
Vol. 20 - Num. 79
Originales
Vivencias sobre la maternidad: aspectos que tener en cuenta en la promoción de la salud infantil
Elena López de Arana Pradoa, Alexander Barandiaran Arteagab
aFacultad de Educación y Deporte. Universidad del País Vasco. Vitoria-Gasteiz. España.
bFacultad de Humanidades y Ciencias de la Educación. Universidad de Mondragon. Escoriaza. San Sebastián.
Correspondencia: E López de Arana. Correo electrónico: elena.lopezdearana@ehu.eus
Cómo citar este artículo: López de Arana Prado E, Barandiaran Arteaga A. Vivencias sobre la maternidad: aspectos que tener en cuenta en la promoción de la salud infantil. Rev Pediatr Aten Primaria. 2018;20:237-43.
Publicado en Internet: 25-07-2018 - Número de visitas: 21022
Resumen
Introducción: en las consultas de Pediatría de Atención Primaria, una de las principales reivindicaciones de las madres es la necesidad de sentirse comprendidas en el afrontamiento de su nuevo rol. Objetivo: el presente estudio trata de conocer las vivencias que un grupo de mujeres relatan sobre la maternidad para identificar los aspectos que tener en cuenta en la promoción de la salud infantil.
Material y métodos: estudio cualitativo con enfoque fenomenológico. Siete madres configuran la muestra. Los grupos de discusión fueron grabados y transcritos para realizar el análisis de contenido. Este se llevó a cabo de forma colaborativa siguiendo los cánones de la codificación abierta hasta la saturación teórica.
Resultados: las vivencias más relevantes se organizan en tres categorías. En cuanto a la relación con sus hijos, subrayan que dicha relación les reporta “felicidad”, aunque señalan el “trabajo” como un obstáculo importante para ello. En referencia a ellas mismas se describen en “alarma constante”, “preocupadas”, con “miedo” frente a la crianza, y con la necesidad de tener “tiempo para ellas”. Respecto al apoyo social, aseguran que, aunque sus parejas se “implican”, suelen “sentirse mal” por comentarios de sus madres, y “presionadas” por los pediatras.
Conclusiones: la formación, si otorga importancia a la comunicación, puede hacer emerger en las consultas de Pediatría de Atención Primaria, relaciones que facilitan la reflexión de las madres sobre la crianza, y que no culpabilizan para asegurar así la adhesión a las recomendaciones pediátricas y la promoción de la salud infantil.
Palabras clave
● Atención Primaria de Salud ● Responsabilidad parental ● Salud del niñoINTRODUCCIÓN
La Pediatría de Atención Primaria (PAP) ha estado siempre íntimamente relacionada con ofrecer respuesta a las necesidades, que, sobre la salud, han padecido los niños. Sin embargo, esta función ha ido evolucionando y complejizándose1. Por un lado, la preparación de médicos internos residentes (MIR) ha supuesto una mayor cualificación de los profesionales de esta área, permitiéndoles la atención, en este primer nivel, de patologías que anteriormente eran tratadas únicamente en el ámbito hospitalario. Por otro lado, a consecuencia de los programas de salud desarrollados, como por ejemplo las vacunas, se ha logrado la desaparición y erradicación de algunas de las enfermedades que antes copaban las consultas. Asimismo, los programas orientados a la educación maternal o a la salud escolar han supuesto un importante descenso de la mortalidad por accidentes infantiles.
Ante esta realidad, cabe reconocer que las prioridades de salud infantil han sufrido un cambio cualitativo1 y, con ellas, la conceptualización de los pediatras sobre su labor, ya que la reconocen dentro del marco de promoción de la salud2,3. Por tanto, se asume que, actualmente, los pediatras son la principal fuente técnica de apoyo para las familias sobre el desarrollo y la educación de sus hijos4,5.
Para el acompañamiento a las familias en su quehacer educativo, es necesario que los pediatras traten de entender los afectos de las madres6 ante los nuevos retos que emergen de la maternidad. No obstante, una de las principales reivindicaciones expresadas por las mujeres sobre la PAP es la necesidad de sentirse apoyadas o acompañadas en el afrontamiento de su nuevo rol7-9.
