
Vol. 20 - Num. 77
Originales
Revisión clínica y diagnóstica de la enfermedad de Kawasaki: estudio descriptivo, retrospectivo y analítico
Beatriz Baleato Gómeza, Carmen González Ávilaa, Borja Souto Cainzosa, Beatriz Iglesias Gonzáleza, Cristina González Menchéna, José Tomás Ramos Amadora
aServicio de Pediatría. Hospital Clínico Universitario San Carlos. Madrid. España.
Correspondencia: B Baleato. Correo electrónico: bea_0019@hotmail.com
Cómo citar este artículo: Baleato Gómez B, González Ávila C, Souto Cainzos B, Iglesias González B, González Menchén C, Ramos Amador JT. Revisión clínica y diagnóstica de la enfermedad de Kawasaki: estudio descriptivo, retrospectivo y analítico. Rev Pediatr Aten Primaria. 2018;20:15-24.
Publicado en Internet: 02-11-2017 - Número de visitas: 26825
Resumen
Introducción: la enfermedad de Kawasaki es una vasculitis aguda, febril y autolimitada, que puede complicarse con alteraciones cardiovasculares. Su diagnóstico se basa en criterios clínicos. A pesar de un tratamiento eficaz, es la principal causa de cardiopatía adquirida en niños de países desarrollados. Objetivos: analizar la prevalencia de alteraciones coronarias en pacientes pediátricos diagnosticados en nuestro medio; evaluar las características demográficas, clínicas y analíticas de la población de estudio y describir los factores de riesgo de alteración coronaria en niños con enfermedad de Kawasaki.
Métodos: se revisaron de forma retrospectiva las historias clínicas de los niños diagnosticados de enfermedad de Kawasaki desde enero de 1997 hasta diciembre de 2016 en el Hospital Clínico San Carlos (Madrid, España). Se consideró diagnóstico de enfermedad de Kawasaki la presencia de los criterios clínicos propuestos por la Academia Americana de Pediatría en 2017.
Resultados: la enfermedad de Kawasaki se presentó fundamentalmente durante el invierno (n = 13; 56,5%) en mujeres (n = 12; 52,2%) de cinco años o menos (n = 18; 78,3%), que desarrollaron fiebre (n = 23; 100%) junto con cambios en la mucosa orofaríngea (n = 21; 91,3%) y presentaron proteína C reactiva y velocidad de sedimentación globular elevadas (n = 20; 86,95% y n = 13; 86,6%). Fueron tratados con inmunoglobulina intravenosa (n = 22; 95,7%) y ácido acetilsalicílico a dosis antiinflamatoria (n = 22; 95,7%) o antiagregante (n = 20; 87%). Tres pacientes (13%) desarrollaron alteraciones coronarias, que terminaron remitiendo.
Conclusiones: en nuestra cohorte, la prevalencia de alteraciones coronarias fue similar a la reportada en nuestro medio y superior a la descrita en estudios internacionales. Los factores de riesgo de alteración coronaria son predominantemente niños con retraso en el diagnóstico y tratamiento, leucocitosis >12 000/ul, proteína C reactiva >3 mg/dl y trombocitosis.
Palabras clave
● Enfermedad coronaria ● Factores de riesgo ● Síndrome mucocutáneo linfonodularINTRODUCCIÓN
La enfermedad de Kawasaki (EK) o síndrome mucocutáneo linfonodular es una vasculitis aguda febril que afecta a vasos de pequeño y mediano calibre. Fue descrita por primera vez en 1967 por Tomisaku Kawasaki1. Aunque se trata de un proceso autolimitado que ocurre principalmente en la infancia, puede producir complicaciones cardiacas con una significativa morbimortalidad. Por ello, es la principal causa de cardiopatía adquirida en niños de países desarrollados2.
Es una enfermedad con mayor incidencia en raza asiática3,4 (incidencia estimada de 30,3/100 000 niños menores de cinco años) y varones (1,5:1)5,6. Es menos frecuente en menores de seis meses o mayores de cinco años, siendo diagnosticada generalmente de manera tardía y por lo tanto con mayor riesgo de alteraciones coronarias (AC).
Aunque es una enfermedad que se conoce desde hace 50 años, su etiología es todavía desconocida4,7. Parecen estar involucrados factores genéticos (países asiáticos y antecedentes familiares), inmunológicos (inicialmente se relacionó con una respuesta inmune desencadenada por un superantígeno, pero estudios actuales se decantan por una respuesta en cascada por un antígeno convencional)6,8 e infecciosos (predominio invernal, con posible relación de infección por virus o bacterias tales como el parvovirus B19, retrovirus, virus de Epstein-Barr, virus del herpes humano, C. pneumoniae y Mycoplasma; así como los síndromes del shock tóxico estafilocócico y estreptocócico). Por todo ello, se considera la base fisiopatológica de la EK como una respuesta inmune patológica y estereotipada ante uno o varios factores ambientales o infecciosos en individuos genéticamente predispuestos4,9.
