

Prevalencia de caries dental en escolares de educación infantil de una zona de salud con nivel socioeconómico bajo
Ana Cubero Santosa, Isabel Lorido Canob, Almudena González Huéscarb, M.ª Ángeles Ferrer Garcíac, M.ª Dolores Zapata Carrascod, Juan Luis Ambel Sánchezc
aPediatra. CS El Progreso. Badajoz. España.
bEnfermera. CS El Progreso. Badajoz. España.
cUnidad de Salud Bucodental de las Zonas Básicas San Fernando, Gévora y El Progreso. Badajoz. España.
dDirección Programas Salud Bucodental. Servicio Extremeño de Salud. Badajoz. España.
Correspondencia: A Cubero. Correo electrónico: anacuberosantos@gmail.com
Cómo citar este artículo: Cubero Santos A, Lorido Cano I, González Huéscar A, Ferrer García MA, Zapata Carrasco MD, Ambel Sánchez JL. Prevalencia de caries dental en escolares de educación infantil de una zona de salud con nivel socioeconómico bajo. Rev Pediatr Aten Primaria. 2019;21:e47-e59.
Publicado en Internet: 17-06-2019 - Número de visitas: 85204
Resumen
Introducción: la caries dental es una enfermedad crónica, con elevada prevalencia en preescolares españoles. La falta de higiene, la alimentación inadecuada y las algias dentarias son problemas de salud frecuentes en nuestra zona básica de salud según los resultados del análisis de situación de salud. El objetivo de este trabajo es estudiar la prevalencia de caries dental en niños de tres a cinco años en nuestra zona básica de salud mediante un estudio descriptivo transversal.
Material y métodos: se realiza la inspección bucodental por dentista y la recogida de datos por higienista dental en escolares de primer, segundo y tercer curso de Educación Infantil. La variable principal estudiada es la presencia de caries. Los datos son registrados en fichas individuales y volcados en una base de datos elaborada en el programa SPSS, donde se realiza el análisis descriptivo de los mismos.
Resultados: de 150 niños escolarizados en educación infantil en la zona, se revisan 121 que acuden a clase el día que se realiza la revisión (80,7%). En primer curso un 46% de los niños presentan caries, en segundo un 40,5% y en tercero encontramos un 77,3% de niños con caries en dientes temporales y un 20,8% en definitivos.
Conclusiones: las cifras de caries en nuestra zona básica de salud son altas, muy superiores a los datos nacionales. Es necesario aumentar las actividades preventivas en la primera infancia, en especial en las zonas de menor nivel social como la nuestra.
Palabras clave
● Caries dental ● Dientes definitivos ● Dientes temporales ● Higiene bucalINTRODUCCIÓN
La caries dental es una enfermedad de alta prevalencia y uno de los principales problemas de salud pública a nivel mundial1-4. Es el proceso patológico que con más frecuencia sufre el diente y es considerada como la primera causa de consulta odontológica en todos los grupos de edad1,2. Es la enfermedad crónica más frecuente en la infancia, con una elevada prevalencia en preescolares españoles5-7.
La caries es una enfermedad multifactorial en la que existe la interacción de tres factores principales: el huésped (la higiene bucal, la saliva y las características de los dientes), la microflora y el sustrato (dieta), que condiciona la desmineralización del tejido duro del diente2,6,7.
Los últimos estudios recientes avalan el rol primordial que tiene el azúcar en su desarrollo. Los azúcares proporcionan un sustrato para que las bacterias orales cariogénicas florezcan y generen ácidos desmineralizadores del esmalte8, produciendo una disbiosis de colonias de bacterias azúcar-dependientes9. La extensa bibliografía científica sobre la caries dental muestra que los azúcares libres son un factor dietético necesario en el desarrollo de la caries dental. Actualmente hay un interés científico creciente en la relación entre los factores de riesgo comunes, como la ingesta de azúcares en la dieta, y las enfermedades no transmisibles: diabetes, obesidad o caries. La caries dental se puede prevenir reduciendo la ingesta de azúcares, con el uso apropiado de flúor y la promoción de una buena higiene oral. La mayoría de los factores involucrados en la caries dental son modificables, permitiendo a los individuos y a los profesionales sanitarios y de la salud bucodental tomar las acciones oportunas para prevenir o reducir la gravedad de la enfermedad10.
Antiguamente se consideró el término caries como sinónimo de cavitación, lo cual no es correcto, ya que la cavitación se produce en los estadios finales de la enfermedad. La lesión de "mancha blanca" es el primer indicio clínico del desequilibrio en la superficie del esmalte. La caries es un proceso dinámico, ya que en la superficie del diente se produce un ciclo continuo de desmineralización y remineralización. Si se diagnóstica la caries en estadio inicial, es posible detener o revertir el proceso1,6,7.
Numerosos estudios han encontrado relación entre la prevalencia de caries y la clase social, tanto en países en vías de desarrollo como en los industrializados. Los niños de menor nivel socioeconómico tienen mayor prevalencia y gravedad de caries6,11-14.
La caries es más frecuente en aquellos niños cuyos padres tienen un deterioro de sus dientes y encías6,15. Los cuidados dentales de los niños, particularmente su higiene bucal, tienen que ver fundamentalmente con la educación sanitaria de los padres16,17. La importancia del problema radica en que se sabe que un niño con caries en los dientes primarios será probablemente un adulto con múltiples caries y restauraciones en la dentición permanente2,6,18.
Según informe de la Organización Mundial de la Salud (OMS), el 60-90% de los escolares y casi el 100% de los adultos tienen caries dental en todo el mundo3. Los efectos de las enfermedades bucodentales en términos de dolor, sufrimiento, deterioro funcional y disminución de la calidad de vida son considerables y costosos. La OMS estima que el tratamiento representa entre el 5% y el 10% del gasto sanitario de los países industrializados, y está por encima de los recursos de muchos países en desarrollo. El elevado costo de los tratamientos odontológicos puede evitarse aplicando medidas eficaces de prevención y promoción de la salud2.
Como ocurre con la salud general, existe un constante gradiente social para las enfermedades bucodentales y estas empeoran conforme lo hace el estatus socioeconómico. Este gradiente social es un fenómeno universal a lo largo de toda la vida, desde la infancia hasta la tercera edad, que afecta a casi todas las enfermedades bucodentales en diversos grados, como la caries dental, las enfermedades periodontales y el cáncer oral. En 2008, la OMS puso de relieve las causas subyacentes de las desigualdades hablando de “determinantes sociales”, es decir, las condiciones en las que las personas nacen, crecen, viven, trabajan y envejecen10.
Según los datos de una encuesta de salud oral en España de 2015, en los niños de cinco y seis años la caries afecta más a quienes provienen de niveles sociales bajos (38,3% frente a 15,6% en niveles altos) y a aquellos nacidos fuera de España (un índice de 2 frente a 1,3), con una diferencia también notable en el acceso a tratamientos19.
En un estudio observacional realizado en 130 escolares de edades comprendidas entre 3 y 12 años se observa una prevalencia de los niños con caries del 33%. Hay una relación estadísticamente significativa (p <0,05) entre la caries y la nacionalidad (p = 0,004) y el nivel de estudios de los padres (p = 0,005). También existe una asociación estadísticamente significativa entre la caries y la presencia de placa (p = 0,002), el tiempo de cepillado (p = 0,005), el uso de chupete con azúcar (p = 0,015) y el bruxismo (p = 0,025). Respecto a los hábitos de alimentación, también se observa una relación estadísticamente significativa entre el consumo de chicles (p = 0,006), bollería (p = 0,009), lácteos (p = 0,093) y medicación y la aparición de caries (p = 0,005)20.
La zona básica de salud (ZBS) El Progreso es urbana, situada geográficamente en la margen derecha del río Guadiana a su paso por la ciudad de Badajoz, muy próxima a Portugal. Está delimitada al sur por la vía de ferrocarril, que supone una barrera geográfica y en cierto modo cultural, que la separa del resto de la ciudad de Badajoz. Se trata de una población regresiva, aunque con una estructura aún joven, donde el grueso de su población se halla entre los 20 y los 55 años, con tasas de fecundidad y natalidad superiores al resto de comunidades de referencia. Aproximadamente el 50% de la población carece de estudios o es analfabeta. El nivel socioeconómico de la población es muy bajo, con una tasa de paro muy alta, y la población activa accede a empleos eventuales o precarios, al tratarse de personas poco cualificadas21,22. También hay que señalar que esta ZBS incluye algunas barriadas que constituyen una bolsa poblacional caracterizada por la marginalidad y la exclusión social.
