
Vol. 21 - Num. 84
Originales
Los pediatras frente a la educación para la salud comunitaria; valoración de la utilidad de una intervención durante el periodo perinatal
M.ª Rosa Pavo Garcíaa, M.ª Ángeles Ordóñez Alonsob, Débora Sanz Álvarezc
aPediatra. CS Villablanca. Madrid. España.
bPediatra. CS La Corredoria. Instituto de Investigación Sanitaria del Principado de Asturias (ISPA). Oviedo. Asturias. España.
cServicio de Pediatría. Hospital Universitario Gregorio Marañón. Madrid. España.
Correspondencia: MR Pavo. Correo electrónico: rosapavo.ped.garcianoblejas@gmail.com
Cómo citar este artículo: Pavo García MR, Ordóñez Alonso MA, Sanz Álvarez D. Los pediatras frente a la educación para la salud comunitaria; valoración de la utilidad de una intervención durante el periodo perinatal . Rev Pediatr Aten Primaria. 2019;21:359-68.
Publicado en Internet: 14-11-2019 - Número de visitas: 15927
Resumen
Introducción: el objetivo general de este trabajo es describir la situación actual de la educación para la salud (EPS) comunitaria en la Pediatría de Atención Primaria (PAP) española y analizar la utilidad de una intervención de EPS perinatal.
Material y métodos: estudio descriptivo observacional, realizado en marzo de 2019, a partir de los datos recogidos a través de una encuesta para profesionales difundida en una lista de distribución (PEDIAP) que cuenta con 1139 suscriptores, en su mayoría pediatras de Atención Primaria (AP).
Resultados: se recogieron 353 respuestas (83,9% mujeres). El 42,8% de las respuestas procede de la Comunidad de Madrid, seguida de Andalucía (12,2%) y Asturias (10,5%). El 84,1% de los profesionales trabaja en centros que imparten EPS comunitaria pero solo el 38% de ellos participa en alguna actividad. Las matronas realizan EPS en el 79,5% de los casos, seguidas por enfermería (77,8%). Pese a no ofertarse actividades en sus centros, al 82,1% le gustaría poder participar en algún proyecto de EPS, pero el 71,4% argumenta como impedimentos la falta de tiempo, el 48,2% la ausencia de compañeros dispuestos a participar y el 39,3% el déficit de formación en el manejo de grupos. El 21,4% reconocía falta de motivación y el 12,5% experiencias previas negativas.
Conclusiones: la inmensa mayoría de los profesionales consideraron útil la EPS perinatal, destacando la posibilidad de empoderar a las familias. Enfermería pediátrica fue el perfil mejor valorado por los profesionales para impartir EPS comunitaria infantil.
Palabras clave
● Atención perinatal ● Atención Primaria de Salud ● Educación en salud ● Estilo de vida saludable ● Promoción de la saludINTRODUCCIÓN
El modelo de Atención Primaria de Salud (APS) en España se basa en los pilares clave reflejados en la Declaración de Alma-Ata y refrendados en Astaná1: es integral, integrada, continua, accesible, multidisciplinaria, participativa y de alta calidad y representa una herramienta poderosa para la equidad. La APS tiene un papel primordial en la coordinación de recursos y en la continuidad asistencial.
Las fortalezas de la Atención Primaria (universalidad, gratuidad, accesibilidad y continuidad de los cuidados) han generado en los últimos 30 años importantes mejoras en la calidad asistencial y en la satisfacción de los usuarios. Sin embargo, también forman parte del origen de las debilidades del sistema: la accesibilidad ilimitada, la escasa inversión económica agravada por la crisis, la insuficiente planificación y organización, la medicalización y la dependencia del sistema2.
Hay estudios que alertan de la alta utilización de los servicios sanitarios, así como del aumento del consumo de diversos fármacos no indicados en la etapa de 0 a 6 meses3. En el nuevo Marco Estratégico para la Atención Primaria y Comunitaria se señalan los problemas prioritarios del Sistema Nacional de Salud (SNS). Entre ellos, la iatrogenia y sus causas latentes más influyentes, destacando la sobreutilización de los servicios asistenciales con el sobrediagnóstico y sobretratamiento consecuentes4.
La Pediatría de Atención Primaria (PAP) proporciona una asistencia sanitaria próxima a los niños y sus familias, teniendo en cuenta las características de su entorno, partiendo de una visión global de la Medicina en la que el objeto fundamental no es la enfermedad sino la población infantojuvenil en todas sus etapas. El pediatra acompaña a las familias durante los primeros meses de la vida de su hijo, en un entorno en el que el soporte familiar y comunitario tiende a ser cada vez más reducido.
Aún no hay evidencias sobre los beneficios que proporcionaría la educación de los padres después del nacimiento en la salud en la demanda de atención sanitaria o en las relaciones entre padres e hijos5,6. La Guía de Práctica Clínica de atención durante el embarazo y el puerperio del SNS recomienda la realización de grupos posparto en Atención Primaria (AP) que ofrezcan apoyo psicológico durante el puerperio y refuercen la adquisición de los conocimientos y habilidades que previamente se han trabajado en los grupos durante el embarazo7.
Cabe señalar la actividad que está llevando a cabo el Grupo de Educación para la Salud (EPS) de la Asociación Española de Pediatría de Atención Primaria (AEPap). Recientemente, este grupo ha desarrollado un programa titulado Uso racional de los servicios de urgencias pediátricas y actuación ante los principales problemas de salud. Si es urgente para ti… ¿Es urgente para mí?8.