Ante dicho reto, es clave tener consciencia de lo que la maternidad implica, reconociendo la transformación vital que supone, al producirse en las mujeres cambios biopsicosociales significativos10,11. La madre nace psicológicamente al igual que su bebé nace físicamente, emergiendo una nueva identidad que estará en continua evolución12. Esto se refleja en los cambios que, durante su maternidad, afirman experimentar las mujeres en cuanto a sus prioridades, valores, y actitudes12-14.
Además, parece que la relación médico-paciente puede vivirse como un apoyo para la transición hacia la maternidad15, si esta se basa en una comunicación orientada a facilitar la expresión de dudas y preocupaciones16. La creación de este nuevo contexto interactivo favorece tanto la mejora del vínculo afectivo madre-hijo17,18 como la comprensión y adhesión a las recomendaciones de los profesionales16.
Atendiendo al desafío planteado por las mujeres que acuden a las consultas de PAP, este estudio trata de acercarse al conocimiento de las vivencias, que un grupo de mujeres relatan sobre la maternidad, con el fin de identificar los aspectos que tener en cuenta en la promoción de la salud infantil. Aunque existen estudios orientados a la comprensión de las experiencias relacionadas con la maternidad13,15, más que de grupos de discusión en los que participan madres no pertenecientes a grupos vulnerables, dichos trabajos parten de intervenciones grupales dirigidas a mujeres pertenecientes a grupos de riesgo. Por tanto, quedaría pendiente indagar sobre las vivencias de madres no pertenecientes a grupos vulnerables13 y poder clarificar así posibles líneas de actuación para la PAP.
MATERIAL Y MÉTODO
Diseño
El diseño fenomenológico de la investigación permite acercarnos a las experiencias individuales subjetivas de las participantes19, esto es, a las percepciones y al significado que la experiencia20 de la maternidad tiene para las mujeres que acudieron al grupo de discusión.
Muestra y participantes
En colaboración con el Servicio de Juventud y Educación del Ayuntamiento de Escoriaza (Guipúzcoa), desde la Facultad de Humanidades Ciencias de la Educación de la Universidad de Mondragón se propuso a las familias residentes en dicha localidad con hijas o hijos de edades comprendidas entre 0 y 3 años la posibilidad de reunirse para compartir experiencias sobre la maternidad.
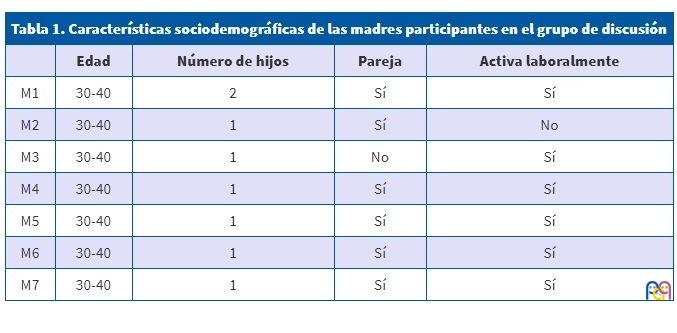
Todas las personas que se ofrecieron a participar, un total de siete madres cuyas características se recogen en la Tabla 1, fueron incluidas, ya que cumplían las características necesarias para el desarrollo del estudio. Por tanto, se puede decir que se trata de un muestreo opinático21, ya que estuvo sujeto más bien al tema objeto de estudio y accesibilidad de las personas contactadas.
| Tabla 1. Características sociodemográficas de las madres participantes en el grupo de discusión | ||||
|---|---|---|---|---|
| Edad | Número de hijos | Pareja | Activa laboralmente | |
| M1 | 30-40 | 2 | Sí | Sí |
| M2 | 30-40 | 1 | Sí | No |
| M3 | 30-40 | 1 | No | Sí |
| M4 | 30-40 | 1 | Sí | Sí |
| M5 | 30-40 | 1 | Sí | Sí |
| M6 | 30-40 | 1 | Sí | Sí |
| M7 | 30-40 | 1 | Sí | Sí |
Recolección y análisis de datos
En el museo de Escoriaza se habilitó un espacio donde se organizaron cinco reuniones mensuales bajo el formato de grupo de discusión22,23. La duración de dichos encuentros fue de dos horas.