La EK se caracteriza por una inflamación sistémica de los vasos de mediano calibre y de múltiples órganos y tejidos durante la fase febril aguda. La clínica es variable y depende de la afectación: gastrointestinal (dolor abdominal, vómitos, diarrea, hepatitis, pancreatitis), pulmonar (neumonitis intersticial), meníngea (meningitis aséptica, irritabilidad), cardiaca (coronariopatía, miocarditis, pericarditis, valvulopatía), urinaria (piuria estéril), musculoesquelética (artritis, artralgias) y nódulos linfáticos (linfadenopatía)4,6,10. La vasculopatía se produce en tres etapas: arteritis necrotizante, un proceso autolimitado (primeras dos semanas), seguido de vasculitis subaguda o crónica, que en un pequeño porcentaje de casos puede perdurar durante meses o años y progresar a proliferación luminal miofibroblástica6,11.
El diagnóstico de EK se basa en la presencia de criterios clínicos1,6,12 que incluyen fiebre ≥5 días asociada al menos a cuatro de los siguientes hallazgos: rash polimorfo, cambios en las extremidades distales (eritema y edema de manos o pies, descamación periungueal a partir de la segunda semana), cambios en mucosa oral (lengua aframbuesada, fisuración, eritema, sequedad), conjuntivitis bilateral no exudativa o linfadenopatía cervical >1,5 cm (generalmente unilateral); en caso de presentar ≥4 criterios clínicos (particularmente en presencia de eritema y edema de manos y pies), puede diagnosticarse EK con solo cuatro días de fiebre. Estas manifestaciones inflamatorias pueden presentarse de forma secuencial. Se diagnostica EK completa o clásica cuando se cumple la definición de caso, y EK incompleta en presencia de fiebre prolongada con menos de cuatro criterios clínicos y hallazgos ecocardiográficos o de laboratorio compatibles6.
Se requiere un índice de sospecha alto ante la presencia de fiebre y algún criterio clínico diagnóstico debido a la inespecificidad de los principales síntomas y signos de enfermedad. Es necesario descartar otras patologías con curso clínico similar, ya que no existe ninguna prueba diagnóstica específica de la EK6.
Los estudios de laboratorio típicamente muestran recuento leucocitario normal o alto con neutrofilia, elevación de reactantes de fase aguda (proteína C reactiva [PCR], velocidad de sedimentación globular [VSG]), anemia normocítica normocrómica, piuria estéril, hipoalbuminemia, hiponatremia, elevación de enzimas hepáticas y trombocitosis6. No obstante, aun siendo inespecífico, apoyan el diagnóstico, destacando su importancia en la EK incompleta.
Las complicaciones más significativas por su gravedad implican cambios patológicos en las arterias coronarias. Estas comprenden aneurismas, ectasia, anomalías vasodilatadoras funcionales, estenosis de la luz vascular, disminución de la contractilidad miocárdica, regurgitación valvular leve y derrame pericárdico, siendo la principal secuela de la EK los aneurismas coronarios. Aproximadamente el 25% de los pacientes no tratados precozmente con altas dosis de inmunoglobulina intravenosa (IGIV) desarrolla complicaciones cardiovasculares, descendiendo a un 4% desde la introducción de la IGIV2. Estudios recientes sugieren que un porcentaje mucho mayor de niños con EK tiene cambios sutiles y a menudo transitorios de las arterias coronarias13. Los factores de riesgo asociados con las alteraciones de arterias coronarias no están bien establecidos, aunque se han descrito el diagnóstico tardío y el retraso en el tratamiento con IGIV, edad <1 año y >9 años, sexo masculino, fiebre prolongada, falta de respuesta a la terapia IGIV inicial y hallazgos de laboratorio sugerentes de inflamación grave y persistente14-18.
Existe una mayor incidencia de AC en la EK incompleta, hallazgo que se ha relacionado con una mayor frecuencia de retraso en el diagnóstico y tratamiento, ya que pueden pasar inadvertidos18.
Para el tratamiento en fase aguda se recomienda administrar una doble terapia con IGIV y ácido acetilsalicílico (AAS) una vez confirmado el diagnóstico, preferentemente antes del décimo día de enfermedad6,19.
La IGIV se administra de manera intravenosa a dosis 2 g/kg en una sola infusión durante 10-12 horas. Aunque su mecanismo es desconocido, parece tener un efecto antiinflamatorio generalizado, considerándose el mejor tratamiento para prevenir las AC6,19.
En fase aguda se recomienda administrar AAS a dosis antiinflamatorias, de 30 a 100 mg/kg/día, dividida en cuatro tomas. Tras 48-72 horas sin fiebre, se cambia a dosis antiagregante de 3-5 mg/kg durante 6-8 semanas si el paciente no presenta afectación coronaria20.
En los pacientes con alto riesgo de desarrollar AC puede considerarse el tratamiento adyuvante con corticosteroides6,21.
En casos refractarios (10-20% de casos), definidos como la ausencia de respuesta tras 36 horas de finalizar la infusión de IGIV, el tratamiento es controvertido6,22. Se recomienda una segunda dosis de IGIV, pudiendo considerarse los corticosteroides (como alternativa o junto con IGIV) o infliximab. Otros tratamientos como la ciclosporina o terapia con anticuerpos monoclonales inmunomoduladores pueden plantearse en caso de resistencia a los anteriores6,22,23.