En esta ZBS se han realizado dos análisis de la situación de salud (ASS) cuyos datos fueron publicados en los años 2007 y 2014 respectivamente21,22. Entre los resultados del último ASS de la zona destaca que las algias dentarias eran el segundo motivo de consulta en Urgencias en adultos y que el problema va en aumento en comparación al análisis anterior. En los datos desglosados por grupos de edad, se obtuvo que en la población infantil la falta de higiene y la alimentación inadecuada, ambas íntimamente relacionadas con la caries, se encontraban entre los problemas de salud más relevantes21,22.
Estos resultados, unidos a nuestra impresión subjetiva de que un porcentaje importante de los niños que acuden a la consulta presentan caries, nos llevó a diseñar este estudio para cuantificar el problema. El objetivo es obtener cifras de prevalencia de caries en niños de tres a cinco años, pertenecientes a la ZBS El Progreso.
MATERIAL Y MÉTODOS
Diseño de estudio
Se realiza un estudio descriptivo transversal en el periodo comprendido entre los meses de abril y octubre del año 2017.
Población
El grupo poblacional al que va dirigido el estudio es el formado por los individuos de la ZBS nacidos en los años 2011, 2012 y 2013, los cuales en el momento de la recogida de datos tienen entre tres y cinco años y están cursando los respectivos cursos del ciclo de educación infantil.
Sujetos de estudio
Para facilitar la recogida de datos, se solicita la colaboración de los tres colegios existentes en la ZBS. De esta manera se recogen datos de los alumnos de segundo ciclo de educación infantil (primer, segundo y tercer curso) de los colegios Nuestra Señora de Fátima (NSF), Santa Engracia (SE) y Nuestra Señora de la Asunción (NSA). Los dos primeros son centros públicos, mientras que el último es un colegio concertado.
Quedan excluidos aquellos niños pertenecientes a la unidad básica asistencial (UBA) de Pediatría del centro de salud El Progreso que estén escolarizados fuera de la ZBS, y que por lo tanto no acuden a los colegios que participan en el estudio.
Variables
Las variables estudiadas en este trabajo son:
- Colegio al que asisten los niños estudiados.
- Curso académico.
- Presencia de caries en dientes deciduos.
- Presencia de caries en dientes definitivos.
- Número de caries en dientes deciduos.
