
Vol. 19 - Num. 75
Originales
Factores asociados a sobrepeso y obesidad en estudiantes de educación secundaria
Juana Aurelia Ninatanta Ortiza, Luz Amparo Núñez Zambranoa, Segunda Aydeé García Floresa, Romaní Romaní Romaníb
aEnfermera. Facultad Ciencias de la Salud. Universidad Nacional de Cajamarca. Perú.
bMédico. Oficina General de Investigación y Transferencia Tecnológica. Instituto Nacional de Salud. Perú.
Cómo citar este artículo: Ninatanta Ortiz JA, Núñez Zambrano LA, García Flores SA, Romaní Romaní F. Factores asociados a sobrepeso y obesidad en estudiantes de educación secundaria. Rev Pediatr Aten Primaria. 2017;19:209-21.
Publicado en Internet: 11-09-2017 - Número de visitas: 29125
Resumen
Objetivos: identificar los factores asociados al sobrepeso y obesidad en estudiantes de educación secundaria de una región andina del norte del Perú.
Material y métodos: se realizó un estudio transversal en una muestra de 586 participantes procedentes de dos distritos de la región de Cajamarca (Perú). Realizamos la evaluación antropométrica según los estándares de crecimiento infantil de la Organización Mundial de Salud (se clasificó según puntuación z del índice de masa corporal). Se recolectó mediante un cuestionario estructurado información sobre los estilos de vida, consumo de alimentos, actividad física, síntomas depresivos, acoso escolar y percepción del peso. Se realizó un análisis de regresión logística multivariado para identificar las características asociadas.
Resultados: la proporción de sobrepeso y obesidad fue de 22,9% y 6,8% de adolescentes, respectivamente. El pertenecer a escuelas públicas resultó un factor protector para sobrepeso (odds ratio ajustada: 0,62; intervalo de confianza del 95%: 0,39 a 0,99) independientemente del género, actividad física y síntomas depresivos. El género masculino (odds ratio ajustada: 2,05; intervalo de confianza del 95%: 1,02 a 4,11) y la baja actividad física (odds ratio ajustada: 4,14; intervalo de confianza del 95%: 1,65 a 10,35) fueron factores de riesgo para obesidad, mientras que pertenecer a escuelas públicas fue factor protector (odds ratio ajustada: 0,43; intervalo de confianza del 95%: 0,20 a 0,92).
Conclusiones: el nivel de actividad física es el principal factor asociado con obesidad, por otro lado, los estudiantes de escuelas públicas presentan menor probabilidad de sobrepeso y obesidad. Las escuelas representan entornos para implementar intervenciones de prevención de exceso de peso basadas en el incremento de la actividad física.
Palabras clave
● Adolescente ● Estudiantes ● Obesidad ● SobrepesoINTRODUCCIÓN
La obesidad es un problema de salud creciente a nivel mundial; se estima que en 2025 afectará al 18% de varones y al 21% de mujeres1. El exceso de peso en adolescentes también es un problema de salud pública2. En Latinoamérica, la magnitud del sobrepeso y la obesidad varía según país, el 40,9 y el 22,9% de adolescentes de México (año 2002) presentaron sobrepeso y obesidad, respectivamente3, en Brasil entre el 25,7 y el 28,8% presentaron sobrepeso, y entre el 10,4 y el 15,4% obesidad4; y en adolescentes de Argentina (2014) se encontró un 26,4% de sobrepeso y un 14,1% de obesidad5. En niños y adolescentes de EE. UU. (2013-2014) la prevalencia de sobrepeso fue del 33,4% y de obesidad del 26,1%6.
En el Perú, se ha incrementado la prevalencia del exceso de peso en adolescentes; según el Instituto Nacional de Salud (INS), el sobrepeso en adolescentes de 10 a 19 años se incrementó del 15,8% (año 2011) al 18,5% (2014), mientras que la obesidad se incrementó del 4,6 al 7,5%. El exceso de peso no se encuentra uniformemente distribuido: en áreas urbanas se encuentra el doble de sobrepeso que en las áreas rurales, mientras que la obesidad es siete veces más frecuente7. Existen distritos con alta prevalencia de exceso de peso distribuidos principalmente en la costa de Perú8. En 2014, en la región andina norte, la prevalencia de sobrepeso y obesidad fue del 16,1 y el 2,1% respectivamente, existiendo una tendencia creciente, pues en 2011 el sobrepeso afectó a un 9,3% y la obesidad a un 1,8% de los adolescentes de dicha región7. La identificación de factores de riesgo modificables permitiría explicar esta tendencia en zonas andinas. En 2015, la población de adolescentes (de 12 a 17 años) en la región de Cajamarca ascendía a 184 167 habitantes, siendo la región andina peruana con mayor población adolescente9. En dicha región, el exceso de peso se inicia e incrementa a partir de la infancia: en 2014, en menores de cinco años, la prevalencia de sobrepeso y obesidad fue del 5,3 y el 1,5% respectivamente8, mientras que en adolescentes se incrementa al rango de 10-20%10.
Estudios transversales en escolares de secundaria provenientes de diversas regiones del Perú han encontrado prevalencias de exceso de peso, que oscilan entre el 6,8 y el 33,7%, dependiendo del género y la región7-12. También se han realizado estudios que han explorado las características asociadas al sobrepeso y la obesidad; un estudio de fuentes secundarias encontró como factores asociados en adolescentes (de 10 a 19 años) el menor nivel educativo del cabeza de familia, la pobreza, ser mujer y vivir en áreas urbanas10. Otro estudio en escolares de 6 a 17 años encontró como características asociadas al exceso de peso el vivir en la costa y tener una baja aptitud respiratoria13. En 2007, en escolares de educación primaria en Lima Metropolitana y Callao, se encontró que en escuelas privadas el porcentaje de sobrepeso era mayor que en las públicas (del 21,6 frente al 10,3%)14. A nivel internacional, se ha encontrado que el exceso de peso podría explicarse por factores de riesgo diferentes al estado físico y el hábito alimentario; hay estudios que han encontrado asociación con sintomatología depresiva15,16, acoso escolar17-19 y percepción de la imagen corporal20,21.
La reducción de la prevalencia del sobrepeso y la obesidad en la infancia y adolescencia debería reducir la magnitud de la obesidad y su morbilidad en etapas posteriores de la vida. Los niños obesos tienen más de cinco veces la probabilidad de ser obesos en la adultez comparados con aquellos niños no obesos2. También se ha observado que el haber presentado obesidad durante la adolescencia está fuertemente asociado con el incremento de la mortalidad durante la adultez por enfermedad cardiaca coronaria y por accidente cerebrovascular22. Frente a dichas evidencias, la reducción del exceso de peso en la adolescencia contribuiría a la disminución de la obesidad y su morbilidad en la adultez. El presente estudio busca determinar la proporción de sobrepeso y obesidad en una muestra de escolares de educación secundaria residentes en una región andina de Perú, así como identificar factores de riesgo modificables asociados, con la finalidad de poder implementar estrategias de promoción de la salud en instituciones educativas de zonas urbanas de Los Andes.