Dentro de la Estrategia de Promoción de la Salud y Prevención en el SNS9, se ha elaborado un programa de parentalidad positiva en versión virtual y presencial10. Se ofertan cada vez más iniciativas sobre EPS para las familias con hijos, algunas con respaldo institucional y otras muchas por parte de sociedades científicas, pediatras y otros profesionales sanitarios. Existen también otros programas internacionales similares entre los que destacamos Start4life11, desarrollado por el departamento de salud pública del National Health System (Reino Unido) que, además, proporciona recursos para que los profesionales sanitarios puedan aplicar las campañas en su entorno local.
En PAP, las actividades de prevención y promoción de la salud se desarrollan habitualmente de forma individual dentro de las consultas concertadas del Programa de Salud Infantil (PSI) y, en menor medida, de forma comunitaria y prenatal. No se han encontrado estudios recientes que analicen la implantación global de la educación comunitaria en PAP en nuestro medio.
Desde la Declaración de Alma-Ata (1978) y la Carta de Ottawa (1986), diversos organismos internacionales han señalado la participación comunitaria como fundamental para aumentar el bienestar de las comunidades y mejorar la salud de las poblaciones. Destacamos la visión y definición del Instituto de Programas Interdisciplinarios en Atención Primaria de la Salud de la Universidad Industrial de Santander (Colombia), que entiende la EPS con enfoque integral como un proceso de generación de aprendizajes para el ejercicio de la ciudadanía, la movilización y la construcción colectiva de la salud en la cual participan las personas y los diferentes sectores del desarrollo.
De cara a capacitar a las familias frente a las situaciones y problemas más frecuentes de la crianza de un hijo, es preciso proporcionar conocimientos sobre el proceso normal del parto, puerperio y lactancia, los cuidados del recién nacido, las características del sueño infantil, la educación para la prevención de enfermedades, la promoción de hábitos saludables y el entrenamiento para reconocer síntomas frecuentes y diferenciarlos de síntomas de alarma. Hipotéticamente, esto permitiría mejorar los resultados en salud infantil, reducir el número de consultas en el centro de salud (CS) y en las urgencias hospitalarias, el desarrollo de las visitas individuales del PSI y, probablemente, la relación entre las familias y los profesionales sanitarios.
Por todo esto, uno de los posibles puntos de mejora en la PAP en los que podrían participar los equipos de Pediatría consistiría en implementar programas de EPS perinatal de forma global, sistemática e institucionalizada.
Los objetivos generales de este trabajo son describir la situación actual de la EPS comunitaria en la PAP española, y analizar la utilidad de la EPS comunitaria perinatal para los profesionales sanitarios.
MATERIAL Y MÉTODOS
Se trata de un estudio descriptivo observacional. Los datos se recogieron a través de una encuesta mediante la tecnología de formularios Google que se difundió en marzo de 2019 a través de la lista de distribución de correos PEDIAP de RedIRIS, que disponía en ese momento de 1139 suscriptores. Se aceptaron respuestas durante una semana.
Se recogieron los siguientes datos:
- Sociodemográficos: formación, comunidad autónoma (CA), sexo, edad.
- Características del CS: ámbito, disponibilidad de enfermería pediátrica y de matrona en el centro, número de cupos; existencia de plazas vacantes o sin cubrir en el centro.
- Conocimiento sobre la regulación de las actividades de EPS en su CA.
- Oferta actual de actividades de EPS grupales o comunitarias en su CS. En el caso de respuesta afirmativa: perfil profesional de sanitarios que impartían EPS grupal o comunitaria en su centro; participación individual del encuestado; experiencia personal. En el caso de respuesta negativa: oferta previa; deseo de participación; motivos por los que no se ofertaba EPS grupal o comunitaria. Comunes: existencia de circuito de información sistemática a las familias sobre cuidados perinatales; valoración de efectividad de actividades de EPS grupal perinatal; valoración de diferentes motivos por los que podría considerarse útil la EPS; valoración del perfil profesional más indicado para desarrollar actividades de EPS grupal o comunitaria.
Los datos obtenidos se almacenaron y procesaron en hojas de cálculo Google y Microsoft Excel. El análisis estadístico se realizó con el programa informático IBM SPSS Statistics. Las variables cualitativas se describieron empleando frecuencias absolutas y relativas. Las variables cuantitativas con medidas de posición como la media o la mediana y con medidas de dispersión como la desviación estándar (DE). La relación entre variables cualitativas se valoró con el test χ2 de Pearson o el test de Fisher, según se verificase o no la hipótesis sobre frecuencias. La comparación de variables cuantitativas entre dos grupos se realizó con el test t de Student. Si los grupos eran tres o más se comprobó la homocedasticidad, además de la normalidad, empleando en la comparación el test ANOVA tras verificar ambas condiciones. El nivel de significación empleado fue de 0,05.
RESULTADOS
Se obtuvieron un total de 353 respuestas (83,9% mujeres). El 94,9% de los participantes fueron especialistas en Pediatría, el 3,1% médicos no especialistas en Pediatría y el 2% restante comunicó otros perfiles como médicos internos residentes (MIR) y enfermería. Esto supone una participación del 31% de las personas suscritas a la lista PEDIAP, que engloba, en su mayoría, a pediatras de AP.
