

Análisis de la cobertura vacunal frente a tétanos en adolescentes: evolución y situación actual en Extremadura (España)
aFarmacéutica de Equipo Atención Primaria. CS de Montijo. Badajoz. España.
Correspondencia: L Serrano. Correo electrónico: laura.serrano@salud-juntaex.es
Cómo citar este artículo: Serrano Peláez L. Análisis de la cobertura vacunal frente a tétanos en adolescentes: evolución y situación actual en Extremadura (España) . Rev Pediatr Aten Primaria. 2019;21:e193-e200.
Publicado en Internet: 21-10-2019 - Número de visitas: 17121
Resumen
Introducción: el tétanos es una enfermedad aguda grave cuyo tratamiento es difícil y, por tanto, es fundamental su prevención. La administración de cinco dosis de vacuna antitetánica es suficiente para conferir una protección a largo plazo. En los últimos años se ha observado cierta disminución en las coberturas, lo que supone la existencia de población no suficientemente inmunizada. El objetivo de este estudio es analizar la cobertura vacunal de la dosis de recuerdo frente al tétanos en adolescentes en la localidad de Santa Amalia, provincia de Badajoz (España), durante los últimos 20 años (1996-2016).
Material y métodos: estudio observacional transversal. Se revisaron las tarjetas de vacunación y los registros de las dosis administradas en los documentos manuscritos y registro informático en el entorno JARA Atención Sanitaria (JARA-AS). Entre 1996 y 2001, la vacunación se hacía en el centro escolar, con registro manual. Desde 2002, se administró la vacuna en el centro de salud, con registro manual (2002-2007) e informático (2008-2016).
Resultados: analizada la cobertura de forma agrupada, los peores resultados de vacunación se apreciaron en centro de salud utilizando registro manual (35,6%), mientras que las mejores cifras de vacunación se encontraron en centro de salud con registro informático (100%), seguido por el grupo de centro escolar (83,0%).
Conclusiones: este estudio pone de manifiesto una alta cobertura de vacunación frente a tétanos en la dosis de recuerdo en adolescentes de 14 años en Santa Amalia, similar a la cobertura nacional, a diferencia de la baja cobertura existente en el resto de Extremadura.
Palabras clave
● Adolescente ● Cobertura de vacunación ● Tétanos ● VacunasINTRODUCCIÓN
El tétanos es una enfermedad aguda grave causada por la acción de la toxina del bacilo Clostridium tetani, que prolifera en condiciones de anaerobiosis en el lugar de una lesión. Las heridas, reconocidas o no, son la puerta de entrada al organismo, y son especialmente peligrosas las heridas producidas por punción o por desgarro y las quemaduras. Las inyecciones contaminadas y algunas técnicas quirúrgicas también pueden causar tétanos. La transmisión de esta enfermedad nunca es por contacto entre personas, siempre se realiza a través de un reservorio. Clínicamente, el tétanos se caracteriza por contracciones musculares dolorosas y una expresión facial muy característica, conocida como “risa sardónica”. El tratamiento de la enfermedad es difícil y, por tanto, es esencial su prevención. Esta solo puede lograrse mediante inmunización activa (vacunación antitetánica) o pasiva (inmunoglobulina específica). La medida de prevención más efectiva es la vacunación1,2.
El tétanos es una enfermedad infecciosa con una baja morbilidad, pero una alta letalidad, y cuenta con una vacuna eficaz, segura y barata como principal abordaje para reducir su incidencia y erradicarla3. Las vacunas salvan millones de vidas cada año y constituyen una de las intervenciones más seguras y efectivas en salud pública, proporcionando beneficios sobre el control y la prevención de enfermedades, así como sociales y económicos. La reciente elaboración del Plan Global de Acción en Vacunas (GVAP) para 2011-2020, aprobado por 194 países en la Asamblea Mundial de la Salud, es una hoja de ruta conjunta que reconoce la importancia de las vacunas y ratifica que expandir la vacunación es avanzar en el bienestar global4. Uno de los objetivos principales de la Organización Mundial de la Salud (OMS) en los países con economías desarrolladas es el de la lucha contra el tétanos mediante el mantenimiento de una cobertura alta de vacunación, con las dosis de refuerzo suficientes para prevenir el tétanos en todos los grupos de edad2.
