Integral. Grupo Básico de Trabajo 2. Policlínico Universitario Carlos Manuel Portuondo Lambert. La Habana. Cuba.
dPediatra. Servicio de Endocrinología Pediátrica. Instituto Nacional de Endocrinología. La Habana. Cuba.
Correspondencia: JM Basain. Correo electrónico: josemb@infomed.sld.cu
Cómo citar este artículo: Basain Valdés JM, Valdés Alonso MC, Pérez Martínez M, Álvarez Viltres M, Marín Juliá SM. Alteraciones del metabolismo de los hidratos de carbono en pacientes pediátricos con obesidad. Rev Pediatr Aten Primaria. 2020;22:371-8.
Publicado en Internet: 02-12-2020 - Número de visitas: 13888
Resumen
Introducción: la elevada prevalencia de la obesidad en las edades pediátricas plantea el desarrollo de comorbilidades, dentro de las cuales se encuentran las alteraciones glucídicas. Objetivo: determinar si existe alteración glucídica en pacientes pediátricos con obesidad.
Material y método: estudio descriptivo, transversal, en 76 pacientes pediátricos con diagnóstico de obesidad atendidos en el Servicio de Endocrinología del Hospital Juan Manuel Márquez (La Habana, Cuba), en el periodo de enero de 2015 a enero de 2019. Las variables en estudio fueron: edad, sexo, tipo de prediabetes, tiempo de evolución y grado de obesidad. Las variables cualitativas se describieron estadísticamente mediante frecuencias absolutas y relativas, la asociación entre las variables categóricas se exploró con el test χ2 y la probabilidad exacta de Fisher. En todas las pruebas estadísticas se consideró un nivel de significación de α igual a 0,05.
Resultados: el 71,05% de los pacientes presentaron prediabetes, de los cuales el 40,59% pertenecían al sexo femenino y el 72,22% eran mayores de 10 años de edad. Predominaron los pacientes con TGA (70,37%), de los cuales el 50,0% eran mayores de 10 años de edad y el 37,04% eran del sexo femenino. El tiempo de evolución de la obesidad no resultó significativo y se constató un incremento de la prediabetes a mayor grado de la obesidad (p = 0,0095).
Conclusiones: se presentaron alteraciones del metabolismo de los hidratos de carbono expresadas por la presencia de prediabetes. Predominó el sexo femenino. No existió asociación entre la prediabetes con el tiempo de evolución de la obesidad, pero sí con el grado de obesidad.
Palabras clave
● Malnutrición ● Obesidad ● PrediabetesINTRODUCCIÓN
Durante los últimos años, han ocurrido modificaciones en el perfil epidemiológico, entre las que destacan una disminución de las enfermedades de origen infeccioso y un progresivo incremento de las enfermedades crónico-degenerativas no transmisibles, como la obesidad y sus complicaciones1, las cuales aparecen cada vez en edades más tempranas, y son visibles en niños y adolescentes (problemas psicológicos, de adaptación social, ortopédicos, hiperlipidemia, hipertensión, apneas del sueño, entre otros)2.
La inflamación inducida por la obesidad juega un papel importante en el desarrollo de la resistencia a la insulina, sin embargo, a fecha de hoy aún se desconoce si la inflamación del tejido adiposo es una causa o una consecuencia de la resistencia a la insulina3.
Estimaciones de 34 países miembros de la Organización para la Cooperación Económica y Desarrollo muestran que el 21% de las niñas y el 23% de los niños tienen sobrepeso4. Según los datos de la Encuesta Nacional de Salud y Nutrición (NHANES), realizada en EE. UU., la obesidad alcanza una prevalencia del 9,5% en niños y niñas 0-2 años de edad, mientras que la prevalencia para los niños de 2-19 años de edad fue de 16,9% en ambos sexos5.
Debido a que la diabetes puede evolucionar por años de forma poco manifiesta, el 46% de quienes la padecen no están al tanto de su enfermedad; incluso existe un grupo de pacientes que, a pesar de no cumplir los criterios para el diagnóstico de diabetes, tienen cifras de glucemia demasiado elevadas como para ser consideradas normales y presentan incremento del riesgo de desarrollar diabetes mellitus (DM)6. Esta situación de disglucemia se conoce como prediabetes.
