
Vol. 19 - Num. 76
Originales
¿Es adecuada la utilización del servicio de urgencias en el periodo neonatal?
Rosa Fornes Vivasa, Rocío Mustienes Bellotb, Agustín Navarro Juanesc, Luis Robledo Díazd, Eva Carvajal Rocae
aServicio de Urgencias de Pediatría. Hospital Católico Universitario Casa de Salud. Valencia. España.
bFacultad de Medicina y Odontología. Universidad Católica San Vicente Mártir . Valencia. España.
cServicio de Urgencias. Hospital Marina Alta. Denia. Valencia. España.
dDepartamento de Sociología y Antropología Social. Facultad de Ciencias Sociales. Universidad de Valencia. Departamento de Gestión. Hospital Católico Universitario Casa de Salud. Valencia. España.
eDepartamento de Pediatría, Ginecología y Obstetricia. Facultad de Enfermería, Medicina y Odontología. Universidad Católica San Vicente Mártir. Valencia. España.
Correspondencia: R Fornes. Correo electrónico: rfornes@comv.es
Cómo citar este artículo: Fornes Vivas R, Mustienes Bellot R, Navarro Juanes A, Robledo Díaz L, Carvajal Roca E. ¿Es adecuada la utilización del servicio de urgencias en el periodo neonatal? Rev Pediatr Aten Primaria. 2017;19:301-9.
Publicado en Internet: 11-10-2017 - Número de visitas: 24272
Resumen
Introducción: los servicios de urgencias son frecuentados, con un elevado índice, por neonatos con patología banal y dudas de puericultura. Nuestro objetivo es analizar, en neonatos, la adecuación del uso de urgencias.
Material y métodos: análisis de los informes de los neonatos que acudieron al Servicio de Urgencias del Hospital Marina Salud de Denia (Alicante, España) durante el año 2014 y de la adecuación del uso de urgencias según los nuevos criterios establecidos: ingreso hospitalario, derivación, clasificación y exploraciones complementarias.
Resultados: los servicios de urgencias son utilizados por neonatos con patología considerada no urgente, llanto, irritabilidad o malestar (32,08%), y vómitos o regurgitaciones del recién nacido (13,21%), siendo el diagnóstico de alta más frecuente el de normalidad (20%). Según los criterios de adecuación establecidos para el uso del servicio de urgencias neonatales, el 63,50% de los motivos de consulta neonatal no fueron adecuados.
Conclusiones: la mayoría de las consultas de neonatos son catalogadas como uso no adecuado de los servicios de urgencias y deberían por tanto manejarse en Atención Primaria.
Palabras clave
● Recién nacido ● Servicios médicos de urgencia ● Uso excesivo de los servicios de saludINTRODUCCIÓN
En los últimos años se ha visto un incremento de las demandas de los servicios de urgencia1,2. Los recién nacidos constituyen un grupo poblacional con un alto índice de frecuentación y en muchos casos son consultas sobre el manejo del recién nacido o patologías banales que podría haber sido resuelta en los centros de Atención Primaria (AP)3,4.
Realizada una amplia revisión bibliográfica y detectadas las líneas de estudio que se han seguido para abordar el tema del manejo del recién nacido, se ha observado que los estudios realizados van principalmente dirigidos a describir los principales motivos por los que acuden los neonatos a los servicios de urgencias y los factores sociodemográficos asociados5. El presente trabajo de investigación tiene por tanto la intención de analizar si existe adecuación con el uso del servicio de urgencias.
El concepto médico de urgencia se define como aquella situación de enfermedad o accidente que requiere tratamiento inmediato por el riesgo vital inherente a la misma5. Esta definición se opone con la idea que tienen los padres y familiares de los enfermos pediátricos sobre la misma y excluye casi dos tercios de las urgencias atendidas.
La OMS5 describe como demanda inadecuada del servicio de urgencias toda situación que no se trate de una emergencia vital o que exija el uso de medios diagnósticos o terapéuticos no disponibles en AP.