La administración de dosis de recuerdo consigue mantener elevado el título de anticuerpos protectores y se considera que con cinco dosis de vacuna antitetánica es suficiente para conferir una protección a largo plazo. En España se utilizan vacunas inactivadas, preparadas con los toxoides de tétanos y difteria adsorbidos en sales de aluminio. Tras la vacunación, se producen anticuerpos frente a los antígenos de la vacuna en prácticamente el 100% de los vacunados, pero la inmunidad conferida decae con el tiempo. El número de dosis de vacuna frente a tétanos y difteria administradas en la infancia tiene mucha influencia en la duración de la inmunidad adquirida tras cada dosis de recuerdo administrada en la edad adulta1.
La primera vez que se implantó en España el calendario de vacunaciones incluyendo una dosis de recuerdo de vacuna antitetánica a los 14 años de edad fue en 19752. En la actualidad, el Comité Asesor de Vacunas de la Asociación Española de Pediatría (CAV-AEP) publica anualmente el calendario de vacunaciones que estima idóneo para los niños residentes en España, teniendo en cuenta la evidencia disponible sobre vacunas, además de recoger las vacunas sistemáticas de los calendarios oficiales actuales. Se sigue recomendando emplear la vacuna de tétanos-difteria-tosferina de baja carga antigénica (Tdpa) a los 12-14 años en la vacunación de la dosis de refuerzo5. A su vez, la Ponencia del Programa y Registro de Vacunaciones, órgano científico-técnico del Consejo Interterritorial del Sistema Nacional de Salud, realiza evaluaciones y propone modificaciones que se incorporan en el calendario de vacunación de las comunidades autónomas (CC. AA.)6. Tras evaluar los programas de vacunación contra el tétanos en España y los países de nuestro entorno y revisar la evidencia científica de la protección de las diferentes pautas de vacunación, propone la recomendación de administrar una dosis de recuerdo de tétanos-difteria (Td) a los 14 años de edad7.
Tanto en el Decreto 14/2016, de 23 de febrero, que modifica el Decreto 161/2006, de 6 de septiembre, por el que aprueba el calendario íntegro de vacunaciones de Extremadura, como en el Decreto 149/2018, de 4 de septiembre, por el que se modifica el Decreto 204/2016, de 14 de diciembre, por el que se aprueba el calendario íntegro de vacunaciones de Extremadura publicado en el Diario Oficial de Extremadura, se recomienda la administración de una dosis de Td a los 14 años. Esta vacuna de tétanos-difteria (Td) presenta una concentración de antígenos frente a difteria reducida y puede utilizarse a partir de los 7 años, estando destinada a niños a partir de los 14 años de edad y para adultos8.
La vacunación sistemática en la población y las altas coberturas alcanzadas han permitido que el tétanos sea una enfermedad poco frecuente en España. No hay casos de tétanos neonatal y los pocos casos de tétanos que ocurren se dan en personas adultas mal vacunadas o con vacunación incompleta6, siguiendo la misma distribución de edad, número de casos y mortalidad que en los países occidentales7. En Extremadura, el último caso notificado databa del año 2005, hasta que el 2 de junio de 2017 se notificó un caso de tétanos en un varón de 68 años, del que no consta vacunación previa frente al tétanos9.
Las vacunas infantiles en España no solo son aceptadas sino mayoritariamente demandadas por la población y, en consecuencia, se registran altas tasas de cobertura vacunal10. En los adultos, la cifra de vacunación completa es escasa, además no hay que olvidar que el título de anticuerpos circulantes disminuye con el tiempo3. A pesar de ello, en los últimos años se ha observado una cierta disminución en estas coberturas, lo que en algunas CC. AA. puede suponer la existencia de verdaderas bolsas de población no inmunizada y, por tanto, no protegida10.
