

Trastorno por déficit de atención e hiperactividad (TDAH) en niños escolarizados de 6 a 17 años
Leónidas José Llanos Lizcanoa, Darwin José García Ruiza, Henry J. González Torresb, Pedro Puentes Rozoc
aResidente de Psiquiatría. Facultad de Ciencias de la Salud. Universidad Simón Bolívar. Barranquilla. Colombia.
bFacultad de Ciencias de la Salud. Universidad Simón Bolívar. Barranquilla. Colombia.
cGrupo de Neurociencias del Caribe. Unidad de Neurociencias Cognitivas. Universidad del Atlántico-Universidad Simón Bolívar. Barranquilla. Colombia.
Correspondencia: LJ Llanos. Correo electrónico: lllanos13@unisimon.edu.co
Cómo citar este artículo: Llanos Lizcano LJ, García Ruiz DJ, González Torres HJ, Puentes Rozo P. Trastorno por déficit de atención e hiperactividad (TDAH) en niños escolarizados de 6 a 17 años. Rev Pediatr Aten Primaria. 2019;21:e101-e108.
Publicado en Internet: 01-08-2019 - Número de visitas: 35935
Resumen
Objetivo: se buscó determinar la prevalencia del trastorno por déficit de atención e hiperactividad (TDAH) en niños de entre 6 a 17 años escolarizados en Barranquilla, para hacer una caracterización epidemiológica del trastorno en la región Caribe colombiana.
Materiales y métodos: se tomaron 383 niños de una institución educativa a los que se les aplicaron pruebas de tamizaje (Checklist y BASC). Aquellos sujetos que registraron una puntuación sugestiva de alguna alteración fueron reprogramados para la realización de la evaluación por medio de la entrevista estructurada (MINI).
Resultados: de los 383 sujetos evaluados inicialmente, 178 resultaron ser casos de algún tipo de alteración, de estos se confirmó que 59 (15%) tenían diagnóstico de TDAH, con una proporción de 38 varones y 21 mujeres, lo que arroja una relación 2:1, la distribución por subtipos se dio en 7,3% combinado, 5% inatento y 3,1% hiperactivo. En total, el 23% de los sujetos evaluados presentaron algún trastorno neuropsiquiátrico y se encontró una relación estadísticamente significativa entre el subtipo inatento con la agorafobia y los episodios depresivos, entre el subtipo hiperactivo con el trastorno oposicionista desafiante y el trastorno de angustia y entre la depresión y el riesgo de suicidio con el subtipo combinado.
Conclusiones: la prevalencia del TDAH en Barranquilla presenta un comportamiento similar a otras regiones del país, tanto en la prevalencia como en la distribución por subtipos, relación por sexo, tipos de comorbilidades. Estos datos no están sujetos a factores psicosociales, lo que confirmaría la teoría de tener una etiología multifactorial.
Palabras clave
● Trastorno por déficit de atención e hiperactividad ● Trastornos del comportamiento ● Trastornos del neurodesarrollo ● Trastornos neuropsiquiátricos en la infanciaINTRODUCCIÓN
El trastorno por déficit de atención e hiperactividad (TDAH) es un síndrome neurológico frecuente caracterizado por hiperactividad, impulsividad y pobre capacidad de atención, alteraciones que son inadecuadas para el grado de desarrollo del niño1. Es uno de los diagnósticos más frecuentes entre niños y adolescentes, y el más común en la juventud2. No hay datos precisos sobre la prevalencia, pero se estima entre el 2 y el 12% en infantes2-7 y entre el 2,5 y el 5% en adultos5-11.
Las regiones con mayor variabilidad en los rangos de prevalencia son África y Suramérica, que además tienen las mayores cifras de prevalencia, las cuales de manera general se encuentran muy por encima de la media12. Según la Liga Latinoamericana para el Estudio del TDAH, en Latinoamérica hay 36 millones de personas afectadas, con menos de una cuarta parte recibiendo un manejo adecuado13.