- Número de caries en dientes definitivos.
Para el diagnóstico de caries se ha empleado el criterio de la OMS (4.ª edición)23 que considera caries a aquella lesión que presente en una fosa o fisura, o en una superficie dental suave, tiene una cavidad inconfundible, un esmalte socavado o un suelo o pared apreciablemente ablandado. Este criterio es el utilizado en la encuesta de salud bucodental oral.
Los niños de primer y segundo curso de educación infantil (tres y cuatro años) aún no presentan piezas definitivas, por lo que en ellos solo se valora la presencia de caries en dietes deciduos. En los escolares de tercer curso sí cabe la posibilidad de que existan piezas permanentes, por lo que en este grupo sí hemos diferenciado entre caries en dientes temporales y en dientes definitivos.
Procedimientos
El equipo de trabajo se forma por la BA del centro de salud El Progreso (pediatra y enfermera), una enfermera residente de salud comunitaria del mismo centro de salud y la unidad de salud bucodental de zona (USB) del centro de salud San Fernando (dentista, higienista y auxiliar), además de la dentista coordinadora de la oficina del plan dental de los servicios centrales del Servicio Extremeño de Salud (SES) en Mérida (Badajoz, España).
Las fuentes de datos utilizadas son el listado total de los menores escolarizados en los colegios de la zona, proporcionada por las secretarías de los mismos, y el listado de los niños pertenecientes a la UBA de Pediatría del centro de salud El Progreso, adquirida a través del sistema integrado de información sanitaria del SES (JARA). Ambos listados se cruzan para conseguir un único listado en el que los individuos se clasifican según colegio y curso académico al que asisten, y pertenencia o no a la UBA de Pediatría del centro de salud El Progreso.
Una vez conocido el número total de individuos a revisar, y habiendo solicitado el consentimiento por escrito a los tutores legales, se concretan con los colegios las fechas para realizar la revisión bucodental a los niños incluidos en el estudio. Dicha revisión es realizada por el equipo formado por la dentista coordinadora de la Oficina del Plan Dental y la higienista dental de la USB. En ella se busca la existencia de síntomas de mala higiene, problemas de caries o de maloclusión