Las personas encargadas de moderar el grupo de discusión fueron los autores del artículo, que optaron por la técnica del embudo24. Dicha técnica se caracteriza por la necesidad de generar un ambiente agradable –según Morgan25, recíproco e interactivo– y centrar la conversación sobre el tema, la maternidad en este caso, facilitando avanzar de aspectos más generales hacia aspectos más específicos.
Tras obtener las autorizaciones necesarias y el consentimiento informado de las madres, se grabaron las reuniones magnetofónicamente, y fueron transcritas, para poder realizar posteriormente el tratamiento de los datos a través del análisis de contenido26. La unidad de análisis fue la frase. Tras leer y analizar los textos de forma individual, los autores construyeron un sistema de categorías y códigos de forma colaborativa, siguiendo los cánones de la codificación abierta, que prescinde de una teoría desde la que aplicar conceptos, leyes o dimensiones al discurso objeto de análisis27, dejando emerger así las categorías y los códigos de forma inductiva hasta la saturación teórica28.
RESULTADOS
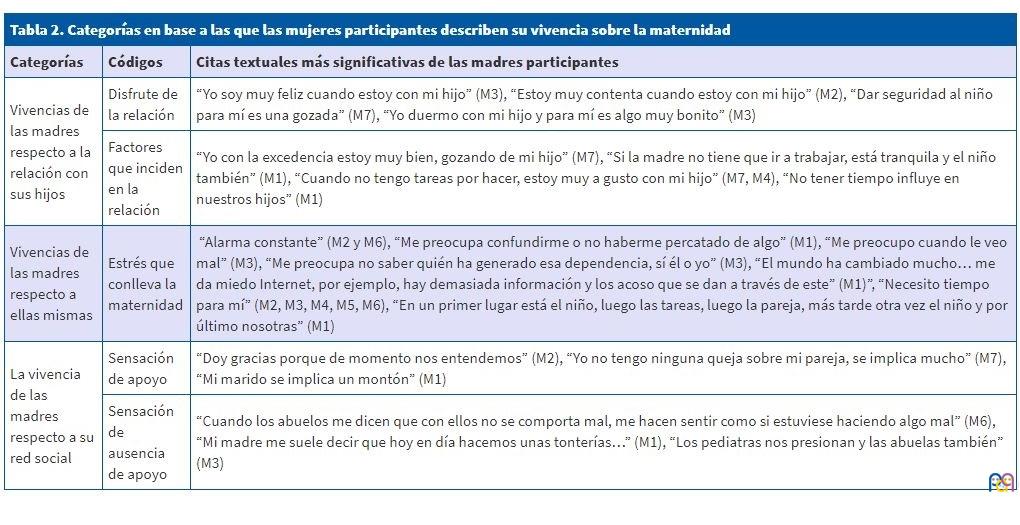
Tres son las categorías en base a las que las mujeres participantes describen su vivencia sobre la maternidad. Dichas categorías se recogen con detalle en la Tabla 2, junto con algunas de las citas textuales más significativas.