El pronóstico está determinado por la AC. En Japón, la recurrencia aproximada es del 3%, más alta en los dos primeros años del caso inicial y presentando mayor riesgo de desarrollar secuelas coronarias. La mortalidad ronda el 0,015%, consecuencia de las secuelas coronarias, con un pico entre los 15-45 días del inicio de la fiebre, habiendo casos de muerte súbita a lo largo del seguimiento6.
Hipótesis: la prevalencia de AC en nuestro medio es similar a la reportada en la literatura médica. Los factores de riesgo para el desarrollo de AC en pacientes pediátricos diagnosticados de EK se cumplen en nuestra muestra.
Objetivos: analizar la prevalencia de AC en pacientes pediátricos diagnosticados de EK en nuestro medio, describir los factores de riesgo de AC en niños con EK y evaluar las características clínicas, analíticas y demográficas de la población de estudio.
MATERIAL Y MÉTODOS
Diseño del estudio
Se diseñó un estudio epidemiológico analítico, observacional, de seguimiento retrospectivo. La muestra de estudio procede del Área Sanitaria del Hospital Clínico San Carlos (HCSC) (Madrid, España) y está compuesta por los niños diagnosticados de EK desde el 1 de enero de 1997 y hasta el 31 de diciembre de 2016.
Criterios de inclusión: todos los pacientes de 0 a 18 años diagnosticados de EK entre las fechas mencionadas. Criterios de exclusión: pacientes con datos insuficientes (ausencia de información sobre los criterios clínicos, analíticas o pruebas de imagen cardiaca durante el proceso diagnóstico); y pacientes diagnosticados de EK que fue posteriormente descartada durante la evolución.
Aspectos éticos
Se realizó una recogida de datos donde se valoran los resultados de las pruebas en los pacientes y distintos parámetros en sus respectivas historias clínicas previa solicitud de la exención del consentimiento informado y aprobación por el Comité Ético de Investigación del HCSC.
Metodología
Se revisaron de forma retrospectiva las historias clínicas de los niños diagnosticados de EK desde enero de 1997 hasta diciembre de 2016 en el HCSC. Se ha incluido en un registro multipropósito diferentes variables epidemiológicas, clínicas, analíticas, de respuesta al tratamiento y complicaciones cardiológicas. Las variables incluidas en el estudio son: epidemiológicas (edad al diagnóstico, sexo, estación y duración de ingresos), clínicas (fiebre, rash polimorfo, cambios en las extremidades distales, linfadenopatía cervical, cambios en la mucosa oral e inyección conjuntival), analíticas (anemia, leucocitosis con neutrofilia, trombocitosis, PCR elevada, VSG elevada, elevación de transaminasas, hipoalbuminemia, piuria estéril y hemocultivos), de respuesta al tratamiento (duración de la fiebre tras tratamiento, uso de AAS y IGIV), y complicaciones cardiovasculares (alteraciones ecocardiográficas, fecha de diagnóstico y resolución).
Los datos utilizados en el análisis estadístico se han obtenido a partir de notas clínicas, informes de hospitalización, datos de ecocardiografías y analíticas.
Se consideró diagnóstico de EK la presencia de los criterios clínicos propuestos por la Academia Americana de Pediatría en 2017, donde se define EK completo o clásico cuando el paciente presenta al menos cuatro días de fiebre junto con ≥4 criterios clínicos y EK incompleto cuando presenta al menos cinco días de fiebre junto con dos o tres criterios clínicos y alteración ecocardiográfica o criterios de laboratorio que apoyen el diagnóstico (PCR ≥3 mg/dl o VSG ≥40 mm/h junto con ≥3 criterios suplementarios: albúmina <3 g/dl, anemia, elevación de la alanina aminotransferasa, trombocitosis tras siete días ≥450 000/μl, leucocitos ≥12 000/μl y piuria estéril). Se clasificó como EK refractaria a IGIV cuando la fiebre persistía tras 36 horas de finalizar la IGIV.
Los pacientes diagnosticados de EK ingresaron en la planta de hospitalización pediátrica cuando se encontraban en los primeros diez días del inicio de la fiebre o pasados los diez días del inicio cuando continuaban con fiebre o presentaban alteraciones analíticas con aumento de los reactantes de fase aguda o alteraciones ecocardiográficas. Los pacientes ingresados recibieron tratamiento con IGIV a 2 g/kg/dosis única o 400 mg/kg en cinco dosis y AAS a 80-100 mg/kg/día hasta permanecer al menos 48 horas afebril, pasando a dosis de mantenimiento entre 3-5 mg/kg/día en una sola dosis durante 4-8 semanas en caso de no presentar AC. Se realizó ecocardiografía, analítica y electrocardiografía al diagnóstico. Tras el alta hospitalaria, se siguieron en las consultas de Cardiología, realizándose un control ecocardiográfico a las cuatro y ocho semanas y posteriormente según la presencia o no de AC.
Análisis estadístico
En el análisis estadístico las variables cualitativas se han presentado con su distribución de frecuencias y porcentajes. Las variables cuantitativas se han resumido en su media y su desviación estándar en el caso de que la variable se distribuyese como una normal, en caso contrario se ha resumido con su mediana y el rango intercuartílico. El programa estadístico utilizado para ello ha sido IBM SPSS® Statistics 23.