Se postula que, en la transición de un individuo normal a un intolerante y luego a un diabético, la sensibilidad a la insulina se deteriora aproximadamente un 40%, mientras la secreción de la insulina se deteriora de 3 a 4 veces7. Actualmente el empleo de nuevos conceptos, como el de la programación epigenética de la expresión de los genes, la composición corporal in utero y en la niñez temprana ofrecen una explicación más adecuada a la interrelación existente entre la obesidad y la DM tipo 2 (DM2), por lo que se ha acuñado el término “diabesidad” para hablar de este problema. El sustrato en que se basa dicha interrelación está dado porque el tejido adiposo se considera un verdadero órgano endocrino, el cual secreta adipoquinas, que presentan una función endocrina variada, y enzimas, como las aromatasas y la 11-beta-hidroxiesteroide-deshidrogenasa (11-β-HSD), que participan activamente en la regulación hormonal. En pacientes obesos se observa una sobreexpresión de la actividad de la 11-β-HSD, lo que se asocia a hipertensión arterial, resistencia a la insulina y dislipidemia, entre otros problemas de salud. Estas alteraciones se relacionan, sobre todo, con el aumento de la grasa abdominal, y esta facilita el establecimiento de estados conocidos como disglucémicos, que comprenden diversos grados de alteraciones del metabolismo de la glucosa8.
La DM2 se considera el resultado del estado de inflamación crónica de bajo grado presente en la obesidad. Sin embargo, los mecanismos que unen a la inflamación sistémica de bajo grado con la obesidad y la DM2 son poco conocidos, aunque diversos mecanismos han sido investigados, como la microbiota intestinal, que tiene un papel importante durante la obesidad al incrementarse la permeabilidad intestinal, lo que resulta en un aumento en los niveles circulantes de lipopolisacáridos (LPS) provenientes de bacterias grampositivas del intestino. Los LPS pueden iniciar una cascada proinflamatoria mediante la activación de receptores de reconocimiento de patrones como TLR4 (receptor de LPS) en adipocitos, que produce inflamación sistémica de bajo grado, resistencia a la insulina y finalmente DM29.
La asociación obesidad-resistencia a la insulina es, con toda probabilidad, una relación de causa-efecto, como se demuestra en los estudios que indican que la ganancia-pérdida de peso se correlaciona de manera indudable con la reducción-incremento de la sensibilidad a la insulina, respectivamente10.
La prediabetes es un término antiguo acuñado por la Organización Mundial de la Salud como un diagnóstico retrospectivo, que describía el estado de una persona previo al diagnóstico de DM11. En la actualidad, la Asociación Americana de Diabetes incorpora al concepto con implicaciones prospectivas, en que un nivel establecido de glucemia o glucemia postsobrecarga pronostica la futura conversión de estas personas con estas cifras de glucemia al estadio “prediabético”, de pasar a ser diabéticos reales o a tener un mayor riesgo de complicaciones cardiovasculares12.
El término disglucemia comprende varias categorías, como la glucemia alterada en ayunas (GAA), la tolerancia a la glucosa alterada (TGA), la prediabetes mixta o prediabetes doble (que incluye la combinación de GAA/TGA) y la diabetes mellitus propiamente dicha. Se considera GAA cuando la glucemia en ayunas se encuentra mayor a 5,6 mmol/l y menor a 7,1 mmol; TGA cuando la segunda hora en una prueba de tolerancia oral a la glucosa, la glucemia se encuentra entre 7,8 y 11 mmol/l, y doble prediabetes cuando se cumplen los criterios de GAA y TGA al unísono8. La duración de esta afección es variable, debido a que está directamente ligada a su historia natural y se estima de 7 a 10 años. Del total de la población prediabética existente, el 70% evolucionará hacia la enfermedad diabética11.
El término TGA fue introducido en 1979 y refleja una resistencia periférica a la acción de la insulina; por su parte, la GAA surgió en 1997, expresa una elevación de la síntesis hepática de glucosa y un defecto en la secreción precoz de insulina. Ambas se consideran estados intermedios entre la tolerancia normal a la glucosa y la DM11.