| Tabla 2. Categorías en base a las que las mujeres participantes describen su vivencia sobre la maternidad | ||
|---|---|---|
| Categorías | Códigos | Citas textuales más significativas de las madres participantes |
| Vivencias de las madres respecto a la relación con sus hijos | Disfrute de la relación | “Yo soy muy feliz cuando estoy con mi hijo” (M3), “Estoy muy contenta cuando estoy con mi hijo” (M2), “Dar seguridad al niño para mí es una gozada” (M7), “Yo duermo con mi hijo y para mí es algo muy bonito” (M3) |
| Factores que inciden en la relación | “Yo con la excedencia estoy muy bien, gozando de mi hijo” (M7), “Si la madre no tiene que ir a trabajar, está tranquila y el niño también” (M1), “Cuando no tengo tareas por hacer, estoy muy a gusto con mi hijo” (M7, M4), “No tener tiempo influye en nuestros hijos” (M1) | |
| Vivencias de las madres respecto a ellas mismas | Estrés que conlleva la maternidad | “Alarma constante” (M2 y M6), “Me preocupa confundirme o no haberme percatado de algo” (M1), “Me preocupo cuando le veo mal” (M3), “Me preocupa no saber quién ha generado esa dependencia, sí él o yo” (M3), “El mundo ha cambiado mucho… me da miedo Internet, por ejemplo, hay demasiada información y los acoso que se dan a través de este” (M1)”, “Necesito tiempo para mí” (M2, M3, M4, M5, M6), “En un primer lugar está el niño, luego las tareas, luego la pareja, más tarde otra vez el niño y por último nosotras” (M1) |
| La vivencia de las madres respecto a su red social | Sensación de apoyo | “Doy gracias porque de momento nos entendemos” (M2), “Yo no tengo ninguna queja sobre mi pareja, se implica mucho” (M7), “Mi marido se implica un montón” (M1) |
| Sensación de ausencia de apoyo | “Cuando los abuelos me dicen que con ellos no se comporta mal, me hacen sentir como si estuviese haciendo algo mal” (M6), “Mi madre me suele decir que hoy en día hacemos unas tonterías…” (M1), “Los pediatras nos presionan y las abuelas también” (M3) | |
La vivencia de las madres respecto a la relación sus con sus hijos
Al igual que en otras investigaciones13,29, en esta también, las madres viven la relación con sus hijos desde la “felicidad”, el “gozo” y el “disfrute”. Pese a esta percepción tan positiva sobre la maternidad, las madres que participaron en esta experiencia subrayan que, para que esto ocurra, deben sentirse liberadas de diversas obligaciones, las relacionadas tanto con el “trabajo” fuera del hogar, como con las “tareas” del hogar, ya que dichos quehaceres les quitan “tiempo” para disfrutar de esta relación.
Señalar el “trabajo” fuera del hogar como factor no facilitador de la relación no es nuevo13. Se piensa que las madres empleadas, es decir, que trabajan fuera del hogar, se esfuerzan por compensar su ausencia para así asegurar que el tiempo que pasan con sus hijos sea de calidad30.
En cuanto a las “tareas” del hogar, algunas investigadoras sostienen que los placeres de la crianza suelen verse comprometidos por el aumento de las tareas domésticas que conlleva la maternidad31, quehaceres que generalmente, según nuestras participantes, recaen sobre ellas.
La vivencia de las madres respecto a ellas mismas
Las participantes relatan que viven en “alarma constante” en cuanto a la crianza. A este respecto, aseguran que la maternidad implica: por un lado “preocupación”, al ver, en ocasiones, mal a sus bebés, o al no saber si están haciendo las cosas bien –testimonio acorde con el estudio de Wilkins14–; y, por otro lado, “miedo”, provocado por la incertidumbre o desconocimiento de los retos o peligros a los que se expondrán sus hijos en un futuro.
Además, las madres de este estudio reivindican “necesitar tiempo para ellas”. Esta declaración coincide con investigaciones previas en las que las madres afirman sentirse estresadas, cansadas, desbordadas13,29, poniendo de manifiesto que les parece que han perdido cierto control sobre sus vidas32. De tener la opción, las madres de este estudio invertirían el “tiempo” que reclaman en volver a estar consigo mismas para reencontrarse con lo que eran antes, con cosas tan simples como recuperar algunas de sus aficiones previas a la maternidad.
Esta sensación de pérdida de control está estrechamente vinculada a la clasificación de prioridades que describen, en el que “en un primer lugar está el niño, luego las tareas del hogar, luego la pareja, más tarde otra vez el niño, y por último ellas”. Como afirma Gilligan33, se puede pensar que las mujeres desarrollan una “ética del cuidado” basado en la responsabilidad hacia los demás.