En Colombia, según el estudio de Hoai Danh Pham, publicado en el 2015, al citar el artículo del doctor Pineda del año 2001, Colombia resulta ser el país con la prevalencia de TDAH más alta a nivel mundial, con un 17,1% de la población6,14. Este dato es igualmente confirmado por Vélez en 2012, cuando describe que la prevalencia en Colombia es mayor que en otros países, además de plantear que se necesitan más estudios estructurados para unificar criterios y poder establecer una prevalencia real en el país, al encontrarse datos muy variados en diferentes estudios realizados en diferentes ciudades y bajo diferentes metodologías15.
Este trastorno está asociado a una alteración en el desarrollo armónico de los individuos afectados, asociándose a alteraciones familiares importantes13; se sabe que hasta un 50% de los niños con TDAH tienen pobres relaciones con sus pares y hasta un 70% de los niños con TDAH que cursan el tercer grado no tienen amistades por sus grandes limitaciones para participar de manera armónica en los intercambios sociales propios de la edad16. Al preguntar a los familiares de personas con TDAH sobre los impedimentos y discapacidades que pudieran asociarse al trastorno, estos reportaron que el TDAH tiene un impacto negativo sobre la escolaridad, la vida diaria, el intercambio social y las relaciones familiares, además impactar de manera negativa sobre el autoestima17. Estas alteraciones en el desarrollo social y escolar son algunas de las principales causas por las que el TDAH se asocia a una mayor tasa de uso y abuso de drogas al comparar a la población con TDAH con controles sin TDAH18.
La importancia que recae sobre el TDAH se debe a que, al ser una patología cuyas manifestaciones se presentan en la infancia, genera una serie de alteraciones en la funcionalidad personal, escolar y social, que conllevan al individuo en plena etapa de formación de su personalidad e identidad, a interactuar de manera errónea con la sociedad, atrayendo sobre si una impronta que sin el manejo adecuado, puede llevar a su marginación social16,19-24. Si bien diferentes estudios han demostrado que estos pacientes presentan múltiples cualidades en áreas creativas y artísticas25, también es importante resaltar la labor que cumplen los colegios con currículos estandarizados, rígidos, en comparación con escuelas de cortes más especializadas en educación artística, vanguardista y estimulante, con aulas y horarios flexibles que permiten una mejor adaptación de estos niños, caso contrario a lo que se encuentra en la región.
Por tal razón, la intervención temprana en niños y adolescentes es de vital importancia, con el fin de disminuir las repercusiones en la adolescencia y en la adultez, que se presentan en forma de desorganización en trabajos escolares, bajo rendimiento escolar y laboral, dificultad para culminar tareas, dificultad para trabajar de forma independiente, comportamientos arriesgados, autoestima baja por fracasos en muchas áreas de su vida, riesgo de consumo de sustancias psicoactivas o inicio de vida sexual temprana, entre otros1.
Es por este motivo por el que se realizó la primera aproximación a la realidad epidemiológica del TDAH a nivel local, teniendo en cuenta las características sociales y culturales de una población que difiere de manera significativa de las poblaciones al interior del país26,27. Además, este estudio se realizó con la aplicación de diferentes test de aproximación diagnóstica, para poder obtener los casos probables, pero el diagnóstico definitivo se realizará por medio de una entrevista clínica estructurada (MINI), aumentando la validez y veracidad del diagnóstico, al no estar limitado simplemente a la realización de encuestas o escalas, las cuales, como se ha mencionado anteriormente, están sujetas a variaciones según las modificaciones de los criterios diagnósticos.
Se busca que este primer estudio siente un precedente a nivel local que permita replicar estudios similares en otras ciudades y además sea la puerta de entrada y el justificante suficiente para poder ampliar en próximos estudios, con mayor número de muestra, que permita correlacionar con un mayor número de factores de riesgo, trastornos asociados y comorbilidades para poder elaborar guías de manejo específicas de la población, las cuales puedan ser incluidos en los planes de política pública de primera infancia y poder abordar a la población más vulnerable desde un punto de vista multimodal y por ende, completo, lo que disminuiría los daños y las repercusiones sobre los sujetos afectados15.