Varios estudios epidemiológicos han sugerido que la reducción de la cifra normal de glucemia en ayunas a 5,6 mmol/l podría optimizar la sensibilidad y la especificidad de la prueba para predecir la probabilidad de padecer DM2, lo que ha permitido introducir el término de disglucemia de ayuno, sobre todo cuando se asocia a obesidad e hipertrigliceridemia. La disglucemia de ayuno, como expresión de la resistencia a la acción de la insulina a nivel hepático, muestra una correlación aproximada de 70% con la resistencia periférica a la hormona13.
Frente a la situación mundial y nacional antes descrita, es que nos surgió la siguiente interrogante: ¿cuál es el comportamiento de la intolerancia a los hidratos de carbono en pacientes pediátricos obesos atendidos en la consulta especializada de obesidad del Servicio de Endocrinología Pediátrica del Hospital Pediátrico Docente Juan Manuel Márquez durante el periodo comprendido de enero del 2015 enero del 2019?
El objetivo de la presente investigación fue determinar alteraciones del metabolismo de los hidratos de carbono en pacientes pediátricos con obesidad atendidos en la consulta especializada de obesidad del Servicio de Endocrinología Pediátrica del Hospital Pediátrico Docente Juan Manuel Márquez durante el periodo comprendido de enero del 2015 enero del 2019.
MATERIAL Y MÉTODOS
Se realizó un estudio descriptivo y de corte transversal en 76 pacientes con diagnóstico de obesidad según criterios de la Organización Mundial de la Salud (N = n = 76), de ambos sexos, en edades comprendidas entre 1 y 18 años, atendidos en la consulta especializada de obesidad en el servicio de Endocrinología del Hospital Pediátrico Docente Juan Manuel Márquez en el periodo de enero del 2015 a enero del 2019. La muestra quedó conformada por 76 pacientes distribuida de la siguiente manera: 38 pacientes menores de diez años de edad y 38 pacientes mayores o iguales a diez años de edad. Se excluyeron aquellos pacientes con presencia de enfermedades genéticas o endocrinas-metabólicas, obesidad de causa medicamentosa y los que las historias clínicas no contaran con todos los datos necesarios para la presente investigación.
Las variables estudiadas fueron edad, sexo, presencia de prediabetes, tipo de prediabetes, tiempo de evolución de la obesidad y grado de obesidad. De las historias clínicas de los pacientes se obtuvieron los siguientes datos: edad, sexo y tiempo de evolución de la obesidad. A todos los pacientes se les realizó las mediciones antropométricas de peso y talla, y posteriormente se les monitorizó la glucemia en ayunas, y la glucemia a las dos horas.
A partir de los valores de peso y talla, se calculó el índice de masa corporal (IMC) según la fórmula de Quetelet: IMC = peso del paciente (kg)/talla del paciente (m2). A partir de los valores del IMC, se ubicó al paciente según sexo en la tabla cubana de percentiles de IMC según edad y sexo correspondiente y se determinó el percentil al que correspondía. Se consideró obesidad cuando se encontró por encima del 97 percentil de acuerdo con el sexo según las tablas cubanas.
Las muestras de laboratorio fueron obtenidas por punción venosa en el laboratorio clínico del Hospital Pediátrico Docente Juan Manuel Márquez, después de 12 horas de ayuno. Las determinaciones de glucemia fueron realizadas en el laboratorio de dicha institución mediante el método de la glucosa oxidasa.
Para el procesamiento de la información, los datos fueron incluidos en una base de datos automatizada con la hoja de cálculo electrónica Excel 2003. Las variables se resumieron estadísticamente mediante cifras frecuencias absolutas y porcentajes. La asociación entre las variables categóricas se identificó con la prueba exacta de Fisher y χ2 de independencia, donde se consideró significativo sí p <0,05. Desde el punto de vista bioético, se solicitó el consentimiento informado a todos los padres o tutores legales, y la investigación fue aprobada por el comité científico y el comité de ética de la investigación del hospital.