La vivencia de las madres respecto al apoyo social percibido
La mayoría de las madres afirman sentirse afortunadas por “entenderse con su pareja” y porque esta se “implica” en la crianza. Cuando hablan sobre la familia extensa, por un lado, reconocen la ayuda que les proporcionan sobre todo sus madres, pero, por otro lado, coinciden en asegurar que dicha ayuda va acompañada muchas veces de cierta crítica respecto a su estilo de crianza, haciéndolas “sentirse mal”.
A esta “presión” se le suma también la provocada por los pediatras. Al parecer, cuando a las madres se les informa sobre el crecimiento correcto de hijo, entienden que indirectamente se les comunica que lo están haciendo bien, generando en torno a este encuentro una vivencia positiva34. Por tanto, se supone que, si ocurre lo contrario, es decir, cuando se da cuenta de que el crecimiento del hijo no es el esperado o deseado, entonces dicho encuentro generará una vivencia negativa, derivada de la sensación de estar siendo evaluadas en la ejecución del rol materno.
Los testimonios recogidos coinciden con estudios previos34,35, en los que las madres ponen de manifiesto la presión social a la que se ven sometidas.
DISCUSIÓN
Al igual que en otros estudios13,14,32, las mujeres participantes reconocen el disfrute que les confiere la maternidad, y señalan como factor obstaculizador la dificultad de conciliar la vida laboral y la familiar. Esta realidad supone que muchas mujeres, sobre todo las laboralmente activas, vivan sumidas en una constante contradicción entre cómo les gustaría ejercer su maternidad, y cómo realmente pueden llevarla a cabo. Por tanto, conviene compartir con ellas los postulados de los estudios36,37 en los que se afirma que, actualmente, estar empleada no afecta al desarrollo evolutivo de sus hijos e hijas, ya que los padres contribuyen más que antes en la crianza y la calidad de las escuelas infantiles ha incrementado considerablemente.
Este estudio pone de manifiesto, al igual que otros14, que las mujeres viven la maternidad desde un estado de alarma constante, preocupación, duda, incertidumbre y miedo debido a la gran exigencia y responsabilidad que conlleva. Paliar esta angustia puede ser uno de los quehaceres de los profesionales de PAP. Para ello, puede ser clave construir una relación médico-paciente basada en el reconocimiento de la ética del cuidado desarrollado por las mujeres33. Además, desde la atención que los pediatras ofrecen, se puede tratar de ayudar a las madres en la identificación de las necesidades individuales de sus hijos, liberándolas de las creencias dogmáticas que no contemplan la existencia de dicha diversidad6.
El discurso de las madres se unifica al exponer la implicación de los padres en la crianza, y al denunciar la presión social a la que se hayan sometidas. Dicha denuncia aparece también en otros estudios34,35, en los que, al igual que en este, se identifica a los pediatras como agentes que participan en el incremento de la exigencia externa vivida. Para dejar de alimentar esta percepción, podría ser de utilidad tomar en consideración las demandas formuladas por las madres, en las que reclaman la necesidad de sentirse entendidas, de recibir apoyo emocional y de reflexionar sobre la crianza sin ser cuestionadas15,38.
Sin embargo, este tipo de relación médico-paciente no es la más habitual ya que, como indican diferentes estudios, las recomendaciones o prescripciones son habituales en las consultas, sean estas solicitadas o no16,39. Por tanto, la identificación de prácticas que escapan al modelo técnico y evaluativo puede ser una estrategia para descubrir nuevas formas de actuación adecuadas a las necesidades expresadas por las madres. La formación parece la llave para este cambio. Si se otorga más importancia a la influencia del bagaje personal de cada pediatra40 y a la comunicación16, es posible lograr capacitar a los profesionales para tratar las dificultades en los procesos evolutivos, sin culpabilizar a las madres, y ayudándolas a deconstruir la fantasía de la maternidad perfecta41, para asegurar así una mayor y mejor adhesión a las recomendaciones pediátricas8,42 y, consecuentemente, la promoción de la salud infantil.