METODOLOGÍA
Se realizó un estudio de tipo analítico, aplicado con enfoque cuantitativo, prospectivo, de corte transversal. El área de estudio fue una escuela de Barranquilla (Colombia). Se realizó un muestreo aleatorio simple para determinar el número de niños que evaluar. La muestra fue de 383 niños, de los cuales 178 niños presentaron alteraciones neuroconductuales que ameritaron la evaluación MINI, previo consentimiento informados de sus padres y asentimiento por parte de los menores. Ninguno de los niños evaluados debía estar diagnosticado o en tratamiento para cualquier trastorno neuropsiquiátrico.
Una vez firmado el consentimiento informado por los padres y obtenido el asentimiento informado de los niños, la evaluación fue realizada del siguiente modo: para determinar si había algún tipo de alteración neuroconductual se les aplicaron consecutivamente el Sistema de Evaluación de Comportamiento en los Niños (BASC, Behavior Assessment System for Children) y la Lista de Síntomas para el Diagnóstico de TDAH (CheckList ADHD)14,28-31.
Aquellos niños que presentaron alteraciones tanto en el BASC como en la ChekList, se les realizó una entrevista estructurada diagnóstica de corta duración con un tiempo promedio de 15 minutos, siguiendo los protocolos de MINI Entrevista Neuropsiquiátrica Internacional (MINI) para niños escolares y adolescentes (NA), versión en español 5.0.0 DSM-IV.
Los resultados del tamizaje realizado con el BASC y CheckList ADHD y los resultados MINI se organizaron en una matriz, aplicándose las medidas de tendencia central: frecuencia observada, media y desviación estándar (±) por subtipo de TDAH. Asimismo, se realizó un análisis de asociación entre sexo, rango etáreo y subtipos utilizando un χ2. Igualmente se realizó un análisis de correspondencias simples entre el subtipo de TDAH y las comorbilidades. Esto se realizó en el paquete estadístico R-CRAN. Esta investigación estuvo supervisada por el Comité de Bioética.
RESULTADOS
En cuanto a las características sociodemográficas de los niños que participaron en el estudio, la edad promedio es de 11 ± 3 años. El 52,75% fueron varones (n = 91). El 60,11% de los niños tenía una edad comprendida entre los 6-11 años (n = 107). Y el 15% (intervalo de confianza [IC]: 12 a 18) cumplieron los criterios para diagnóstico de TDAH, tal como se evidencia en la Tabla 1.
| Tabla 1. Prevalencia de TDAH en la población evaluada | |||
|---|---|---|---|
| Frecuencia observada | Frecuencia porcentual | Intervalo de confianza | |
| Sanos | 205 | 54% | 49-59% |
| Sano MINI | 87 | 23% | IC 19-27% |
| TDAH | 59 | 15% | IC 12-19% |
| Otro diagnóstico | 32 | 8% | IC 6-11% |
| Total | 383 | 100% | - |

Es de observar que el 8% (IC: 6 a 10) de los sujetos que ameritaron evaluación MINI presentaron criterios para otros trastorno neuropsiquiátricos. Los niños con TDAH y los otros diagnósticos, suman el 23%, es decir, que casi un cuarto de la población evaluada presenta un diagnóstico de alguna patología mental, subrayando que esta es menor de edad.
Del grupo que cumplió criterios para TDAH, el 62,7% (n = 37) su rango etario estuvo entre 6-11 años, se encontró diferencia estadísticamente significativa (p <0,01). Asimismo, se observó una predominancia significativa del diagnóstico para el sexo masculino (64,4%, p <0,01).