RESULTADOS
Un total de 25 pacientes fueron diagnosticados de EK entre los años 1997-2016. Se perdió información relativa al diagnóstico en un paciente y se descartó EK en otro paciente tras comenzar con exudación amigdalar bilateral con buena respuesta a antibioterapia oral, siendo ambos excluidos del estudio. Del total de la muestra (n = 23), 20 (87%) fueron diagnosticados de EK clásica y 3 (13%) de EK incompleta. La mediana de edad al diagnóstico en la muestra fue de 2,8 (rango 1,4-5,0) años.
En cuanto al sexo, 11 fueron varones (47,8%) y 12 fueron mujeres (52,2%). Los diagnósticos se hicieron mayoritariamente en invierno, 13 pacientes (56,5%), seguido por el verano con cinco pacientes (21,7%). La estancia media de los pacientes fue de seis días (rango 4,0-12,0).
Criterios clínicos
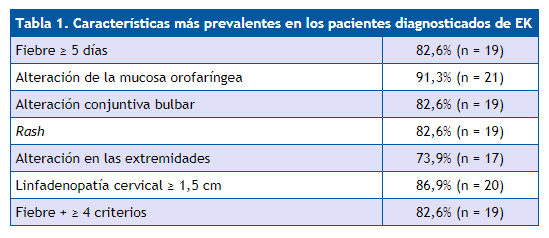
En cuanto a los criterios clínicos, 20 pacientes (86,9%) presentaron fiebre ≥5 días. Se palparon adenopatías cervicales >1,5 cm en 20 pacientes (86,9%). El rash polimorfo lo desarrollaron 19 pacientes (82,6%). Se encontraron cambios en las extremidades distales en 17 pacientes (73,9%) y en la mucosa oral en 21 pacientes (91,3%). Finalmente, presentaron inyección conjuntival bilateral no supurativa 19 pacientes (82,6%). El total de criterios clínicos que presentaban de media fue de 4,17 ± 0,95, con un valor máximo de cinco criterios en ocho pacientes (34,7%) (Tabla 1).
| Tabla 1. Características más prevalentes en los pacientes diagnosticados de EK | |
|---|---|
| Fiebre ≥5 días | 82,6% (n = 19) |
| Alteración de la mucosa orofaríngea | 91,3% (n = 21) |
| Alteración conjuntiva bulbar | 82,6% (n = 19) |
| Rash | 82,6% (n = 19) |
| Alteración en las extremidades | 73,9% (n = 17) |
| Linfadenopatía cervical ≥1,5 cm | 86,9% (n = 20) |
| Fiebre + ≥4 criterios | 82,6% (n = 19) |
Criterios analíticos
Los resultados del análisis de los parámetros analíticos recogidos son: 11 pacientes (47,8%) mostraron leucocitosis con neutrofilia, 13 pacientes (59,1%) presentaron leucocitosis >12 000/mm3. En cuanto a las alteraciones plaquetarias, nueve pacientes (42,9%) presentaron trombocitosis, dos (9,5%) trombocitopenia y diez (47,6%) se encontraron dentro de la normalidad. El valor de la PCR encontró elevada (>3 mg/dl) en 20 pacientes (86,95%). Se analizó la VSG en 15 pacientes, observándose VSG elevada en 13 de ellos (86,6%). También se registraron los valores de hemoglobina encontrando anemia en diez (43,5%) de los pacientes. En cuanto al hallazgo de piuria estéril, solo en cuatro pacientes (18,2%) resultó positiva. Se realizaron hemocultivos en diez pacientes, siendo negativo en el 100%. Otras variables recogidas fueron: albúmina, registrada solo en seis pacientes, en los cuáles en la mitad (n = 3) se encontró baja y en la otra mitad (n = 3) dentro del rango de normalidad y el valor de las transaminasas, observándose elevadas en 11 pacientes (57,9%) frente a ocho pacientes (42,1%).
Tratamiento
De los pacientes de la muestra (n = 23), 22 (95,7%) fueron tratados con IGIV. Hubo un paciente que no fue tratado con IGIV por retraso en el diagnóstico (>10 días), normalización de la analítica y control ecocardiográfico normal a su llegada a Urgencias. Este fue diagnosticado de EK clásica y el único tratamiento que recibió fue AAS a dosis antiagregante (3-5 mg/kg/día).
Se registra la dosis recibida en 19 de estos pacientes, donde 17 de ellos (89,5%) fueron tratados con IGIV a dosis de 2 g/kg/dosis única, mientras que en los otros dos (10,5%) la dosis fue de 400 mg/kg/5 dosis, pauta en desuso desde 2004. Desde el inicio del cuadro febril, se tardó en administrar el tratamiento con IGIV siete (5,0-9,0) días, siendo tres pacientes los que se trataron más allá del décimo día.
En cuanto al tratamiento con AAS, 22 pacientes (95,7%) lo recibieron a dosis antiinflamatorias (80-100 mg/kg/día), tardando en recibirlo desde la fecha de ingreso un (0,0-2,0) día. Solo se recogió la duración del mismo en 15 pacientes, que fue de tres (2,5-4,0) días. Por otra parte, 20 pacientes (87%) recibieron AAS a dosis antiagregante (3-5 mg/kg/día), uno de ellos sin haber recibido previamente AAS a dosis antiinflamatorias. Ningún paciente fue tratado con clopidogrel.
