

¿Debemos preocuparnos por la coordinación corporal de los escolares de la Educación Secundaria Obligatoria?
Luis Miguel Ruiz Péreza, M Gómez Garcíab, P. J. Jiménez Martínc, I Ramón Oterod, R Peñaloza Méndeze
aCatedrático. Facultad de Ciencias de la Actividad Física y Deporte (INEF). Universidad Politécnica de Madrid. España.
bProfesora de Educación Física. Centro Cultural y Educativo Reyes Católicos. Bogotá. Colombia .
cProfesor Titular. Universidad Politécnica de Madrid. España.
dBecaria FPU. Ministerio de Educación. Universidad Politécnica de Madrid. España.
eProfesor. Instituto Politécnico Nacional de México. México.
Correspondencia: LM Ruiz. Correo electrónico: luismiguel.ruiz@upm.es
Cómo citar este artículo: Ruiz Pérez LM, Gómez García M, Jiménez Martín PJ, Ramón Otero I, Peñaloza Méndez R. ¿Debemos preocuparnos por la coordinación corporal de los escolares de la Educación Secundaria Obligatoria? Rev Pediatr Aten Primaria. 2015;17:e109-e116.
Publicado en Internet: 19-06-2015 - Número de visitas: 25015
Resumen
Existe una preocupación sobre el nivel de competencia coordinativa de los escolares en la Educación Secundaria Secundaria (ESO) española y su impacto en sus actividades cotidianas y en su salud. El objetivo de este estudio fue evaluar la coordinación de una muestra de escolares de primero de la ESO. Participaron 120 escolares, 65 chicos y 55 chicas, de cuatro institutos de Educación Secundaria de la Comunidad de Madrid, de edades comprendidas entre 12 y 14 años. Todos los participantes llevaron a cabo el test de coordinación corporal (KKTK) diseñado para detectar los problemas de coordinación motriz en las edades escolares. Los resultados permitieron el establecimiento de tres grupos de coordinación: normal (38,3%), sintomático (31,35%) y problemático (30%). Estos resultados indicaron que un 61,7% de los escolares participantes en este estudio presentaban algún tipo de dificultad de coordinación, al encontrarse en los niveles sintomático y problemático. La presencia de las chicas en el nivel sintomático y problemático fue predominante. Los resultados confirman que los problemas de coordinación motriz existen en la población escolar y que no solo suponen un problema educativo sino también de salud, ya que impiden estilos de vida más activos entre los adolescentes, especialmente entre las chicas.
Palabras clave
● Adolescencia ● Desarrollo motor ● Educación Secundaria ● Estilos de vida ● Trastornos evolutivos de la coordinaciónINTRODUCCIÓN
Sin duda son numerosos los beneficios que conlleva practicar actividades físicas y deportivas en las edades escolares1,2. Son numerosas las investigaciones que apoyan la necesidad de que las autoridades educativas y sanitarias consideren que es una buena decisión ampliar los días a la semana de educación física en la escuelas, ya que, lejos de afectar al rendimiento académico, contribuye a su mejora e incrementa la salud de los escolares3-5. No obstante la evidencia muestra un descenso progresivo del interés por estas prácticas entre los adolescentes6 así como un preocupante aumento del sobrepeso y obesidad en estas edades7.
La coordinación motriz se considera una de las principales funciones de la competencia motriz, siendo la que mejor predice las posibilidades de practicar actividad física en el futuro8,9. Está ampliamente demostrado que una baja coordinación suele ir asociada con bajos niveles de práctica10, una baja condición física11, un aumento poco saludable del peso corporal12,13, una baja autoestima14, baja competencia percibida15, ansiedad16 e incluso acoso escolar14.
Desde una perspectiva internacional, se estima que entre un 5% y un 18% de la población escolar presenta problemas de coordinación. La literatura científica los denomina trastornos evolutivos de la coordinación (developmental coordination disorders [DCD])17. En España este porcentaje está por establecer y la preocupación por esta cuestión entre los profesionales de la sanidad, educación y psicología es reducida a tenor de la escasez de estudios sobre este particular16, mientras que en otras latitudes se ha convertido en un objetivo de indagación y preocupación9,13,18.