MATERIAL Y MÉTODOS
Diseño y población de estudio
La región de Cajamarca está ubicada en la zona norte de Los Andes de Perú. El estudio fue realizado en los distritos de Chota y Cajamarca. Cajamarca está ubicado en la provincia del mismo nombre, cuenta con 246 536 habitantes (población estimada en 2015), mientras que el de Chota cuenta con 48 698 habitantes (2015) (Series Nacionales INEI).
La muestra estuvo conformada por 586 escolares de educación secundaria del primer y segundo año de cuatro escuelas del área urbana de los distritos seleccionados que participaron en el “Estudio prevalencia de síndrome metabólico en estudiantes de secundaria, universitarios y madres residentes de una región andina del Perú”23. Dicho estudio fue realizado entre junio y octubre del 2014. El tamaño muestral del estudio original fue calculado considerando una prevalencia de síndrome metabólico del 19,1%, un nivel de confianza del 95% y un margen de error relativo del 15%.
Medición de variables
- Evaluación antropométrica. El sobrepeso y obesidad se definieron según los estándares de crecimiento infantil de la Organización Mundial de la Salud (OMS) de 2007 para mayores de cinco años. Se clasificó según puntuación z del índice de masa corporal (IMC) para la edad (ZIMC) usando la macro para SPSS® de la OMS (who.int/childgrowth/software/es/). Se consideró como sobrepeso si ZIMC > +1 y ≤ +2 y obesidad si ZIMC > +224.
- Estilos de vida. Mediante un cuestionario estructurado se recolectó información sobre hábitos nocivos: consumo de cigarrillos alguna vez en la vida (Sí/No) y consumo de bebidas alcohólicas alguna vez en la vida (Sí/No). El hábito alimentario se exploró mediante la frecuencia semanal de consumo de los siguientes de alimentos (número de días/semana): bebidas gaseosas, aperitivos, agua, frutas, verduras, lácteos (leche/yogur), huevos, carne de pollo, carnes rojas, pescado y embutidos. Se categorizó el consumo de fruta y verdura en adecuado (Sí/No) para consumos de dichos alimentos de cuatro a siete días/semana, se consideró como consumo adecuado de agua ocho o más vasos de agua por día (Sí/No). La actividad física se midió usando el Cuestionario Internacional de Actividad Física (IPAQ) en su versión corta, sus criterios se usaron para definir los niveles bajo, moderado y alto, para el análisis bivariado y multivariado se recategorizó en baja y moderada/alta25. Se consideró como descanso óptimo dormir de siete a ocho horas por noche (Sí/No).
- Síntomas depresivos. Se aplicó la escala de Zung adaptada para adolescentes26, se categorizó la puntuación obtenida en normal (puntuación ˂ 50), depresión leve (50-59), depresión moderada (60-69) y severa (≥ 70). Para el análisis bivariado y multivariado se recategorizó en normal, depresión leve y depresión moderada/severa.
- Acoso escolar. Para identificar casos de victimización y agresividad escolar se plantearon 14 tipos de situaciones siguiendo la metodología de la Comisión Nacional para el Desarrollo y Vida sin Drogas (DEVIDA)27. Las situaciones fueron:
- Alguien te amenazó con algún arma, alguien te pegó, alguien escondió tus cosas, alguien rompió tus cosas y alguien robó alguna de tus cosas fueron clasificadas como tipos de violencia física.
- Fueron consideradas como violencia verbal las siguientes situaciones: alguien te insultó, alguien te puso apodos o “chapas” y alguien habló mal de ti.
- Fueron consideradas como exclusión social las siguientes situaciones: te ignoraron/no te hicieron caso, no te dejaron participar y alguien te discriminó.
- Dentro de formas mixtas se consideró: alguien te amenazó para inspirar miedo, alguien te chantajeó/te han obligado a hacer cosas que no quieres y alguien te acosó sexualmente.
- Para identificar casos de agresividad escolar, se planteó la pregunta “¿En lo que va de tus estudios secundarios, has hecho o participado en alguna de las siguientes situaciones?” para las 14 situaciones previas. Las respuestas para cada situación fueron Sí/No. Se otorgó un puntaje de “1” a la respuesta afirmativa y “0” a la respuesta negativa. Se consideró como víctima o agresor a aquellos con puntaje ≥
- Percepción de la imagen corporal. Se planteó la pregunta “¿Para su edad considera que su peso es…?”. Las categorías planteadas fueron bajo, normal y exceso de peso.
Recolección de datos
Se aplicó un cuestionario estructurado sobre los datos sociodemográficos, los antecedentes patológicos familiares, las prácticas saludables (hábitos alimentarios y actividad física), hábitos nocivos, síntomas depresivos, acoso escolar y percepción de la imagen corporal. La antropometría (peso, talla) fue realizada por personal de salud certificado por el Centro Nacional de Alimentación y Nutrición del INS, según las guías técnicas nacionales de valoración nutricional antropométrica28.
Análisis estadístico
Se estimó la prevalencia puntual del exceso de peso (sobrepeso y obesidad) y con intervalo de confianza del 95% (IC 95:. Se realizó el análisis descriptivo (frecuencias y porcentajes) de las características sociodemográficas, estilos de vida, síntomas depresivos, acoso escolar y percepción de la imagen corporal. Se comparó la proporción de estilo de vida según género usando la prueba χ2. Se comparó mediante diagramas de caja el número de días de consumo de alimentos según género. Se realizó el análisis bivariado mediante la comparación de proporciones mediante χ2 o exacta de Fisher para identificar características asociadas al estado nutricional. Se elaboró un modelo multivariado de regresión logística, en el cual se ingresaron las variables estadísticamente asociadas al estado nutricional en el análisis bivariado. Se incluyeron en el modelo las variables “consumo adecuado de agua” y “sueño óptimo”; luego que el análisis estratificado mostró que son variables confusoras en la asociación tipo de colegio y estado nutricional. Se emplearon los programas estadísticos Epi-Dat® 3.1 y SPSS® versión 22 para Windows (2013, EE. UU. SPSS Inc).
Aspectos éticos
El protocolo de investigación del estudio original fue aprobado por el Comité de Ética en Investigación del Instituto Nacional de Salud. Todos los participantes fueron informados de los objetivos del estudio, los procedimientos se aplicaron previo consentimiento/asentimiento informado escrito.
RESULTADOS
Características generales
La edad media fue de 12,74 ± 0,94 años, la mediana fue de 13 años (intervalo intercuartil: 12-13). El 48,0% (n = 281) fueron del género masculino. No se encontraron diferencias significativas entre las medias de edad según género (12,68 ± 0,92 años en varones frente a 12,78 ± 0,95 en mujeres, p = 0,19). El 78,3% (n = 459) proceden de escuelas públicas. El 7,2% (n = 42) reporta familiares con antecedente de diabetes mellitus, el 13,7% (n = 80) reporta antecedentes familiares de hipertensión arterial (HTA), el 3,1% (n = 18) reporta antecedente familiar de cáncer y el 2,6% (n = 15) reporta antecedente de accidente cardiovascular (ACV).