mediante examen visual empleando buena luz natural y equipo no invasivo. Los datos encontrados quedan registrados en una ficha individual que recoge los datos identificativos del alumno (nombre, colegio, curso al que asiste y pertenencia o no al cupo de Pediatría de la ZBS), además de los problemas bucodentales anteriormente mencionados, en caso de existir. La recogida de datos se realiza en los meses de mayo y junio del año 2017.
Análisis estadístico
Los datos recogidos en las fichas individuales se vuelcan en una base de datos elaborada en el programa SPSS Statistics (versión 22.0), donde se realiza el análisis descriptivo de las variables.
RESULTADOS
De un total de 150 niños y niñas escolarizados, 120 acuden a clase el día que se realiza la primera revisión en el colegio, y uno más acude posteriormente a revisión en la consulta de Salud Bucodental. Por lo tanto, obtenemos una muestra de 121 alumnos, que supone el 80,7% del total de la población de estudio.
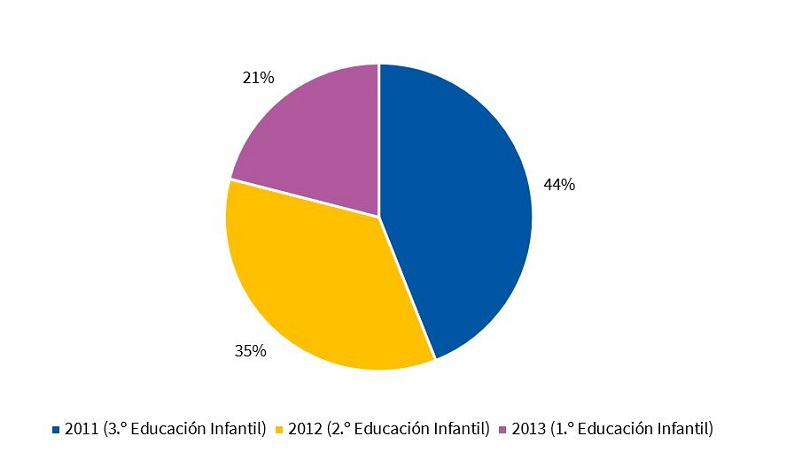
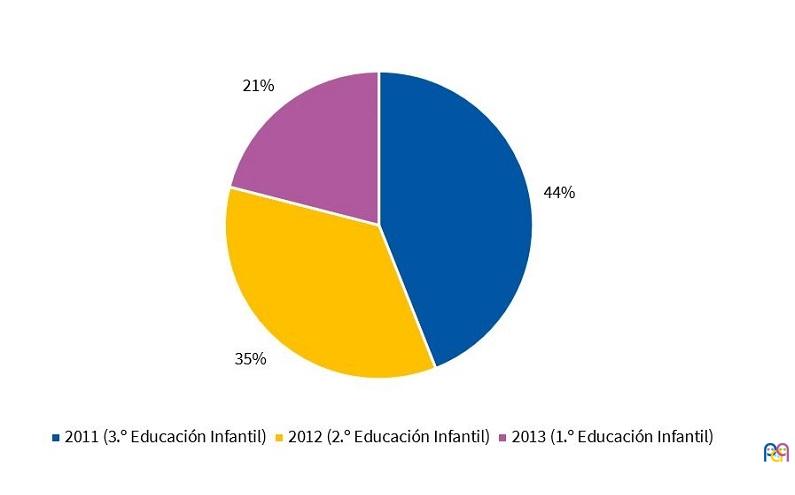
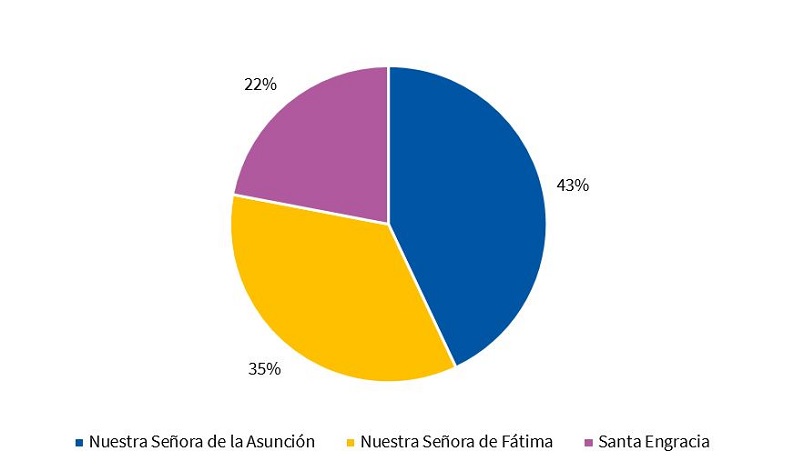
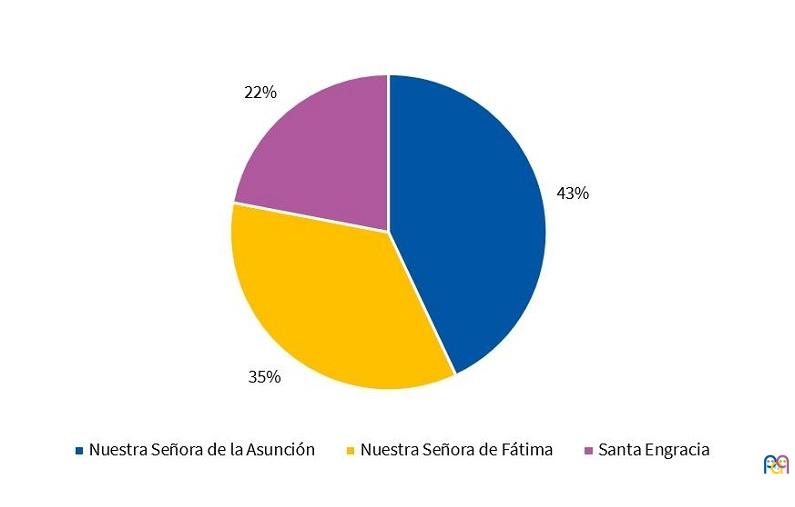
De ellos, el 21,5% están en primer curso de segundo ciclo de educación infantil, el 34,7% en segundo curso y el 43,8% en tercer curso (Fig. 1). En cuanto al colegio de la zona en el que están escolarizados, el 34,7% está en NSF, el 43% en NSA y el 22,3% en SE (Fig. 2).
| Figura 1. Distribución en porcentaje de niños según año de nacimiento |
|---|
 |
| Figura 2. Distribución en porcentaje de niños según el colegio al que asisten |
|---|
 |
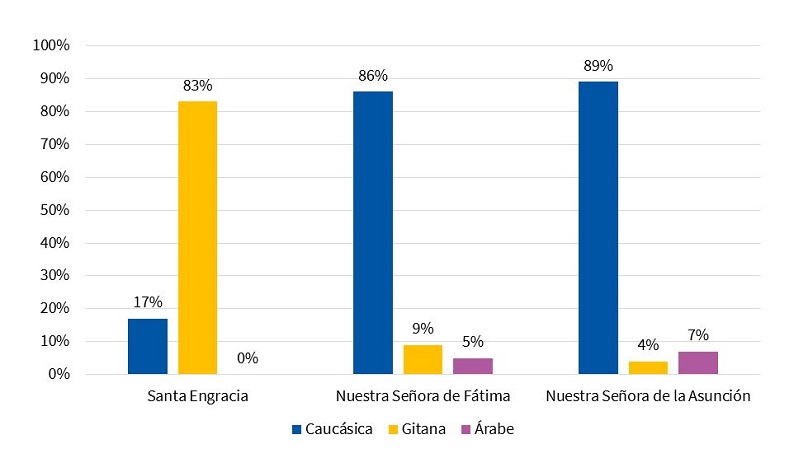
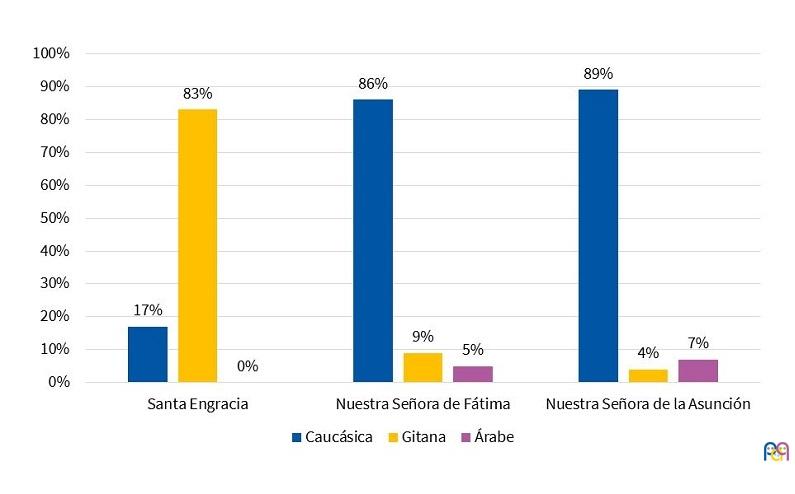
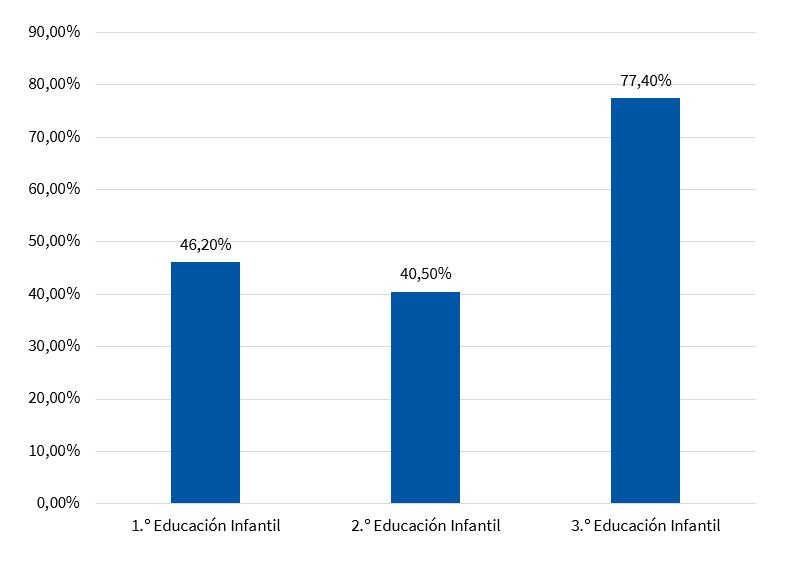
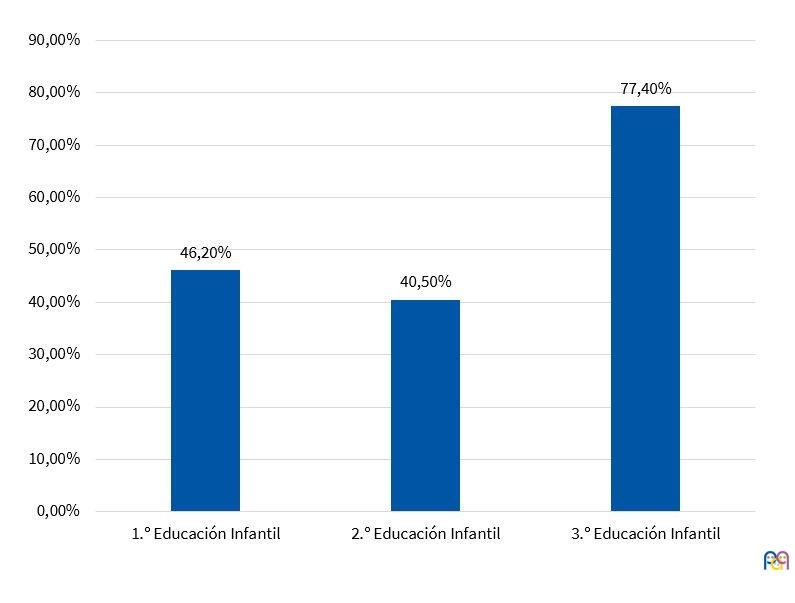
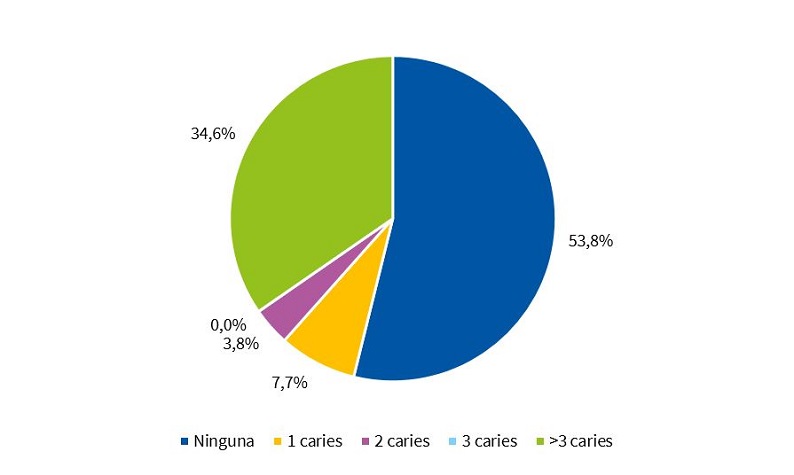
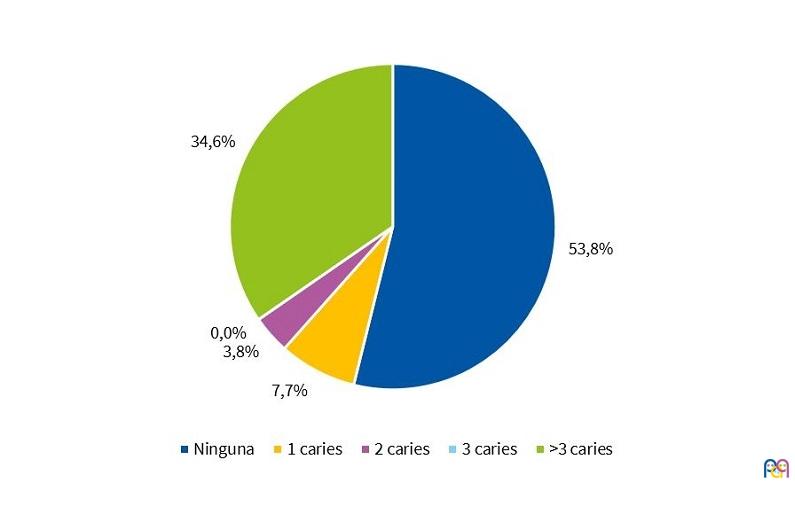
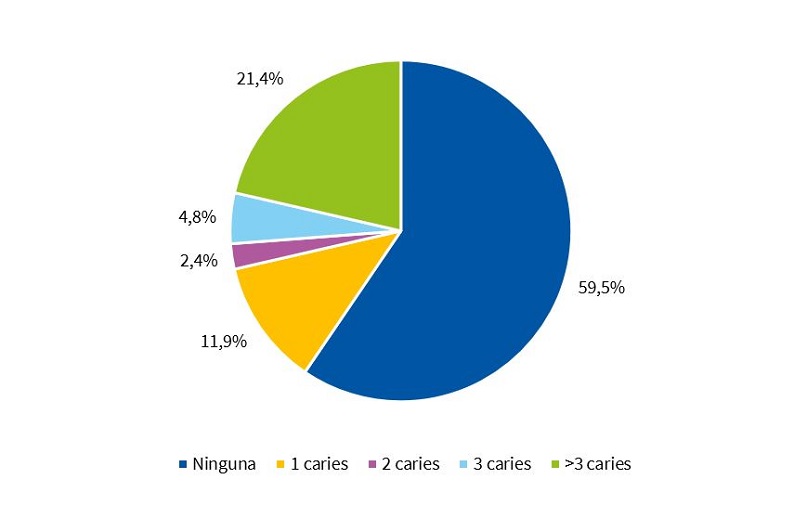
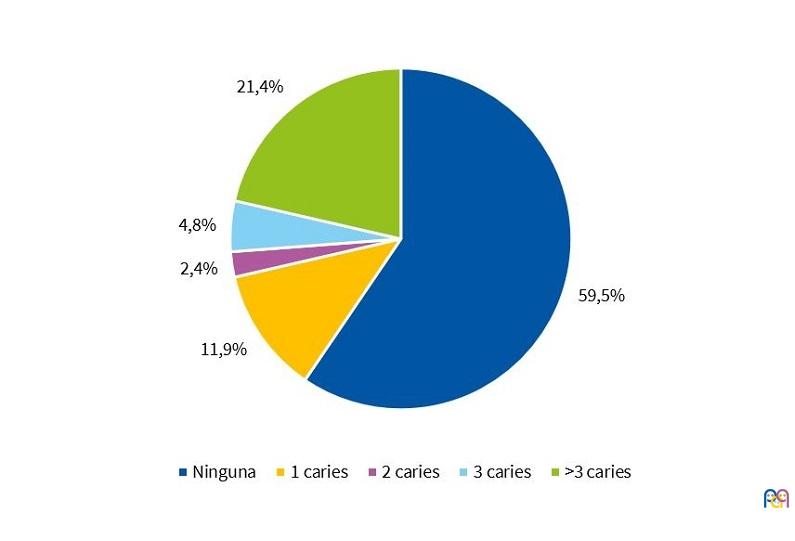
La distribución según etnias en los tres colegios viene reflejada en la Fig. 3. La Fig. 4 refleja el porcentaje de caries en dientes temporales distribuidos según curso. Según curso académico, en el 46,2% de los escolares de primer curso se observan caries, y el 34,6% presenta más de tres (Fig. 5). En los escolares de segundo curso existen caries en el 40,5%, teniendo el 21,4% más de tres (Fig. 6).