La respuesta clínica al tratamiento con IGIV fue recogida en 20 pacientes, siendo seis (30%) los que presentaron EK refractaria. Se administró una segunda dosis de IGIV en cinco pacientes (22,7%), tres de los cuales presentaban EK refractaria según los criterios actuales.
Alteraciones coronarias
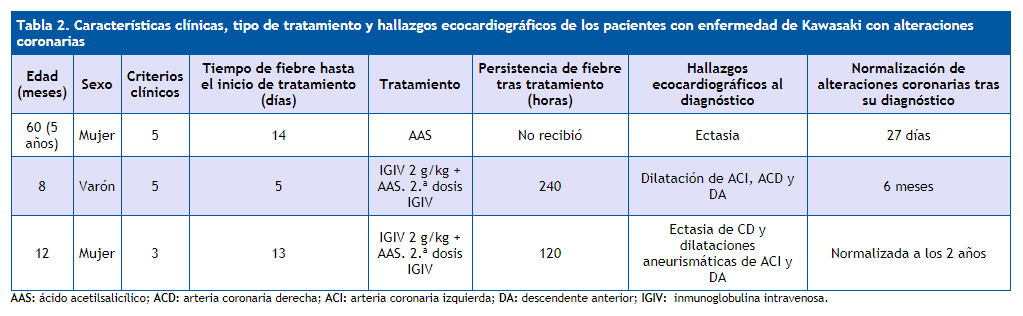
De los 23 pacientes de la muestra, tres de ellos desarrollaron AC (13%), uno de ellos ectasia coronaria (paciente A), otro dilataciones aneurismáticas (paciente B) y el restante ectasia y dilataciones aneurismáticas (paciente C).
La paciente A era una mujer de cinco años diagnosticada de EK clásico en invierno. El paciente B era un varón de ocho meses diagnosticado de EK clásico en invierno. Finalmente, la paciente C era una mujer de 12 meses diagnosticada de EK incompleto en invierno.
Las alteraciones analíticas que presentaba la paciente A fueron leucocitosis con desviación a la izquierda (leucocitos 25 300/μl con 68,3% de neutrófilos), trombocitosis (714 000/μl), piuria estéril (25 leucocitos por campo), PCR (11,6 mg/dl) y VSG (116 mg/dl) elevadas. El paciente B presentaba leucocitosis (14 460/μl), PCR (8,3 mg/dl) y VSG elevadas, trombocitosis (992 000/μl), anemia (12,6 g/dl), hemocultivo negativo e hipoalbuminemia. El paciente C presentaba leucocitosis con neutrofilia (19 600/μl con 57,7% de neutrófilos), trombocitosis (527 000/μl), PCR elevada (10,8 mg/dl), anemia (10,7 g/dl), piuria estéril, hipoalbuminemia y transaminasas ligeramente elevadas.
En relación con el tratamiento, la paciente A no fue tratada con IGIV. Recibió únicamente AAS a dosis antiagregante durante tres meses. El paciente B fue tratado con IGIV a 2 g/kg/dosis única tras cinco días de haber comenzado con el cuadro febril, con AAS a dosis antiinflamatorias durante 23 días y posteriormente a dosis antiagregante durante 6,5 meses. Persistió la fiebre 240 horas desde el inicio del tratamiento, por lo que necesitó retratamiento con IGIV. Finalmente, la paciente C fue tratada con IGIV a 2 g/kg/dosis única tras 13 días de haber comenzado con el cuadro febril, con AAS a dosis antiinflamatorias durante tres días y a dosis antiagregante durante 36 meses. Presentó fiebre 120 horas desde el inicio del tratamiento, por lo que necesitó retratamiento con IGIV.
En cuanto a los hallazgos ecocardiográficos, la paciente A fue diagnosticada de ectasia en el tercer control ecocardiográfico realizado un mes y 25 días tras el diagnóstico, siendo el primer y segundo control normales a los 13 y 32 días respectivamente del diagnóstico de EK. Se observa normalización en el cuarto control a los 27 días del diagnóstico de dicha alteración. El paciente B fue diagnosticado de dilataciones aneurismáticas en el segundo control ecocardiográfico 17 días después del diagnóstico de EK, siendo el primer control normal a los dos días del diagnóstico. Normalización en el cuarto control, seis meses y 20 días tras el diagnóstico del hallazgo en arterias coronarias. El paciente C fue diagnosticado de EK, ectasia y dilataciones aneurismáticas el mismo día de ingreso. Se desconoce el seguimiento de las alteraciones de este paciente, únicamente se registra un control dos años después en el que se observa la normalización de las arterias coronarias (Tabla 2).