Estilos de vida
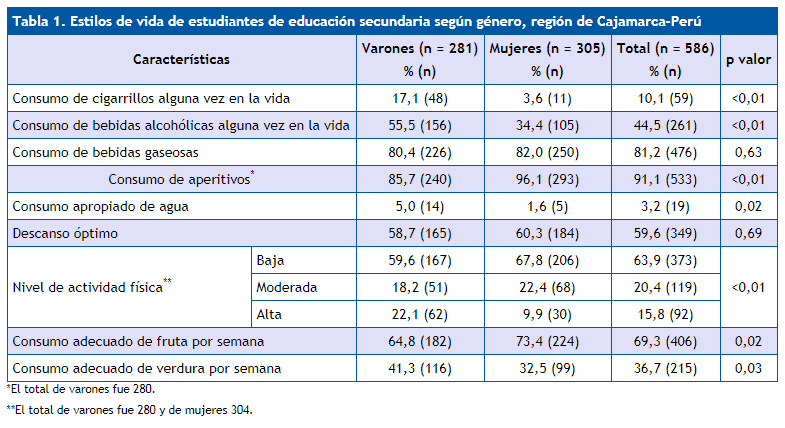
En la Tabla 1 se detallan los resultados de la encuesta sobre estilos de vida en la muestra.
| Tabla 1. Estilos de vida de estudiantes de educación secundaria según género, región de Cajamarca-Perú | |||||
|---|---|---|---|---|---|
| Características | Varones (n = 281)
% (n) |
Mujeres (n = 305)
% (n) |
Total (n = 586)
% (n) |
p valor | |
| Consumo de cigarrillos alguna vez en la vida | 17,1 (48) | 3,6 (11) | 10,1 (59) | <0,01 | |
| Consumo de bebidas alcohólicas alguna vez en la vida | 55,5 (156) | 34,4 (105) | 44,5 (261) | <0,01 | |
| Consumo de bebidas gaseosas | 80,4 (226) | 82,0 (250) | 81,2 (476) | 0,63 | |
| Consumo de aperitivos* | 85,7 (240) | 96,1 (293) | 91,1 (533) | <0,01 | |
| Consumo apropiado de agua | 5,0 (14) | 1,6 (5) | 3,2 (19) | 0,02 | |
| Descanso óptimo | 58,7 (165) | 60,3 (184) | 59,6 (349) | 0,69 | |
| Nivel de actividad física** | Baja | 59,6 (167) | 67,8 (206) | 63,9 (373) | <0,01 |
| Moderada | 18,2 (51) | 22,4 (68) | 20,4 (119) | ||
| Alta | 22,1 (62) | 9,9 (30) | 15,8 (92) | ||
| Consumo adecuado de fruta por semana | 64,8 (182) | 73,4 (224) | 69,3 (406) | 0,02 | |
| Consumo adecuado de verdura por semana | 41,3 (116) | 32,5 (99) | 36,7 (215) | 0,03 | |
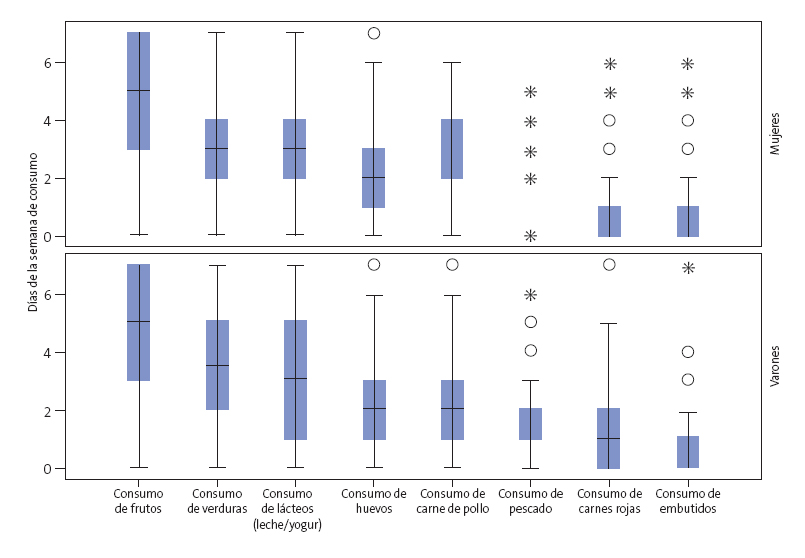
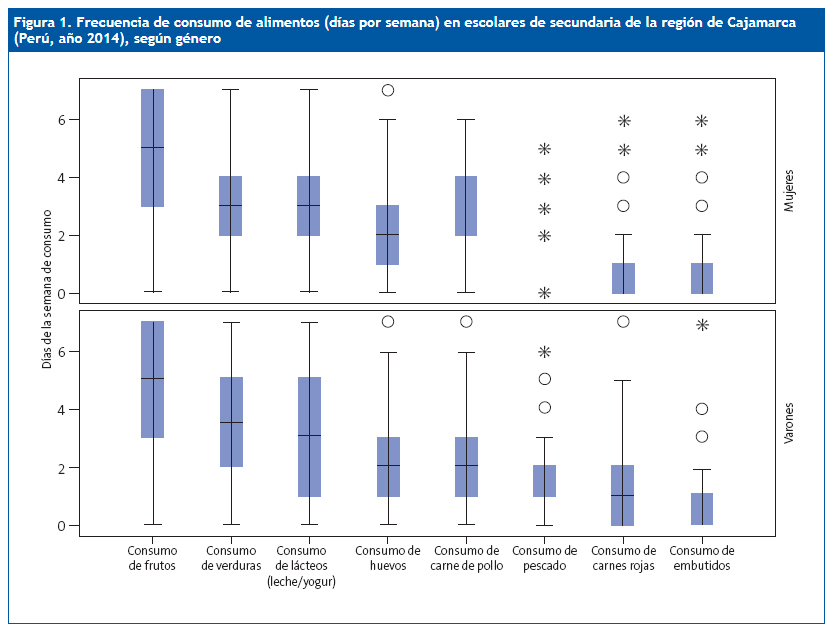
Respecto a la frecuencia de consumo por semana de determinados de alimentos, se observa en ambos géneros que las frutas, verduras, lácteos y huevos son los más comúnmente consumidos (Fig. 1). Entre los alimentos menos consumidos, el 11,0% (31/281) de varones y el 18,4% (56/305) de mujeres refiere no consumir pescado durante la semana, mientras que el 52,7% (148/281) de varones y el 59,7% (182/305) de mujeres refiere consumirlo un día a la semana. Las carnes rojas no son consumidas por el 28,2% de estudiantes, siendo este porcentaje mayor en mujeres (del 30,5 frente al 25,6%); el 43,4% (122/281) de varones y el 53,4% (163/305) de mujeres refiere consumirlas solo un día por semana. En relación con los embutidos, el 63,8% de escolares refiere no consumirlos (el 60,5% de varones y el 66,9% de mujeres); el 26,0% (73/281) de varones y el 23,6% (72/305) de mujeres los consume una vez por semana, mientras que el 9,3% (26/281) de varones y el 6,2% (19/305) de mujeres los consume dos días por semana.
| Figura 1. Frecuencia de consumo de alimentos (días por semana) en escolares de secundaria de la región de Cajamarca (Perú, año 2014), según género |
|---|
 |
Síntomas depresivos
El 8,9% (52/586) de escolares presentó una puntuación correspondiente a la categoría de “ligeramente deprimido”, el 0,5% (3/586) resultó “moderadamente deprimido” y el 0,3% (2/586) resultó “gravemente deprimido”. Entre los varones, el 11% (31/281), el 0,7% (2/281) y el 0,4% (1/281) resultó con sintomatología depresiva de intensidad leve, moderada y grave; en mujeres dichas proporciones fueron del 6,9% (21/305), el 0,3% (1/305) y el 0,3% (1/305), respectivamente. No se encontró asociación estadística entre género y la presencia de síntomas depresivos (odds ratio [OR]: 1,68; IC 95: 0,97 a 2,94, p = 0,06).
