
Vol. 17 - Num. 66
Original Papers
Risk factors for early sexual debut in adolescents
Pablo Royuela Ruiza, Luis Rodríguez Molinerob, José Manuel Marugán de Miguelsanzc, V Carbajosa Rodrígueza
aMédico de Familia. Unidad de Urgencias Hospital Universitario Río Hortega. Valladolid. España.
bServicio de Pediatría. Hospital Recoletas Campo Grande. Valladolid. España.
cServicio de Pediatría. Hospital Clínico de Valladolid. Universidad de Valladolid. Valladolid. España.
Correspondence: P Royuela. E-mail: pabloroyuela@yahoo.es
Reference of this article: Royuela Ruiz P, Rodríguez Molinero L, Marugán de Miguelsanz JM, Carbajosa Rodríguez V. Risk factors for early sexual debut in adolescents. Rev Pediatr Aten Primaria. 2015;17:127-36.
Published in Internet: 18-06-2015 - Visits: 150974
Abstract
Introduction: in the last years, sexual initiation in our young people seems to have anticipated. In this study we want to find out what risk factors have statistically significant relation to having sexual relations with penetration in adolescents.
Methods: 1289 students of 2.º and 3.º grade of Secondary Education in the region of Castilla-León (Spain) were interrogated in the 2010-2011 school year. Multiple epidemiological variables were analyzed, calculating centralization and dispersion in quantitative variables, and distribution of frequencies in qualitative variables.
Results: 563 boys and 726 girls were studied. The students’ media age was 14.05 years (median and mode: 14 years; range: 12-17 years). 17.5% had had sexual relations with penetration. (9% at 12; 6% at 13; 10.6% at 14; 34.2% at 15; 53.2% at 16 and 57.1% at 17 years). This percentage was greater in boys (20.2%) than girls (15.4%). Other statistically significant associated factors (p< 0.05) were being older, worse relation with his parents, divorced parents, worse relation between their parents, smoking, drinking alcohol, getting drunk, consuming drugs, worse present health, worse feeding, worse memory, having more erotophilia and being agnostic or atheist.
Conclusions: adolescent sexual precocious initiation risk factors are alcohol, tobacco, drug consumption, a bad relationship with their parents and between their parents.
Keywords
● Adolescent ● Risk factors ● SexualityINTRODUCTION
There is a high variability between individuals in the time of sexual debut; however, evidence suggests that adolescents in Spain are having sex at increasingly younger ages and becoming more promiscuous.1
Leaving aside the matter of moral or religious prohibitions, early sexual debut poses problems due to its association with other high-risk sexual behaviours. Adolescents that have intercourse at very early ages more frequently report having a sexually transmitted infection (STI), having a greater number of sex partners, and using condoms less frequently.2
Unwanted pregnancy is yet another risk associated with early sexual debut. The Observatorio de Salud Reproductiva (Reproductive Health Observatory) of the Consejo Superior de Investigaciones Científicas has declared that in recent years there has been a sustained increase in the number of adolescent pregnancies, so that the number of pregnancies per 1000 women aged 15 to 19 years has increased from 15.12 in 1999 to 24.21 in 2009. A similar increase has been observed in the fertility rate of this age group, which in Spain was 8.54 in 1999 and had risen to 11.78 in 2009. This was associated with an increase in the proportion of unwanted pregnancies, which went from 95.35% in 1999 to 98.15% in 2009, and in the rate of voluntary termination of pregnancy per 1000 women aged 15 to 19 years, which rose from 7.49 in 2000 to 12.74 in 2009.3
The aim of this study was to identify the risk factors for adolescents having sex with penetration in students of the second and third year of secondary compulsory education (Educación Secundaria Obligatoria [ESO]) of Castile and León. We believe that these data will be very useful for health promotion in present-day and future adolescents.
MATERIALS AND METHODS
The population under study were students enrolled in second and third year of ESO in schools of Castile and León during the 2010–2011 academic year. There were a total of 44 031 students (male, 50.84%; female, 49.16%).4
For the purposes of data collection, we performed random cluster sampling. The students that participated in our study were grouped into several schools, and each year (2nd and 3rd of ESO) in each school constituted a student cluster.5,6 We conducted a survey of all the students included in each cluster selected during sampling.