Algunos autores6 defienden que una visita al servicio de urgencias pediátricas es clasificada como no urgente cuando no ha sido remitida por otro médico, cuando el código de clasificación en el momento de admisión sea valorado como no urgente, cuando no se requieren exploraciones complementarias en el servicio de urgencias y cuando el neonato ha sido recientemente dado de alta del hospital. Otros definen que el motivo de consulta a Urgencias es no urgente cuando retrasos en la asistencia de las mismas no incrementan el riesgo de padecer un efecto adverso y entienden por motivo de consulta inapropiado cuando se trata de visitas que, habiendo sido derivadas por otro médico o siendo espontáneas, por su gravedad o por la atención prestada se podrían haber atendido en otro nivel asistencial7.
La ansiedad familiar, la falta de confianza en el pediatra (muchos todavía no han acudido a la primera revisión), la falta de educación sanitaria de los progenitores o la incomprensión de la misma, la incompatibilidad de horario laboral con el del centro de salud o la dificultad para su acceso, la comodidad o cercanía al hospital y la facilidad para realizar pruebas complementarias son algunos de los factores que llevan al mal uso y sobresaturación del servicio de urgencias8.
Algunos autores han descrito que el alta precoz de los servicios de maternidad está relacionada con visitas al servicio de urgencias por motivos y dudas sobre nociones básicas del recién nacido, que tradicionalmente eran resueltas durante la estancia hospitalaria.
Por otro lado, se debe tener en cuenta que, al acudir al servicio de urgencias o a cualquier medio hospitalario, el recién nacido queda expuesto a infecciones dada su elevada vulnerabilidad, lo que supone un motivo de preocupación para el pediatra ya que esto impide su correcta valoración.
Dado que actualmente no existe un consenso sobre lo que se considera motivo de consulta no urgente, en este estudio establecemos, basándonos en los estudios citados anteriormente, un nuevo concepto de adecuación al servicio de urgencias en la población neonatal.
El objetivo de este estudio es analizar la adecuación del uso del servicio de urgencias de los neonatos que acudieron al Hospital Marina Salud de Denia (HMSD) (Alicante, España) durante el 2014.
MATERIAL Y MÉTODOS
Estudio transversal donde se analizó la adecuación del uso del servicio de urgencias por parte de los recién nacidos que acudieron.
El lugar de realización del estudio fue el Hospital de Denia, un hospital comarcal perteneciente al grupo AB de Conselleria de Sanidad de la Generalitat Valenciana, dotado con 266 camas y que presta asistencia a la población de la Comarca de la Marina Alta de la Comunidad Valenciana (España). Pertenece al modelo de concesión administrativa (“Modelo Alzira”). Sin embargo, dada la dotación de recursos de especialidades disponibles, IAMETRICS de IASIST lo clasifica como un hospital de tercer nivel. Desde el 14 de diciembre de 2009 está certificado por AENOR en el Sistema de Gestión de la Calidad UNE-EN-ISO 9001:2008 y está integrado en la historia clínica electrónica de Cerner Millennium®. El Servicio de Urgencias del Hospital de Denia cuenta con una sala de espera específica de Pediatría, dos consultas pediátricas y una sala de reanimación específica pediátrica. La asistencia pediátrica es inicialmente prestada por médicos de Urgencias, existiendo la disponibilidad de un pediatra consultor de guardia con presencia física las 24 horas.
El análisis de la adecuación del uso de urgencias que propiciaron estas visitas abarcó el periodo del 1 de enero del 2014 a 31 de diciembre de 2014.Se incluyeron a los recién nacidos menores de 28 días de vida que acudieron a puertas de Urgencias del HMSD.
Para la realización del análisis de la adecuación del uso del servicio de urgencias no se precisó cálculo del tamaño muestral, puesto que fueron analizados todos los recién nacidos que acudieron a dicho servicio durante el periodo establecido.
Recogida de información
Antes del inicio del estudio, se solicitó autorización para su realización a la Comisión de Investigación del Departamento de Salud de Denia mediante la “Solicitud de autorización de proyectos de investigación por la Comisión de Investigación del Departamento de Salud de Denia”, y se firmó el “Compromiso del Investigador”, aceptando que el estudio fuese tratado y controlado siguiendo lo establecido en el protocolo autorizado por la Comisión de Investigación del Departamento de Salud Denia y la legislación vigente sobre investigación biomédica y protección de datos de carácter personal. Asimismo, los datos referidos a las historias clínicas se obtuvieron a partir de la base de datos del servicio de urgencias y la revisión de la historia clínica electrónica (Cerner Millenium®) de todos los recién nacidos que acudieron durante el año 2014 al servicio.