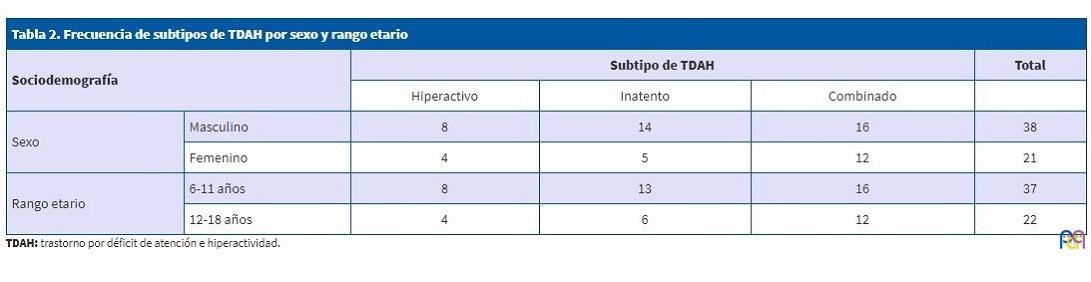
Para el diagnóstico por subtipo, del total de la muestra (n = 59), se encontró que la prevalencia para el subtipo hiperactivo fue del 20%, para el subtipo inatento del 32% y para el subtipo combinado del 47%. No se encontrón una asociación significativa entre los subtipos y el sexo (χ2: 1,38; p >0,05), así como para los subtipos y el rango etario (χ2: 0,71; p >0,05).
| Tabla 2. Frecuencia de subtipos de TDAH por sexo y rango etario | |||||
|---|---|---|---|---|---|
| Sociodemografía | Subtipo de TDAH | Total | |||
| Hiperactivo | Inatento | Combinado | |||
| Sexo | Masculino | 8 | 14 | 16 | 38 |
| Femenino | 4 | 5 | 12 | 21 | |
| Rango etario | 6-11 años | 8 | 13 | 16 | 37 |
| 12-18 años | 4 | 6 | 12 | 22 | |
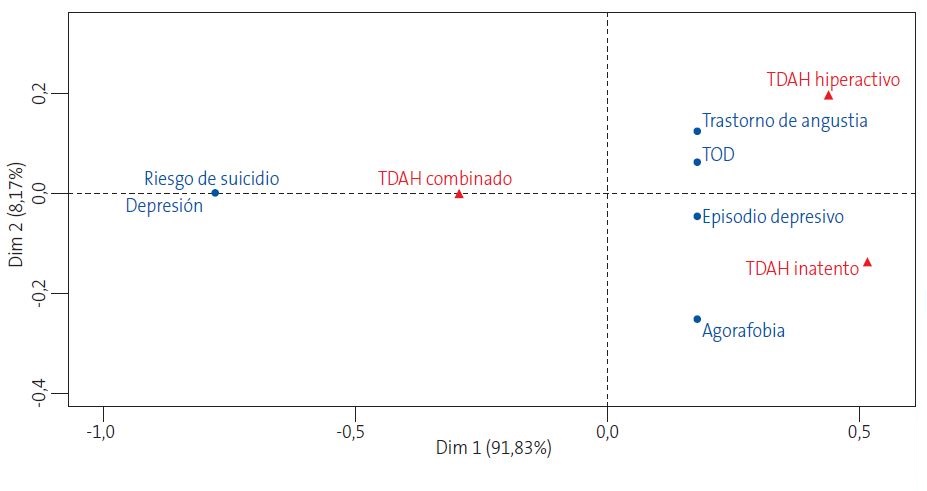
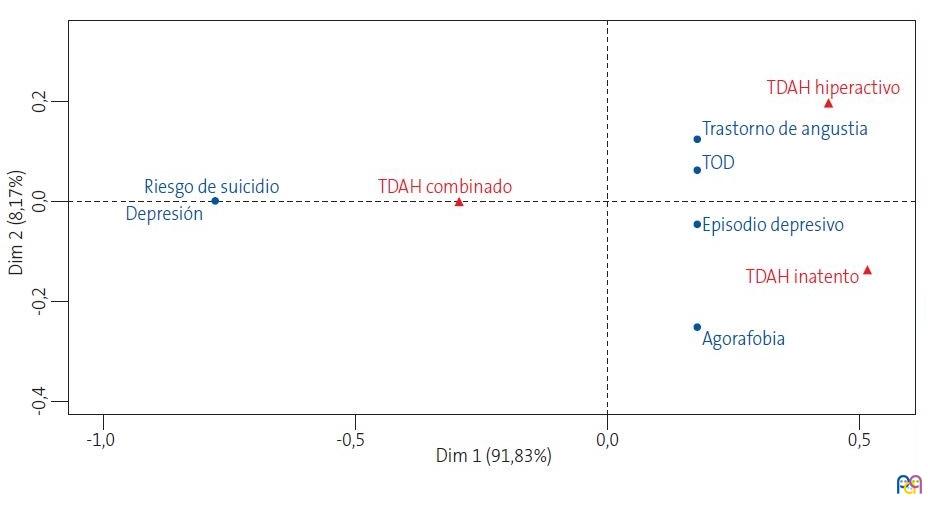
Como se puede observar, las comorbilidades asociadas al subtipo hiperactivo fueron trastorno de angustia y trastorno oposicionista desafiante, mientras que el inatento estuvo relacionado espacialmente con los episodios depresivos y la agorafobia. Es de notar que el subtipo combinado estuvo en la mitad del eje de dispersión, indicando la evidente combinación de los otros dos subtipos (hiperactivo e inatento), en estos pacientes se puede observar que la depresión va de la mano con el riesgo suicida.
| Figura 1. Análisis de correspondencias simples entre los subtipos de trastorno por déficit de atención e hiperactividad y las comorbilidades |
|---|
 |
Existen otras características evaluadas que merecen ser mencionadas: ninguno respondió afirmativamente sobre provocar de manera intencional incendios, engañar a otras personas para quitarles dinero u obtener objetos ajenos, utilizar armas u objetos que puedan hacer daño a otros, robar o atracar usando armas o amenazando a otros, forzar o amenazar a alguien para tener relaciones sexuales, ni ser cruel con los animales o gustarle hacerlos sufrir.