| Figura 3. Porcentaje de niños según etnia en cada colegio |
|---|
 |
| Figura 4. Porcentaje de niños con caries en dientes temporales según curso |
|---|
 |
| Figura 5. Niños de 1.º de Educación Infantil según existencia de caries en dientes temporales |
|---|
 |
| Figura 6. Niños de 2.º de Educación Infantil según existencia de caries en dientes temporales |
|---|
 |
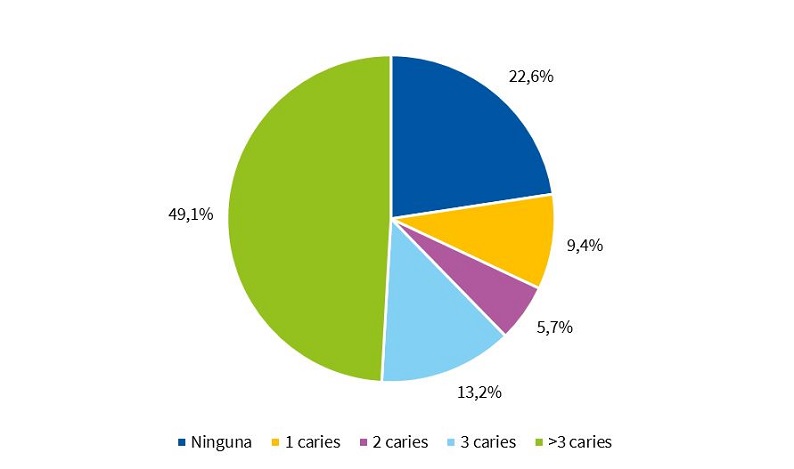
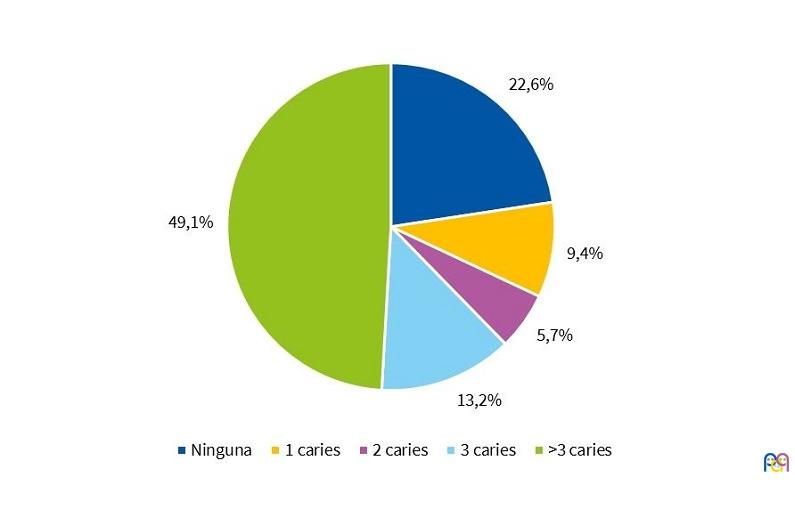
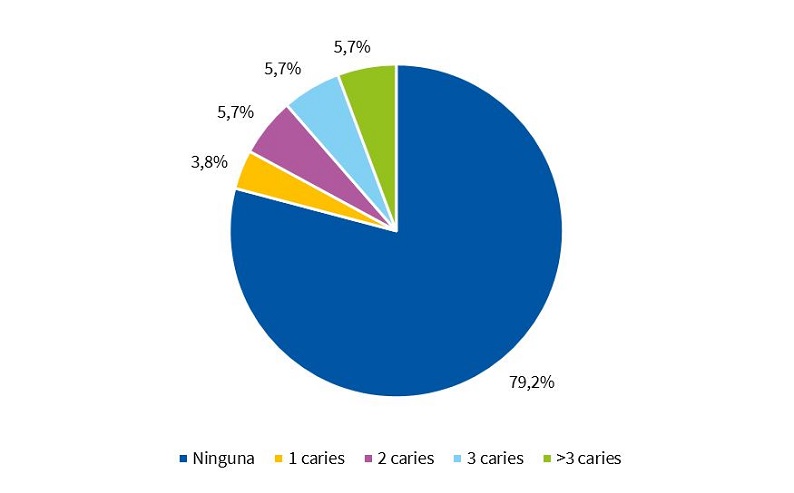
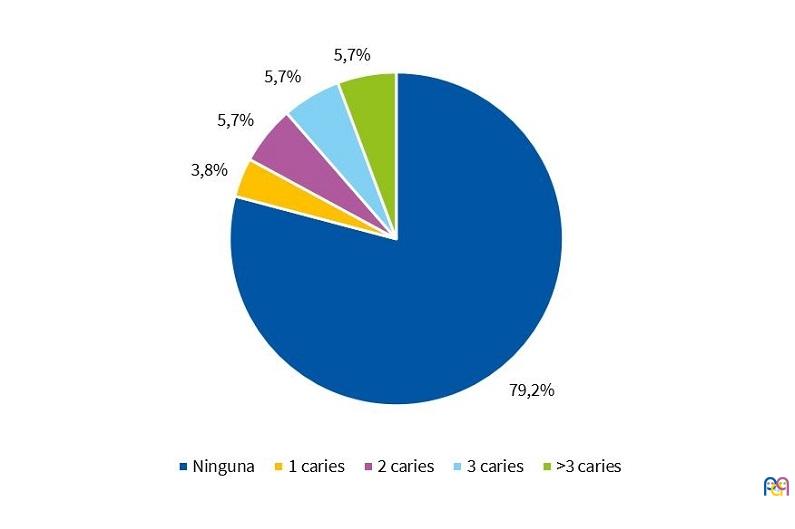
En los niños que cursan tercero de educación infantil sí podemos hacer diferenciación entre dientes deciduos y definitivos. De esta manera, la caries está presente en piezas temporales en el 77,3 % de los niños, teniendo más de tres el 49,1%. En piezas definitivas la caries está presente en el 20,8 % de los niños y tienen más de tres el 5,7% (Figs. 7 y 8).
| Figura 7. Niños de 3.º de Educación Infantil según existencia de caries en dientes temporales |
|---|
 |
| Figura 8. Niños de 3.º de Educación Infantil según existencia de caries en dientes definitivos |
|---|
 |
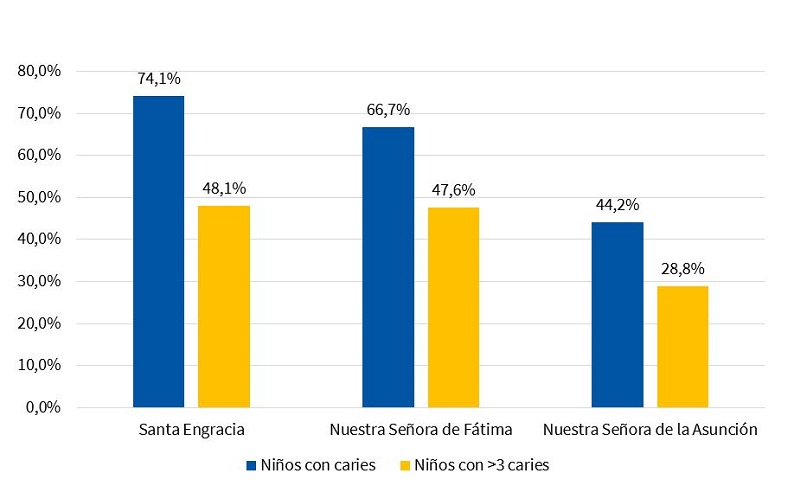
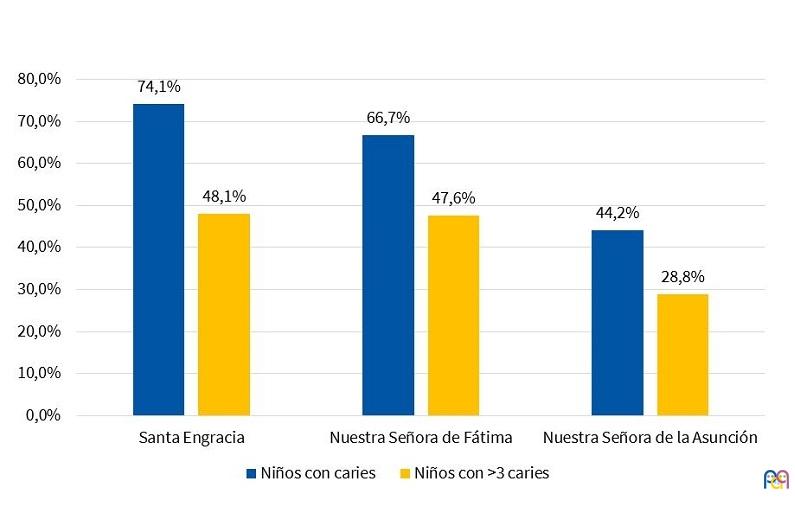
Según el colegio al que asisten, también hemos observado diferencias en las cifras de caries. El 66,7% de los niños estudiados que acuden a NSF presentan caries, teniendo el 47,6% más de tres. En los niños estudiados del colegio NSA se observan caries en el 44,2% y el 28,8% presenta más de tres. En el colegio SE, el 74,1% de los niños estudiados tienen caries, y en el 48,1% se observan más de tres (Fig. 9).
| Figura 9. Porcentajes de niños con caries y con >3 caries por colegio |
|---|
 |
Del total de niños revisados, el 41,3% no presenta ninguna caries dental ni en dientes temporales ni en definitivos.
DISCUSIÓN
La OMS reconoce a la calidad de vida relacionada con la salud bucal como una parte integral de la salud general y el bienestar. Una boca sana y un cuerpo sano van de la mano. Por el contrario, una mala salud bucodental puede tener consecuencias desfavorables en el bienestar físico y psicosocial de la persona2,3.
Los primeros molares son los primeros dientes permanentes en hacer erupción, por ello la OMS toma como indicadores a los primeros molares inferiores permanentes para determinar la prevalencia de caries dental.