Un avance del análisis de las cifras de coberturas de vacunación de las dosis de recuerdo frente a tétanos-difteria para el año 2016 nos muestra que para la población global española de 14-16 años la cobertura es del 82%11. Por CC. AA., Cataluña, con un 96,4%, es la que mayor cobertura presenta, mientras que Extremadura solo tiene un 52,7% de población vacunada a los 14 años de edad12. En el Área de Salud de Don Benito-Villanueva, la cobertura es del 71,1% (datos de Servicio Extremeño de Salud, del 18 de agosto de 2017).
Se realiza el siguiente análisis al no conocer la existencia de estudios previos de estas características en nuestro medio, debido a que son escasos los trabajos que aportan datos globales que permiten una comparación con criterios similares. Asimismo, se piensa que es una aportación útil para el conocimiento de la cobertura de vacunación, pues se utilizan datos reales y no estimaciones, que pueden ayudar a mejorar la planificación de las políticas de inmunización en el Sistema Sanitario Público extremeño.
El objetivo principal de este estudio es analizar la cobertura de vacunación de la dosis de recuerdo de tétanos-difteria (Td) administrada a los 14 años de edad en la localidad extremeña de Santa Amalia (Área de Salud Don Benito-Villanueva) con el fin de conocer su evolución en el periodo 1996-2016. Asimismo, como objetivo secundario, se plantea la posibilidad de conocer si la cobertura es menor en adolescentes de 14 años (en adelante adolescentes) que hayan sido vacunados en centro de salud con respecto a los vacunados en el centro escolar.
MATERIAL Y MÉTODOS
Tipo de diseño de investigación: estudio observacional, descriptivo transversal, de todas las dosis de tétanos administradas a los 14 años de edad a los residentes de la localidad de Santa Amalia, provincia de Badajoz (España), en los últimos 20 años (1996-2016).
Población de referencia: adolescentes de 14 años de edad residentes en la localidad de Santa Amalia.
Población de estudio: adolescentes de 14 años residentes en la localidad de Santa Amalia vacunados de tétanos en el centro escolar o el centro de salud.
Criterios de inclusión: haber sido vacunado en centro escolar o centro de salud a los 14 años de edad estando empadronado en Santa Amalia.
Criterios de exclusión: tener edad distinta a los 14 años en el momento de la vacunación (año de nacimiento distinto), desconocer la edad del adolescente vacunado (año de nacimiento desconocido) o ser residente de otra localidad diferente a Santa Amalia (Valdehornillos, Torrefresneda, Conquista del Guadiana, Hernán Cortés, Yelbes o Medellín).
Tamaño muestral y procedimiento de muestreo: un total de 1142 adolescentes de 14 años de edad residentes en la localidad de Santa Amalia. Vacunados 869, en el centro de salud 551 y 318 en el centro escolar. Al inicio se partía de una cantidad mayor de individuos, sin embargo, al aplicar los criterios de exclusión, se eliminaron a 142 niños de los vacunados de 1996 a 2007. Los adolescentes finalmente evaluados en este estudio son los que han sido vacunados, como se muestra en la Tabla 1, donde se representan las coberturas de vacunación.
| Tabla 1. Cobertura vacunal con vacuna Td en el CS Santa Amalia, 1996-2016 | ||||||||
|---|---|---|---|---|---|---|---|---|
| Centro escolar | ||||||||
| 1996 | 1997 | 1998 | 1999 | 2000 | 2001 | |||
| 85,7 | 56,3 | 108,0 | 100,0 | 78,7 | 78,1 | |||
| Centro de salud registro manual | ||||||||
| 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | |||
| 52,8 | 55,1 | 12,7 | 10,0 | 4,0 | 88,0 | |||
| Centro de salud registro informático | ||||||||
| 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 |
| 94,2 | 95,7 | 81,5 | 102,9 | 117,0 | 114,0 | 89,8 | 92,5 | 116,0 |

Recogida de datos y cálculos de cobertura: se confecciona una hoja de cálculo agrupando de forma numérica a los individuos vacunados por fecha de año de administración de la vacuna de tétanos para la población de estudio, así como para la población de referencia. Se diferencian tres grupos o periodos: centro escolar (1996-2001), centro de salud y registro manual (2002-2007) y centro de salud y registro informático (2008-2016). Finalmente se calcula la cobertura de vacunación expresada en porcentajes con un decimal.