DISCUSIÓN
Los estudios de prevalencia son de gran importancia, especialmente en áreas que presentan vacíos de conocimiento. Si bien el TDAH es uno de los trastornos del neurodesarrollo más frecuentes en la infancia, no hay datos epidemiológicos suficientes en la literatura médica que permitan tener un dato fehaciente, por lo cual este estudio se ha enfocado en esta temática1,2. En Colombia hay estudios limitados acerca de la prevalencia del TDAH, y los que existen están centrados en la población del interior del país; aun no existen datos epidemiológicos en la región Caribe colombiana que nos permitan evaluar el comportamiento de esta entidad y poder hacer comparaciones en relación con lo encontrado por otros autores a nivel mundial y nacional, por lo que nuestra investigación quiere lograr ser la primera aproximación para estimar la prevalencia del TDAH en la población escolarizada de la ciudad de Barranquilla y ser un impulso para el desarrollo de nuevos trabajos de investigación a futuro de esta temática.
El TDAH tiene una prevalencia variada a nivel mundial, para algunos se estima que este alrededor de un 7,2%32), sin embargo, otros estudios reportan un amplio rango de entre el 4 y el 13,3%3,33. En Colombia la prevalencia se aleja de lo descrito a nivel mundial, dentro de lo evaluado, se ha encontrado una prevalencia entre el 15-17%1,14. El presente estudio corrobora los datos reportados en los estudios realizados en nuestro país, lo que apoya nuestros resultados del 15% de la población estudiada, esto nos deja vislumbrar un panorama de alto riesgo en la salud mental para escolares en la ciudad de Barranquilla, así como en Colombia.