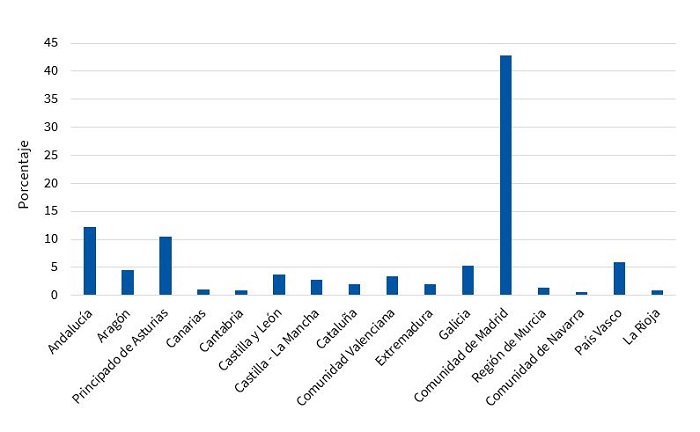
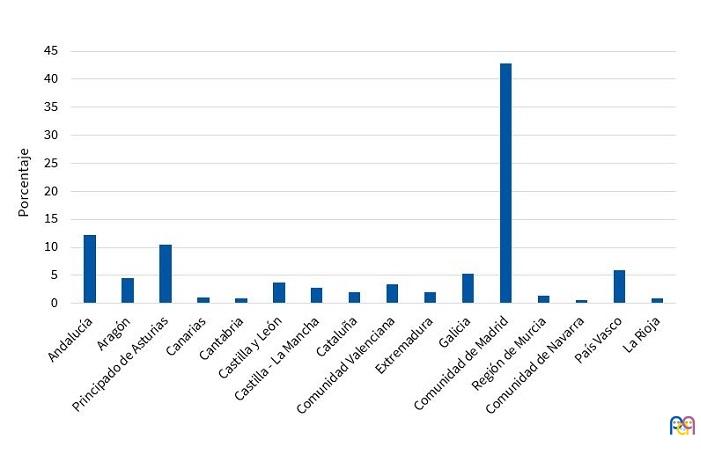
Madrid ha sido la comunidad que ha aportado más participantes, con un 42,8%, seguida de Andalucía, con un 12,2% y Principado de Asturias, con un 10,5% (Fig. 1).
| Figura 1. Distribución de los participantes por comunidades autónomas |
|---|
 |
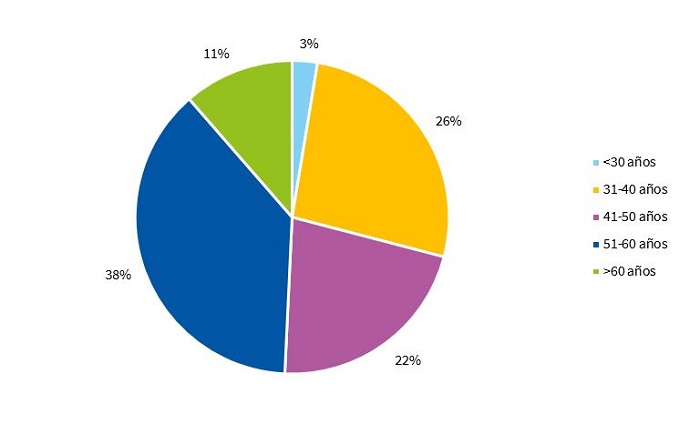
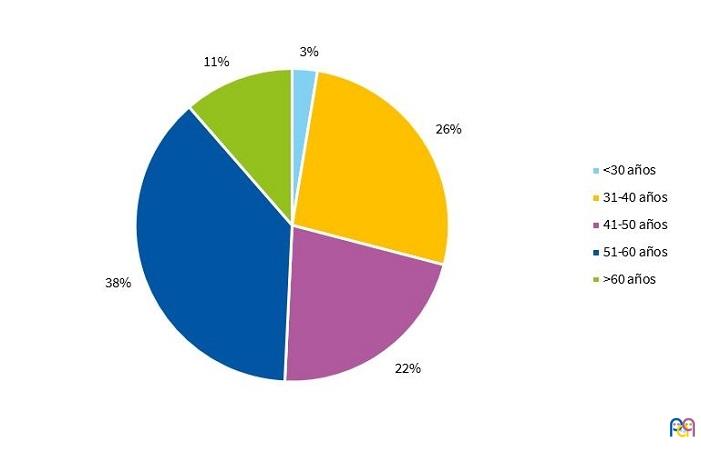
La distribución por edades de los encuestados se detalla en la Fig. 2.
| Figura 2. Distribución de los participantes por grupos de edad |
|---|
 |
El 74,8% de los participantes desempeña su trabajo en ámbito urbano, 15% rural y 10,2% mixto.
En cuanto a la dotación del equipo pediátrico, el 68,3% respondieron que disponen en sus centros de enfermería pediátrica y el 80,2% de matrona.
Eran profesionales de Pediatría únicos un 11,6% de los encuestados. El 50,4% trabaja en CS con dos o tres cupos y el 38% con cuatro o más, aunque el 19,5% del total respondieron que existe alguna plaza sin cubrir en el momento actual.
El 55% de los profesionales encuestados desconoce la regulación de la prestación de actividades de EPS. El 20,5% afirma que no está regulado en su CA. El 16,4% refiere que lo está a través de la cartera de servicios, frente a un 2,3 y un 2,9% que responden que a través del contrato programa del centro u otros pactos de gestión y del PSI, respectivamente.