| Tabla 2. Características clínicas, tipo de tratamiento y hallazgos ecocardiográficos de los pacientes con enfermedad de Kawasaki con alteraciones coronarias | |||||||
|---|---|---|---|---|---|---|---|
| Edad (meses) | Sexo | Criterios clínicos | Tiempo de fiebre hasta el inicio de tratamiento (días) | Tratamiento | Persistencia de fiebre tras tratamiento (horas) | Hallazgos ecocardiográficos al diagnóstico | Normalización de alteraciones coronarias tras su diagnóstico |
| 60 (5 años) | Mujer | 5 | 14 | AAS | No recibió | Ectasia | 27 días |
| 8 | Varón | 5 | 5 | IGIV 2 g/kg + AAS. 2.ª dosis IGIV | 240 | Dilatación de ACI, ACD y DA | 6 meses |
| 12 | Mujer | 3 | 13 | IGIV 2 g/kg + AAS. 2.ª dosis IGIV | 120 | Ectasia de CD y dilataciones aneurismáticas de ACI y DA | Normalizada a los 2 años |
Además se detectaron dos pacientes con otras AC: una mujer de 12 años con diagnóstico de EK incompleto y hallazgo de disfunción ventricular leve en el primer control ecocardiográfico realizado a los dos días del diagnóstico, con resolución del mismo a los 16 días, y, por último, un varón de 20 meses con EK incompleta, en el que se observa derrame pericárdico leve alrededor de la aurícula y ventrículo derechos en el primer control a los dos días del diagnóstico, con normalización al mes.
DISCUSIÓN
La EK es una vasculitis sistémica aguda febril autolimitada, de etiología desconocida7. Presenta una incidencia en nuestro medio de 15,1/100 000 niños de ≤ 5 años24, algo inferior a la de EE. UU., cuya incidencia estimada es de 25 casos/100 000 niños ≤ 5 años5.
Hasta el momento, no se han demostrado hallazgos clínicos patognomónicos ni pruebas diagnósticas específicas para el diagnóstico de EK, por lo que nos basamos en una serie de criterios clínicos6 que no están exentos de limitaciones al no ser completamente sensibles25. En función de estos criterios, podemos diagnosticar a los pacientes de EK completa o incompleta.
En nuestra muestra, los pacientes con EK presentan características demográficas, clínicas y analíticas similares a las observadas en la literatura médica.
La mayoría de los diagnósticos se realizaron en menores de 5 años (78,3%; n = 18), durante el invierno o el verano (78,3%; n = 18). Datos muy semejantes a los encontrados en otras series como la de Prieto Tato et al.26, la incidencia de la enfermedad en función del sexo fue de 11 varones (47,8%) y 12 mujeres (52,2%). Dado la similitud en el resto de las características demográficas, pensamos que el predominio del sexo femenino se debe a que se está evaluando, en una muestra demasiado pequeña, una variable dicotómica con un pequeño margen de diferencia (1,5 varones:1 mujer)5.
El cuadro se presentó con fiebre (100%; n = 23) junto con cambios en la mucosa orofaríngea (91,3%, n = 21), inyección conjuntival bilateral no supurada (86,9%, n = 20), palpación de adenopatías cervicales (86,9%, n = 20) y rash polimorfo (82,6%; n = 19), mientras que los cambios en la extremidades distales fue la variable clínica que menos se observó entre los pacientes de la muestra (73,9%, n = 17). Datos similares se encuentran en la muestra de Prieto Tato26 donde predominaron la fiebre y la afección bucofaríngea (100%), mientras que la afección de las extremidades (67%) fue la menos frecuente26. También existe concordancia con los datos descritos por Kawasaki27, cuya muestra desarrolló preferentemente fiebre >38 °C más de seis días (100%, n = 50), inyección conjuntival bilateral no supurada (98%, n = 49) y cambios en la mucosa oral (96%, n = 48), siendo de nuevo los cambios en las extremidades la variable menos frecuente (44%, n = 22)27. Pensamos que una alta asociación entre las variables clínicas es lo esperable en una enfermedad cuyo diagnóstico se basa en la presencia de dichas manifestaciones.
Actualmente las alteraciones analíticas no forman parte de los criterios diagnósticos de la EK, pero son sugestivas de la enfermedad y apoyan el diagnóstico de EK incompleta. Las alteraciones analíticas que más se han encontrado en nuestro estudio son PCR y VSG elevadas (86,95% y 86,6% respectivamente), siendo estas también las más sugestivas según la American Heart Association (AHA)6. Destacan también leucocitosis, neutrofilia, trombocitosis, anemia y aumento de transaminasas, encontradas en alrededor de la mitad de los pacientes de la muestra. Estudios realizados en España encuentran datos similares28,29.
Las AC son la principal complicación cardiovascular de la EK, con una prevalencia del 25%, reduciéndose a aproximadamente un 4% en pacientes tratados con una sola dosis de IGIV. En la mayoría de los casos se encuentran dilataciones que se resuelven en un periodo de cuatro a ocho semanas, pero pueden llegar a aneurismas de gran tamaño, con riesgo de infarto de miocardio y muerte súbita6.
En la muestra del estudio, tres pacientes (13%) desarrollaron AC, pero solo dos de ellos recibieron tratamiento con IGIV. Teniendo esto en cuenta, el 9% de los pacientes que recibieron IGIV presentaron AC, en cualquier caso, valores superiores a los descritos por la AHA6. Sin embargo, estos datos se aproximan más a los descritos por Caballero-Mora28 y Prieto26 en sus estudios, cuyos valores de prevalencia de AC en nuestro medio son de 15,7% y 13% respectivamente. La resolución ecocardiográfica se produjo en los tres pacientes, hecho que coincide también con estos estudios.