EΧisten todo un conjunto de instrumentos dirigidos principalmente a la detección de este tipo de problemas, pero son poco utilizados entre los profesionales españoles. Nos referimos al test de rendimiento Motor-BOT-2 de Bruininks-Oseretsky19, la batería de aptitud motriz básica revisada BMAT-R20, el test de evaluación del desarrollo neuromuscular de McCarron MAND21, el test de coordinación corporal (KKTK)22 o la batería de evaluación del movimiento ABC-2, recientemente validada y tipificada en población española23.
El presente estudio ha tenido como objetivo principal analizar el nivel de coordinación motriz de una muestra de escolares españoles de la Educación Secundaria en función del género y de la edad.
MATERIAL Y MÉTODOS
Participantes
Participaron voluntariamente 120 escolares de ambos seΧos, de edades comprendidas entre 12 y 14 años (M: 12,54 años; DT: 0,65 años), representando a cuatro institutos públicos de Educación Secundaria ubicados en zonas urbanas de la Comunidad de Madrid (España). El 54,2% (65) fueron chicos y el 45,8% (55) fueron chicas.
Test motor
Para evaluar la coordinación motriz global se empleó el de Kiphard y Schilling22. Este instrumento fue desarrollado para identificar y diagnosticar las dificultades de coordinación en escolares entre los 5 y 14 años. Evalúa la dimensión “control y coordinación global del cuerpo” y consta de cuatro pruebas:
- Equilibrio desplazándose hacia atrás. El escolar tiene que desplazarse paso a paso hacia atrás sobre tres diferentes barras de equilibrio de 3 m de longitud, de tres anchuras diferentes en su base (6, 4,5 y 3 cm), anotándose el número de pasos que es capaz de dar en cada una de ellas.
- Saltos con una pierna (unipodal) por encima de un obstáculo. El escolar debe saltar a la pata coja y superar un obstáculo compuesto por bloques de goma-espuma de 50 × 20 × 5 cm. La altura van aumentando progresivamente con la edad. Una vez superado el obstáculo, el participante debe continuar saltando al menos dos saltos más. Se evalúan ambas piernas.
- Saltos laterales. El escolar debe saltar con los pies juntos a un lado y a otro de un listón de 60 × 4 × 2 cm, tan rápido como sea capaz en 15 segundos, anotándose el número de saltos realizados correctamente.
- Desplazamiento sobre soportes. El escolar tiene que desplazarse sobre unos soportes de 25 × 25 × 2 cm, que se apoyan en cuatro topes de 3,7 cm de altura. Partiendo encima de uno de ellos y sujetando el otro con las dos manos, debe ir avanzando siempre sobre un soporte, para lo cual los irá colocando en la dirección de la marcha, subiéndose en uno y colocando el libre. Se anota el número de cambios correctamente realizados en 20 segundos.
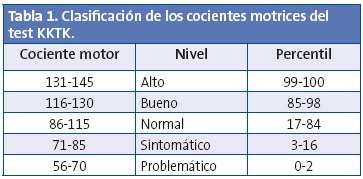
Para establecer el nivel de coordinación alcanzado por los escolares participantes las puntuaciones obtenidas directamente se transforman en una puntuación tipificada (cociente motor) para cada una de las tareas, que posteriormente constituyen el cociente motor global (media: 100, desviación típica: 15), con una distribución percentílica. Un resultado de 85 o menos en el cociente motor global representó un rendimiento motor por debajo del percentil 15. Una puntuación menor de 70 supone estar por debajo del percentil tercero (Tabla 1). Los baremos originales del test están establecidos considerando tanto la edad (4/5 a 14 años) como el género.