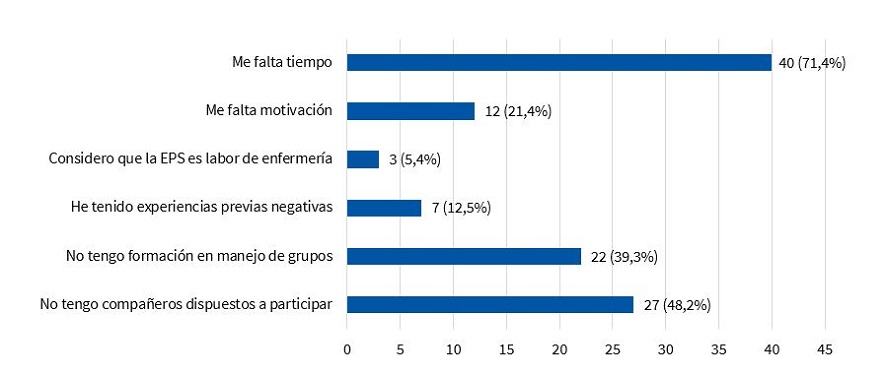
El 15,9% de los participantes respondieron que en su CS no se impartía ninguna actividad de EPS en el momento actual, aunque en el 35,7% de esos centros se habían impartido con anterioridad y el 32,1% no sabía contestar. Pese a no ofertarse actividades en sus centros, al 91,1% le parecería útil la realización de talleres durante el periodo perinatal. Al 82,1% le gustaría poder participar en algún proyecto de EPS, pero el 71,4% argumentaba como impedimentos la falta de tiempo, el 48,2% la ausencia de compañeros dispuestos a participar y el 39,3% el déficit de formación en técnicas de manejo de grupos. El 21,4% reconocía falta de motivación y el 12,5% experiencias previas negativas. El 5,4% consideraba que la EPS es labor de enfermería (Fig. 3).
| Figura 3. Motivos que dificultan a los profesionales la realización de educación para la salud (EPS) comunitaria |
|---|
 |

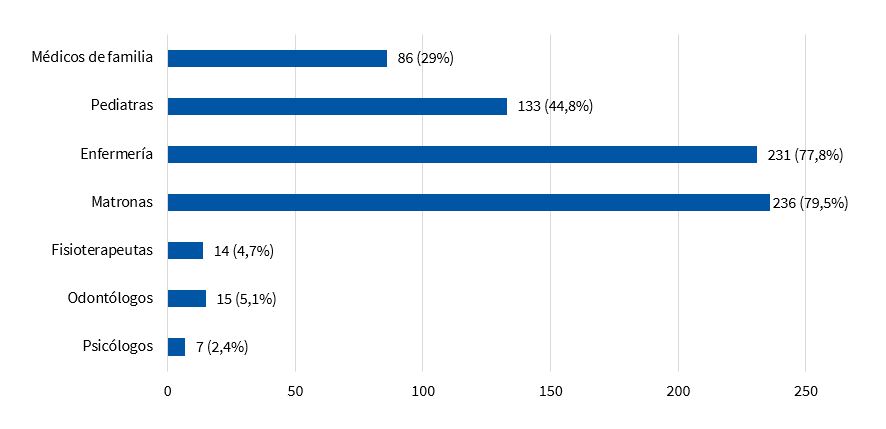
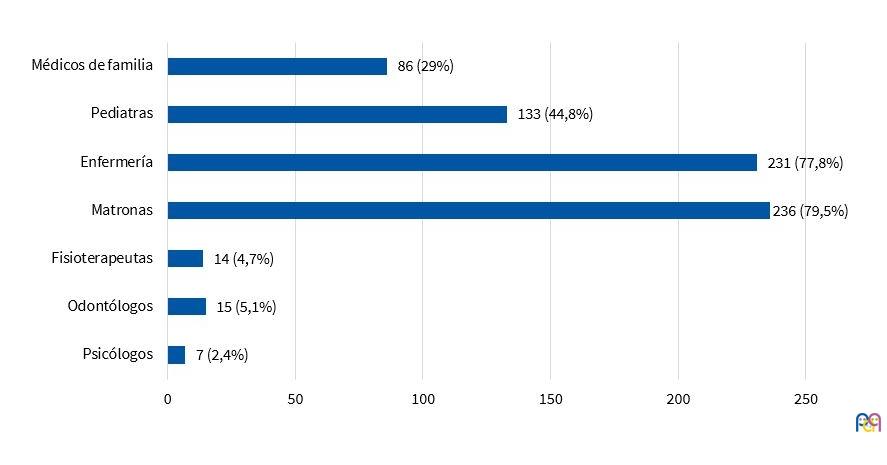
El 84,1% restante de los participantes respondieron que en sus centros de trabajo existía alguna actividad de EPS comunitaria. Las matronas participaban en un 79,5% de los casos, seguidas por enfermería (77,8%). En tercer lugar, se encontrarían los pediatras, que estarían activos en un 44,8% de los centros en los que se realiza EPS (Fig. 4). El 38% de los encuestados refería participar actualmente en alguna actividad en su centro.