RESULTADOS
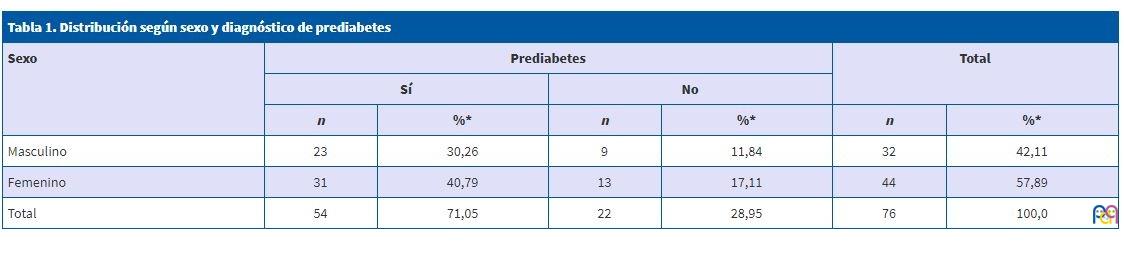
En la Tabla 1 se muestra la distribución según sexo y diagnóstico de prediabetes. De los pacientes estudiados, el 71,05% presentaron prediabetes y el sexo femenino predominó con un 40,79%.
| Tabla 1. Distribución según sexo y diagnóstico de prediabetes | ||||||
|---|---|---|---|---|---|---|
| Sexo | Prediabetes | Total | ||||
| Sí | No | |||||
| n | %* | n | %* | n | %* | |
| Masculino | 23 | 30,26 | 9 | 11,84 | 32 | 42,11 |
| Femenino | 31 | 40,79 | 13 | 17,11 | 44 | 57,89 |
| Total | 54 | 71,05 | 22 | 28,95 | 76 | 100,0 |
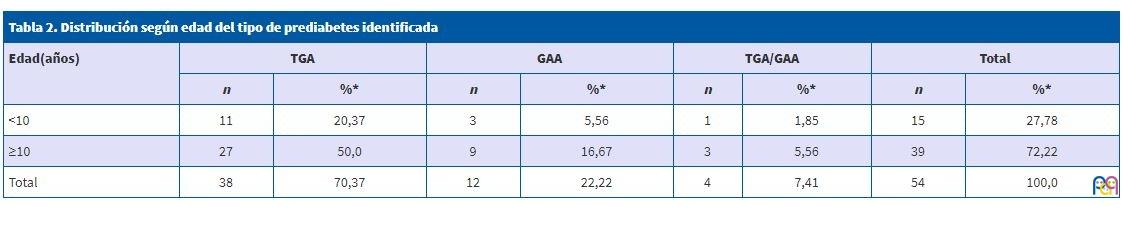
La distribución según edad del tipo de prediabetes identificada se muestra en la Tabla 2. No se encontraron valores significativos (p = 0,9572) entre la edad y el tipo de prediabetes; no obstante, el 70,37% de los pacientes estudiados presentaron una TGA, el 22,22% resultaron con una GAA y un porcentaje mínimo (7,41%) presentó una doble prediabetes.
| Tabla 2. Distribución según edad del tipo de prediabetes identificada | ||||||||
|---|---|---|---|---|---|---|---|---|
| Edad(años) | TGA | GAA | TGA/GAA | Total | ||||
| n | %* | n | %* | n | %* | n | %* | |
| <10 | 11 | 20,37 | 3 | 5,56 | 1 | 1,85 | 15 | 27,78 |
| ≥10 | 27 | 50,0 | 9 | 16,67 | 3 | 5,56 | 39 | 72,22 |
| Total | 38 | 70,37 | 12 | 22,22 | 4 | 7,41 | 54 | 100,0 |
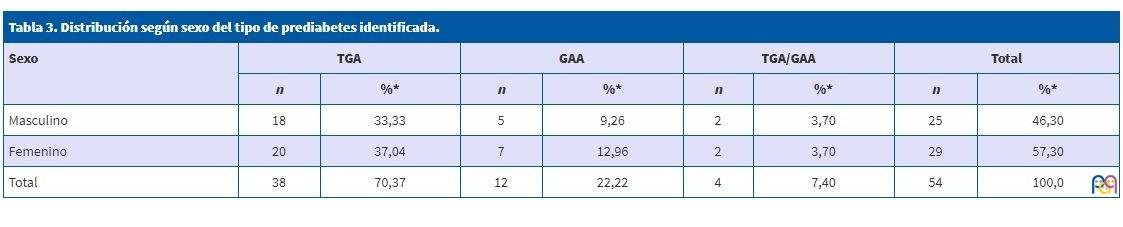
En la Tabla 3 se muestra la distribución según sexo del tipo de prediabetes identificada. Como se puede observar, no existieron valores significativos entre estas dos variables estudiadas.