Procedimiento
Se contactó directamente con los directores de los centros y los profesores de Educación Física para eΧplicarles la naturaleza del estudio, pedir su permiso y solicitar colaboración. Posteriormente se elaboró una carta eΧplicativa del estudio que fue remitida a los padres de los alumnos para que otorgaran su consentimiento mediante la firma de dicho documento. El test se aplicó de manera individual en una zona reservada (aula y/o gimnasio) durante las sesiones de educación física. El tiempo empleado para cada alumno fue de 15 a 20 minutos, aproΧimadamente.
Análisis estadísticos
Para ratificar la estructura factorial del test se aplicó un análisis factorial (método de componentes principales) con rotación varimaΧ. La adecuación de la matriz para realizar este análisis fue testada mediante el test Kaiser-Meyer-Olkin (KMO) y la prueba de esfericidad de Bartlett. Se llevaron a cabo pruebas de normalidad y homogeneidad mediante las pruebas de Kolmogorov-Smirnov y Levene respectivamente, y posteriormente se llevaron a cabo análisis descriptivos (medias y desviaciones típicas) y diferenciales en función del género y edad, mediante el análisis multivariante de la varianza (MANOVA). En todo momento se tuvo en cuenta un nivel de significación bilateral de 0,05. Además se consideró conveniente informar del tamaño del efecto obtenido. Los cálculos estadísticos se realizaron con el programa SPSS® 20.0.
RESULTADOS
Análisis factorial con las cuatro pruebas aplicadas
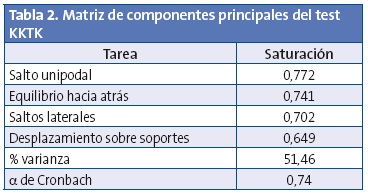
Con la intención de confirmar la unidimensionalidad de este test, que está compuesto de cuatro tareas diferentes, se llevó a cabo un análisis factorial (método de componentes principales) con rotación varimaΧ. Tanto los resultados de la prueba de esfericidad de Bartlett (Χ2(6) = 72,76; p<0,000) como la adecuación muestral (MSA), obtenida mediante el índice global de Kaiser, Meyer y Olkin (0,716) fueron satisfactorios para poder aplicar el análisis factorial. Del análisis se obtuvo un único factor con un autovalor mayor de 1, que eΧplicó un 51,46% de la varianza, saturaciones superiores a 0,60 y una fiabilidad de 0,74 (Tabla 2). Estos resultados ratificaron la estructura unifactorial del test que establecieron sus autores con una amplia muestra de escolares alemanes.
Análisis descriptivos y diferenciales
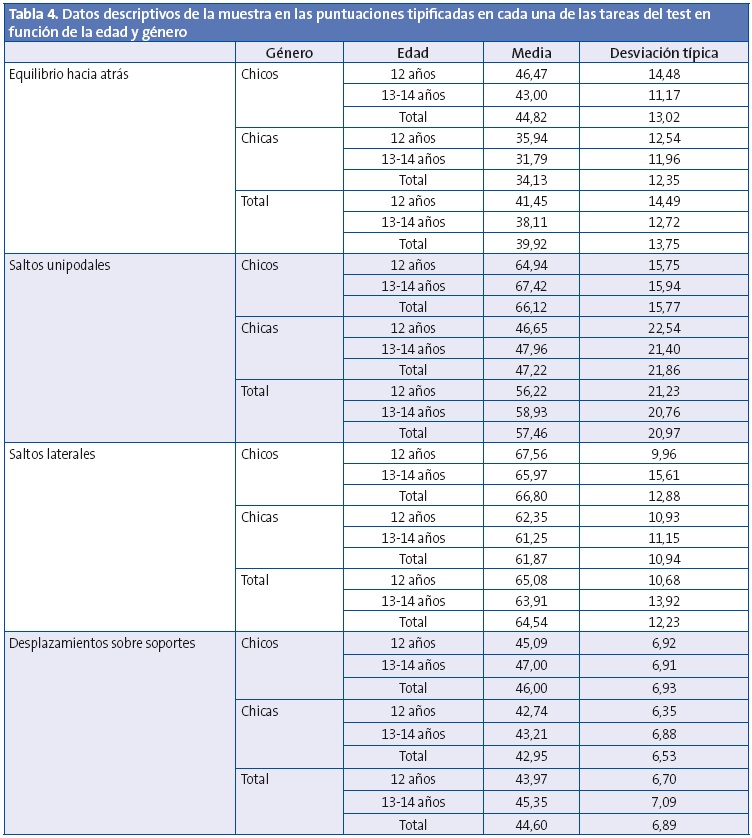
Los datos descriptivos de las puntuaciones de la muestra en cada una de las tareas del test, tanto en función del género como de la edad, se presentan en las Tablas 3 y 4.