| Figura 4. Profesionales que realizan educación para la salud (EPS) en los centros de salud. Expresado en n (porcentaje) |
|---|
 |
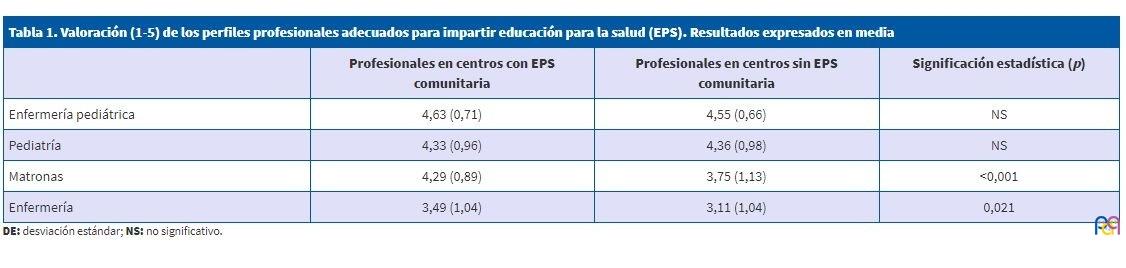
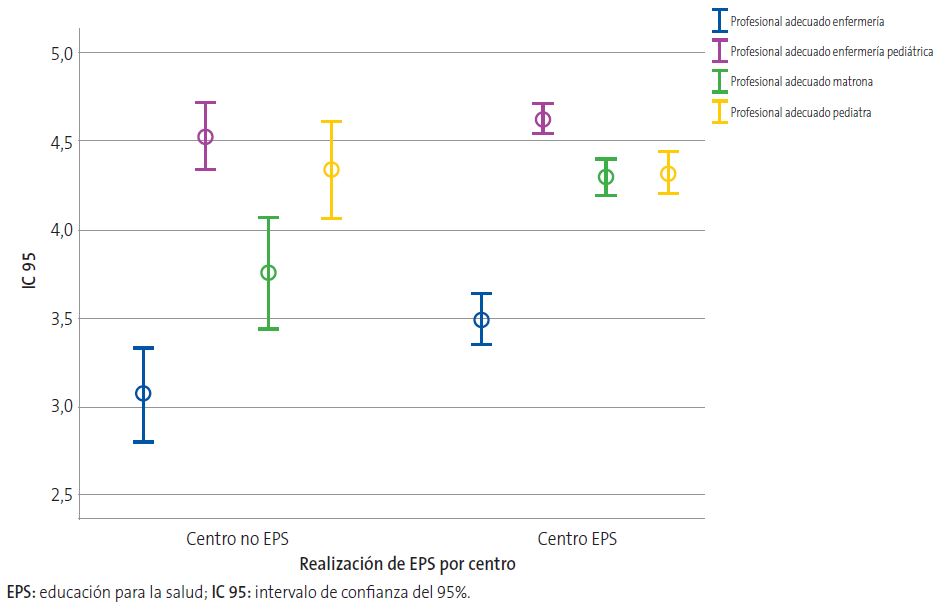
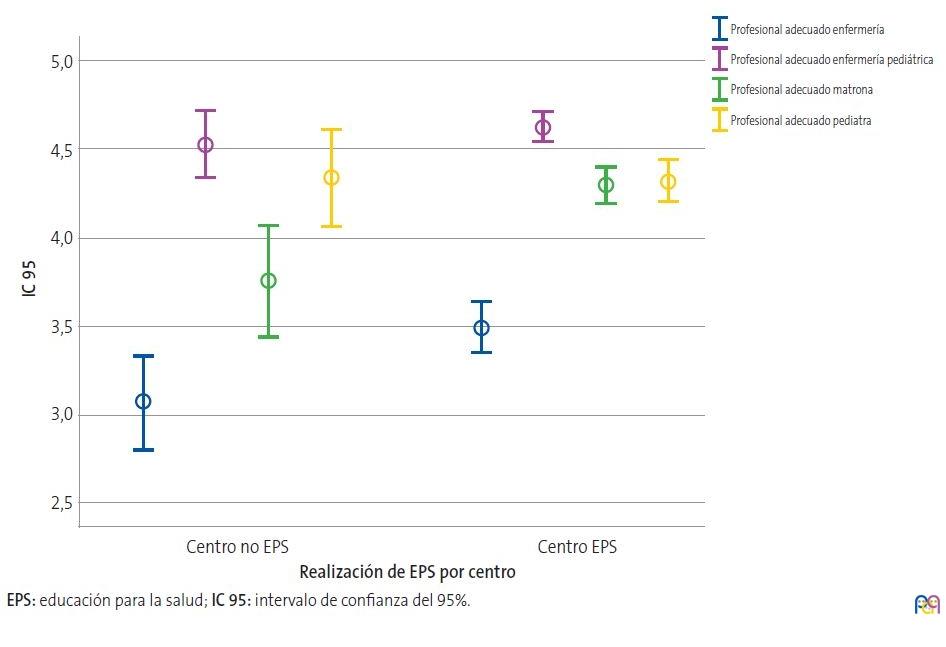
Los encuestados valoraron a la enfermería pediátrica como mejor perfil profesional para impartir EPS, seguida de Pediatría, matronas y enfermería. Se encontraron diferencias significativas en cuanto a la puntuación obtenida por enfermería y matronas en función de que el profesional trabajara en centros con EPS comunitaria o no (Tabla 1 y Fig. 5).
| Tabla 1. Valoración (1-5) de los perfiles profesionales adecuados para impartir educación para la salud (EPS). Resultados expresados en media | |||
|---|---|---|---|
| Profesionales en centros con EPS comunitaria | Profesionales en centros sin EPS comunitaria | Significación estadística (p) | |
| Enfermería pediátrica | 4,63 (0,71) | 4,55 (0,66) | NS |
| Pediatría | 4,33 (0,96) | 4,36 (0,98) | NS |
| Matronas | 4,29 (0,89) | 3,75 (1,13) | <0,001 |
| Enfermería | 3,49 (1,04) | 3,11 (1,04) | 0,021 |
| Figura 5. Valoración media del profesional más adecuado para impartir educación para la salud (EPS) en Atención Primaria (AP) según la opinión de profesionales que trabajan en centros con EPS frente a centros sin EPS |
|---|
 |
Los participantes de centros en los que no se imparte EPS comunitaria valoran en primer lugar, dentro de las utilidades de la EPS perinatal, la posibilidad de empoderar a las familias (media: 4,04; DE 1,19) seguida de la prevención de accidentes, enfermedades y problemas de salud (nota media: 3,89, DE 1,15) (Fig. 6).