Establecimiento de los criterios de adecuación del uso del servicio de urgencias
Basándonos en los estudios citados en la introducción, se estableció como uso no adecuado del servicio de urgencias aquellas consultas que no cumplían ninguno de los siguientes criterios de clasificación de gravedad (Tabla 1). Asumimos como uso adecuado del servicio aquellas consultas que cumplían al menos uno de dichos criterios.
| Tabla 1. Criterios de gravedad |
|---|
| I. Criterio de derivación: recién nacido remitido por Atención Primaria u otro especialista de la salud |
| II. Criterio de ingreso hospitalario: recién nacido cuya alta del servicio de urgencias se corresponde con ingreso hospitalario |
| III. Criterio de clasificación de Manchester (MTS): recién nacido clasificado con nivel ≤ 3 |
| IV. Criterio de necesidad de exploraciones complementarias: recién nacido con necesidad de realización de alguna exploración complementaria |

Dado que el HMSD no dispone del sistema de clasificación de Manchester adaptado para Pediatría, nos encontramos con que la mayoría de los recién nacidos, solo por el hecho de su edad, son estratificados por el personal de enfermería con un nivel de clasificación mayor al que les correspondería por su motivo de consulta.
Al estar incluido como criterio de gravedad el nivel de clasificación ≤ 3, y asumiendo que el nivel 1 y 2 se corresponden con situaciones de alta gravedad y por tanto uso adecuado del servicio de urgencias, nos planteamos la forma de discernir qué neonatos del nivel 3 realizaron verdaderamente un uso adecuado del servicio de urgencias. Para ello aplicamos a este grupo de niños los otros criterios de adecuación: derivación, ingreso hospitalario y necesidad de exploraciones complementarias, obteniendo de esta forma el número de neonatos que, siendo clasificados como un nivel 3, no realizaron un uso adecuado del servicio de urgencias.
El análisis de todos los datos se realizó en colaboración con el Servicio de Medicina Preventiva y Salud Pública del HMSD, con el asesoramiento del responsable del mismo. El análisis de todos los datos fue realizado mediante los paquetes estadísticos Epidat® 3.1 e Intercooled Stata® 9.1 para Windows®.
Las variables cualitativas fueron descritas mediante las correspondientes frecuencias absolutas y relativas. Las variables cuantitativas se describieron con media y desviación estándar, o con mediana y rango intercuartílico en caso de distribución significativamente distinta a una normal (test de Kurtosis y asimetría, p valor menor de 0,05). Se añadieron para el análisis gráfico diagramas de barras y sectores para las variables cualitativas e histogramas para las variables cuantitativas.
RESULTADOS
Análisis general de los datos recogidos en las historias clínicas
Durante el periodo de estudio se atendieron en el Servicio de Urgencias del HMSD un total de 8893 de consultas pediátricas de edades comprendidas entre 0 a 15 años, de las cuales correspondieron a pacientes entre 0 y 12 meses de edad un total de 1382 (15,54%) y entre 0 y 30 días de vida un total de 228, es decir, un 16,49% de los menores de 12 meses y un 2,56% del total de urgencias pediátricas. Del grupo de pacientes menores de un mes, correspondieron a neonatos un total de 167 (12,08% del total de menores de un año).
Atendiendo a la edad del neonato según sus días de vida, observamos que la distribución de aquellos que acudieron al servicio de urgencias no siguió una normal (test de Kurtosis y asimetría, p < 0,0001).