Por último, aunque debido a la homogeneidad de la muestra pueda considerarse suficiente43, la generalización de los resultados de este estudio está limitada por su reducido tamaño. Esto sugiere que, en futuros estudios, la muestra, además de ser mayor, también debe ser más heterogénea, con el fin de conocer la diversidad existente sobre la vivencia de la maternidad. Así, se podría adecuar mejor la atención a las necesidades de las diferentes madres que acuden a las consultas de PAP.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
MIR: médicos internos residentes • PAP: Pediatría de Atención Primaria.
AGRADECIMIENTOS
Queremos hacer constar nuestro agradecimiento al Servicio de Juventud y Educación del Ayuntamiento de Escoriaza (Guipúzcoa), que ha colaborado en este estudio ayudando a configurar la muestra y ofreciendo un lugar donde desarrollar los grupos de discusión.
BIBLIOGRAFÍA
- Ruiz-Canela Cáceres J, Martín Muñoz P. Futuro de la Pediatría de Atención Primaria desde la perspectiva de un pediatra de hoy. Rev Pediatr Aten Primaria. 2004;6:187-97.
- Nunes C. Pediatricians’ ideas about child development and education. Psicol Reflex Crit. 2011;24:765-72.
- Tanner L, Stein MT, Olson LM, Radecki L, Frintner MP. Reflections on well-child care practice: a national study of pediatric clinicians. Pediatrics. 2009;124:849-57.
- Berkule-Silberman SB, Dreyer BR, Huberman HS, Klass PE, Mendelsohn AL. Sources of parenting information in low SES mothers. Clin Pediatr (Phila). 2010;49:560-8.
- Cheng T, Savageau J, Bigelow C, Charney E, Kumar S, DeWitt T. Assessing mothers’ attitudes about the physician’s role in child health promotion. Am J Public Health. 1996;86:1809-12.
- Burrueco J. Primeros vínculos (en la vida y en las consultas). Rev Pediatr Aten Primaria. 2002;4:137-46.
- Ammentorp J, Sabroe S, Kofoed P, Mainz J. The effect of training in communication skills on medical doctors’ and nurses’ self-efficacy. A randomized controlled trial. Patient Educ Couns. 2007;66:270-7.
- Clayman ML, Wissow LS. Pediatric residents’ response to ambiguous words about child discipline and behaviour. Patient Educ Couns. 2004;55:16-21.
- Baker LH, O’Connell D, Platt FW. What else? Setting the agenda for the clinical interview. An Inter Med. 2005;143:766-70.
- Thomson R, Kehily MJ, Hadfield L, Sharpe S. Making modern mothers. Bristol: Policy Press; 2011.
- Kralik D, Visentin K, Van Loon A. Transition: a literature review. J Adv Nursing. 2006;55:320-9.
- Mercer RT. Nursing support of the process of becoming a mother. J Obstet Gynecol Neonatal Nur. 2006;35:649-51.
- Berlanga-Fernández S, Vizcaya-Moreno MF, Pérez-Cañaveras RM. Percepción de la transición a la maternidad: estudio fenomenológico en la provincia de Barcelona. Aten Primaria. 2013;45:409-17.
- Wilkins C. A qualitative study exploring the support needs of firsttime mothers on their journey towards intuitive parenting. Midwifery. 2006;22:169-80.
- Leahy-Warren P. First-time mothers: social support and confidence in infant care. J Adv Nursing. 2005;50:479-88.
- Nunes C, Ayala M. ¿Consejo o prescripción? Análisis de las recomendaciones pediátricas en las consultas del programa de salud infantil. Rev Pediatr Aten Primaria. 2013;15:135-43.
- Nelson AM. Transition to motherhood. J Obstet Gynecol Neonatal Nurs. 2003;32:465-77.
- Nyström K, Öhrling K. Parenthood experiences during the child’s first year: literature review. J Adv Nursing. 2004;46:319-30.