We needed to adjust the sample size calculated by means of the formula shown in Figure 1 to avoid what is known as the design effect, which is the proportion of the variance of simple random sampling explained by the variance of cluster sampling.6
To find out the expected prevalence (p) of sex with intercourse in girls enrolled in second and third year of ESO in our region, we started by performing a literature search, but found no useful data. Thus, we had to conduct a pilot study on 40 adolescents enrolled in second and third year of ESO in a school chosen at random to be able to calculate the necessary sample size and make the questionnaire more understandable. In this pilot study, the prevalence of having had sexual intercourse in students of the second and third year of ESO was 10%, and we used this figure for the sample size calculation.
Based on the reviewed literature and the data obtained in the pilot study, we thought it would be appropriate to estimate the design effect at 1,4; that is, we assumed that there would be a 40% increase in variance in the estimators used in our design compared to simple randomised sampling. Thus, the sample size needed to use cluster sampling, for a margin of error of 3% and a 95% confidence level, was 528 girls and 529 boys.
To achieve this number of completed questionnaires, we needed to reach a large enough number of schools. Thus, we chose schools at random and surveyed the students until we had collected data for more than 528 girls and more than 529 boys. When a school declined to participate, we randomly selected another school from the list of 390 institutions that offer ESO in Castile and León.
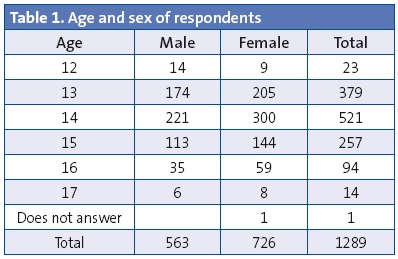
In the end, we needed to include 16 schools to obtain 1289 completed questionnaires corresponding to 726 girls and 563 boys. The questionnaires were administered between October 2010 and April 2011 (Table 1).
The questionnaire consisted of 86 items. Its length was about 20 minutes. The questions were grouped into sections based on subject matter: a) relationship with the parents; b) health, physical activity, self-esteem, religious beliefs; c) legal and illegal drugs, and d) sexuality.
One of the researchers (in addition to the students’ teacher) was in the classroom during the administration of the questionnaire to answer questions and ensure anonymity. The questionnaire was only administered to students that had submitted the parental consent form. None of the parents overtly refused to let their children participate in the survey, but approximately 12% of the students failed to bring the consent form signed by their parents, ostensibly due to carelessness or indifference. These students were not given the questionnaire, and were mostly male (this is the main reason for the differences between sexes found in the analysis of the data).
In the statistical analysis, we calculated the mean, median, range, standard deviation and standard error for quantitative variables, and the frequency distribution for qualitative variables. We compared means using Student’s t test and frequencies with the chi-square test, setting the level of statistical significance at P < 0.05. We also calculated the relative risk for dichotomous variables
RESULTS
The mean age of the respondents was 14.05 years with a standard deviation of 0.98 (median and mode, 14 years; range, 12–17 years). The mean age of the boys was 14.00 years (standard deviation, 0.98) and that of girls 14.09 years (standard deviation, 0.97), with no statistically significant differences between sexes.
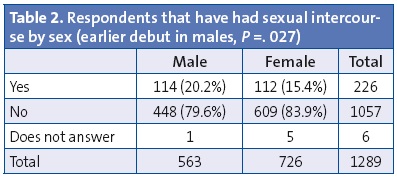
Of all surveyed adolescents, 17.5% reported having had sexual intercourse (Tables 3 and 4). This percentage was higher in males (20.2%) than in females (15.4%). The difference between the sexes was statistically significant (P = .027).
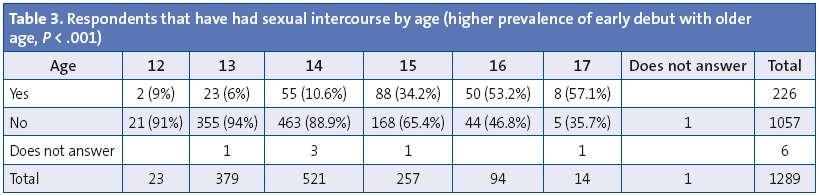
As Table 3 shows, as respondents grew in age, a greater proportion reported having had sex with intercourse. Furthermore, we ought to remember that there were only twenty-three 12-year-old participants, and only fourteen aged 17 years, so comparing them to the remaining groups (which were much larger) could have led to biased results. For this reason, they were not taken into account when the results were adjusted for age.