Percepción de la imagen corporal
El 82,4% (483/586) de escolares considera que tiene un peso adecuado para su edad, el 9,2% (54/586) considera que presenta sobrepeso y el 0,5% (3/586) considera que es obeso. Por otro lado, un 7,8% (46/586) considera que se encuentra bajo de peso. No se encontró asociación entre la percepción de la imagen corporal con el género (p = 0,85).
Victimización y agresividad escolar
El 74,2% (435/586) de escolares reportó ser víctima de acoso escolar. Considerando el nivel de victimización, el 31,4% (184/586) reporta victimización leve, el 26,8% (157/586) moderada y el 16,0% (94/586) grave. Respecto a la proporción de agresividad, el 61,4% (360/586) reporta haber cometido actos de violencia contra sus compañeros. El 27,1% (159/586) reporta agresividad leve, el 14,2% (83/586) agresividad moderada y el 20,1% (118/586) un nivel grave. Entre los agresores, el 90% refiere ser víctima de acoso; mientras en los no agresores el 49,1% es victimizado, encontrándose asociación entre agresividad y victimización (OR: 9,32; IC 95: 6,05 a 14,36; p < 0,01). No se encontró asociación entre género con agresividad escolar (el 63,3% en varones frente al 59,7% en mujeres, p = 0,36) o victimización (el 74,7% en varones frente al 73,8% en mujeres; p = 0,79).
Prevalencia del exceso de peso
El 29,69% (IC 95: 25,91 a 33,48) (174/586) de escolares presenta exceso de peso. La prevalencia de sobrepeso es del 22,86% (IC 95: 19,38 a 26,35) (134/586) y de la obesidad es del 6,83% (IC 95: 4,69 a 8,95) (40/586). No se encontró asociación entre género y estado nutricional por antropometría (Tabla 2). En escolares de 11 años, la proporción de exceso de peso fue del 21,7%, en los de 12 años del 32,1%, en los de 13 años del 31,0%, en los de 14 años del 26,4%, en los de 15 años del 16,7%; no se encontraron casos en escolares de 16 y 17 años.
| Tabla 2. Características de estudiantes de educación secundaria según estado nutricional, región de Cajamarca (Perú) | |||||
|---|---|---|---|---|---|
| Variables | Estado nutricional | ||||
| No sobrepeso ni obesidad % (n) | Sobrepeso % (n) | Obesidad % (n) | p | ||
| Tipo de escuela | Público (459) | 72,8 | 21,1 | 6,1 | 0,044 |
| Privado (127) | 61,4 | 29,1 | 9,4 | ||
| Género | Masculino (281) | 69,8 | 21,4 | 8,9 | 0,138 |
| Femenino (305) | 70,8 | 24,3 | 4,9 | ||
| Antecedente familiar de DM | No (544) | 71,1 | 22,4 | 6,4 | 0,212 |
| Sí (42) | 59,5 | 28,6 | 11,9 | ||
| Antecedente familiar de HTA | No (506) | 70,6 | 22,9 | 6,5 | 0,763 |
| Sí (80) | 68,8 | 22,5 | 8,8 | ||
| Antecedente familiar de ACV | No (571) | 70,4 | 23,1 | 6,5 | 0,103* |
| Sí (15) | 66,7 | 13,3 | 20,0 | ||
| Consumo de cigarrillos | No (527) | 70,6 | 22,6 | 6,8 | 0,884 |
| Sí (59) | 67,8 | 25,4 | 6,8 | ||
| Consumo de alcohol | No (325) | 69,5 | 23,1 | 7,4 | 0,815 |
| Sí (261) | 71,3 | 22,6 | 6,1 | ||
| Consumo de gaseosas | No (110) | 60,9 | 30,0 | 9,1 | 0,057 |
| Sí (476) | 72,5 | 21,2 | 6,3 | ||
| Consumo de aperitivos | No (52) | 63,5 | 25,0 | 11,5 | 0,312 |
| Sí (533) | 70,9 | 22,7 | 6,4 | ||
| Consumo óptimo de agua | No (567) | 71,4 | 22,0 | 6,5 | 0,005 |
| Sí (19) | 36,8 | 47,4 | 15,8 | ||