| Figura 6. Valoración de la utilidad de la realización de educación para la salud (EPS) comunitaria en centros según realización de EPS |
|---|
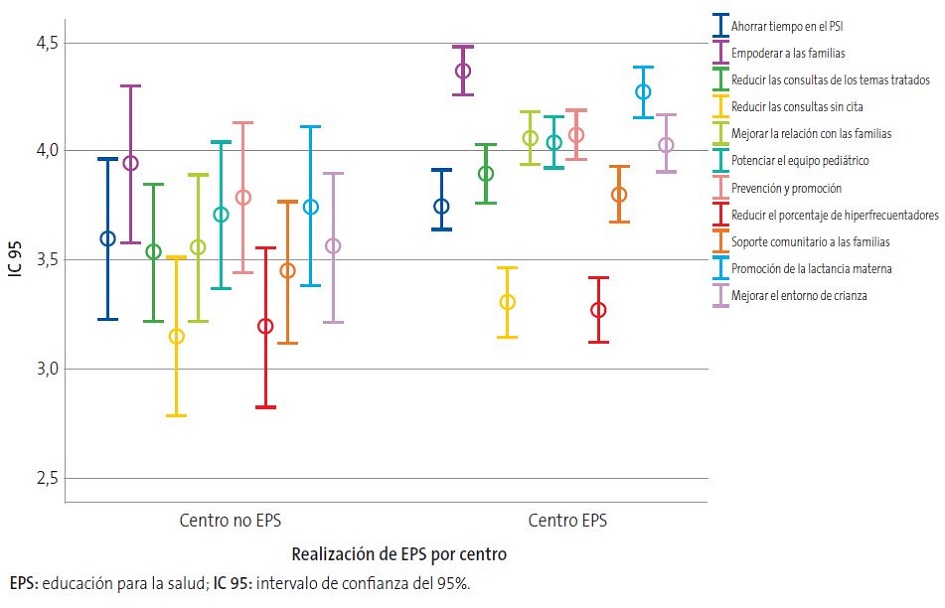 |
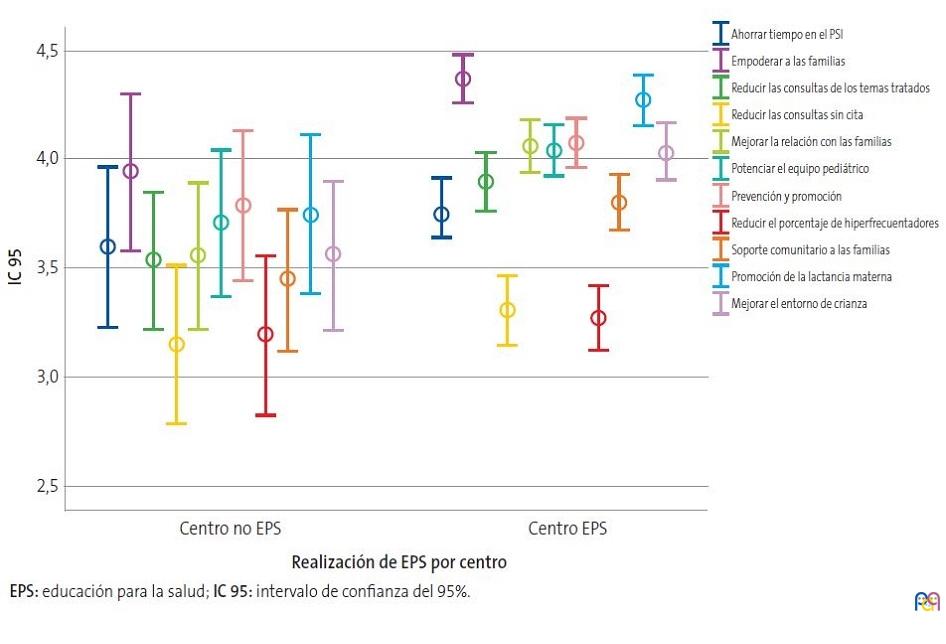
Al 95,6% de los participantes de los centros en los que se realiza EPS comunitaria le parecería útil la realización de actividades de EPS perinatal. El aspecto mejor valorado fue, de nuevo, la posibilidad de empoderar a las familias (nota media: 4,37; DE: 0,93) seguido en este caso de la promoción de la lactancia materna (4,28; DE: 0,96) (Fig. 6).
En cuanto a la utilidad percibida por parte de profesionales de centros con EPS comunitaria frente a centros sin EPS comunitaria, solo se encontraron diferencias significativas en la valoración sobre la promoción de la lactancia materna (p = 0,035).
El 89,9% de los encuestados de los centros con EPS, frente al 75% en los centros sin EPS, responde que se informa sistemáticamente, por parte de enfermería o matrona del centro de salud o del hospital, sobre los cuidados del recién nacido (p <0,005).
Un total de 113 profesionales (88,5% mujeres) respondieron que actualmente participaban en actividades de EPS en sus centros de salud. La franja de edad más activa fue la correspondiente a los 51-60 años, existiendo una diferencia estadísticamente significativa con respecto al resto de edades (p = 0,044). No se encontraron diferencias según sexo, número de cupos del centro, existencia de vacantes o tipo de centro.