- Mertens DM. Research and evaluation in Education and Psychology: Integrating diversity with quantitative, qualitative, and mixed methods. 2.ª edición. Thousand Oaks: Sage; 2005.
- Bogdan RC, Biklen SK. Qualitative research for education. 4.ª edición. Boston: Allyn & Bacon; 2003.
- Hernández R, Fernández C, Baptista P. Metodología de la investigación. 4.ª edición. México: McGraw-Hill lnteramericana; 2006.
- Krueger RA. El grupo de discusión: guía práctica para la investigación aplicada. Madrid: Pirámide; 1991.
- Gil Flores J. La metodología de investigación mediante grupos de discusión. La metodología de investigación mediante grupos de discusión. Enseñanza & Teaching: Revista Interuniversitaria de Didáctica. 1992;10-11:199-214.
- Llopis R. Grupos de discusión. Madrid: ESIC; 2004.
- Morgan DL. Focus groups as qualitative research. Newbury Park, CA: Sage; 1988.
- Krippendorff K. Content analysis. Beverly Hills: Sage Publications; 1980.
- San Martín D. Teoría fundamentada y Atlas.ti: recursos metodológicos para la investigación educativa. Rev Elect Inves Educativa. 2014;16:104-22.
- Glaser B, Strauss A. The discovery of grounded theory: strategies for qualitative research. Nueva York: Aldine Publishing Company; 1967.
- Berlanga-Fernández S, Vizcaya-Moreno MF, Pérez-Cañaveras RM, Berlanga-Fernández F. Satisfacción en la provisión de redes de apoyo social en grupos de acompañamiento a la maternidad. Enferm Global. 2014;13:18-32.
- Broom BL. Impact of marital quality and psychological wellbeing on parental sensitivity. Nursing Res. 1994;43:138-43.
- Nomaguchi KM, Milkie MA. Costs and rewards of children: the effects of becoming a parent on adults’ lives. J Marriage Fam. 2003;65:356-74.
- Darvill R, Skirton H, Farrand P. Psychological factors that impact on women’s experiences of first-time motherhood: a qualitative study of the transition. Midwifery. 2010;26:357-66.
- Gilligan C. La moral y la teoría. Psicología del desarrollo femenino. México: Fondo de Cultura Económica; 1985.
- Berlanga-Fernández S, Pérez-Cañaveras RM, Vizcaya-Moreno MF, Berlanga-Fernández F, González NA. Experiencias en un grupo de apoyo para madres con niños menores de un año. Enferm Global. 2013;30:458-69.
- Leahy P. Social support for first-time mothers: an Irish study. Am J Maternal Child Nurs. 2007;32:368-74.
- Lombardi CM, Coley RL. Early maternal employment and children’s school readiness in contemporary families. Develop Psychology. 2014;50:2071-84.
- Lombardi CM, Coley RL. Early maternal employment and children’s academic and behavioral skills in Australia and the United Kingdom. Child Development. 2017;88:263-81.
- Berlanga-Fernández S, Pérez-Cañaveras RM, Vizcaya-Moreno MF, Tarrés-Cansado R. Apoyo social formal a un grupo de madres con hijos menores de un año. Aquichan. 2013;13:206-15.
- Manning KM, Ariza AJ, Massimino TK, Binns HJ. Health supervision visits of very young children: time addressing 3 key topics. Clin Pediatr. 2009;48:931-8.
- Ganal CD, Foster CW. Parenting in practice: help or hindrance? Pediatr Ann. 2008;37:256-60.
- Panadero Utrilla E, Escribano Ceruelo E, Duelo Marcos M. La maternidad perfecta. La lactancia materna y sus expectativas. Rev Pediatr Aten Primaria. 2010;12:543-6.
- Nunes C, Ayala A. ¿Qué piensan las madres sobre el programa de seguimiento de la salud infantil? Rev Pediatr Aten Primaria. 2007;9:411-25.
- Holloway I, Wheeler S. Qualitative research in nursing. 2.ª edición. Oxford: Blackwell Science; 2002.