| Horas de sueño | Riesgo (237) | 75,5 | 20,3 | 4,2 | 0,035 |
| Óptimo (349) | 66,8 | 24,6 | 8,6 | ||
| Actividad física | Baja (373) | 68,1 | 22,8 | 9,1 | 0,015 |
| Moderada / alta (211) | 73,9 | 23,2 | 2,8 | ||
| Consumo adecuado de fruta | No (180) | 68,9 | 22,8 | 8,3 | 0,625 |
| Sí (406) | 70,9 | 22,9 | 6,2 | ||
| Consumo adecuado de verdura | No (371) | 69,8 | 23,7 | 6,5 | 0,761 |
| Sí (215) | 71,2 | 21,4 | 7,4 | ||
| Imagen corporal | Bajo de peso (46) | 95,7 | 2,2 | 2,2 | <0,01 |
| Normal (483) | 74,1 | 22,2 | 3,7 | ||
| Exceso de peso (57) | 17,5 | 45,6 | 36,8 | ||
| Síntomas depresivos | Normal (519) | 71,5 | 22,5 | 6,0 | 0,018* |
| Leve (49) | 61,5 | 26,9 | 11,5 | ||
| Moderado / grave (5) | 40,0 | 20,0 | 40,0 | ||
| Agresividad escolar | No (226) | 67,3 | 23,9 | 8,8 | 0,239 |
| Sí (360) | 72,2 | 22,2 | 5,6 | ||
| Victimización escolar | No (151) | 69,5 | 21,2 | 9,3 | 0,359 |
| Sí (435) | 70,6 | 23,4 | 6,0 | ||
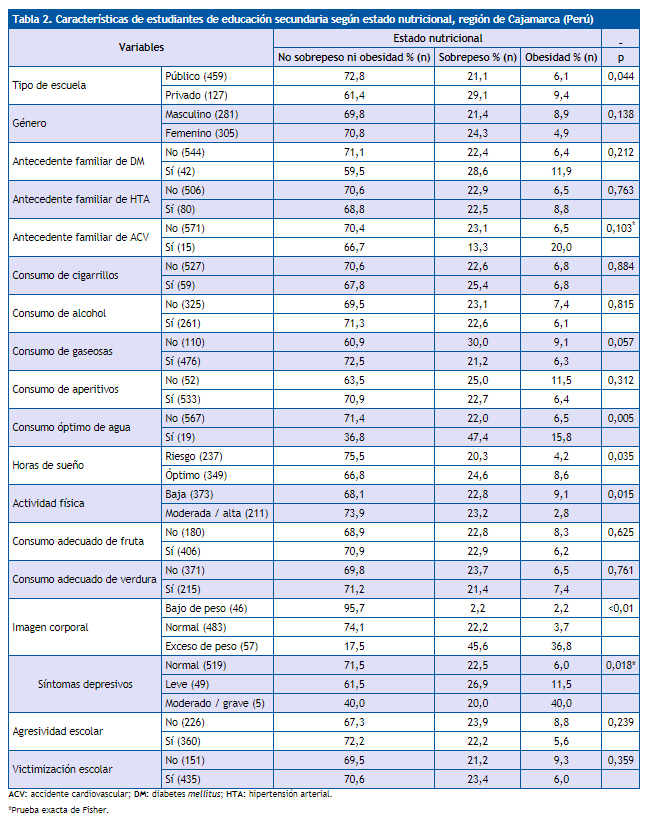
Características asociadas al exceso de peso
Se detallan en la Tabla 2. En el análisis de regresión logística multinomial se consideró como categoría de referencia “No sobrepeso/obesidad”. Se incluyeron en el modelo aquellas variables que tuvieron asociación significativa en el análisis bivariado (p ˂ 0,05). Las variables “consumo óptimo de agua” y “descanso óptimo” fueron identificadas como confusoras. En el análisis bivariado, se encontró asociación entre colegio de procedencia y exceso de peso (OR cruda: 1,67; IC 95: 1,11 a 2,53), sin embargo, se encontró que el consumo adecuado de agua resultó fuertemente asociado con pertenecer a colegios privados (OR cruda: 5,32; IC 95: 2,1 a 13,6), y también con el exceso de peso (OR cruda: 4,28; IC 95: 1,65 a 11,08). El descanso óptimo presentó un comportamiento similar, al estar asociado tanto con proceder de colegio privado (OR cruda: 1,56; IC 95: 1,03 a 2,37), como con el exceso de peso (OR cruda: 1,53; IC 95: 1,06 a 2,22).
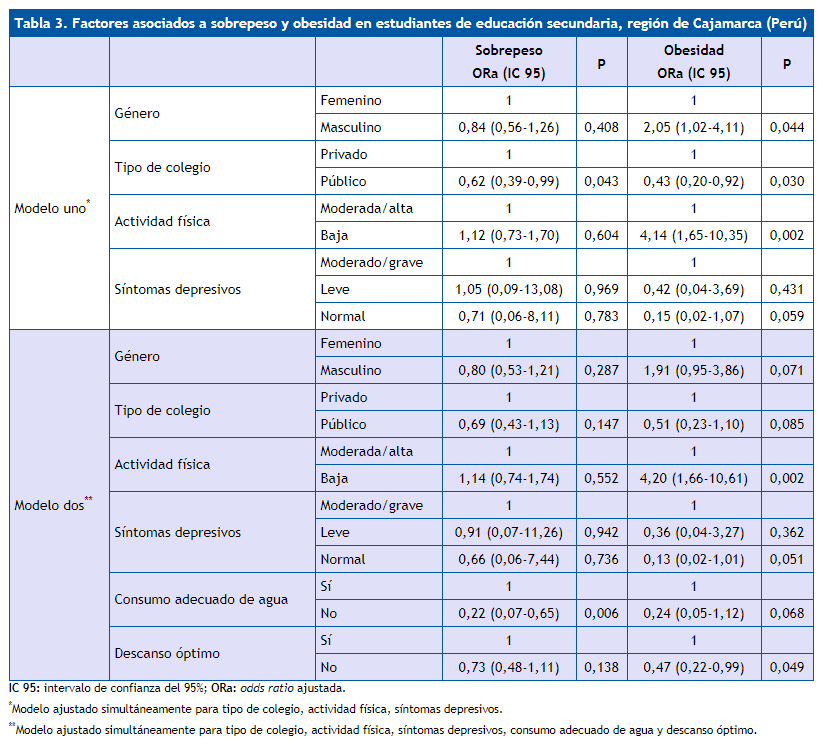
En la Tabla 3 se presentan dos modelos. En el primero, el tipo de colegio resultó independientemente asociado con sobrepeso (OR ajustada: 0,62; IC 95: 0,39 a 0,99; p = 0,043). Con respecto a la obesidad, se encontró asociación con baja actividad física (OR ajustada: 4,14; IC 95: 1,65 a 10,35; p = 0,002) y con el género masculino (OR ajustada: 2,05; IC 95: 1,02 a 4,1; p = 0,044); pertenecer a colegios públicos fue un factor protector contra la obesidad (OR ajustada: 0,43; IC 95: 0,20 a 0,92; p = 0,030). El segundo modelo incluye las variables confusoras, resultando asociadas de forma independiente como factor protector de sobrepeso el “no adecuado consumo de agua” (OR ajustada: 0,22; IC 95: 0,07 a 0,65; p = 0,06); proceder de un colegio público no resultó asociado, aunque mantiene su tendencia a comportarse como factor protector (OR ajustada: 0,69; IC 95: 0,43 a 1,13; p = 0,147). Los factores independientemente asociados a obesidad fueron el bajo nivel de actividad física (OR ajustada: 4,20; IC 95: 1,66 a 10,61; p = 0,002), y como factor protector no tener descanso óptimo (OR ajustada: 0,47; IC 95: 0,22 a 0,99; p = 0,049).