A pesar de tratarse de una enfermedad con buen pronóstico, su importancia reside en la aparición de AC. Por ello, numerosos estudios han relacionado factores clínicos y/o analíticos con el desarrollo de AC, lo cual supone una valiosa herramienta para identificar pacientes con alto riesgo de AC.
Aunque en la literatura médica encontramos numerosos estudios publicados, es difícil encontrar un consenso global. Se han relacionado los siguientes factores: sexo varón, edad <12-24 meses y >9 años, retraso en el diagnóstico y tratamiento (>10 días del inicio del cuadro febril sin recibir IGIV), enfermedad refractaria, fase febril de larga duración, PCR elevada, leucocitos >12 000/mm3, trombocitosis, hipoalbuminemia y anemia13-18,26,28,30.
En el estudio de Beiser14 se encuentra relación entre el desarrollo de AC y sexo varón, al observarse AC en el 8,3% de mujeres frente al 17% de varones. En el estudio Caballero-Mora18, en el que se analizan posibles factores de riesgo en nuestro medio se obtienen diferencias estadísticamente significativas para sexo masculino, PCR elevada y anemia. En nuestra muestra, los tres pacientes que desarrollaron AC presentaban PCR >8 mg/dl, con un valor medio de 10,23 mg/dl; mientras que en los pacientes sin AC y elevación de la PCR, el valor medio encontrado fue de 8,1 mg/dl. Además dos de estos tres pacientes presentaron anemia. Sin embargo, solo un paciente fue varón.
En cuanto a la edad, los resultados del estudio de Honkanen15 muestran alteraciones ecocardiográficas en 10 de los 14 pacientes diagnosticados de EK <1 año. De los cinco pacientes de nuestra muestra que presentan alteraciones, tres tenían menos de 12 meses y uno más de nueve años.
En el estudio de Maric17 se describen como factores de riesgo leucocitosis, trombocitosis e hipoalbuminemia, datos que coinciden con los pacientes que desarrollan AC en nuestro estudio.
Berdej-Szczot18 analiza a 73 pacientes diagnosticados entre 2003 y 2016, concluyendo como factores de riesgo independientes: duración prolongada de la fiebre, enfermedad refractaria, diagnóstico tardío, curso sintomático sutil y trombocitosis. En nuestra muestra encontramos que dos de los pacientes con AC fueron diagnosticados y tratados con un curso febril de >10 días, 13 y 14 días concretamente, siendo además uno refractario al tratamiento. El tercer paciente, a pesar de recibir tratamiento de forma correcta y precoz, continuó con fiebre diez días más, siendo por tanto también refractario a IGIV.
Limitaciones
Este trabajo está limitado por su naturaleza retrospectiva y el número reducido de pacientes, lo que dificulta el análisis estadístico al disminuir la potencia. Además, los diagnósticos se realizan a lo largo de 20 años, por lo que no hay uniformidad de protocolos en el manejo, pudiendo existir un sesgo de metodología. Se requieren estudios con series más amplias que nos permitan un mejor conocimiento de la enfermedad en nuestro medio.
CONCLUSIONES
En nuestra cohorte, la prevalencia de AC fue similar a la reportada en nuestro medio y superior a la descrita en los medios internacionales.
Los factores de riesgo de AC encontrados en nuestra serie son semejantes a los descritos en la literatura médica, presentándose predominantemente en los niños con retraso en el diagnóstico y tratamiento, leucocitosis >12 000/ul, PCR >3 mg/dl y trombocitosis.
En nuestro medio, la EK se presentó fundamentalmente durante el invierno en mujeres de cinco años o menos, las cuales desarrollaron fiebre junto con cambios en la mucosa orofaríngea, así como PCR y VSG elevadas.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
AAS: ácido acetilsalicílico • AC: alteraciones coronarias • AHA: American Heart Association • EK: enfermedad de Kawasaki • IGIV: inmunoglobulina intravenosa • PCR: proteína C reactiva • VSG: velocidad de sedimentación globular.
BIBLIOGRAFÍA
- Kawasaki T. Acute febrile mucocutaneous síndrome with lymphoid involvement with specific desquamation of the fingers and toes in children. Arerugi. 1967;16:178-222.
- Rowley AH, Shulman ST. Kawasaki syndrome. Pediatr Cardiol. 1999;46:313-29.
- Kao AS, Getis A, Brodine S, Burns JC. Spatial and temporal clustering of Kawasaki syndrome cases. Pediatr Infect Dis J. 2008;27:981.
- Sundel R. Kawasaki disease: epidemiology and etiology. En: UpToDate [en línea] [consultado el 27/10/2017]. Disponible en www.uptodate.com/contents/kawasaki-disease-epidemiology-and-etiology
- Holman RC, Belay ED, Christensen KY, Folkema AM, Steiner CA, Schonberger LB. Hospitalizations for Kawasaki síndrome among children in the United States, 1997-2007. Pediatr Infect Dis J. 2010;29:483-8.
- McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, et al. Diagnosis, treatment and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation. 2017;135:927-99.
- Takahashi K, Oharaseki T, Yokouchi Y. Pathogenesis of Kawasaki disease. Clin Exp Immunol. 2011;164:20-22.