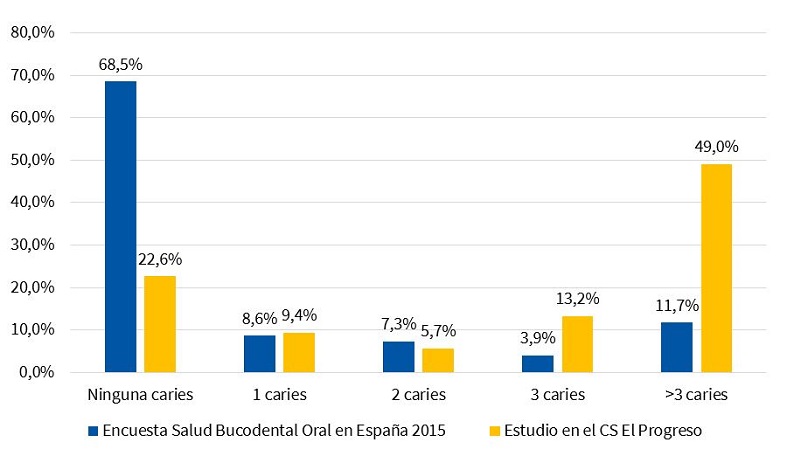
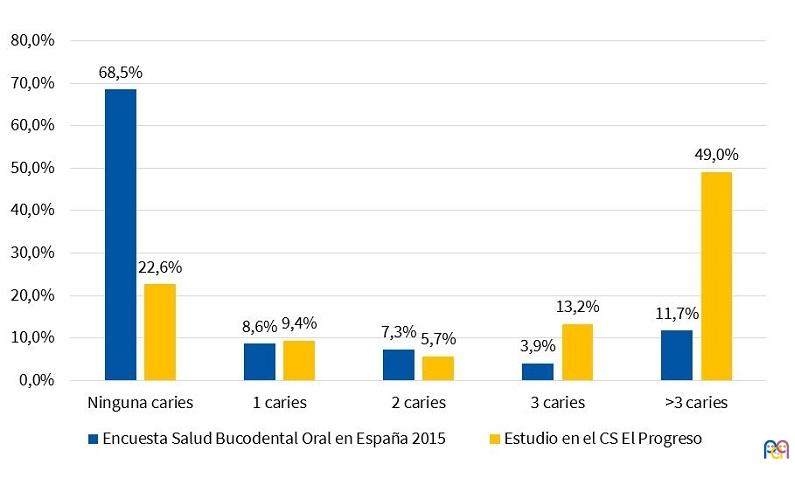
En los resultados de nuestro estudio destacamos una prevalencia de niños con caries muy superior a la referida en la última encuesta de salud oral nacional de 201519, como puede verse en la Fig. 10.
| Figura 10. Porcentaje de caries según la Encuesta de Salud Bucodental en España 2015 y nuestro estudio en el centro de salud El Progreso de Badajoz |
|---|
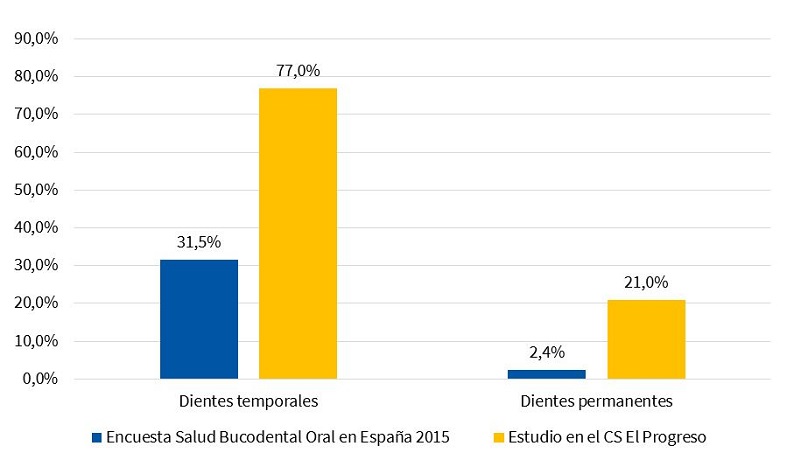 |
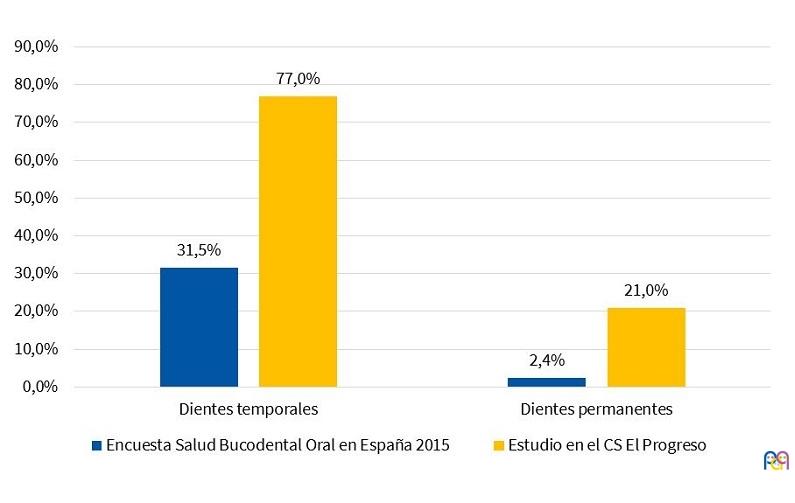
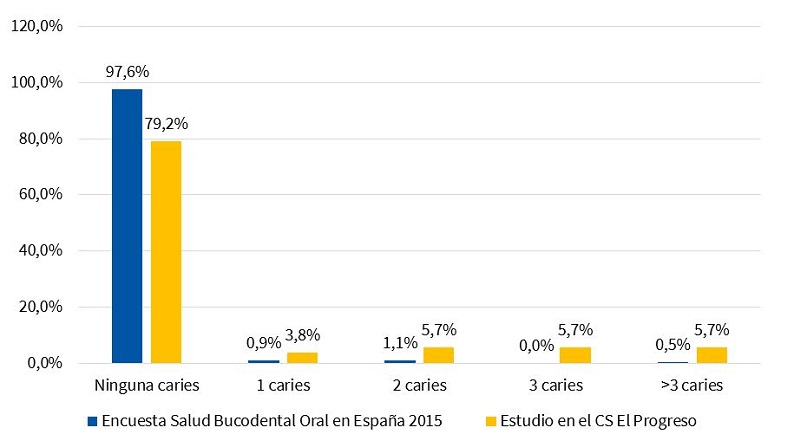
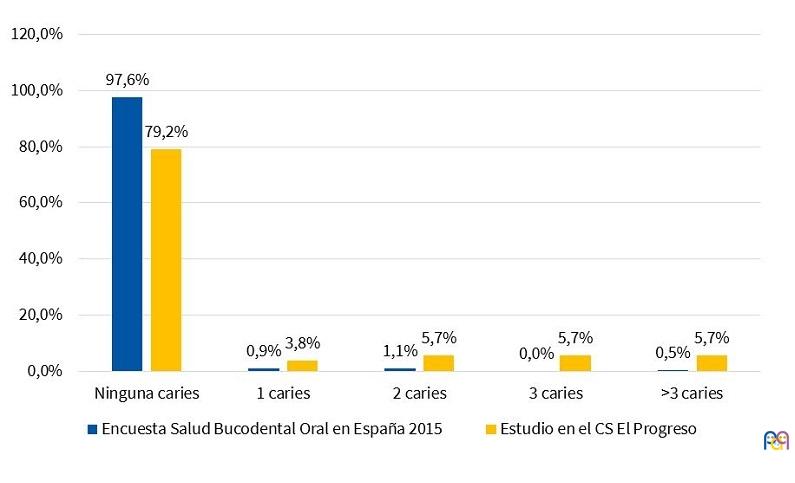
En cuanto a los datos desglosados según las caries afecten a dentición temporal (Fig. 11) o definitiva (Fig. 12), nuestras cifras también destacan por ser muy superiores a las cifras nacionales.
| Figura 11. Porcentaje de n.º caries en la dentición temporal según la Encuesta de Salud Bucodental en España 2015 y nuestro estudio en el centro de salud El Progreso de Badajoz |
|---|
 |
| Figura 12. Porcentaje de n.º caries en la dentición permanente según la Encuesta de Salud Bucodental en España 2015 y nuestro estudio en el centro de salud El Progreso de Badajoz |
|---|
 |
El estudio prospectivo Delphi (periodos 2008-2020) establece unos objetivos de salud oral para el año 2020 respecto a la dentición temporal en población infantil23.