DISCUSIÓN
Paradójicamente, en la era de la “infoxicación” atendemos a muchas familias con carencias de conocimiento, escasa experiencia y falta de habilidades en el manejo de los cuidados básicos, crianza y principales problemas de salud infantil. Esto se traduce en dificultades para asumir la responsabilidad en la toma de decisiones y dependencia de la figura del profesional sanitario.
La EPS grupal es una intervención que se puede incorporar a la actividad de la PAP para dotar a las familias de conocimientos, habilidades y herramientas que faciliten el proceso de la maternidad y de la paternidad y que favorezcan la salud de sus hijos e hijas.
En la encuesta realizada, enfermería pediátrica y pediatras son la principal apuesta para llevar a cabo las actividades de EPS comunitaria. Los profesionales encuestados que trabajaban en centros que impartían EPS comunitaria otorgaban mejor valoración a la enfermería y a las matronas frente a los que participantes de centros sin EPS comunitaria, probablemente en relación con la experiencia práctica en sus CS.
También sería interesante y enriquecedor valorar la participación de otros profesionales como psicólogos, nutricionistas, pedagogos, etc.
Los factores limitadores más frecuentemente señalados por los profesionales encuestados son la falta de tiempo en la práctica diaria y la escasa formación.
El papel de la enfermera especialista en Pediatría es fundamental para la puesta en marcha de iniciativas comunitarias y el óptimo desempeño del equipo pediátrico. Sería deseable que todos los equipos de Pediatría dispusieran de enfermería pediátrica en su dotación ya que, por su formación específica, proporcionan la mejor atención de la población pediátrica. Además, el trabajo en equipo permitiría además repartir la carga asistencial de los facultativos, asignando a cada profesional aquellas tareas para las cuales es más eficiente y está mejor formado.
Por su experiencia en los talleres mal llamados de “preparación al parto” y su conocimiento sobre las necesidades y demandas de las gestantes y acompañantes, las matronas son una de las figuras más importantes en los programas de EPS comunitaria en nuestros CS. Juegan un papel primordial en el diseño de programas de EPS durante el periodo perinatal, tanto por su experiencia como por su potencial en la captación de las familias para el desarrollo de programas perinatales.
La Orden SCO/3148/2006 por la que se aprueba y publica el programa formativo de la especialidad de Pediatría y sus Áreas Específicas recoge que: “A la Pediatría le incumbe cuanto se refiere a los cuidados del niño y adolescente sano (Pediatría preventiva), a los modos de asistencia médica integral, total y continuada durante el estado de enfermedad (Pediatría clínica) y a cuanto atañe al niño y adolescente sano y enfermo en sus interrelaciones individuales y con la comunidad en el medio físico y humano en que de manera ininterrumpida y con características propias se desarrolla (Pediatría social)”. Un 5,4% de los encuestados considera que la EPS es una tarea de enfermería y la enfermería pediátrica es el perfil mejor valorado por parte de los encuestados. Pero los pediatras de AP no debemos olvidar que la Pediatría preventiva forma parte de nuestro cometido. Para lograr cambios significativos, debemos contribuir a la puesta en marcha de programas de atención comunitaria basados en un correcto diagnóstico conductual que permita identificar las necesidades de nuestro entorno e involucrar a nuestra comunidad.
En el nuevo Marco estratégico para la Atención Primaria y comunitaria4, que acaba de publicarse, se plantea la necesidad de actualizar la Atención Primaria para adaptarla a los cambios sociales. Se han desarrollado 100 propuestas de acción incorporadas en seis líneas estratégicas y 23 objetivos dirigidos a mejorar la atención de salud y avanzar hacia el fortalecimiento y liderazgo de la APS. Una de estas líneas estratégicas (D) es “Reforzar la orientación comunitaria, la promoción de la salud y prevención en APS”.
Es alentador que las máximas instituciones y autoridades sanitarias aboguen por un cambio en el paradigma de la APS en el que se contempla textualmente: “mejorar la capacidad de decisión a las personas, las familias y las comunidades, generando usuarios activos o ‘activados’ y tratando de conseguir una alianza duradera con la población basada en la toma de decisiones compartida que le permita organizarse y desplegar todas sus capacidades para vivir más tiempo con un mayor grado de bienestar y mejor calidad de vida. Es necesario la reorientación, reorganización y flexibilización de los recursos y las actividades de promoción de la salud y prevención, contando con la posibilidad de la introducción de sistemas innovadores que fomenten los entornos y estilos de vida saludables […]”.
Esta encuesta realizada sobre la situación actual de la EPS en nuestro medio arroja como dato interesante que en casi un 16% de los CS no se realiza ninguna actividad comunitaria y solo el 32% de los encuestados participaba actualmente en alguna. Sin embargo, la inmensa mayoría de los participantes consideraron que sería útil la implantación de un programa de EPS durante el periodo perinatal y, dentro de sus utilidades, destacaron la posibilidad de empoderar a las familias.
La respuesta por comunidades autónomas fue bastante heterogénea. Madrid es la más representada, seguida de Andalucía y Principado de Asturias. No se obtuvieron respuestas procedentes de Baleares, Ceuta ni Melilla.
Cabe señalar que existe un probable sesgo de selección al tratarse de una muestra recogida a través de una lista de distribución de correos, por lo que la representatividad de los datos obtenidos no está asegurada. Para motivar la participación se ofreció un incentivo tras finalizar la encuesta (https://vimeo.com/jacobfrey/thepresent).