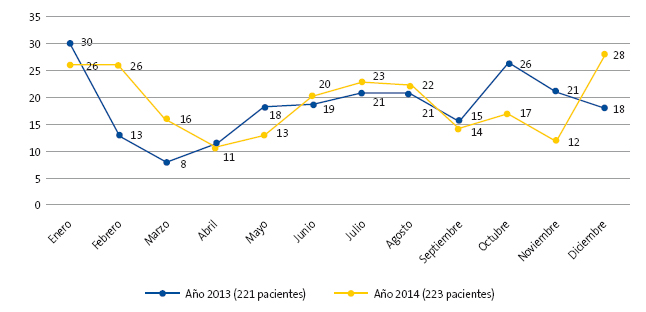
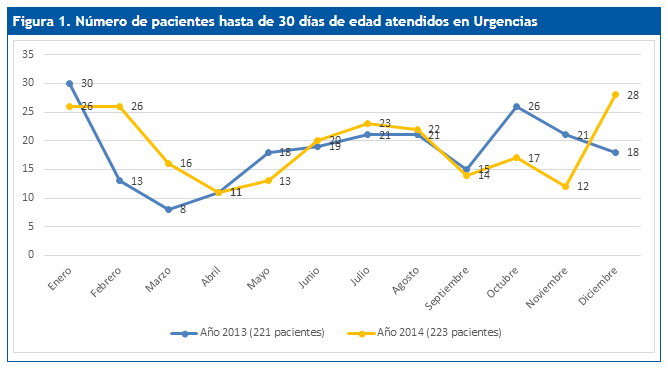
La distribución de las consultas por periodos estacionales fue el 17,96% en primavera, con un 20% de ingresos; el 28,74% en verano, con un 12,50% de ingresos; en otoño el 19,76%, con un 21,20% de ingresos, y en invierno el 33,76%, con un porcentaje de ingresos del 33,90% (Fig. 1).
| Figura 1. Número de pacientes hasta de 30 días de edad atendidos en urgencias |
|---|
 |
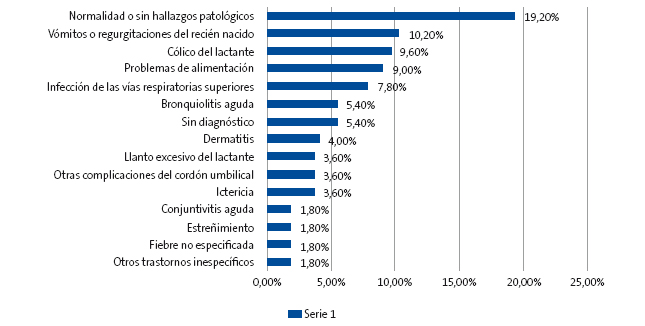
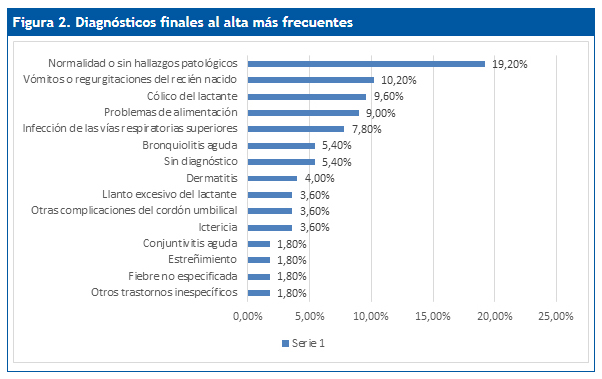
En cuanto a los diagnósticos finales al alta, codificados según el CIE.9, destacaron entre los más frecuentes: el 19,20%, normalidad o sin hallazgos patológicos; el 10,20%, vómitos o regurgitaciones del recién nacido; el 9,60%, cólico del lactante; el 9%, problemas de alimentación; el 7,8%, infección de vías respiratorias superiores, y se detectó un 5,4% con código CIE sin diagnóstico (Fig. 2).
| Figura 2. Diagnósticos finales al alta más frecuentes |
|---|
 |
Análisis de la adecuación según los criterios de gravedad establecidos
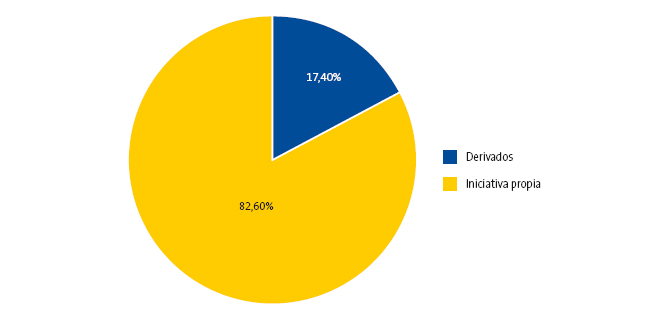
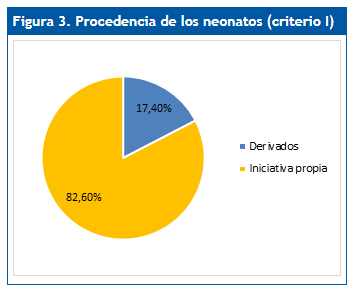
Criterio I (derivación): el 17,36% (n = 29) acudió por derivación otro centro o especialista y el 82,64% de los neonatos (n = 138) acudió por iniciativa de sus progenitores (Fig. 3).