- Al menos el 90% de los niños de tres años libres de caries (53,8% en nuestro estudio en 2017).
- Al menos el 83% de los niños de cuatro años libres de caries (59,5% en nuestro estudio en 2017).
- Al menos el 75% de los niños de cinco y seis años libres de caries (22,6% en nuestro estudio en 2017).
Según los datos de nuestro estudio, estamos muy lejos de conseguir este objetivo.
Nuestros resultados concuerdan con la mayoría de las publicaciones revisadas que revelen una relación de la caries con nivel social, económico y educativo bajo, tanto en países industrializados como en países en vías de desarrollo6,10-13. Para afirmar que nuestra población cumple estas características de nivel socioeducativo bajo, nos basamos en los resultados del ya mencionado “Análisis de Situación de Salud”21, que revela que se trata de una población de nivel cultural bajo, con unas altas tasas de absentismo y abandono escolar. Esto genera una población poco cualificada, con acceso a empleos precarios, alta tasa de desempleo y muy dependiente de ayudas sociales. Uno de sus principales problemas es la dificultad económica para atender las necesidades básicas. Además, destacamos que, en nuestra zona, hay un sector de la población en riesgo de exclusión social, marginalidad, etnia mayoritariamente gitana y consumo de drogas asociados, en especial centrada en el barrio donde se sitúa el colegio de Santa Engracia, que es donde se han detectado las cifras de caries más alarmantes (74,1%).
Destacamos el estudio realizado en comunidades rurales de países africanos que muestra un incremento en la incidencia de caries en niños pertenecientes a clases altas con poder adquisitivo debido a que eran los que tenían la posibilidad de consumo de golosinas a base de glucosa y sacarosa24. Esto no es nuevo, ya sucedió en el siglo pasado. En poblaciones que habían padecido la Segunda Guerra Mundial, en las que faltaban alimentos, el bajo o nulo consumo de azúcares hizo disminuir la incidencia de caries de forma drástica. El informe de la OMS alerta también de este potencial problema futuro, de que con el cambio en las condiciones de vida es probable que la caries dental aumente en muchos países en desarrollo de África, sobre todo debido al creciente consumo de azúcares y a una exposición insuficiente al flúor2.
Existen profundas disparidades en la salud bucodental en las regiones, los países y dentro de los países. Estas pueden estar relacionadas a la situación socioeconómica, raza u origen étnico, edad, sexo o estado general de la salud. Si bien las enfermedades dentales comunes son prevenibles, no todos los miembros de la comunidad están informados o están en condiciones de beneficiarse de las medidas de promoción de la salud bucodental adecuadas, como refleja la Carta de Otawa25. La reducción de las disparidades requiere de enfoques amplios, de gran alcance, dirigidos a las poblaciones en mayor riesgo de enfermedades bucodentales específicas e implica mejorar el acceso a los servicios existentes25.
Los protocolos de prevención de la caries de las sociedades odontológicas aconsejan la primera visita del niño al odontopediatra al cumplir el primer año. En ese momento se debe evaluar de manera individual el riesgo de caries y para ello el odontopediatra puede ayudarse de varias herramientas que permiten establecer el riesgo de caries de cada individuo. Uno de los más usados es el cuestionario Caries Management by Risk Assessment (CAMBRA), que sirve para evaluar el riesgo mediante un cuestionario para el grupo de niños de hasta cinco años de edad y otro para los niños a partir de seis años5.
Trabajar con las familias para que adquieran el hábito de higiene oral diaria desde el periodo de lactante es un factor clave para la prevención de la caries5,8,26,27. Es nuestra responsabilidad como profesionales sanitarios hacer que los padres y cuidadores sean conscientes de su importancia. Muchos padres desconocen que alimentos y bebidas nutritivas tales como leche de fórmula y jugos de fruta contienen azúcares que contribuyen al proceso de la caries, al igual que la lactancia materna a demanda y nocturna cuando ya han erupcionado los dientes. Debemos informar a los padres que desde la erupción del primer diente se debe comenzar con la higiene oral, cepillando con la cantidad de un grano de arroz de pasta fluorada (1000 ppm) al menos dos veces al día y siempre antes de dormir. Para ello se puede utilizar un cepillo dental adecuado o un dedal de silicona, con el que limpiarán las encías y los nuevos dientes, tanto en el maxilar superior como en el inferior, sin aclararlo después. Este grano de arroz pasará a ser como una lenteja con tres años y como un guisante con cinco años, ampliando entonces la dosis de flúor hasta 1450 ppm8. Debemos transmitir a padres y cuidadores que el cuidado de la boca de sus hijos es su responsabilidad hasta que el niño adquiera la habilidad motora suficiente para hacerlo por sí solo, lo cual no suele ocurrir antes de los siete u ocho años. A partir de ese momento y hasta la adolescencia, los expertos recomiendan que un adulto siga supervisando al menos el cepillado nocturno.
La higiene oral desde el primer año sirve tanto para establecer buenos hábitos como para proteger los dientes temporales. Todos nacemos con las bacterias que causan la caries, pero no con la enfermedad; adquirimos de nuestros educadores los buenos o los malos hábitos tanto de higiene como alimenticios y de ello dependerá nuestra salud y la de nuestra boca8. Debemos explicar que no son buenas prácticas compartir utensilios con el bebé (cepillos dentales, cucharas, juguetes, etc.), especialmente durante los primeros dos años de vida, limpiar el chupete con saliva, enfriar la comida soplando directamente sobre la cuchara de comida del bebé ni permitir que se le den besos en la boca o que las mascotas le laman la cara.
La buena higiene oral, la reducción en el consumo de azúcares de la dieta y un uso regular y adecuado del flúor son elementos clave para la prevención de la caries. Los sustitutos del azúcar como el sorbitol y el xilitol se caracterizan por tener un potencial cariogénico nulo, mientras que los edulcorantes artificiales como el ciclamato o el aspartamo no son cariógenos.
Los programas de asistencia dental comenzaron a funcionar en España en País Vasco y Navarra en el año 19904. En Extremadura, el programa de salud bucodental infantil PADIEX28 se implantó mucho más tarde, en el año 2005, y los niños permanecen en él desde el año que cumplen seis años hasta el año que cumplen 15. Incluye revisión al menos una vez al año y comprende el análisis del estado dental y de índices de caries, la valoración de hábitos inadecuados e información sobre medidas higiénicas, entre otras actuaciones. Se realizan además aplicaciones de flúor tópico, tratamientos de sellado de fosas o fisuras profundas y tartrectomías (limpiezas de boca). Al igual que ha ocurrido en otras comunidades autónomas (CC. AA.), este programa de atención a la salud bucodental infantil se ha demostrado eficaz para reducir la caries en mayores de seis años, pero resulta insuficiente, al no incluir tratamientos en menores de esta edad ni en dentición temporal. Con la intención de paliar este problema, en Extremadura, desde el año 2018, al igual que ya lo está disponible en otras CC. AA., se ha implantado un nuevo plan dental dirigido a menores de seis años29, centrado únicamente en actividades preventivas y adquisición de buenos hábitos, del que aún no podemos evaluar resultados por el corto tiempo que lleva en marcha.
La caries no es un motivo de consulta frecuente en la consulta de Pediatría de Atención Primaria, pero los casos que acuden son porque provocan síntomas y están en un estadio avanzado.
Como aspecto positivo a la hora de pensar cómo diseñar estrategias para abordar el problema, según resultados del ASS, nuestra población es consciente de que la alimentación inadecuada y la higiene, ambos íntimamente relacionados con la caries, son problemas importantes en sus niños. Pensamos que diseñar actividades preventivas trabajando estos aspectos deben centrar parte de nuestro esfuerzo.
Tras las revisiones en los colegios, se mandó el resultado a los padres junto a una cita en el centro de salud para informarles, realizar tratamientos preventivos y planificar un seguimiento con periodicidad variable según la situación de riesgo individual. La evaluación de este seguimiento consideramos puede ser objetivo de un estudio posterior.
Limitaciones del estudio
Una de las dificultades que nos encontramos al tratar de abordar a una población de estas características es la falta a las consultas programadas y a los tratamientos pautados. Por este motivo se decidió organizar las revisiones en los colegios previa información y petición de consentimiento a los padres, para captar al mayor número posible de niños. Aun así, al tratarse de un estudio en niños de educación infantil, etapa en que la escolarización no es obligatoria, y en una zona de alto absentismo escolar, solo pudimos captar a 121 de los 150 niños matriculados. Sospechamos que en esos niños de población marginal que no hemos conseguido captar, las cifras pudieran ser incluso peores.