En cuanto a la distribución por sexos, encontramos que el TDAH fue más frecuente en hombres que en mujeres, con una relación de 2:1, información que se asemeja a lo estipulado a nivel mundial y en otras poblaciones colombianas1,14,34. De igual forma, la prevalencia por rango de edad hallada en nuestro estudio arroja una mayor proporción en los niños menores (6 a 11 años) 62,7% en comparación a los sujetos mayores de 12 años 37,3%; estos hallazgos son similares a los descritos por otros autores7, y que algunos investigadores explican por las alteraciones en la maduración cerebral, que según los expertos se presenta los pacientes con TDAH mostrando niveles de maduración y engrosamiento cerebral con entre dos y tres años de retraso en referencia a los niños sin TDAH35.
Cornejo JW et al. describieron en la población de Sabaneta, Antioquía, en el año 2005, que la frecuencia de presentación según los subtipos fue primero el combinado, seguido por el inatento y finalmente el hiperactivo, lo que coincide con lo encontrado en nuestro estudio, presentando distribuciones y proporciones similares, del 7,3, el 5,0 y el 3,1% respectivamente1.
Dentro de los 16 trastornos psiquiátricos estudiados, según la selección de la entrevista estructurada (MINI), como comorbilidades, encontramos que la alteración más frecuente es el trastorno oposicionista desafiante con un 44,06%, lo cual es un hallazgo común al revisar la literatura médica21,36, y carga una importancia significativa ya que es uno de los factores de peor pronóstico para el TDAH. Ese trastorno se caracteriza por la presencia de conductas hostiles hacia figuras de autoridad, desobediencia y actitudes retadoras, que conllevan a una serie de alteraciones familiares, escolares y sociales, que en últimas se asocian a conductas delictivas y de riesgo.
Los trastornos del estado del ánimo fueron la segunda causa de comorbilidad más frecuente entre la población de niños con TDAH con una presentación del 30,5%, hallazgo similar al estudio realizado por Artigas-Pallares en 2003. Birmaher, en su publicación de 2007 describe que el TDAH suele concurrir de manera bastante frecuente con los trastornos del estado del ánimo. La relación causa efecto de la comorbilidad de estos trastornos con el TDAH no está descifrada del todo, algunos autores responsabilizan las alteraciones en las esferas familiares, educacionales y sociales como por ejemplo las discusiones con los padres y demás familiares, las dificultades para relacionarse con pares y el bajo rendimiento académico a una disminución de la autoestima13. Para otros autores, las alteraciones a nivel molecular y genético propias del TDAH son las que se asocian a las alteraciones del estado de ánimo, que pueden o no estar influidas por factores externos37.
Teniendo en cuenta que, los trastornos psiquiátricos más frecuentes en la población infantil son los de ansiedad, en nuestro estudio su comorbilidad con TDAH el resultado fue de 20,3%, se va a encontrar con un porcentaje elevado, esto es explicado además de lo anteriormente mencionado, a que a pesar de que estos dos trastornos se heredan de forma independiente, las hipótesis genéticas han evaluado que se potencian entre ellos1.
Actualmente no existen marcadores biológicos para realizar de manera segura el diagnóstico de TDAH, y el uso de test o evaluaciones clínicas, se considera poco objetivo, al existir el riesgo de cometer errores o imprecisiones al momento del diagnóstico, en consecuencia se dificulta la comparación de las cifras de prevalencia del TDAH resultante de estudios tanto nivel nacional como a nivel mundial1,22,38.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo. Este artículo es parte del trabajo de tesis de la especialidad de Psiquiatría de Leónidas José Llanos Lizcano y Darwin José García Ruiz. Fue financiado con recursos de los investigadores.
ABREVIATURAS
BASC: Sistema de Evaluación de Comportamiento en los Niños · CheckList ADHD: Lista de Síntomas para el Diagnóstico de TDAH · IC: intervalo de confianza · MINI: MINI Entrevista Neuropsiquiátrica Internacional · TDAH: trastorno por déficit de atención e hiperactividad.
BIBLIOGRAFÍA
- Cornejo Ochoa JW, Osío Uribe O, Sánchez Mosquera Y, Carrizosa J, Sánchez,Grisales H, et al. Prevalencia del trastorno por déficit de atención-hiperactividad en niños y adolescentes colombianos. Rev Neurol. 2005;40:716.