| Figura 3. Procedencia de los neonatos (criterio I) |
|---|
 |
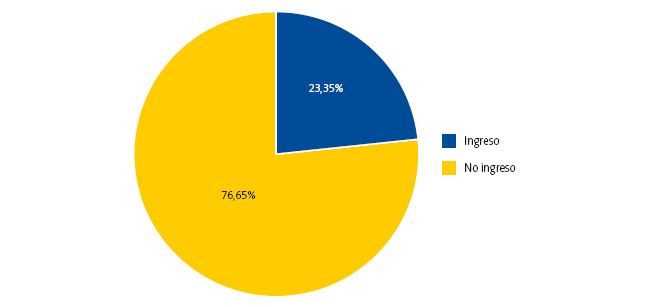
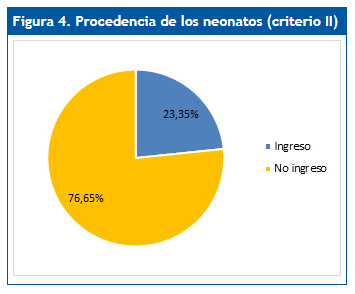
Criterio II (ingreso hospitalario): un 23,4% (n = 39) de los neonatos atendidos en el servicio de urgencias requirió ingreso. El 76,65% (n = 128) fue dado de alta con destino a su domicilio tras la valoración en el servicio de urgencias (Fig. 4).
| Figura 4. Procedencia de los neonatos (criterio II) |
|---|
 |
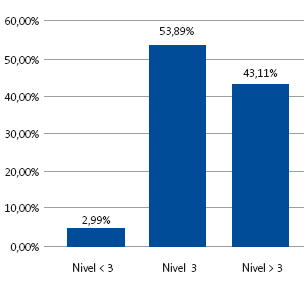
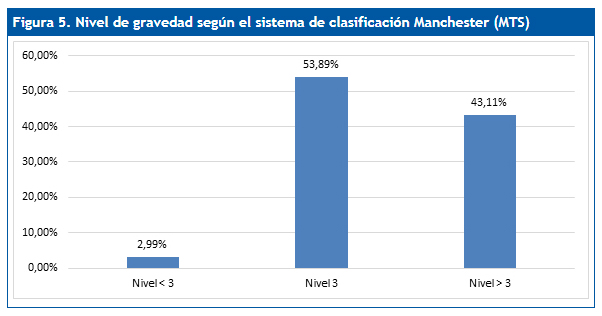
Criterio III (nivel de clasificación según el sistema de clasificación de Manchester [MTS]): encontramos un 3% (n = 5) de neonatos con clasificación de nivel inferior a 3 (1-2), el 53,9% (n = 90) presentó una clasificación de nivel 3, mientras que el 43,1% (n = 72) obtuvo una clasificación de nivel superior a 3 (4-5) (Fig. 5).
| Figura 5. Nivel de gravedad según el sistema de clasificación Manchester (MTS) |
|---|
 |
En referencia a los análisis estadísticos realizados para excluir a los neonatos asignados al nivel 3 exclusivamente por el factor edad, detallamos los siguientes resultados: dentro de los neonatos asignados a con un nivel 3 de clasificación, el 28,9% (26 neonatos) requirió ingreso hospitalario, el 14,4% (n = 13) fue derivado por AP, otro centro u otro especialista de la salud, mientras que el 85,6% acudió por iniciativa de sus progenitores (77 neonatos).
Entre los neonatos clasificados dentro del nivel 3 de clasificación (MTS), un 96,67% no requirió exploraciones complementarias, observándose que ninguno de los que no fueron derivados ni ingresados tras su valoración en el servicio de urgencias requirió las mismas.
Por tanto, de los tres criterios analizados, el 33,5% (n = 56) de los neonatos cumplía al menos uno de ellos: hospitalizado, derivado o caso nivel de clasificación de Manchester menor o igual a 3. Aquellos que cumplían más de un criterio de gravedad fueron contabilizados de manera individual.