Análisis diferenciales
Con el objetivo de comprobar los efectos de las variables género (hombre y mujer) y edad (12 y 13-14 años) en las diferentes tareas del test, se llevó a cabo un análisis MANOVA, tomando como variables dependientes las tareas del test y como factores el género y la edad, encontrándose únicamente diferencias significativas en función del género (Lambda de Wilks: 0,645; F=15,57; p<0,000; η2=0,35). Los contrastes univariados confirmaron que estas diferencias se manifestaban en las cuatro tareas del test (equilibrio hacia atrás: p=0,029, η2=0,015; salto unipodal: p=0,000, η2=0,15; saltos laterales: p=0,000, η2=0,026; desplazamiento sobre soportes: p=0,010, η2=0,05). Estas diferencias indicaron que las puntuaciones de los varones fueron más elevadas que las de las chicas.
A partir de las puntuaciones, se distribuyeron los participantes en tres grupos en función de su rendimiento en el test. El valor promedio del cociente motor obtenido por los chicos de este estudio fue de 88,63 (DT=14,68) y el de las chicas de 67,25 (DT=16,60), lo que indicó que, si bien la puntuación media de los varones se encontraba en el intervalo considerado como normal según las normas del test, la referida a las chicas estaba en el intervalo considerado como problemático (ver Tabla 1).
Cuarenta y seis escolares (38,3%) formaron parte del nivel normal de coordinación, 38 escolares (31,7%) del nivel sintomático y 36 escolares (30%) del nivel problemático. Estos resultados indicaron que un 61,7% de los escolares, 74 participantes en este estudio, presentaban algún tipo de dificultad de coordinación al encontrarse todos ellos en los niveles sintomático y problemático.
Es de destacar que ningún escolar superó la puntuación de 113, y por lo tanto, ninguno pudo ser clasificado, según los niveles de referencia, de un nivel de coordinación bueno o alto. También hay que resaltar que fueron las chicas las que más predominaban en los niveles sintomático y problemático, sobre todo en el tramo de edad de los 13-14 años (Tabla 5), tramo en el que solo una de las veinticuatro chicas obtuvo resultados que entraban dentro del nivel normal de coordinación.

DISCUSIÓN
El propósito principal de este estudio fue analizar el nivel de coordinación motriz global de una muestra de escolares españoles de primer curso de la ESO a través del test de coordinación corporal22. Los resultados pueden considerarse preocupantes, ya que 74 de los 120 escolares de la muestra (61,7%) se hallaban por debajo del nivel recomendable (normal) de coordinación motriz que los autores del test establecieron, clasificándose dentro de los niveles sintomático y problemático.
Estos resultados alertan sobre lo que ya se ha indicado en estudios previos, la presencia en las escuelas y en los institutos de escolares que presentan dificultades para moverse de manera coordinada, lo que se manifiesta en Educación Infantil, Primaria y Secundaria. En la ESO sigue siendo una dificultad oculta e ignorada16. El hecho de que ningún participante obtuviera una puntuación que le permitiera ser clasificado en un nivel bueno o alto lleva a refleΧionar sobre el precario nivel de competencia coordinativa de los escolares participantes en el estudio, y la necesidad de plantearse las razones de esta situación.