Los datos de adolescentes vacunados que se utilizan para este estudio se obtuvieron de distintas fuentes. Los años 1996-2007 proceden de la consulta de las tarjetas de vacunación y los registros manuscritos archivados de las dosis de vacunas administradas que se realizaban con carácter mensual. A partir de 2008 y hasta 2016, los datos se obtienen del registro de dosis administradas y registradas históricamente en los aplicativos informáticos específicos del entorno JARA Atención Sanitaria (JARA-AS), el utilizado en el Servicio Extremeño de Salud.
El cálculo de la cobertura se realiza en función de la siguiente fórmula:
Cobertura vacunal (%) = población vacunada × 100 / población de referencia.
La población de referencia para los años de 1997 a 2016 incluidos se extrae de los datos del padrón del Instituto Nacional de Estadística (INE). Para el año 1996 se utiliza como población de referencia la aplicación poblacional CIVITAS, el Sistema Informático y Gestión Poblacional y de Gestión de Recursos Sanitarios en Extremadura. El INE empezó en 1997, y por tanto no tiene datos del padrón de 1996.
RESULTADOS
Las coberturas de vacunación de la dosis de recuerdo en adolescentes en la localidad de Santa Amalia alcanzadas están reflejadas en la Tabla 1, divididas en tres periodos según los diferentes ámbitos de administración o registro de vacunas: 1996-2001, 2002-2007 y 2008-2016.
Al comparar los datos de una manera global en cada uno de los periodos en esta localidad, puede apreciarse que en el grupo de vacunación en centro de salud con registro informático, 2008-2016, se encuentran las mejores cifras de vacunación frente a tétanos, seguido por el grupo de centro escolar, 1996-2001, con coberturas altas también. Y muy alejado de ellos, con los peores datos de cobertura, se encuentra el registro manual en centro de salud en el periodo 2002-2007. Durante los años 2004, 2005 y 2006 se observan las coberturas más bajas alcanzadas en la localidad extremeña de Santa Amalia (Área de Salud Don Benito-Villanueva). En estos tres años se pierde un mayor porcentaje de individuos (40, 44,4 y 75% respectivamente) porque tienen alguno de los criterios de exclusión.
DISCUSIÓN
Este estudio evalúa la cobertura vacunal frente al tétanos en la localidad de Santa Amalia, provincia de Badajoz, en los últimos 20 años (1996-2016), durante los cuales se ha vacunado a los adolescentes frente a tétanos en diferentes ámbitos y utilizando distintos métodos de registro. Entre 1996 y 2001, la vacunación se hacía en centro escolar y el registro era manual. Desde 2002 se administró la vacuna en centro de salud, primero con registro manual (2002-2007) y posteriormente informático (2008-2016).
La estrategia de vacunación en centro escolar para tétanos (1996-2001) lograba altas tasas de cobertura; se podría decir que era un método que funcionaba bien. En un mismo día se vacunaba de forma masiva prácticamente a toda la población diana. De hecho, las coberturas eran casi tan buenas como las actuales, conseguidas con el aplicativo informático JARA-AS desde su implantación en 2008. En el periodo de transición de vacunación en el centro escolar al centro de salud, 2002-2007, se han encontrado peores resultados. En este periodo, los adolescentes acudían al centro de salud para la revisión del niño sano en la que se incluía la vacunación de tétanos. Las posibles causas de este descenso dramático en la vacunación pudieran ser debidas al olvido de la revisión en el año en cuestión, el registro manual o su inadecuado sistema de archivo, de forma caótica y con poco rigor, en el que se encontraron mezclados meses y años, anotaciones incompletas (fecha de nacimiento, domicilio o localidad) y existencia de registros duplicados, entre otros.