| Tabla 3. Distribución según sexo del tipo de prediabetes identificada. | ||||||||
|---|---|---|---|---|---|---|---|---|
| Sexo | TGA | GAA | TGA/GAA | Total | ||||
| n | %* | n | %* | n | %* | n | %* | |
| Masculino | 18 | 33,33 | 5 | 9,26 | 2 | 3,70 | 25 | 46,30 |
| Femenino | 20 | 37,04 | 7 | 12,96 | 2 | 3,70 | 29 | 57,30 |
| Total | 38 | 70,37 | 12 | 22,22 | 4 | 7,40 | 54 | 100,0 |
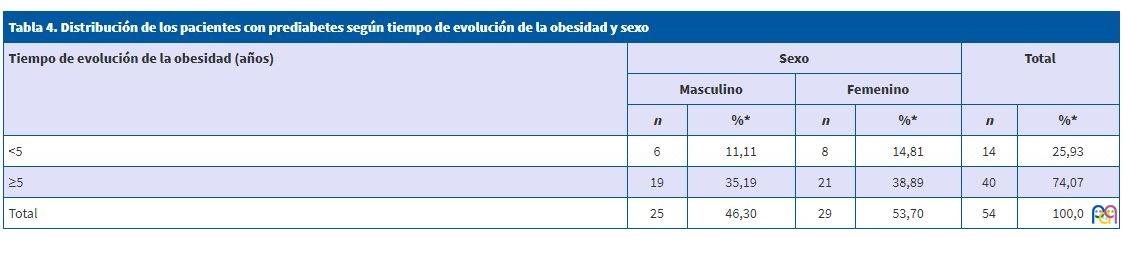
La distribución de los pacientes con prediabetes según el tiempo de evolución de la obesidad y sexo se muestra en la Tabla 4. Con relación al tiempo de evolución de la obesidad no resultó significativa (p = 0,7640) la alteración de la glucosa.
| Tabla 4. Distribución de los pacientes con prediabetes según tiempo de evolución de la obesidad y sexo | ||||||
|---|---|---|---|---|---|---|
| Tiempo de evolución de la obesidad (años) | Sexo | Total | ||||
| Masculino | Femenino | |||||
| n | %* | n | %* | n | %* | |
| <5 | 6 | 11,11 | 8 | 14,81 | 14 | 25,93 |
| ≥5 | 19 | 35,19 | 21 | 38,89 | 40 | 74,07 |
| Total | 25 | 46,30 | 29 | 53,70 | 54 | 100,0 |
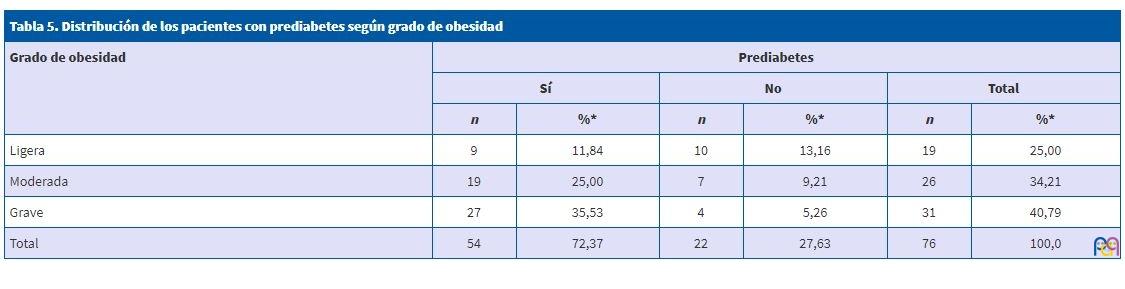
En la Tabla 5 se muestra la distribución de los pacientes con prediabetes según el grado de obesidad. Existieron valores significativos (p = 0,0095) entre estas dos variables.