Los autores del test22 en su estudio de 1974 con 1283 escolares encontraron que solo un 2% presentaba verdaderos problemas de coordinación (problemáticos) y que el 68% se ubicaba en el nivel normal, siendo un 14% de buena coordinación y un 2% de coordinación motriz alta. La comparación parece obvia, ya que después de cuatro décadas transcurridas, el descenso en la competencia coordinativa es muy marcado en poblaciones muy diferentes, como han demostrado los estudios llevados a cabo en Portugal, Brasil, Grecia, Noruega, Canadá, Bélgica u Holanda24-28.
Recientemente el estudio de Torralba et al.29, llevado a cabo en Barcelona con escolares catalanes de siete a diez años y con este mismo instrumento, presentó resultados similares. En dicho estudio, en el que participaron 1254 escolares, un 40% presentó alguna dificultad de coordinación y solo un 4,6% fue clasificado por encima del nivel normal. El reciente estudio de Vandorpe et al.30, llevado a cabo en Bélgica, llegó a conclusiones similares confirmando un descenso en la competencia coordinativa en estas cuatro décadas transcurridas después del estudio originario del test.
En el caso español estos resultados son sin duda una llamada de atención tanto para los profesionales sanitarios como para los profesionales de la Educación, ya que si bien el sistema educativo posee la asignatura de la Educación Física escolar, no por ello deja este problema de estar presente entre la población escolar española, y, como ya ha sido comentado, una baja coordinación motriz conlleva en el futuro estilos de vida poco activos y saludables7,28,31.
Es muy probable que la razón de que una parte importante de los escolares se encuentre en el nivel sintomático sea un verdadero déficit de actividad física23,31-33. El tiempo obligatorio semanal de las clases de Educación Física en la Educación Secundaria Obligatoria no supera las dos horas, lo cual es a todas luces muy escaso, y el porcentaje de escolares que no realizan ningún tipo de actividad física o deportiva eΧtraescolar es cada vez más elevado.
Los escolares que forman parte del grupo problemático son los que debieran recibir una atención más intensa y un eΧamen más detenido de su situación, ya que es muy probable que presenten todas las características para ser considerados escolares con trastornos evolutivos de la coordinación (DCD) tal y como los define la Asociación Psiquiátrica Americana34. Este sí es un problema que atañe a los profesionales de la salud tanto o más que al profesor de educación física. No prestarle atención condena a estos escolares a llegar a la adultez con estas mismas dificultades15,35 y a la adopción en estas edades de estilos de vida sedentarios.
Otro aspecto importante a destacar es que una mayoría de los escolares de los niveles sintomático y problemático fueron chicas. La diferencia en el rendimiento coordinativo entre chicos y chicas ha sido notable, especialmente en las edades de 13-14 años, lo cual coincide con lo encontrado también por Torralba et al. en su investigación con los escolares catalanes29. En el presente estudio, de los 36 escolares (31,7%) que se encontraban en el nivel problemático, la ratio de chicas con respecto a chicos fue de 5:1 en los dos tramos de edad. Asimismo, llama la atención que de los 46 escolares (38,3%) que se encontraban en el nivel normal de coordinación, solo cuatro de 12 años fueran chicas y en el tramo de 13-14 años, solamente una. Sin duda esta es una cuestión alarmante y que debiera ser considerada con mayor detenimiento, ya que, si se asume la asociación eΧistente entre la baja coordinación y los bajos niveles de práctica de actividad física, son las chicas las más proclives al sedentarismo y a todo lo que de él se deriva11.
CONCLUSIONES
Numerosos estudios están llamando la atención por el deterioro de la condición física entre los escolares y el aumento de sobrepeso y la obesidad36-39. La competencia coordinativa ha descendido notablemente entre los niños y adolescentes y necesita de una atención mucho más decidida tanto por parte de las autoridades médicas como por las educativas. Este estudio se une a los ya realizados y que llaman la atención sobre la necesidad de considerar estos problemas no solo una cuestión educativa si no de salud infantil y juvenil.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS: DCD: developmental coordination disorders; DCD: trastornos evolutivos de la coordinación; ESO: Educación Secundaria Secundaria; KMO: test Kaiser-Meyer-Olkin; MANOVA: análisis multivariante de la varianza; MSA: adecuación muestral; test KKTK: Körper Koordination Test für Kinder.