Entre las limitaciones que se detectan, las vacunaciones realizadas en el centro educativo se hacían por curso escolar, es decir, no tenían en cuenta el año de nacimiento del adolescente o la localidad de residencia. Hubo que utilizar criterios de exclusión para homogeneizar ambas poblaciones. En 1997 se vacunó en dos periodos: en febrero al curso 1996/1997 y, entre los meses de octubre y noviembre, al correspondiente curso escolar 1997/1998.
Otra limitación encontrada para la correcta interpretación de estos datos es la existencia de ámbitos distintos en los que se realizaba la vacunación (centro escolar frente a centro de salud) y los problemas de registro, realizado de forma manual o informática. De hecho, en algunos años, las cifras de coberturas vacunales superiores al 100% pueden deberse a la inclusión en el numerador de niños vacunados que no están incluidos en la población de referencia o que no figuran como residentes en esa localidad. Se ha considerado como no vacunados a individuos que no cumplían estrictamente los criterios de inclusión establecidos y, probablemente, la mayoría de ellos sí estén correctamente vacunados.
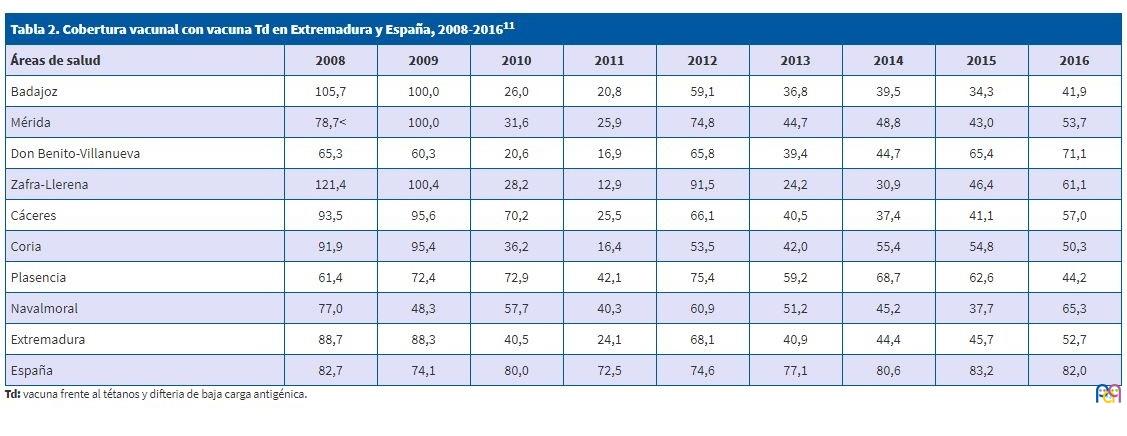
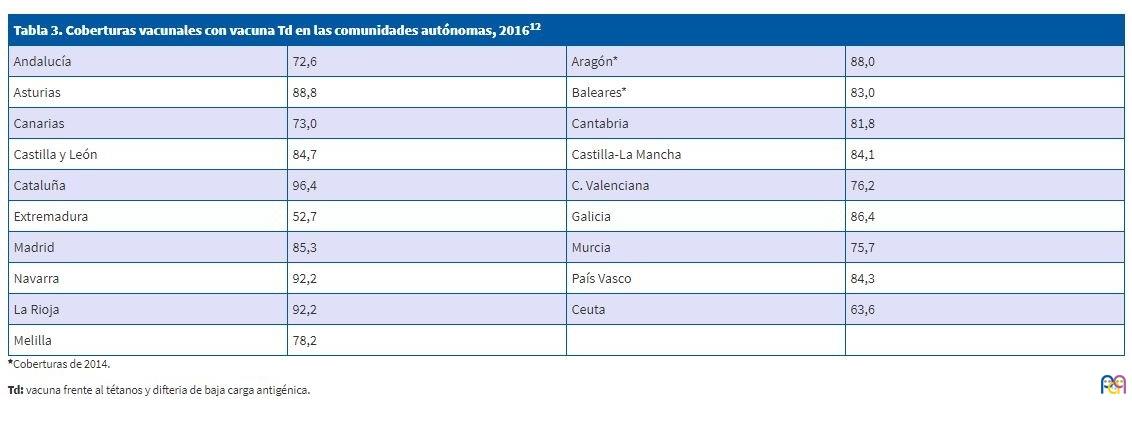
Enmarcando los datos de vacunación de Santa Amalia respecto a la cobertura en el Área de Salud de Don Benito-Villanueva, esta localidad tiene una alta tasa, siendo en todos los años muy superior a la del Área (Tabla 2). Se entiende como correctamente vacunado al niño al que se le administra la dosis de recuerdo en el mismo año en el que cumple la edad de 14 años. Al comparar esta localidad con los datos de vacunación nacional frente a tétanos en adolescentes en los últimos nueve años, la cobertura en Santa Amalia es similar o algo superior a la media española (Tabla 2). Si comparamos los datos obtenidos en 2016 (Tabla 2), se puede observar que mientras España presenta un 82,0% de cobertura, Extremadura logra el 52,7%. Está muy lejos de la media nacional, así como del resto de CC. AA., que presentan unos datos similares al estatal (Tabla 3). Aunque no hay que olvidar que para una correcta comparación a diferentes niveles (nacional, CC. AA. y áreas de salud) es necesario que las bases de datos utilizadas en el cálculo de coberturas se correspondan con la población real, y sería conveniente que fueran comparables entre sí.