| Tabla 3. Factores asociados a sobrepeso y obesidad en estudiantes de educación secundaria, región de Cajamarca (Perú) | ||||||
|---|---|---|---|---|---|---|
| Sobrepeso
ORa (IC 95) |
p | Obesidad
ORa (IC 95) |
p | |||
| Modelo uno* | Género | Femenino | 1 | 1 | ||
| Masculino | 0,84 (0,56-1,26) | 0,408 | 2,05 (1,02-4,11) | 0,044 | ||
| Tipo de colegio | Privado | 1 | 1 | |||
| Público | 0,62 (0,39-0,99) | 0,043 | 0,43 (0,20-0,92) | 0,030 | ||
| Actividad física | Moderada/alta | 1 | 1 | |||
| Baja | 1,12 (0,73-1,70) | 0,604 | 4,14 (1,65-10,35) | 0,002 | ||
| Síntomas depresivos | Moderado/grave | 1 | 1 | |||
| Leve | 1,05 (0,09-13,08) | 0,969 | 0,42 (0,04-3,69) | 0,431 | ||
| Normal | 0,71 (0,06-8,11) | 0,783 | 0,15 (0,02-1,07) | 0,059 | ||
| Modelo dos** | Género | Femenino | 1 | 1 | ||
| Masculino | 0,80 (0,53-1,21) | 0,287 | 1,91 (0,95-3,86) | 0,071 | ||
| Tipo de colegio | Privado | 1 | 1 | |||
| Público | 0,69 (0,43-1,13) | 0,147 | 0,51 (0,23-1,10) | 0,085 | ||
| Actividad física | Moderada/alta | 1 | 1 | |||
| Baja | 1,14 (0,74-1,74) | 0,552 | 4,20 (1,66-10,61) | 0,002 | ||
| Síntomas depresivos | Moderado/grave | 1 | 1 | |||
| Leve | 0,91 (0,07-11,26) | 0,942 | 0,36 (0,04-3,27) | 0,362 | ||
| Normal | 0,66 (0,06-7,44) | 0,736 | 0,13 (0,02-1,01) | 0,051 | ||
| Consumo adecuado de agua | Sí | 1 | 1 | |||
| No | 0,22 (0,07-0,65) | 0,006 | 0,24 (0,05-1,12) | 0,068 | ||
| Descanso óptimo | Sí | 1 | 1 | |||
| No | 0,73 (0,48-1,11) | 0,138 | 0,47 (0,22-0,99) | 0,049 | ||
DISCUSIÓN
Encontramos que uno de cada tres escolares de educación secundaria de una región andina del Perú presenta exceso de peso. La proporción de sobrepeso llegó al 22,9%, mientras que la obesidad afectó al 6,8% de adolescentes. En base a nuestros resultados, en 2014 existirían en la región de Cajamarca (Perú) entre 47 000 y 62 000 adolescentes que estarían afectados por el exceso de peso. Nuestros hallazgos están en la línea de lo estimado para la región norte de los andes peruanos (año 2014), donde el sobrepeso y la obesidad afectaron respectivamente al 18,5 y 7,5% de adolescentes7. Sin embargo, se confirma la tendencia creciente de la magnitud del exceso de peso, superando el 20% reportado en el periodo 2009-2010 para dicha región10.
La magnitud encontrada es inferior a la de un distrito de Lima Metropolitana (año 2012), donde en una muestra de 1743 escolares la prevalencia de sobrepeso y obesidad fue del 33,7 y el 14,4% respectivamente12. Otros estudios realizados en Perú estiman magnitudes inferiores: en un estudio realizado en centros educativos de cuatro regiones de Perú se encontró una prevalencia de exceso de peso del 11,3%11; en 2010 en una ciudad de la sierra peruana se encontró sobrepeso en el 6,8 y el 3,6% de los varones y las mujeres, respectivamente, mientras que en ciudades de la selva, la prevalencia de sobrepeso fue del 16,6% en mujeres y del 13,7% en varones, mientras que la obesidad afectó al 2,4% de mujeres y el 2,7% de varones13.
Entre los estilos de vida más difundidos está el consumo de bebidas alcohólicas (44,5%), el alto consumo de bebidas gaseosas (81,2%) y aperitivos (91,1%). Algunos estilos de vida estuvieron asociados con el género; en varones se encontró un mayor consumo de cigarrillos, bebidas alcohólicas y verduras; además de un mayor nivel de actividad física; en mujeres se observó un mayor consumo de aperitivos y frutas. La dieta se caracteriza por el alto consumo semanal de frutas, verduras y lácteos, tanto en varones como en mujeres; los embutidos tienen baja frecuencia de consumo. La carne de mayor consumo es la de pollo, siendo menos frecuente el consumo de carne de pescado y carnes rojas. La dieta encontrada evidencia una disminución en la dieta tradicional y hecha en casa, con incremento del consumo de productos comerciales, comida rápida y comida preparada fuera del hogar. El consumo de agua es usualmente menor del recomendado, y la mayor contribución de líquidos proviene del consumo de bebidas carbonatadas y edulcoradas. Esto podría explicarse porque en el escenario de las escuelas, donde los adolescentes pasan la mayor parte del tiempo, las opciones de comidas saludables son escasas o inexistentes, proliferando alimentos de baja calidad29.
Nuestros hallazgos reportan que los adolescentes de escuelas públicas tienen una menor probabilidad de tener sobrepeso u obesidad; estos resultados se han obtenido en países desarrollados30 y en desarrollo31,32. El tipo de colegio (privado frente a público) se comportaría como una variable subrogada del nivel de ingreso de los padres: el mayor ingreso promovería que la familia consuma sus recursos monetarios en bienes y servicios que generan un mayor riesgo para el exceso de peso en el adolescente como videojuegos, comidas preparadas fuera del hogar (entre ellas la comida rápida) y un mayor consumo de dulces, aperitivos y bebidas carbonatadas.
Encontramos que los escolares varones tienen mayor probabilidad de ser obesos comparados con las mujeres, lo cual ha sido reportado en estudios en adolescentes de Puerto Rico31, Brasil32, Arabia Saudita30 y asiático-americanos de EE. UU.33. Sin embargo, las diferencias de prevalencias encontradas entre género son pequeñas, por lo que no se ha visto consistencia en la predominancia del exceso de peso entre varones o mujeres34.
Otro factor modificable independientemente asociado con la obesidad fue el bajo nivel de actividad física. Este hallazgo es consistente con la creciente evidencia que indica que la inactividad física es un factor de riesgo importante en el desarrollo de obesidad en la adolescencia35,36,37. Un metaanálisis de ensayos clínicos aleatorizados38, en el cual la intervención fue ejercicio aeróbico de cuatro o más semanas de duración en niños y adolescentes de 2 a 18 años con sobrepeso y obesidad, encontró una reducción del IMC de 1,08 kg/m2. Un estudio transversal realizado entre 2001 y 2002 en adolescentes de 10 a 16 años de 34 países encontró que el bajo nivel de actividad física y un elevado número de horas de televisión están asociados con sobrepeso, independientemente de variables relacionadas con la dieta39. Una revisión que evaluó los factores de riesgo para sobrepeso y obesidad en adolescentes de países asiáticos encontró en seis de ocho estudios que la falta de actividad física está asociada con el exceso de peso40.
Al igual que en otros estudios, no encontramos asociación del estado nutricional con factores modificables como el consumo de bebidas gaseosas, aperitivos o consumo de frutas y verduras. Un estudio en adolescentes de 11 a 16 años de Canadá no encontró un patrón consistente de asociación del exceso de peso con el consumo de frutas, verduras y aperitivos36 en niños y adolescentes de 5 a 18 años del norte de China, tampoco se encontró asociación entre sobrepeso/obesidad con el consumo de ≥ 4 días/semana de frutas frescas, vegetales, bebidas gaseosas y comidas rápidas41. Una explicación de la falta de asociación sería la mayor probabilidad de sesgo en el reporte de consumo de alimentos entre individuos con sobrepeso y obesidad comparado con aquellos con peso normal42; por otro lado, en nuestro estudio solo se obtuvo la frecuencia de consumo de alimentos, sin considerar el tamaño de la ración de comidas no saludables, que podría ser mayor en adolescentes con exceso de peso.