Relationship with the parents
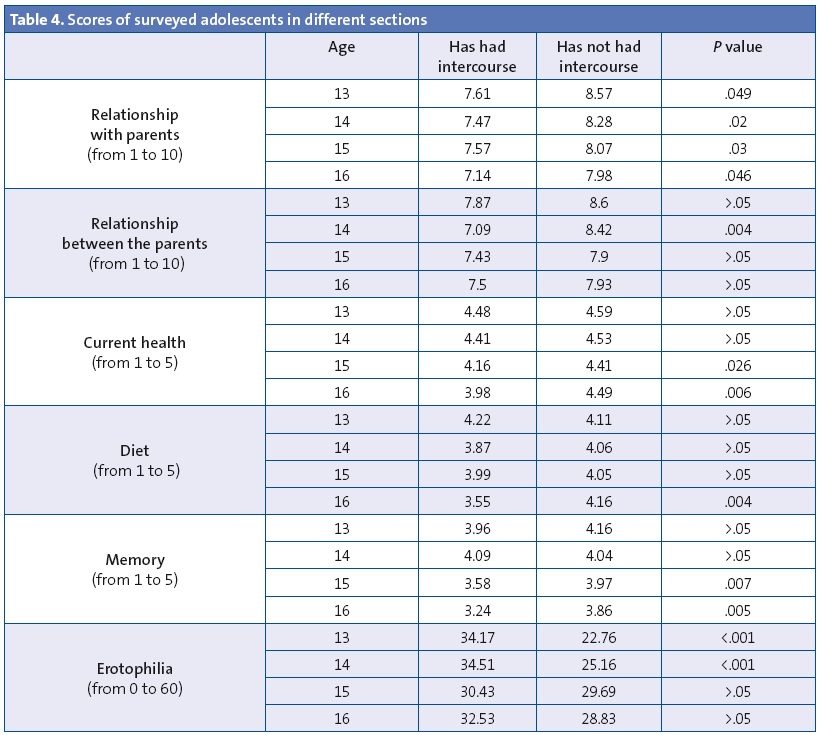
Overall, adolescents that had had intercourse had scored a mean of 7.45 points out of 10 in the section devoted to their relationship with their parents, while adolescents that had not had intercourse had a mean score of 8.34 (P < .001). Taking into consideration the age of the participants, the correlation of intercourse with a poorer relationship with the parents reached statistical significance in every age group (Table 4).
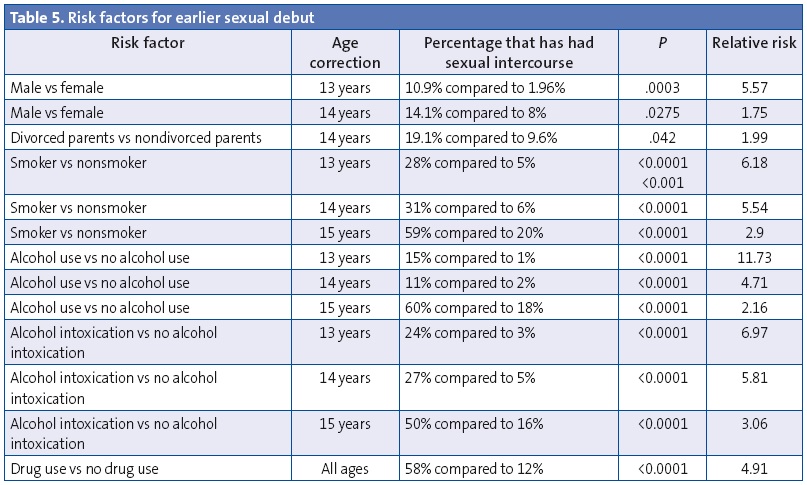
Furthermore, the relationship between the parents was also important. Adolescents aged 14 years with divorced parents (Table 5) or with parents that did not have a good relationship (Table 4) had their sexual debut at earlier ages.
Drug use
Adolescents in our survey that had used alcohol, tobacco and other drugs also had earlier sexual debuts more frequently (Table 5).
Other associations found in the study
We also found a statistically significant correlation between self-perceived memory, diet quality or current health and having or not having had sexual intercourse (Table 4). However, we only found differences in certain age intervals, so we should be cautious in making any inferences.
When it came to religion, we found that at age 13 years, 52% of respondents that had had intercourse identified as agnostics or atheists compared to 22% of nonpractising Catholics and 26% of hardly-practising Catholics. Meanwhile, of the same-age peers that had never engaged in intercourse, 19% identified as agnostics or atheists, 28% as nonpractising Catholics, 28% as hardly-practising Catholics, 23% as practising Catholics and 2% as believers of a different faith. These differences were statistically significant (P = .01).
Factors that did not influence first intercourse at early or earlier ages
Our questionnaire also asked about other circumstances for which we found no significant differences between adolescents that had had sexual intercourse and adolescents that had not. They included being members of a group (P = .97), the level of information on the effects of drug use (P = .13), being physically active (P = .19), taking the subject of sexuality at school (P = .26), believing that pregnancy is a risk in adolescence (P = .07), sexual orientation (P = .24) and health during childhood (P = .31).