| Tabla 2. Cobertura vacunal con vacuna Td en Extremadura y España, 2008-201611 | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Áreas de salud | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 |
| Badajoz | 105,7 | 100,0 | 26,0 | 20,8 | 59,1 | 36,8 | 39,5 | 34,3 | 41,9 |
| Mérida | 78,7 | 100,0 | 31,6 | 25,9 | 74,8 | 44,7 | 48,8 | 43,0 | 53,7 |
| Don Benito-Villanueva | 65,3 | 60,3 | 20,6 | 16,9 | 65,8 | 39,4 | 44,7 | 65,4 | 71,1 |
| Zafra-Llerena | 121,4 | 100,4 | 28,2 | 12,9 | 91,5 | 24,2 | 30,9 | 46,4 | 61,1 |
| Cáceres | 93,5 | 95,6 | 70,2 | 25,5 | 66,1 | 40,5 | 37,4 | 41,1 | 57,0 |
| Coria | 91,9 | 95,4 | 36,2 | 16,4 | 53,5 | 42,0 | 55,4 | 54,8 | 50,3 |
| Plasencia | 61,4 | 72,4 | 72,9 | 42,1 | 75,4 | 59,2 | 68,7 | 62,6 | 44,2 |
| Navalmoral | 77,0 | 48,3 | 57,7 | 40,3 | 60,9 | 51,2 | 45,2 | 37,7 | 65,3 |
| Extremadura | 88,7 | 88,3 | 40,5 | 24,1 | 68,1 | 40,9 | 44,4 | 45,7 | 52,7 |
| España | 82,7 | 74,1 | 80,0 | 72,5 | 74,6 | 77,1 | 80,6 | 83,2 | 82,0 |
| Tabla 3. Coberturas vacunales con vacuna Td en las comunidades autónomas, 201612 | |||
|---|---|---|---|
| Andalucía | 72,6 | Aragón* | 88,0 |
| Asturias | 88,8 | Baleares* | 83,0 |
| Canarias | 73,0 | Cantabria | 81,8 |
| Castilla y León | 84,7 | Castilla-La Mancha | 84,1 |
| Cataluña | 96,4 | C. Valenciana | 76,2 |
| Extremadura | 52,7 | Galicia | 86,4 |
| Madrid | 85,3 | Murcia | 75,7 |
| Navarra | 92,2 | País Vasco | 84,3 |
| La Rioja | 92,2 | Ceuta | 63,6 |
| Melilla | 78,2 | ||
Sería útil que se llevaran a cabo estudios más amplios de los datos de cobertura vacunal, empezando por el resto de las localidades del Área de Don Benito-Villanueva, pudiéndose ampliar a otras áreas de salud, con vistas a concretar las causas de estas bajas coberturas, y que ello contribuyera a mejorar las estrategias de vacunación y lograr coberturas vacunales que nos permitan acercarnos a la media estatal. A pesar de que el registro informático se implantó en toda Extremadura a la vez en el año 2008, existen grandes diferencias de cobertura aparentemente injustificables en todas las áreas de salud en diferentes años (Tabla 2). Durante los nueve años de uso de la aplicación informática (2008-2016), se ha conseguido vacunar correctamente a la mitad de los adolescentes de 14 años. Los datos son muy similares de unas áreas de salud a otras. Y en todas se encuentran años con una alta tasa de vacunación frente a otros con una cobertura muy baja, sin que se siga una tendencia clara en ninguna de ellas.