- Parker A, Corkum P. ADHD Diagnosis: as simple as administering a questionnaire or a complex diagnostic process? J Atten Disord. 2012;20:478-86.
- Polanczyk G, De Lima MS, Horta BL, Biederman J, Rohde LA. The worldwide prevalence of ADHD: A systematic review and metaregression analysis. Am J Psychiatry. 2007;164:942-8.
- Russell G, Rodgers LR, Ukoumunne OC, Ford T. Prevalence of parent-reported ASD and ADHD in the UK: Findings from the millennium cohort study. J Autism Dev Disord. 2014;44:31-40.
- Wolraich ML, McKeown RE, Visser SN. The prevalence of ADHD: its diagnosis and treatment in four school districts across two states. J Atten Disord. 2014;18:563-75.
- Pham HD, Nguyen HBH, Tran DT. Prevalence of ADHD in primary school children in Vinh Long, Vietnam. Pediatr Int. 2015;57:856-9.
- Huang CL, Weng S, Ho C. Gender ratios of administrative prevalence and incidence of attention-de fi cit/hyperactivity disorder (ADHD) across the lifespan: a nationwide population-based study in Taiwan. Psychiatry Res. 2016;244:382-7.
- Gao Q, Qian Y, He X, Sun L, Chang W, Li Y. Childhood predictors of persistent ADHD in early adulthood : Results from the fi rst follow-up study in China. Psychiatry Res. 2015;230:905-12.
- Demontis D, Walters RK, Martín J, Mattheisen M, Als TD, Agerbo E, et al. Discovery of the first genome-wide significant risk loci for ADHD. Nat Genet. 2019;51:63-75.
- Marwaha S, Thompson A, Bebbington P. Adult attention deficit hyperactivity symptoms and psychosis: Epidemiological evidence from a population survey in England. Psychiatry Res. 2015;229:49-56.
- Smalley SL, Loo SK, Hale TS. Mindfulness and attention deficit hyperactivity disorder. J Clin Psychol. 2009;65:1087-98.
- Polanczyk GV, Willcutt EG, Salum GA, Kieling C, Rohde LA. ADHD prevalence estimates across three decades: An updated systematic review and meta-regression analysis. Int J Epidemiol. 2014;43:434-42.
- De la Peña F, Palacio J, Barragán E. Declaración de Cartagena para el Trastorno por Déficit de Atención con Hiperactividad (TDAH): rompiendo el estigma. Rev Ciencias Salud. 2010;8:93-8.
- Pineda DA, Lopera F, Henao GC, Palacio JD, Castellanos FX. Confirmación de la alta prevalencia del trastorno por déficit de atención en una comunidad colombiana. Rev Neurol. 2001;32:217-22.
- Vélez-Álvarez C, Vidarte Claros JA. Trastorno por déficit de atención e hiperactividad (TDAH), una prolematica a abordar en la política pública de primera infancia en Colombia. Rev Salud Pública. 2012;14:113-28.
- Wehmeier PM, Schacht A, Barkley RA. Social and emotional impairment in children and adolescents with adhd and the impact on quality of life. J Adolesc Heal. 2010;46:209-17.
- Caci H, Asherson P, Donfrancesco R. Daily life impairments associated with childhood/adolescent attention-deficit/hyperactivity disorder as recalled by adults: results from the European Lifetime Impairment Survey. Eur Psychiatry. 2014;29:316-23.
- Biederman J, Wilens TE, Mick E, Faraone SV, Spencer T. Does attention-deficit hyperactivity disorder impact the developmental course of drug and alcohol abuse and dependence? Biol Psychiatry. 1998;44:269-73.
- Salmeron PA. Childhood and adolescent attention-deficit hyperactivity disorder: Diagnosis, clinical practice guidelines, and social implications. J Am Acad Nurse Pract. 2009;21:488-97.