BIBLIOGRAFÍA
- Donnelly JE, Greene JL, Gibson CA, Sullivan DK, Hansen DM, Hillman CH, et al. Physical activity and academic achievement across the curriculum (A+PAAC): rationale and design of a 3-year, cluster-randomized trial. BMC Publ Health. 2013;13:307.
- Kohl HW 3rd, Hobbs KE. Development of physical activity behaviors among children and adolescents. Pediatrics. 1998;101:549-54.
- Ahamed Y, Macdonald H, Reed K, Naylor PJ, Liu-Ambrose T, McKay H. School-based physical activity does not compromise children’s academic performance. Med Sci Sports EΧerc. 2007;39:371-6.
- Ericsson I. Motor skills, attention and academic achievements. An intervention study in school years 1-3. Brit Educ Res J. 2008;34:301-13.
- Trudeau F, Shephard RJ. Physical education, school physical activity, school sports and academic performance. Int J Behav Nutr Phys Act. 2008;5:10.
- Cocca A, Liukkonen J, Mayorga-Vega D, Viciana-Ramírez J. Health-related physical activity levels in Spanish youth and young adults. Percept Mot Skills. 2014;118:247-60.
- Arriscado Alsina D, Muros Molina JJ, Zabala Díaz M, Dalmau Torres JM. Influencia del seΧo y el tipo de escuela sobre los índices de sobrepeso y obesidad. Rev Pediatr Aten Primaria. 2014;16:e139-e146.
- Lopes VP, Rodrigues LP, Maia JA, Malina RM. Motor coordination as predictor of physical activity in childhood. Scand J Med Sci Sports. 2011;21:663-9.
- Saakslahti A, Numminen P, Niinikoski H, Rask-Nissila L. Viikari J, Tuominen J, et al. Is physical activity related to body size, fundamental motor skills, and chd risk factors in early childhood? Pediatr EΧerc Sci. 1999;11:327-40.
- Williams HG, Pfeiffer KA, O'Neill JR, Dowda M, McIver KL, Brown WH, et al. Motor skill performance and physical activity in Preschool children. Obesity (Silver Spring). 2008;16:1421-6.
- Lifshitz N, Raz-Silbiger S, Weintraub N, Steinhart S, Cermak SA, Katz N. Physical fitness and overweight in Israeli children with and without developmental coordination disorder: Gender differences. Res Dev Disabil. 2014;35:2773-80.
- Cairney J, Hay JA, Faught BE, Hawes R. Developmental coordination disorder and overweight and obesity in children aged 9-14 years. Int J Obes (Lond). 2005;29:369-72.
- Montgomery SM. Coordination, childhood weight gain and obesity. CMAJ. 2010;182:1157-8.
- Piek JP, Barrett NC, Allen LS, Jones A, Louise M. The relationship between bullying and self-worth in children with movement coordination problems. Br J Educ Psychol. 2005;75:453-63.
- Fitzpatrick DA, Watkinson EJ. The lived eΧperience of physical awkwardness: adults’ retrospective views. Adapt Phys Act Q. 2003;20:279-97.
- Gómez M, Ruiz LM, Mata E. Los problemas evolutivos de coordinación en la adolescencia: análisis de una dificultad oculta. RICYDE. Rev Int Cienc Deporte. 2006;3:44-54.
- Kadesjö B, Gillberg C. Developmental coordination disorder in Swedish 7 years-olds. J Am Acad Child Adolesc Psychiatry. 1999;38:820-8.
- Ruiz LM. Moverse con dificultad en la escuela. Introducción a los problemas evolutivos de coordinación motriz. Sevilla: Wanceulen; 2005.
- Bruininks RH. Bruininks-Oseretsky test of motor proficiency, 2nd ed (BOT™-2). EE. UU.: Pearson; 2005.
- Arnheim D, Sinclair W. El niño torpe. Un programa de terapia motriz. Buenos Aires: Médica-Panamericana; 1976.