There were other items that at first seemed to be associated with having had sex with intercourse, but when we adjusted for age the differences were not statistically significant (P = .05). These were information on STIs, information on sexuality, mood, and self-esteem.
DISCUSSION
Male versus female
In our study, and nearly in every study of sexual behaviour in adolescents, the answers to each item are compared based on the sex of the respondent. According to our results, boys have intercourse earlier than girls. This was also found in several previous studies.3,7
Furthermore, males tend to have casual partners and engage in riskier behaviours than females. On the other hand, females tend to have sex in the context of a stable relationship associated with trust and affection.7
This is because male and female adolescents experience sexuality differently, even though these differences seem to have become less marked in recent years. Females are more likely to associate sexual activity with affection, intimacy and commitment than their male counterparts. In fact, they tend to have fewer partners and assign a stronger emotional and social meaning to past or present partners. Another factor in which the sexes differ is that males have sexual fantasies more frequently, experience sexual desire more intensely and seek sex more actively than females.8,9
These differences in motivation, exclusivity, attraction, desire, fantasies and initiative reflect a clear pattern: male adolescents have more explicit sexual urges that are geared to a greater number of individuals, and sex is more present in their minds and their sexual feelings, while female adolescents rather tended to associate sex with affection and with a single partner or a smaller number of individuals, while thinking of sex less explicitly. Still, a considerable number of teenagers did not fit this pattern, which seems to be in the process of changing. This process seems particularly evident when we consider age-related changes, with females closing the gap with males as they gain in years.7,8
Biological, evolutionary and cultural reasons can explain this double pattern, say López et al. According to these authors, the most important shift that has occurred in our society in recent years is that women can take the initiative in sex, can freely agree or refuse, and have ceased to conform with the role assigned to them by traditional societies: “say no to men unless it is in the context of heterosexual marriage and with the purpose of having children.”8
Alcohol and other drugs
One of the most extensively studied risk factors for early sexual debut is alcohol and substance use. Several studies demonstrate that there is a tendency to increased drug use when there is perceived potential for sexual encounters in night recreational settings. Many young individuals appreciate substances (especially alcohol, but also others like marihuana, cocaine or MDMA) for their role in facilitating sexual exploits, and use them for a wide range of objectives that go from loosening up to complete loss of inhibition. When interviewed for a recent study, adolescents admitted that the best way to hook up was to go straight to specific venues where they know patrons are commonly under the influence of drugs or alcohol.10,11
Alcohol is the substance preferred by adolescents because it facilitates sex and engagement in riskier behaviours and increases arousal. The second most-valued substance is cocaine because it helps prolong sexual intercourse.
But there is also evidence of the negative repercussions of the association between substance use and sexual activity. These are due to the lowered risk perception that results from using these substances, which increases the probability of engaging in unprotected sex and in turn results in a greater number of unwanted pregnancies and sexually transmitted diseases.12 Drug use is also associated with ephemeral sexual experiences such as "one-night stands".13
The National Institute on Alcohol Abuse and Alcoholism of the United States has reported that individuals with alcohol use disorders have a higher probability of becoming infected by human immunodeficiency virus (HIV) and acquiring other sexually transmitted diseases than the general population due to having unprotected sex, multiple partners, sex with sex workers, and sex in exchange for alcohol or drugs.14
Calafat et al conducted two studies that concluded that women are more aware than men of the risks involved in having sex under the influence of alcohol, yet this was not associated with taking preventive measures. We ought to mention that they found an association between alcohol use and engagement in risk behaviours, especially in first-time sexual experiences.10,11 A recent study showed that while women used drugs less and were more aware of potential negative consequences, there was no difference between the sexes in the use of condoms or birth control methods nor in engagement in sexual activity they later regretted, although males did have sex under the influence of alcohol or drugs more often.11
Our data are consistent with other studies that support that the use of substances such as alcohol, marihuana, cocaine or MDMA before age 16 years is associated with sexual debut at younger ages. Furthermore, adolescents that used drugs in the context of partying had had more sexual partners, and may have even bought sex.12 There is also evidence of a positive correlation between drug use and the use of emergency contraception.15
Drug use is known to loosen sexual inhibitions and consequently leads to engaging in reckless and unprotected sexual activity. In a recent study, 46.75% of adolescents acknowledged that drugs and alcohol had played a role in their engagement in unprotected sex. Yet, in the 12 months preceding the survey, 8.2% had engaged in sexual activity that they came to regret due to substance use, and 24.5% had been tested for STIs, which demonstrates awareness of the risks involved in engaging in these sexual behaviours.