Esta baja cobertura debería alertar a las autoridades sanitarias y a los profesionales de la salud sobre la posible evolución de esta. Podría considerarse como una de las causas de la baja cobertura la disminución de las visitas al pediatra para la revisión del niño sano a los 14 años de edad.
Posibles mejoras para evitar la baja cobertura en dosis de refuerzo sería establecer una mejor estrategia de captación, haciendo coincidir su administración con visitas programadas recogidas en los programas de salud, además de alertar a los profesionales de medicina y enfermería sobre la necesidad de revisar y actualizar calendarios vacunales en cualquier visita e incluir avisos en la historia clínica electrónica, entre otras fórmulas que mejoren las actuales coberturas. Tal vez se alcanzaran mayores coberturas si se volvieran a realizar campañas de vacunaciones de tétanos en el centro escolar, como actualmente se está haciendo con la vacuna frente al virus del papiloma humano en niñas. Por otro lado, es importante contar con miembros en el equipo de Atención Primaria concienciados con la importancia de una correcta vacunación y llevar esta a cabo de manera rigurosa, anotando cada administración de vacuna, entradas y salidas de las unidades de almacenamiento y conservación de estas en los centros sanitarios. El concepto de salida de una vacuna abarca desde su administración hasta las pérdidas por roturas de cadena de frío o durante la manipulación en el momento de la vacunación, entre otras, que deben ser tenidas en cuenta a la hora de establecer la cobertura. Para ello es especialmente importante que tanto el personal de enfermería de Pediatría como los responsables de las vacunas, que en Extremadura son farmacéuticos, estén motivados adecuadamente para desempeñar su labor de manera rigurosa. La formación sobre vacunas es también un aspecto fundamental en este sentido.
Finalmente, dada la baja cobertura vacunal frente a tétanos en la dosis de recuerdo en adolescentes de 14 años en Extremadura durante los últimos años, aunque no es así en la localidad de Santa Amalia, habría que hacer estudios más amplios para evaluar la situación real y poder encontrar las verdaderas razones para estar tan alejados de la media nacional. Es obvio que existe la necesidad de actuar y realizar un cambio en la vacunación tal y como se está llevando a cabo hoy en día.
No ha sido objeto de este estudio el año 2017 puesto que para la obtención de la cobertura correspondiente el Ministerio de Sanidad, Consumo y Bienestar Social ha utilizado por primera vez otro sistema para su cálculo, acordado por la Comisión de Salud Pública en octubre de 2017.
CONFLICTO DE INTERESES
La autora declara no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
El contenido de este texto está basado en el trabajo práctico final del Curso de Diplomado en Salud Pública 2017 de la Escuela de Estudios de Ciencias de la Salud y de la Atención Sociosanitaria de Extremadura, acreditado por la Escuela Nacional de Sanidad, y la autora es la única responsable de la veracidad de los datos publicados.
ABREVIATURAS
CAV-AEP: Comité Asesor de Vacunas de la Asociación Española de Pediatría · CC. AA.: comunidades autónomas · GVAP: Plan Global de Acción en Vacunas · INE: Instituto Nacional de Estadística · OMS: Organización Mundial de la Salud · Td: vacuna de tétanos y difteria de baja carga antigénica · Tdpa: vacuna de tétanos, difteria y tosferina acelular de baja carga antigénica.