| Tabla 5. Distribución de los pacientes con prediabetes según grado de obesidad | ||||||
|---|---|---|---|---|---|---|
| Grado de obesidad | Prediabetes | |||||
| Sí | No | Total | ||||
| n | %* | n | %* | n | %* | |
| Ligera | 9 | 11,84 | 10 | 13,16 | 19 | 25,00 |
| Moderada | 19 | 25,00 | 7 | 9,21 | 26 | 34,21 |
| Grave | 27 | 35,53 | 4 | 5,26 | 31 | 40,79 |
| Total | 54 | 72,37 | 22 | 27,63 | 76 | 100,0 |
DISCUSIÓN
Existe un bajo número de artículos nacionales en los que se pueda extraer conclusiones sobre prevalencia de prediabetes. González Tabares et al.6 consideran que esto se debe a que el diagnóstico del estado glucémico no se realiza en un solo paso, sino que es un proceso en el que intervienen varios instrumentos: glucemia en ayunas, prueba de tolerancia a la glucosa oral y más recientemente hemoglobina glucosilada A1C. La mayoría de los estudios disponibles se basan en declaración del paciente y no en investigación o pruebas. Según este principio, una serie secular para la provincia de Ciego de Ávila aporta una prevalencia de DM muy baja, de solo 2,89%, y de prediabetes no aporta datos14.
En una investigación con 50 pacientes prediabéticos, pertenecientes al poblado de Boniato, en la provincia de Santiago de Cuba, realizada por Girón Bombull et al.11, encuentran que predomina el sexo femenino con un 92,0%, lo que coincide con González et al.15, quienes encuentran que, de los 40 casos de la serie estudiada, 29 correspondieron al sexo femenino, resultados similares a los de la presente investigación.
En 2009, en un estudio que realizan Valdés et al.16 encuentra que predomina la TGA con respecto a la GAA. Asimismo, la Asociación Americana de Diabetes17 considera que la GAA es mejor para definir el riesgo de DM.
En una investigación que realizan Girón Bombull et al.11 en 2012, en el poblado de Boniato de Santiago de Cuba, encuentra que prevalece la intolerancia a la glucosa en ayunas en un 64,0%.
La prevalencia de la glucemia en ayunas alterada hallada en la investigación realizada por Bustillo Solano et al.18 sobre prevalencia de la diabetes mellitus y de la GAA en un área de la ciudad de Sancti Spíritus fue de un 25,22%.
En la búsqueda electrónica de la información biomédica no existen otras investigaciones publicadas de prevalencia de la GAA en otras ciudades o provincias en Cuba.
En un estudio reciente efectuado en cuatro ciudades de la India, la prevalencia de la GAA o de la TGA osciló entre el 8,1 y el 14,6%19.
No está bien establecido si la TGA y la GAA son dos etapas de un proceso continuo que va desde la tolerancia a la glucosa normal hasta la DM2, o si son dos fenotipos diferentes de deterioro de la tolerancia a la glucosa20. Los estudios son discordantes en relación al diagnóstico de estos dos estados, la mayor frecuencia de GAA detectada en el estudio coincide con investigaciones desarrollados en varias poblaciones como EE. UU., China, Dinamarca, India21 y en Cuba, con la investigación desarrollada en el municipio de Centro Habana, donde se encuentra que el 16,1% de la muestra estudiada presenta glucemia en ayunas alterada22, mientras que en una investigación en Sancti Spíritus se reporta una alta cifra de GAA de un 25,22%18. Estos resultados coinciden con los resultados obtenidos en la presente investigación.
En este estudio se encontró mayor número de pacientes de ambos sexos con prediabetes y ninguno presentó diabetes mellitus, así como incremento paralelo con la edad, con predominio de la GAA, algo que está en correspondencia con lo que plantean Arteaga et al.23, pero que difiere de lo que reportan Alayón et al.24 en Cartagena de Indias, donde se encuentra que la DM presenta una mayor prevalencia.