En total, un 36,66% (n = 33) de los 90 neonatos incluidos en el nivel 3 habían acudido a Urgencias por derivación o requirieron ingreso hospitalario como resultado de la consulta al servicio de urgencias.
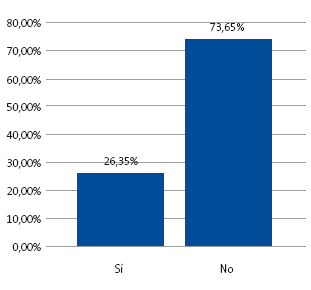
Criterio IV (exploraciones complementarias): el 73,65% (n = 123) de los neonatos no precisó exploraciones complementarias y el 26,35% (n = 44) sí precisó las mismas (Fig. 6).
| Figura 6. Exploraciones complementarias (criterio IV) |
|---|
 |

De los 44 neonatos que requirieron pruebas complementarias, el 11,36% (n = 5) no estaban incluidos en los criterios anteriores (derivado, ingresado o nivel de clasificación menor o igual a 3), uniéndose al 33,5% (n = 56) que sí los cumplían.
En total se añaden a los 56 neonatos que hicieron un uso adecuado del servicio de urgencias (hospitalización/derivado/grave) cinco neonatos que, no cumpliendo los criterios anteriores, sí precisaron alguna exploración complementaria.
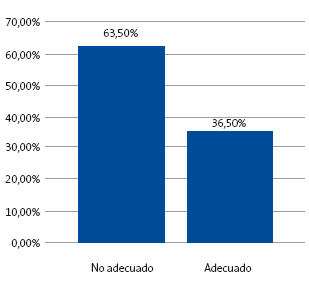
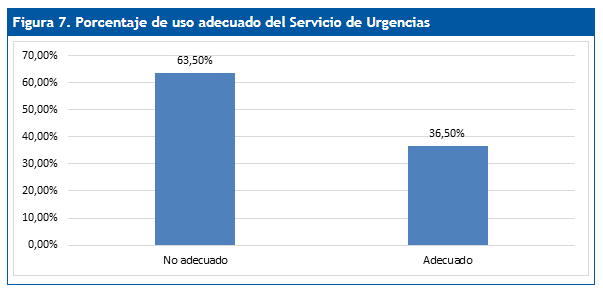
Por tanto, de los 167 neonatos analizados, el 36,5% (n = 61) se clasificó como un uso adecuado del servicio de urgencias, mientras que el 63,50% (n = 106) se catalogó como uso no adecuado del mismo (Fig. 7).
| Figura 7. Porcentaje de uso adecuado del servicio de urgencias |
|---|
 |
Atendiendo a la edad, no se observan diferencias significativas en proporción del uso adecuado por quincena de edad (χ2, p = 0,713). El 65% de los neonatos que acudieron en los primeros 14 días de vida hizo un uso no adecuado del mismo, así como el 62% de los que acudieron en los segundos 14 días de vida.
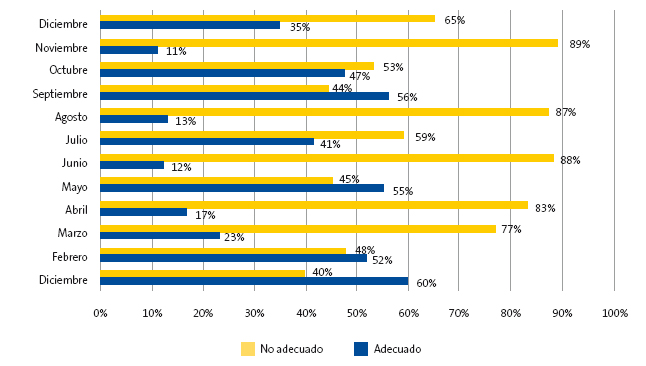
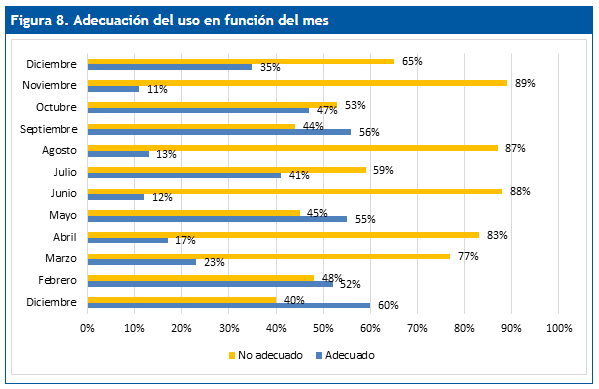
En función del mes en que acudieron, se observan variaciones significativas en la proporción de uso adecuado (test exacto de Fisher, p = 0,024) (Fig. 8).