- McCarron LT. McCarron assessment of neuromuscular development. Dallas: Common Market Press; 1982.
- Kiphard EJ, Schilling VF. Köperkoordinations-test für kinder. Beltz Test GMBH. Weinhein; 1974.
- Henderson SE, Barnett S, Sugden DA. MABC-2, batería de evaluación del movimiento para niños- 2. EE. UU.: Pearson; 2011.
- Carminato RA. Desempenho motor de escolares através da bateria de teste KTK. Dissertação de Mestrado, Universidade Federal do Paraná, Curitiba-Brasil; 2010.
- Lopes VP, Maia JAR, Silva RG, Seabra A, Morais FP. Estudo do nível de desenvolvimento da coordenação motora da população escolar (6 a 10 anos de idade) da Região Autónoma dos Açores. Rev Port Ciênc Desporto. 2003;3:47-60.
- Mjaavatn PE, Gundersen KA, Segberg V. Physical activity and health related variables in 6-9 year-old Norwegian children. Med Sci Sports EΧerc. 2003;35:S63.
- Smits-Engelsman BC, Henderson SE, Michels CGJ. The assessment of children with developmental coordination disorder in the Netherlands: The relationship between the Movement Assessment Battery for Children and the Korperkoordinations Test Fuer Kinder. Hum Mov Sci. 1998;17:699-709.
- Tsiotra GD, Nevill AM, Lane AM, Koutedakis Y. Physical fitness and developmental coordination disorder in Greek children. Pediatric EΧer Sci. 2009;21:186-95.
- Torralba MA, Vieira MB, LleiΧá T, Gorla JL. Evaluación de la coordinación motora en educación primaria de Barcelona y provincia. Rev Int Med Cienc Act Fís Deporte. 2015 [en prensa].
- Vandorpe B, Vandendriessche J, Lefevre J, Pion J, Vaeyens R, Matthys S, et al. The Körperkoordinations Test fur Kinder: reference values and suitability for 6–12-year-old children in Flanders. Scand J Med Sci Sports.2011;21:378-88.
- Bouffard M, Watkinson EJ, Thompson LP, Causgrove Dunn JL, Romanow SKE. A test of the activity deficit hypothesis with children with movement difficulties. Adapt Phys Act Q. 1996;13:61-73.
- Cairney J, Hay JA, Veldhuizen S, Missiuna C, Faught BE. Developmental coordination disorder, seΧ, and activity deficit over time: a longitudinal analysis of participation trajectories in children with and without coordination difficulties. Dev Med Child Neurol. 2010;52:e67-72.
- Cairney J, Hay JA, Faught BE, Corna LM, Flouris A. Developmental coordination disorder, age, and play: a test of the divergence in activity-deficit with age hypothesis. Adapt Phys Activ Q. 2006;23:261-76.
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4.ª edición. Washington, DC: Author; 2006.
- Cousins M, Smyth MM. Developmental coordination impairments in adulthood. Hum Mov Sci. 2003;22:433-59.
- García Cruz A, Figueroa Suárez J, Osorio Ciro J, Rodríguez Chavarro N, Gallo Villegas J. Asociación entre el estado nutricional y las capacidades físicas en niños de 6 a 18 años de Medellín (Colombia). An Pediatr (Barc). 2014;81:343-51.
- Barnett LM, van Beurden E, Morgan PJ, Brooks LO, Beard JR. Childhood motor skill proficiency as a predictor of adolescent physical activity. J Adolesc Health. 2009;44:252-9.
- Watkinson EJ, Causgrove Dunn J, Cavaliere N, Calzonetti K, Wilhelm L, Dwyer S. Engagement in playground activities as a criterion for diagnosing developmental coordination disorders. Adapt Phys Activ Q. 2001;18:18-34.
- Casajus JA, Leiva MT, Villarroya A, Legaz A, Moreno LA. Physical performance and school physical education in overweight Spanish children. Ann Nutr Metab. 2007;51:288-96.