En un estudio realizado por Díaz Díaz et al.8 en 1982 pacientes que asistían a las consultas del Instituto Nacional de Endocrinología por sospecha de diabetes mellitus tipo 2, encuentra que, en el sexo masculino, las disglucemias más frecuentes son la GAA, en 95 pacientes (20,9%) del total de la muestra, seguida por la DM en 60 pacientes (13,2%), la prediabetes mixta o doble en 38 pacientes (8,4%) y TGA en 25 pacientes (5,55%), mientras que la disglucemia más frecuente en el sexo femenino fue la GAA, en 36 pacientes (6,9%) del total de la muestra, seguida por la TGA en 31 pacientes (5,9%), la prediabetes mixta o doble en 24 pacientes (4,6%) y la DM en 19 pacientes (3,6%).
Japón estudia la influencia de la glucemia, y realiza a sujetos normoglucémicos un test de tolerancia y separándolos por cuartiles, donde encuentra que, a más niveles de glucosa, mayor correlación con obesidad25.
En Trujillo, en el 2011, Castillo et al.26, en un estudio poblacional en adultos, encuentran que, con el aumento de la glucosa alterada en ayunas, se incrementa gradualmente el IMC.
Los resultados obtenidos en este trabajo apuntan hacia la necesidad de la búsqueda activa de prediabetes; lo cual constituye un punto de partida para iniciar la investigación de esta alteración del metabolismo de los hidratos de carbono y comenzar desde la Atención Primaria de Salud a trazar pautas para la prevención de la misma.
CONCLUSIONES
Se presentaron alteraciones del metabolismo de los hidratos de carbono expresadas por la presencia de prediabetes. Predominó el sexo femenino y las edades mayores o iguales a diez años. No existió asociación entre la prediabetes con el tiempo de evolución de la obesidad, pero sí con el grado de obesidad.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
11-β-HSD: 11 beta hidroxiesteroide deshidrogenasa · DM: diabetes mellitus · DM2: diabetes mellitus tipo 2 · GAA: glucemia alterada en ayunas · IMC: índice de masa corporal · LPS: lipopolisacáridos · NHANES: Encuesta Nacional de Salud y Nutrición · TGA: tolerancia a la glucosa alterada.
BIBLIOGRAFÍA
- Muzzo BS, Monckeberg BF. Reflexiones sobre el aumento de la obesidad en Chile. Rev Chil Nutr. 2012;39:113-5.
- Rodríguez Domínguez L, Fernández-Britto Rodríguez JE, Díaz Sánchez ME, Ruiz Álvarez V, Hernández Hernández H, Herrera Gómez V, et al. Sobrepeso y dislipidemias en adolescentes. Rev Cubana Pediatr. 2014;86:433-44.
- Bluher M. Adipose tissue inflammation: a cause or consequence of obesity-related insulin resistance? Clin Sci (Lond). 2016;130:1603-14.
- Saavedra JM, Dattilo AM. Factores alimentarios y dietéticos asociados a la obesidad infantil: recomendaciones para su prevención antes de los dos años de vida. Rev Peruana Med Exp Salud Pública. 2012;29:379-85.
- Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999-2008. JAMA. 2010;303:235-41.
- González Tabares R, O’Relly Noda D, Guirola Fuentes J, Pérez Barly L, Acosta González FA, Navarro de Armas OL. Disglucemia y aterosclerosis en población laboralmente activa. Rev Cubana Med Militar. 2016;45:277-90.
- Gross Melo FJ, Huamán Saavedra JJ, Gonzáles Saldaña J, Gutiérrez Arana J, Álvarez Vargas M, Osada Liy JE. Características de los componentes del síndrome metabólico en pacientes con glucosa normal y disglicemia en ayunas. Rev Med Hered. 2018;29:137-46.
- Díaz Díaz O, Hernández Rodríguez J, Domínguez Alonso E, Martínez Montenegro I, Bosch Pérez Y, del Busto Mesa A, et al. Valor de corte de la circunferencia de la cintura como predictor de disglucemia. Rev Cubana Endocrinol. 2017;28:1-15.