| Figura 8. Adecuación del uso en función del mes |
|---|
 |
DISCUSIÓN Y CONCLUSIONES
El aumento del número de visitas a Urgencias se ha visto incrementado en los últimos años1,2 a pesar de las mejoras sanitarias a nivel de AP, manteniéndose una excesiva demanda hospitalaria entre los recién nacidos. Las causas que motivan estas visitas son muy variadas y continúan siendo objeto de estudio para todos aquellos que se dedican al abordaje de esta problemática6,9.
En el servicio de urgencias del HMSD, entre los pacientes pediátricos que atiende, considerados estos hasta los 14 años de edad y con unas cifras totales durante el año 2014 de 8893 de urgencias pediátricas, los recién nacidos suponen cuantitativamente una pequeña proporción (2,56%). Sin embargo, este grupo de edad presenta una serie de peculiaridades que lo diferencia del resto de pacientes pediátricos, consecuencia de la gran ansiedad que generan entre su familia ante cualquier síntoma.
Gran parte de los trabajos3,9,10 publicados concluyen que los neonatos acuden al servicio de urgencias por procesos habitualmente banales que podrían haberse evitado con unos conocimientos básicos de puericultura y/o manejo del recién nacido.
Al analizar los diagnósticos de alta de las historias clínicas, observamos que el diagnóstico más frecuente, con casi un 20% del total de consultas realizadas, es el de normalidad, es decir, ausencia de patología. Se observó una alta frecuencia también en los diagnósticos de vómitos o regurgitaciones del recién nacido, cólico del lactante y problemas de alimentación. Es decir, la mayoría de diagnósticos clínicos al alta podrían considerarse dentro de la patología banal del recién nacido, así como dentro los conceptos de puericultura. Esto coincide con los datos aportados por la mayoría de estudios realizados sobre las visitas de neonatos a los Servicios de Urgencias, planteando una nueva línea de investigación que analice la posible relación y concordancia entre los motivos de consulta y los diagnósticos finales al alta.
En los resultados de nuestro estudio, un alto porcentaje (82,64%) de los recién nacidos que acudieron al servicio de urgencias lo hicieron por iniciativa de sus progenitores, sin haber sido derivados por ningún centro de AP u otro especialista, siendo muy bajo el porcentaje de estos los que requirieron ingreso hospitalario, tan solo un 19,56%. Se observa que la gran mayoría de consultas realizadas por iniciativa de los progenitores de los recién nacidos al servicio de urgencias tienen como resultado de la valoración un destino domiciliario, por lo que probablemente sus motivos de consulta podrían haber sido resultas en otros centros de atención.
Acorde a nuestro estudio, varias publicaciones coinciden9 en que los neonatos que son derivados requieren con mayor frecuencia ingreso comparado con aquellos que acuden a Urgencias por iniciativa de sus progenitores. Sin embargo, algunos autores11 discrepan en esta asociación, probablemente debido a la falta de conocimiento sobre el neonato que tienen algunos pediatras u otros médicos que los atienden en determinados servicios de AP, derivándolos, en consecuencia, por motivos que no requieren atención hospitalaria.
A diferencia de algunos autores9 que afirman que no existe una frecuentación menor del servicio de urgencias por parte de los neonatos durante los meses de verano, en este estudio se detectó el mayor porcentaje de visitas (87,97%) en dichos meses, lo cual podría ser atribuido a la ubicación del HMSD en un área vacacional. Sin embargo, solo un 12,50% de las consultas realizadas durante estos meses requirió ingreso hospitalario. Esta mayor frecuentación en los meses de verano podría ser justificada por la necesidad de resolver los problemas habituales que pueden aparecer en los recién nacidos durante los primeros días de vida y no disponer de su pediatra de confianza o centro de AP conocido.