- Matsubara T, Ichiyama T, Furukawa S. Immunological profile of peripheral blood lymphocytes and monocytes/macrophages in Kawasaki disease. Clin Exp Immunol. 2005;141:381-7.
- Burgner D, Harnden A. Kawasaki disease: what is the epidemiology telling us about the etiology? Int J Infect Dis. 2005;9:185-94.
- Amano S, Hazama F, Kubagawa H, Tasaka K, Haebara H, Hamashima Y. General pathology of Kawasaki disease: on the morphological alterations corresponding to the clinical manifestations. Acta Pathol Jpn. 1980;30:681-94.
- Orenstein JM, Shulman ST, Fox LM, Baker SC, Takahashi M, Bhatti TR, et al. Three linked vasculopathic processes characterize Kawasaki disease: a light and transmission electronmicroscopic study. PloS One. 2012;7:e38998.
- Council on Cardiovascular Disease in the Young; Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease; American Heart Association. Diagnostic guidelines for Kawasaki disease. Circulation. 2001;103:335-6.
- Sundel R, Klein-Gitelman M, Kaplan S, TePas E. Kawasaki disease: complications. En: UpToDate [en línea] [consultado el 27/10/2017]. Disponible en www.uptodate.com/contents/kawasaki-disease-complications
- Beiser AS, Takahashi M, Baker AL, Sundel RP, Newburger JW, US Multicenter Kawasaki Disease Study Group. A predictive instrument for coronary artery aneurysms in Kawasaki disease. Am J Cardiol. 1998;81:1116-20.
- Honkanen VE, McCrindle BW, Laxer RM, Feldman BM, Schneider R, Silverma ED. Clinical relevance of the risk factors for coronary artery inflammation in Kawasaki disease. Pediatr Cardiol. 2003;24:122-6.
- Koren G, Lavi S, Rose V, Rowe R. Kawasaki disease: review of risk factors for coronary aneurysms. J Pediatr. 1986;108:388-92.
- Maric LS, Knezovic I, Papic N, Mise B, Roglic S, Markovinovic L, et al. Risk factors for coronary artery abnormalities in children with Kawasaki disease: a 10‑year experience. Rheumatol Int. 2015;35:1053-8.
- Berdej-Szczot E, Małecka-Tendera E, Gawlik T, Firek-Pędras M, Szydłowski L, Gawlik A. Risk factors of immunoglobulin resistance and coronary complications in children with Kawasaki disease. Kardiol Pol. 2017;75:261-6.
- Shulman ST. Intravenous immunoglobulin for the treatment of Kawasaki disease. Pediatr Ann. 2017;46:e25-e28.
- Sundel R. Kawasaki disease: initial treatment and prognosis. En: UpToDate [en línea] [consultado el 27/10/2017]. Disponible en www.uptodate.com/contents/kawasaki-disease-initial-treatment-and-prognosis
- Chen S, Dong Y, Yin Y, Krucoff MW. Intravenous immunoglobulin plus corticosteroid to prevent coronary artery abnormalities in Kawasaki disease: a meta-analysis. Heart. 2013;99:76-82.
- Campbell AJ, Burns JC. Adjunctive therapies for Kawasaki disease. J Infect. 2016;72:1-5.
- Kimura M, Harazaki M, Fukuoka T, Asakura I, Sakai H, Kamimaki T, et al. Targeted use of prednisolone with the second IVIG dose for refractory Kawasaki disease. Pediatr Int. 2017;59:397-403.
- Martínez Ruiz M, del Castillo Martín F, Borque Andrés C, García Miguel MJ, de José Gómez MI, Martínez Cortés F, et al. Incidencia y características clínicas de la enfermedad de Kawasaki. An Pediatr (Barc). 2003;59:323-7.
- Witt MT, Minich LL, Bohnsack JF, Young PC. Kawasaki disease: more patients are being diagnosed who do not meet American Heart Association criteria. Pediatrics. 1999;104:10.
- Prieto Tato LM, Cuesta Rubio MT, Guillén Martín S, Ruiz Jiménez M, Cortés Coto MT, Rubio Gribble B, et al. Enfermedad de Kawasaki: diagnóstico y tratamiento. An Pediatr (Barc). 2010;73:25-30.
- Kawasaki T. Pediatric acute febrile mucocutaneous lymph node syndrome with characteristic desquamation of fingers and toes: my clinical observation of fifty cases. Pediatr Infect Dis J. 2002;21:1-38.
- Caballero-Mora FJ, Alonso-Martín B, Tamariz-Martel-Moreno A, Cano-Fernández J, Sánchez-Bayle M. Enfermedad de Kawasaki en 76 pacientes. Factores de riesgo de aparición de aneurismas coronarios. An Pediatr (Barc). 2011;74:232-8.
- González Pascual E, Villanueva Lamas J, Ros Viladoms J, Pons Odena M, Ruiz García-Diego S. Enfermedad de Kawasaki. Presentación de cincuenta casos. An Pediatr Esp. 1999;50:39-43.
- Galeotti C, Kaveri SV, Cimaz R, Koné-Paut I, Bayry J. Predisposing factors, pathogenesis and therapeutic intervention of Kawasaki disease. Drug Discov Today. 2016;21:1850-7.