- Cruz Sánchez JJ. Niveles plasmáticos de adiponectina e interleucina-1beta y su asociación con marcadores antropométricos, bioquímicos y clínicos en mujeres adultas mexicanas con obesidad y diabetes mellitus tipo 2. [Tesis para optar por el título de Máster en Ciencias en Nutrición]. Monterrey: Universidad Autónoma de Nuevo León; 2018.
- Godínez-Gutiérrez SA, Valerdi-Contreras L. Obesidad: resistencia endocrina múltiple. Rev Endocrinol Nutr. 2012;20(4):152-68.
- Girón Bombull JA, Fernández González A, Trujillo Feliciano Y, Ramos Labrada N, Silva Durán O. Caracterización clinicoepidemiológica de la prediabetes. MEDISAN. 2013;17:2096-3000.
- Díaz Díaz O. Primer consenso cubano de prediabetes. Rev Cubana Endocrinol. 2011;22:1.
- Buchaca Faxas EF. La pesquisa de los trastornos asintomáticos de la glucemia es una necesidad. Rev Cubana Endocrinol. 2013;24:103-6.
- Ramírez Leyva E, Álvarez Aldana D, García Moreiro R, Álvarez Fernández M, Rodríguez Bebet Y, Matos Valdivia Y. Diabetes mellitus en Ciego de Ávila: serie secular 1997-2008. Rev Cub Endocrinol. 2009;20.
- González Suárez RM, Perich Amador P, Arranz Calzado C. Heterogeneidad de los trastornos metabólicos de las etapas iniciales de la diabetes mellitus 2. Rev Cubana Endocrinol. 2009;20.
- Valdés S, Delgado E. Epidemiología de la prediabetes en España. Av Diabetol. 2009;25:99-104.
- American Diabetes Asociation. Standards of medical care in diabetes. Diabetes Care. Actualización Médica Periódica. 2009;32:S13-S61.
- Bustillo Solano EE, Bustillo Madrigal EE, Pérez Francisco Y, Pérez Sosa R, Brito García A, González Iglesia A, et al. Prevalencia de la diabetes mellitus y de la glucemia alterada en ayunas en un área de la ciudad de Sancti Spíritus. Rev Cubana Endocrinol. 2013;24:107-24.
- Di Flaviani A, Picconi F, Di Stefano P, Giordani I, Malandrucco I, Maggio P, et al. Impact of glycemic and blood pressure variability on surrogate measures of cardiovascular outcomes in type 2 diabetic patients. Diabetes Care. 2011;34:1605-9.
- Valdés Gómez W, Leyva Álvarez de la Campa G, Espinosa Reyes TM. Prediabetes y riesgo cardiovascular en población de alto riesgo en Atención Primaria de salud. Revista ALAD. 2014;4:22-9.
- Díaz Díaz O, Cabrera Rode E, Orlandi González N, Araña Rosaínz MJ, Díaz Horta O. Aspectos epidemiológicos de la prediabetes, diagnóstico y clasificación. Rev Cubana Endocrinol. 2011;22:3-10.
- Bermúdez S, Buchaca E,SuárezY, RodríguezL, Alonso CA, Mansur M, et al. Trastornos de la glucemia y de la acción de la insulina en una población de riesgo de diabetes. Rev Cubana Endocrinol. 2009;20:120-30.
- Arteaga A, Pollak F, Robres L, Velasco N. Características clínicas y metabólicas de los estados de intolerancia a la glucosa y glicemia de ayuno alteradas. Rev Méd Chile. 2009;137:193-9.
- Alayón AN, Alvear C. Prevalencia de desórdenes del metabolismo de los glúcidos y perfil del diabético en Cartagena de Indias (Colombia), 2005. Salud Uninorte Barranquilla (Col.). 2006;22:20-8.
- Thomas GN, McGhee SM, Schooling CM. Determinants of normoglycemia and contribution to cardiovascular risk factors in a Chinese population: the Hong Kong Cardiovascular Risk Factor Study. J Endocrinol Invest. 2006;29:528-35.
- Castillo K, Ríos M, Huaman J. Frecuencia y características de la glicemia basal alterada en adultos de Trujillo según criterios diagnósticos. Acta Médica Peru. 2011;28:132-45.