AGRADECIMIENTOS
A los siguientes profesionales sanitarios, por sus valiosas aportaciones tanto en la realización de un estudio de investigación como en la revisión del texto para su publicación: Adolfo Arias Senso, médico de familia del CS de Santa Amalia; Teresa Gallego-Martín, farmacéutica, bioquímica, doctora en Investigación Biomédica, investigadora posdoctoral en la Universidad de Pittsburgh (EE. UU.); Eulalio Ruiz Muñoz, médico y técnico superior de Salud Pública de la Dirección General de Salud Pública del Servicio Extremeño de Salud.
BIBLIOGRAFÍA
- Grupo de trabajo recomendaciones Td 2017. Ponencia de Programa y Registro de Vacunaciones. Recomendaciones de utilización de vacunas Td. En: Ministerio de Sanidad, Servicios Sociales e Igualdad [en línea] [consultado el 14/10/2019]. Disponible en www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/docs/TetanosDifteria_2017.pdf
- Ponencia de Programa y Registro de Vacunaciones. Vacunación en adultos. Recomendaciones. Vacuna de difteria y tétanos. Actualización 2009. En: Ministerio de Sanidad y Consumo [en línea] [consultado el 14/01/2019]. Disponible en www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/docs/TetanosDifteria_2009.pdf
- Torres MM, Ramos E, Bonillo A, Sánchez F. Estrategia de seguimiento de la vacunación antitetánica en adultos. Vacunas. 2004;5:61-4.
- Tuells J. Controversias sobre vacunas en España, una oportunidad para la vacunología social. Gac Sanit. 2016;30:1-3.
- Moreno-Pérez D, Álvarez FJ, Arístegui J, Cilleruelo MJ, Corretger JM, García N, et al. Calendario de vacunaciones de la Asociación Española de Pediatría (CAV-AEP): recomendaciones 2017. An Pediatr (Barc). 2017;86:98.e1-98.e9.
- Limia-Sánchez A, Andreu MM, de Viarce Torres de Mier M, Navarro-Alonso JA. Nuevo calendario de vacunación para España, 2016 (Parte 1). Rev Esp Salud Pública. 2016;90:e20001.
- Navarro-Alonso JA, Taboada-Rodríguez JA, Limia-Sánchez A. Nuevo calendario de vacunación para España, 2016 (Parte 2). Rev Esp Salud Pública. 2016;90:e20002.
- Dirección General de Salud Pública. Programa de vacunaciones en Extremadura; año 2017. En: Servicio Extremeño de Salud, Consejería de Sanidad y Políticas Sociales, Junta de Extremadura [en línea] [consultado el 14/10/2019]. Disponible en https://saludextremadura.ses.es/filescms/ventanafamilia/uploaded_files/CustomContentResources/Programas%20de%20vacunaciones%20en%20Extremadura.%20DG%20de%20Salud%20P%C3%BAblica.%202017.pdf
- Mauro Ramos J. Declarado un caso de tétanos en adulto sin vacunar en Extremadura [Noticias en portal del SES]. 4 de julio de 2017 [consultado el 31/07/2017]. [Acceso restringido en Internet; solo accesible para personal del Servicio Extremeño de Salud]
- Grupo de Patología Infecciosa de la AEPap. Posicionamiento de la Asociación Española de Pediatría de Atención Primaria sobre vacunación infantil: análisis crítico y propuestas de mejora. 2016. En: Acta Sanitaria [en línea] [consultado el 14/10/2019]. Disponible en www.actasanitaria.com/wp-content/uploads/2016/01/documento-de-posicionamiento.pdf
- Tabla 2A Coberturas de vacunación de recuerdo. España 2008-2016. En: Ministerio de Sanidad, Consumo y Bienestar Social [en línea] [consultado el 14/10/2019]. Disponible en www.mscbs.gob.es/en/profesionales/saludPublica/prevPromocion/vacunaciones/docs/CoberturasVacunacion/Tabla2.pdf
- Tabla 6: Coberturas de vacunación de refuerzo en niños de 4 a 14 años. Comunidades autónomas, 2016. En: Ministerio de Sanidad, Servicios Sociales e Igualdad [en línea] [consultado el 14/10/2019]. Disponible en www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/docs/CoberturasVacunacion/Todas_las_tablas2016.pdf