Encontramos que la probabilidad de sobrepeso y obesidad disminuye conforme los síntomas depresivos son leves o están ausentes. Al ser un estudio transversal, no se puede determinar la temporalidad como criterio para definir si se trata de una asociación causa-efecto. Se ha reportado en una muestra representativa de adolescentes de Canadá que ser obeso entre los 6 y los 12 años incrementa el riesgo de depresión a los 13 años16. Otro estudio examinó la asociación entre síntomas depresivos y el incremento del IMC en adolescentes de 11 a 16 años, no encontrando a los síntomas depresivos como un factor predictivo de ganancia de peso excesiva durante la adolescencia15. En nuestro estudio se encontró que la percepción de exceso de peso está asociada con tener sobrepeso y obesidad; sin embargo, en un estudio realizado en adultos y adolescentes de España, se encontró que a pesar del incremento en la prevalencia del exceso de peso entre 1987 y el 2007, los padres de niños de ambos sexos cada vez más perciben como normales a sus hijos que objetivamente tienen exceso de peso43.
En nuestro estudio no encontramos asociación entre el estado nutricional y cualquiera de las formas de acoso escolar (agresividad y victimización). Nuestros hallazgos son similares a lo reportado en adolescentes de EE. UU.18 y Finlandia20, donde tener sobrepeso u obesidad no estuvo asociado con agresividad o victimización. Sin embargo, un metaanálisis publicado en 2014 encontró que entre adolescentes con sobrepeso existe un 19% más de probabilidad de ser victimizado, mientras que en obesos la probabilidad es un 51% mayor17; incluso, en adolescentes de Italia, se encontró que la participación en el acoso escolar está en función del nivel del exceso de peso, en adolescentes varones gravemente obesos se encontró mayor probabilidad de ser victimizado y ser agresor; en el mismo estudio se encontró que los adolescentes obesos estuvieron más involucrados como agresores respecto a adolescentes con peso normal o sobrepeso19.
Los resultados del presente estudio deben ser interpretados considerando sus debilidades. La primera es que la muestra estudiada proviene de un estudio diseñado originalmente para estimar la prevalencia de síndrome metabólico: por ende, las estimaciones de sobrepeso y obesidad no pueden ser extrapolables a la población estudiada; segundo, el potencial sesgo de memoria en la medición de la actividad física, antecedentes familiares, hábitos alimentarios y victimización/agresividad escolar, lo cual podría explicar la ausencia de asociación con el exceso de peso; por último, el diseño transversal no permite establecer asociaciones de tipo causal entre los diversos factores estudiados con el exceso de peso.
En conclusión, encontramos que tres de cada diez escolares adolescentes residentes en áreas urbanas de los andes peruanos presentaron exceso de peso, siendo el sobrepeso la alteración más frecuente. El bajo nivel de actividad física es el principal factor de riesgo independiente para el desarrollo de obesidad. Los adolescentes pertenecientes a escuelas privadas presentan un mayor riesgo de sobrepeso y obesidad; sin embargo, dicha asociación se ve influenciada por estilos de vida como el adecuado consumo de agua y el descanso óptimo, que actuaron como variables confusoras. Los resultados del estudio apoyan la necesidad de implementar estrategias para incrementar el nivel de actividad física en el entorno educativo, y que dicha práctica saludable se traslade al hogar. Si bien no encontramos asociación con determinados hábitos de la dieta, es alarmante la elevada frecuencia de consumo de bebidas alcohólicas, gaseosas y aperitivos.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
FINANCIACIÓN
La investigación fue financiada por la Universidad Nacional de Cajamarca, según la Resolución Rectoral N.° 038-2013-UNC, de fecha 27 de febrero del 2013, donde se resuelve “aprobar los proyectos de investigación, presentados por los docentes de la Universidad Nacional de Cajamarca para ser financiados con Fondos Concursables Provenientes del Canon Minero, Sobrecanon y Regalías Mineras, correspondientes a la convocatoria 2012, Financiamiento de investigación Docente Canon Minero”.
ABREVIATURAS
ACV: accidente cardiovascular • HTA: hipertensión arterial • IC 95: intervalo de confianza del 95% • IMC: índice de masa corporal • INS: Instituto Nacional de Salud • OMS: Organización Mundial de la Salud • OR: odds ratio • ZIMC: puntuación z del índice de masa corporal para la edad.
BIBLIOGRAFÍA
- NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet. 2016;387:1377-96.
- Simmonds M, Burch J, Llewellyn A, Griffiths C, Yang H, Owen C, et al. The use of measures of obesity in childhood for predicting obesity and the development of obesity-related diseases in adulthood: a systematic review and meta-analysis. Health Technol Assess. 2015;19:1-336.
- Forrest KYZ, Leeds MJ. Prevalence and associated factors of overweight among Mexican-American adolescents. J Am Diet Assoc. 2007;107:1797-800.
- Niehues JR, Gonzales AI, Lemos RR, Bezerra PP, Haas P. Prevalence of overweight and obesity in children and adolescents from the age range of 2 to 19 years old in Brazil. Int J Pediatr. 2014;2014:583207.
- Catalani F, Fraire J, Pérez N, Mazzola M, Martínez AM, Mayer MA. Prevalencia de bajo peso, sobrepeso y obesidad en adolescentes escolarizados de la provincia de La Pampa. Arch Argent Pediatría. 2016;114:2-3.
- Skinner AC, Perrin EM, Skelton JA. Prevalence of obesity and severe obesity in US children, 1999-2014. Obesity. 2016;24:1116-23.
- Instituto Nacional de Salud, Centro Nacional de Alimentación y Nutrición. Observatorio de nutrición y estudio del sobrepeso y obesidad. Situación del sobrepeso y obesidad en la población peruana. En: Observa-T Perú [en línea] [consultado el 07/09/2017]. Disponible en www.observateperu.ins.gob.pe/sala-situacional/situacion-nutricional
- Hernández-Vásquez A, Bendezú-Quispe G, Díaz-Seijas D, Santero M, Minckas N, Azañedo D, et al. Análisis espacial del sobrepeso y la obesidad infantil en el Perú, 2014. Rev Peru Med Exp Salud Pública. 2016;33:489.
- Día Mundial de la Población 2015. En: Instituto Nacional de Estadística e Informática de Perú [en línea] [consultado el 07/09/2017]. Disponible en www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1251/Libro.pdf
- Álvarez-Dongo D, Sánchez-Abanto J, Gómez-Guizado G, Tarqui-Mamani C. Sobrepeso y obesidad: prevalencia y determinantes sociales del exceso de peso en la población peruana (2009-2010). Rev Peru Med Exp Salud Pública. 2012;29:303-13.
- Núñez-Robles E, Huapaya-Pizarro C, Torres-Lao R, Esquivel-León S, Suarez-Moreno V, Yasuda-Espinoza M, et al. Prevalence of cardiovascular and metabolic risk factors in school students, university students, and women from community-based organizations in the districts of Lima, Callao, la Libertad and Arequipa, Peru 2011. Rev Peru Med Exp Salud Pública. 2014;31:652-9.