CONCLUSIÓN
La caries en la infancia no es solo un problema del niño y su familia, sino también de la sociedad y del sistema sanitario. Los pediatras jugamos un papel importante, tanto para su detección en estadio precoz como para su prevención con la adecuada información a las familias. El niño con caries en los dientes de leche será probablemente un adulto con caries en la dentición definitiva, cuando no sea tratado en la primera fase en que la mancha blanca o incipiente se puede controlar2,5,8,18, y si no es así, necesitará probablemente tratamientos restauradores o irá perdiendo sus dientes de forma prematura.
Queremos alertar de las alarmantes cifras de caries en niños de tres a seis años en nuestra ZBS, muy superiores a lo referido en la encuesta de salud oral nacional de 2015 y muy lejos de cumplir los objetivos del estudio Delphi.
Debemos centrar nuestros esfuerzos en la prevención de la caries desde edades tempranas más que en el tratamiento de esta, insistiendo en el uso de las USB para su primera revisión con el primer cumpleaños8,28. Esos esfuerzos deben ser aún mayores en zonas socioeconómicamente deprimidas7 y con escasos o sin recursos odontológicos, como es el caso de la nuestra.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
ASS: análisis de la situación de salud · CC. AA.: comunidades autónomas · NSA: Nuestra Señora de la Asunción · NSF: Nuestra Señora de Fátima · OMS: Organización Mundial de la Salud · SE: Santa Engracia · SES: Servicio Extremeño de Salud · UBA: unidad básica asistencial · USB: unidad de salud bucodental · ZBS: zona básica de salud.
BIBLIOGRAFÍA
- Cerón Bastidas XA. El sistema ICDAS como método complementario para el diagnóstico de caries dental. CES Odont. 2015;28:100-9.
- Informe sobre el problema mundial de las enfermedades bucodentales. En: Organización Mundial de la Salud [en línea] [consultado el 10/06/2019]. Disponible en www.who.int/mediacentre/news/re leases/2004/pr15/es/
- Salud bucodental. Nota informativa n.º 318. Abril de 2012. En: Organización Mundial de la Salud [en línea] [consultado el 10/06/2019]. Disponible en www.who.int/mediacentre/factsheets/fs318/es
- Crovetto Martínez R, Ortuzar Otxoa L, Martínez Rodríguez A, Fernández Alonso J, Escobar-Martínez A. Valoración del riesgo de caries infantil en un servicio hospitalario de urgencias. Enferm Glob. 2016;15:1-9.
- Casals Peidró E, García Pereiro MA. Guía de práctica clínica para la prevención y tratamiento no invasivo de la caries dental. RCOE. 2014;19:189-248.
- Hernández Juyol M. Diagnóstico, pronóstico y prevención de la caries de la primera infancia. En: Protocolo de la Sociedad Española de Odontopediatría [en línea] [consultado el 10/06/2019]. Disponible en www.odontologiapediatrica.com/wp-content/uploads/2018/06/SEOP_-_Caries_precoz_de_la_infancia_fin4.pdf
- González Sanz AM, González Nieto BA, González Nieto E. Salud dental: relación entre la caries dental y el consumo de alimentos. Nutr Hosp. 2013;28:64-71.
- Sheimham A. James WPT. Diet and dental caries: the pivotal role of free sugars reemphasized. J Dent Research. 2015;94:1341-7.
- Simón-Soro A, Mira A. Solving the etiology of dental caries. Trends Microbiol. 2015;23:76-82.
- Fukai K, Ogawa H, Hescot P. Oral health for healthy longevity in an ageing society: maintaining momentum and moving forward. Int Dental J. 2017;67:3-6.
- Mora León L, Martínez Olmos J. Prevalencia de caries y factores asociados en niños de 2-5 años de los Centros de Salud Almanjáyar y Cartuja de Granada capital. Aten Primaria 2000;26:398-404.
- Watanabe MK, Hostetler JT, Patel YM, Vergel de Dios JM, Bernardo MA, Foley ME. The impact of risk-based care on early childhood and youth populations. J Calif Dent Assoc. 2016;44:367-77.
- Medina Solis CE, Maupomé G, Pelcastre Villafuerte B, Ávila Burgos L, Vallejos Sánchez AA, Casanova Rosado AJ. Desigualdades socioeconómicas en salud bucal. Rev Invest Clin. 2006;58:296-304.
- Apaza Ramos S, Torres Ramos G, Blanco Victorio D, Antezana Vargas V, Montoya Funegra J. Influencia de los factores sociodemográficos, familiares y el estado de la salud bucal en la calidad de vida de adolescentes peruanos. Rev Estomatol Herediana. 2015;25:87-99.
- Herschfeld JJ. W. D. Miller and the “chemico-parasitic” theory of dental caries. Bull Hist Dent. 1978;26:11-20.
- Marrs JA, Trumbley S, Malik G. Early childhood caries: determining the risk factors and assessing the prevention strategies for nursing intervention. Pediatr Nurs. 2011;37:9-16.
- González Sanz A, González Nieto B, González Nieto E. Nutrición, dieta y salud oral. En: Castaño A, Ribas B. Odontología preventiva y comunitaria. La odontología social, un deber, una necesidad, un reto. Sevilla: Fundación Odontología Social; 2012. p. 155-69.
- Espasa E, Boj JR, Hernández M. Caries dental en el niño. En: Boj JR, Catalá M, García-Ballesta C, Mendoza A, Planells P. Odontopediatría. La evolución del niño al adulto joven. Madrid: Ripano; 2011. p. 213-23.
- Bravo Pérez M, Almerich Silla JM, Ausina Márquez V, Avilés Gutiérrez P, Blanco González JM, Canorea Díaz E, et al. Encuesta de Salud Oral en España 2015. RCOE. 2016;21:8-48.
- Alcaina Lorente A, Cortés Lillo O, Galera Sánchez MD, Guzmán Pina S, Canteras Jordana Caries dental: influencia de los hábitos de higiene bucodental y de alimentación en niños en edad escolar. Acta Pediatr Esp. 2016;74:246-52.
- Equipo de Atención Primaria. Análisis de la Situación de Salud de la Zona de Salud El Progreso. Centro de Salud El Progreso. Badajoz: Edita SES; 2014.
- Maynar Mariño I, Nieto Ramírez R, Montero de Espinosa Pérez P, Madueño García MA, Fernández López MD, Maynar Mariño MA. Proyecto Progreso: un sistema sanitario participado para el desarrollo integral del modelo de Atención Primaria de Salud. Comunidad. 2010;12:12-7.
- Llodra Calvo JC, Denis Bourgeois D. Estudio prospectivo Delphi. La salud bucodental en España 2020. Tendencias y objetivos de salud oral. En: Fundación Dental Española [en línea] [consultado el 10/06/2019]. Disponible en www.consejodentistas.es
- Enwonwu C. Review of oral disease in Africa and the influence of socio-economic factors. Oral Dent Africa. 1981;31:1-5.
- Carta de Otawa para el Fomento de la Salud. Primera Conferencia Internacional sobre la Promoción de la Salud, Otawa. Ginebra: Organización Mundial de la Salud; 1986.
- Wagner Y, Greiner S, Heinrich-Weltzien R. Evaluation of an oral health promotion program at the time of birth on dental caries in 5-year-old children in Vorarlberg, Austria. Community Den Oral Epidemiol. 2014;42:160-9.
- Plutzer K, Spencer AJ. Efficacy of an oral health promotion intervention in the prevention of early childhood caries. Community Dent Oral Epidemiol. 2008;36:335-46.
- Decreto 195/2004, de 29 de diciembre, sobre asistencia dental a la población infantil de la Comunidad Autónoma de Extremadura. En: Diario oficial de Extremadura (DOE) [en línea] [consultado el 10/06/2019]. Disponible en http://doe.juntaex.es/pdfs/doe/2005/20o/04040210.pdf
- Periódico del Servicio Extremeño de Salud [en línea] [consultado el 10/06/2019]. Disponible en https://digitalextremadura.com/marcha-plan-atencion-dental-ninos-menores-6-anos/