Dado que actualmente no existe un consenso sobre cuál es el concepto de uso adecuado de los servicios de urgencias, este estudio ha establecido el concepto de adecuación de su uso en base a diferentes criterios, como son la necesidad de ingreso hospitalario, la procedencia del neonato (derivación), el nivel de gravedad establecido según el sistema de clasificación de Manchester y la necesidad de exploraciones complementarias.
Según los criterios establecidos para definir la adecuación del servicio de urgencias, podemos afirmar que, de todos los neonatos que acudieron al servicio de urgencias, tan solo el 36,5% (n = 61) hizo un uso adecuado de dicho servicio, el 63,5% (n = 116), es decir, más de la mitad de las visitas de los neonatos a Urgencias, se consideró un uso no adecuado y los diagnósticos más frecuentes al alta fueron el de recién nacido normal o sin alteraciones patológicas.
Confirmamos que los servicios de urgencias son utilizados frecuentemente por patología considerada como no urgente y por dudas de puericultura, que deberían ser manejada de forma más adecuada en los niveles de AP sin necesidad de acudir al servicio de urgencias. Opinamos que, de esta forma se evitarían retrasos en los tiempos de asistencia de los servicios de urgencias hospitalarias, al ser considerado el neonato como población de riesgo, y que podrían ser dedicados a los casos urgentes.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
AP: Atención Primaria • CIE: Clasificación Internacional de Enfermedades • HMSD: Hospital Marina Salud de Denia • MTS: sistema de clasificación de Manchester • OMS: Organización Mundial de la Salud.
BIBLIOGRAFÍA
- Millar K, Gloor J, Wellington N, Joubert G. Early neonatal presentations to the pediatric emergency department. Pediatr Emerg Care. 2000;16:145-50.
- Pérez Sánchez A, Begara de la Fuente M, Núñez Fuster J, Navarro González J. Consultas reiterativas en la urgencia hospitalaria pediátrica. An Esp Pediat. 1996:44:321-5.
- Ruiz L, Ruggeri N. Urgencias de recién nacidos en hospital pediátrico. X Reunión Anual de la Sociedad Española de Urgencias de Pediatría (IV). An Pediatr (Barc). 2006;65:278-300.
- Chimeti Camacho P, Iglesias Fernández C, Marsinyach Ros I, Crespo Medina M, Mínguez Navarro C, Marañón Pardillo R. Uso del servicio de urgencias por los menores de un mes de vida. X Reunión Anual de la Sociedad Española de Urgencias de Pediatría (IV). An Pediatr (Barc). 2006;65:278-300.
- Lapeña López de Armentia S, Reguero Celada S, García Rabanal M, Gutiérrez Fernández M, Abdallah I, González Aparicio H. Estudio epidemiológico de las urgencias pediátricas en un hospital general. Factores implicados en una demanda inadecuada. An Esp Pediatr. 1996;44:121-5.
- Kennedy TJT, Purcell LK, LeBlanc JC, Jangaard KA. Emergency Department use by infants less than 14 days of age. Pediatr Emer Care. 2004;20:437-42.
- Flanagan CF, Stewart M. Factors associated with early neonatal attendance to a paediatric emergency department. Arch Dis Child. 2014;99:239-43.
- Uscher-Pines L, Pines J, Kellermann A, Gillen E, Mehrotra A. Deciding to visit the Emergency Department for nonurgent conditions: a systematic review of the literature. Am J Manag Care. 2013;19:47-59.
- Sharma V, Simon S, Bakewell J, Ellerbeck E, Fox M, Wallace D. Factors influencing infant visits to Emergency Departments. Pediatrics. 2000;106:1031-9.
- Pérez Solís D, Pardo de la Vega R, Fernández González N, Ibáñez Fernández A, Prieto Espuñes S, Fanjul Fernández JL. Atención a neonatos en una unidad de urgencias pediátricas. An Pediatr (Barc). 2003;59:54-8.
- Fernández Ruiz C, Trenchs Sainz de la Maza V, Curcoy Barcenilla AI, Lasuen del Olmo N, Luaces Cubells C. Asistencia a neonatos en el servicio de urgencias de un hospital pediátrico terciario. An Pediatr (Barc). 2006;65:123-8.
- Assandri Dávila E, Ferreira García MI, Bello Pedrosa O, de Leonardis Capelo D. Hospitalización neonatal desde el servicio de urgencias en un centro hospitalario de Uruguay. An Pediatr (Barc). 2005;63:413-7.