- Lozano-Rojas G, Cabello-Morales E, Hernández-Diaz H, Loza-Munarriz C. Prevalencia de sobrepeso y obesidad en adolescentes de un distrito urbano de Lima, Perú 2012. Rev Peru Med Exp Salud Pública. 2014;31:494-500.
- Bustamante A, Maia J. Weight status and cardiorespiratory fitness in school students in the central region of Peru. Rev Peru Med Exp Salud Pública. 2013;30:399-407.
- Liria M, Mispireta M, Lanata C, Creed-Kanashiro H. Perfil nutricional en escolares de Lima y Callao. 1.ª edición. Lima, Perú: Instituto de Investigación Nutricional (ISIL); 2008.
- Larsen JK, Otten R, Fisher JO, Engels RC. Depressive symptoms in adolescence: a poor indicator of increases in body mass index. J Adolesc Health. 2014;54:94-9.
- Ames ME, Wintre MG, Flora DB. Trajectories of BMI and internalizing symptoms: Associations across adolescence. J Adolesc. 2015;45:80-8.
- Van Geel M, Vedder P, Tanilon J. Are overweight and obese youths more often bullied by their peers? A meta-analysis on the correlation between weight status and bullying. Int J Obes (Lond). 2014;38:1263-7.
- Odar Stough C, Merianos A, Nabors L, Peugh J. Prevalence and predictors of bullying behavior among overweight and obese youth in a nationally representative sample. Child Obes. 2016;12:263-71.
- Bacchini D, Licenziati MR, Garrasi A, Corciulo N, Driul D, Tanas R, et al. Bullying and victimization in overweight and obese outpatient children and adolescents: an italian multicentric study. PloS One. 2015;10:e0142715.
- Kaltiala-Heino R, Lankinen V, Marttunen M, Lindberg N, Fröjd S. Overweight, perceived overweight and involvement in bullying in middle adolescence. Child Abuse Negl. 2016;54:33-42.
- Brixval CS, Rayce SLB, Rasmussen M, Holstein BE, Due P. Overweight, body image and bullying--an epidemiological study of 11- to 15-years olds. Eur J Public Health. 2012;22:126-30.
- Twig G, Yaniv G, Levine H, Leiba A, Goldberger N, Derazne E, et al. Body-mass index in 2.3 million adolescents and cardiovascular death in adulthood. N Engl J Med. 2016;374:2430-40.
- Ninantanta J, Núñez L, García S, Romaní F. Frecuencia de síndrome metabólico en estudiantes de secundaria, universitarios y madres residentes de una región andina del Perú. Rev Peru Med Exp Salud Pública. 2016;33:640-50.
- De Onís M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. 2007;85:660-7.
- Universidad de Granada. Traducción de las guías para el procesamiento de datos y análisis del Cuestionario Internacional de Actividad Física (IPAQ). Versiones corta y larga. En: Junta de Andalucía [en línea] [consultado el 07/09/2017]. Disponible en www.juntadeandalucia.es/salud/sites/csalud/galerias/documentos/p_4_p_2_promocion_de_la_salud/actividad_fisica_alimentacion_equilibrada/IPAQ_Guia_Traducida.pdf
- Cogollo Z, Díaz C, Campo A. Exploración de la validez de constructo de la escala de Zung para depresión en adolescentes escolarizados. Colom Med. 2006;37:102-6.
- Observatorio Peruano de Drogas. Informe Ejecutivo: IV Estudio nacional de prevención y consumo de drogas en estudiantes de secundaria, 2012. Lima: DEVIDA; 2013.
- Aguilar L, Contreras M, Calle M del C. Guía técnica para la valoración nutricional antropométrica de las personas adolescentes. En: Ministerio de Salud, Instituto Nacional de Salud [en línea] [consultado el 07/09/2017]. Disponible en http://repositorio.ins.gob.pe/bitstream/INS/214/1/CENAN-0056.pdf
- Aceves-Martins M, Llauradó E, Tarro L, Solà R, Giralt M. Obesity-promoting factors in Mexican children and adolescents: challenges and opportunities. Glob Health Action. 2016;9:29625.
- Al-Hazzaa HM, Abahussain NA, Al-Sobayel HI, Qahwaji DM, Musaiger AO. Lifestyle factors associated with overweight and obesity among Saudi adolescents. BMC Public Health. 2012;12:354.
- Elías-Boneta AR, Toro MJ, García O, Torres R, Palacios C. High prevalence of overweight and obesity among a representative sample of Puerto Rican children. BMC Public Health. 2015;15:219.
- Rosaneli CF, Auler F, Manfrinato CB, Rosaneli CF, Sganzerla C, Bonatto MG, et al. Evaluation of the prevalence and nutritional and social determinants of overweight in a population of schoolchildren: a cross-sectional analysis of 5037 children. Rev Assoc Medica Bras (1992). 2012;58:472-6.
- Cook WK, Tseng W, Bautista R, John I. Ethnicity, socioeconomic status, and overweight in Asian American adolescents. Prev Med Rep. 2016; 4:233-7.
- Sweeting HN. Gendered dimensions of obesity in childhood and adolescence. Nutr J. 2008;7:1.
- Leatherdale ST. A cross-sectional examination of school characteristics associated with overweight and obesity among grade 1 to 4 students. BMC Public Health. 2013;13:982.
- Janssen I, Katzmarzyk PT, Boyce WF, King MA, Pickett W. Overweight and obesity in Canadian adolescents and their associations with dietary habits and physical activity patterns. J Adolesc Health. 2004;35:360-7.
- Saikia D, Ahmed SJ, Saikia H, Sarma R. Overweight and obesity in early adolescents and its relation to dietary habit and physical activity: a study in Dibrugarh town. Clin Epidemiol Glob Health. 2016;4:S22-28.
- Kelley GA, Kelley KS, Pate RR. Exercise and BMI in overweight and obese children and adolescents: a systematic review and trial sequential meta-analysis. Biomed Res Int. 2015;2015:704539.
- Janssen I, Katzmarzyk PT, Boyce WF, Vereecken C, Mulvihill C, Roberts C, et al. Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationships with physical activity and dietary patterns. Obes Rev. 2005;6:123-32.
- Mistry SK, Puthussery S. Risk factors of overweight and obesity in childhood and adolescence in South Asian countries: a systematic review of the evidence. Public Health. 2015;129:200-9.
- Guo X, Zheng L, Li Y, Yu S, Sun G, Yang H, et al. Differences in lifestyle behaviors, dietary habits, and familial factors among normal-weight, overweight, and obese Chinese children and adolescents. Int J Behav Nutr Phys Act. 2012;9:120.
- Vance VA, Woodruff SJ, McCargar LJ, Husted J, Hanning RM. Self-reported dietary energy intake of normal weight, overweight and obese adolescents. Public Health Nutr. 2009;12:222-7.
- Salcedo V, Gutiérrez-Fisac JL, Guallar-Castillón P, Rodríguez-Artalejo F. Trends in overweight and misperceived overweight in Spain from 1987 to 2007. Int J Obes (Lond). 2010;34:1759-65.