- Abikoff H, Hechtman L, Klein RG. Symptomatic improvement in children with ADHD Treated with long-term methylphenidate and multimodal psychosocial treatment. J Am Acad Child Adolesc Psychiatry. 2004;43:802-11.
- Barra FE de la, Vicente B, Saldivia S, Melipillan R. Epidemiology of ADHD in Chilean children and adolescents. Atten Defic Hyperact Disord. 2013;5:1-8.
- Artigas Pallarés J. Comorbilidad en el trastorno por déficit de atención/hiperactividad. Rev Neurol. 2003;36:68-78.
- Yoshimasu K, Barbaresi WJ, Colligan RC. Childhood ADHD is strongly associated with a broad range of psychiatric disorders during adolescence: a population-based birth cohort study. J Child Psychol Psychiatry Allied Discip. 2012;53:1036-43.
- Hong SB, Kim JW, Choi BS. Blood manganese levels in relation to comorbid behavioral and emotional problems in children with attention-deficit/hyperactivity disorder. Psychiatry Res J. 2014;220:418-25.
- Cramond B. Attention-deficit hyperactivity disorder and creativity - what is the connection? J Creat Behav. 1994;28:193-210.
- Song J, Leventhal BL, Koh Y. Cross-cultural aspect of behavior assessment system for Children-2, Parent Rating Scale-Child: standardization in Korean children. Yonsei Med J. 2017;58:439-48.
- Timimi S, Taylor E. ADHD is best understood as a cultural construct. Br J Psychiatry. 2004;184:8-9.
- Pineda DA, Lopera F, Palacio JD, Ramírez D, Henao GC. Prevalence estimations of attention-deficit/hyperactivity disorder: differential diagnoses and comorbidities in a Colombian sample. Int J Neurosci. 2003;113:49-71.
- Pineda D a, Kamphaus RW, Mora O, Restrepo MA, Puerta IC, Palacio LG, et al. Sistema de evaluación multidimensional de la conducta. Escala para padres de niños de 6 a 11 años, versión colombiana. Rev Neurol. 1999;28:672-81.
- Pineda D, Acosta J, Cervantes-Henríquez M. Conglomerados de clases latentes en 408 miembros de 120 familias nucleares de Barranquilla con un caso índice afectado de trastorno de atención hiperactividad (TDAH). Acta Neurol Col. 2016;32:275-84.
- Pineda DA, Henao GC, Puerta IC, Mejía SE. Uso de un cuestionario breve para el diagnóstico de deficiencia atencional. Rev Neurol. 1999;28:365-72.
- Thomas R, Sanders S, Doust J, Beller E. Prevalence of attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. Pediatrics. 2015;135:e994-1001.
- Willcutt EG. The prevalence of DSM-IV attention-deficit/hyperactivity disorder: a meta-analytic review. Neurotherapeutics. 2012;9:490-9.
- Barrios O, Matute E, Ramírez-Dueñas ML, Chamorro Y, Trejo S, Bolaños L. Características del trastorno por déficit de atención e hiperactividad en escolares mexicanos de acuerdo con la percepción de los padres. Suma Psicol. 2016;23:101-8.
- Shaw P, Eckstrand K, Sharp W. Attention-deficit/hyperactivity disorder is characterized by a delay in cortical maturation. Proc Natl Acad Sci U S A. 2007;104:19649-54.
- Joffre-Velázquez VM, García-Maldonado G, Martínez-Perales G. Trastorno por déficit de la atención e hiperactividad. Un estudio descriptivo en niños mexicanos atendidos en un hospital psiquiátrico. Bol Med Hosp Infant Mex. 2007;64:153-60.
- Dark C, Homman-Ludiye J, Bryson-Richardson RJ. The role of ADHD associated genes in neurodevelopment. Dev Biol. 2018;438:69-83.
- Gorga M. Trastorno por déficit de atención con hiperactividad y el mejoramiento cognitivo. ¿Cuál es la responsabilidad del médico? Rev Bioét. 2013;21:241-50.