Como profesionales responsables, tenemos la obligación de participar en los cambios para la mejora de la situación de la PAP y la sostenibilidad del sistema analizando en qué medida realizamos un uso racional de los recursos, contribuimos a la pediatra-dependencia de las familias, a la saturación de las consultas, asumimos tareas aun sabiendo que no somos el profesional más eficiente y qué acciones correctoras podemos implementar en nuestro medio.
El nuevo marco estratégico constituye una esperanza para la APS y el abordaje comunitario nos ofrece una excelente oportunidad de mejora o, simplemente, una vuelta a los orígenes para retomar lo que siempre debió ser labor del pediatra de Atención Primaria y ha quedado relegada a un segundo plano por una sobrecarga asistencial superflua.
CONCLUSIONES
- La inmensa mayoría de los encuestados consideraría útil la existencia de programas de EPS perinatal y estaría interesado en participar en actividades comunitarias.
- La enfermería pediátrica es el perfil profesional mejor valorado para realizar EPS comunitaria por parte de los participantes.
- El nuevo Marco Estratégico para la Atención Primaria y Comunitaria es una oportunidad para la mejora de la PAP. Como profesionales, tenemos la obligación de participar en la modernización del sistema de APS, ofreciendo un abordaje biopsicosocial, salutogénico y comunitario.
CONFLICTO DE INTERESES
Las autoras declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
Este trabajo forma parte de un trabajo de fin de máster para el Máster Pediatría de Atención Primaria organizado por la Universidad Complutense de Madrid y la Asociación Española de Pediatría de Atención Primaria, pero no ha sido previamente publicado ni remitido simultáneamente a otra publicación.
M.ª Ángeles Ordóñez y M.ª Rosa Pavo han participado en la elaboración y diseño del estudio, análisis de los datos, resultados y conclusiones. Débora Sanz ha participado en el análisis estadístico de los datos. Todas las autoras han leído y aprobado la versión del manuscrito finalmente remitida.
ABREVIATURAS
AEPap: Asociación Española de Pediatría de Atención Primaria · AP: Atención Primaria · APS: Atención Primaria de Salud · CA: comunidad autónoma · CS: centro de salud · DE: desviación estándar · EPS: educación para la salud · MIR: médicos internos y residentes · PAP: Pediatría de Atención Primaria · PSI: programa de salud infantil · SNS: Sistema Nacional de Salud.
BIBLIOGRAFÍA
- Declaración de Astaná. En: Organización Mundial de la Salud [en línea] [consultado el 05/11/2019]. Disponible en www.who.int/docs/default-source/primary-health/declaration/gcphc-declaration-sp.pdf
- Domínguez Aurrecoechea B, Valdivia Jiménez C. La Pediatría de Atención Primaria en el sistema público de salud del siglo XXI. Informe SESPAS 2012. Gac Sanit. 2012;26:82-7.
- Ordóñez Alonso MÁ, Domínguez Aurrecoechea B, Pérez Candás JI, López Vilar P, Fernández Francés M, Coto Fuente M, et al. Influencia de la asistencia a guarderías en la frecuentación en Urgencias y Atención Primaria. Rev Pediatr Aten Primaria. 2016;18:243-52.
- Resolución de 26 de abril de 2019, de la Secretaría General de Sanidad y Consumo, por la que publica el Marco estratégico para la Atención Primaria y comunitaria. En: Boletín Oficial del Estado [en línea] [consultado el 05/11/2019]. Disponible en www.boe.es/diario_boe/txt.php?id=BOE-A-2019-6761
- Bryanton J, Beck CT, Montelpare W. Postnatal parental education for optimizing infant general health and parent-infant relationships. Cochrane Database Syst Rev. 2013;(11):CD004068.
- Gagnon AJ, Sandall J. Individual or group antenatal education for childbirth or parenthood, or both. Cochrane Database Syst Rev. 2007;(3):CD002869.
- Grupo de trabajo de la Guía de práctica clínica de atención en el embarazo y puerperio. Guía de práctica clínica de atención en el embarazo y puerperio. En: Ministerio de Sanidad, Consumo y Bienestar Social [en línea] [consultado el 05/11/2019]. Disponible en www.mscbs.gob.es/organizacion/sns/planCalidadSNS/pdf/GPC_de_embarazo_y_puerperio.pdf
- Vázquez Fernández ME, Núñez Jiménez C, Serrano Poveda M. Programa de EPS. Uso racional de los servicios de urgencias pediátricas y actuación ante los principales problemas de salud. Si es urgente para ti… ¿Es urgente para mí? En: AEPap [en línea] [consultado el 05/11/2019]. Disponible en www.aepap.org/sites/default/files/documento/archivos-adjuntos/educacion_para_la_salud_web_pdf_urgencias.pdf
- Estrategia aprobada por el Consejo Interterritorial del Sistema Nacional de Salud el 18 de diciembre de 2013. En: Ministerio de Sanidad, Consumo y Bienestar Social [en línea] [consultado el 05/11/2019]. Disponible en www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/Estrategia/docs/EstrategiaPromocionSaludyPrevencionSNS.pdf
- Rodrigo MJ, Martín JC, Máiquez ML (dirs.). Parentalidad positiva: ganar salud y bienestar de 0-3 años. Guía para el desarrollo de talleres presenciales grupales. En: Ministerio de Sanidad, Consumo y Bienestar Social [en línea] [consultado el 05/11/2019]. Disponible en www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/Estrategia/docs/Parentalidad_Positiva.pdf
- Start4Life [en línea] [consultado el 05/11/2019]. Disponible en www.nhs.uk/start4life