The relaxation, euphoria, disinhibition, loss of self-control and lowered risk perception induced by psychoactive substances lead individuals that use them to be less careful and forget the safe-sex messages that they would have put into practise had they remained sober.13
Our data are consistent with all of the above: we found a clear association between sexual behaviour in adolescents and alcohol and drug use. Thus, adolescents that used alcohol and drugs were more likely to have had earlier sexual debuts, had more sexual partners and engaged in more high-risk sexual behaviours compared to peers that did not use alcohol and drugs.13
Family dysfunction
Our study found that children who did not have good relationships with their parents and 14-year-old children of divorced parents had their first sexual intercourse at earlier ages. According to the international literature, children raised by both parents and children living in two-parent households engage less in sexual activity and have their sexual debut at older ages. On the other hand, a poor parent-child relationship, poor family communication and having been born to adolescent mothers or fathers, or in short, family dysfunction, is associated with sexual debut before 15 years of age.16
There is also evidence that lack of parental supervision and parent-child communication, and the degree to which parents accept sexual activity in their children are important determinants of early sexual activity.
A recent study found a significantly greater percentage of adolescents that had had intercourse among the adolescents that did not seek information from their parents. Its results showed that adolescents that had frequent discussions with their parents about love and infatuation and about topics related to sexual biology, such as the sexual changes they experience, were less likely to have had sexual intercourse.17
Thus, it seems that involving the parents should be a priority in any programme for the prevention of adolescent pregnancy.16
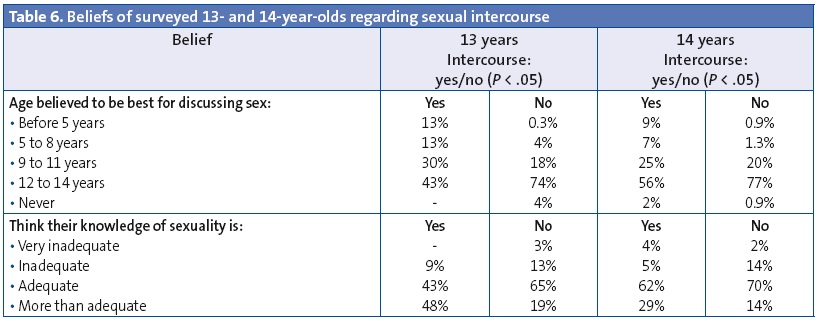
They believe that they have adequate knowledge of sex
Compared to peers that had not had sexual intercourse, adolescents aged 13 and 14 years who have had sex were more likely to state that they knew enough about sex. This fact is in contradiction with different studies that report a positive correlation between having a later sexual debut and having greater knowledge of STDs and the prevention of unwanted pregnancy.
Their belief that they know more than enough about sex is reason to be concerned. Various studies demonstrate that most adolescents do not know much about sexuality,18 and there is fear that the overconfidence of those who are sexually active may lead to an increase in the incidence of STDs and unwanted pregnancies.
Less religious
Our study found statistically significant differences in early sexual behaviour in 13-year-old adolescents that identify as nonreligious, agnostic or atheists. Thus, it seems greater involvement in Catholic religion is associated to a later start in sexual relations. This is consistent with the findings of other studies.17,19 Other authors have found that even parental religiosity is positively correlated to a late sexual debut in both sexes.16
More erotophilic
Erotophilia is positively correlated to a greater frequency of autoerotic activity, a greater number of past sexual experiences and a greater number of sexual partners. It makes sense that the most erotophilic adolescents have earlier sexual debuts.20 The silver lining is that, according to the scientific literature, more erotophilic individuals are more attentive to, process and remember sexual information to a greater extent, and anticipate the possibility of having sex and avail themselves of contraceptive methods, all of them skills that are effective in the prevention of risk behaviours.7
CONCLUSIONS
Early sexual behaviour in the adolescent population is strongly correlated to drug, alcohol and tobacco use. It is also associated with higher degrees of erotophilia and with male sex.
Furthermore, adolescents that have had sexual intercourse believe that they are very knowledgeable (even more than enough) in matters concerning sexuality, which raises the concern that they may use protective measures even less.
Another factor that is clearly associated with early sexual behaviour is poor parent-child relationship quality. This may be the area in which paediatricians, educators, the authorities and above all parents may have the chance to intervene to promote healthy sexual behaviours in adolescents. It is a challenging task, but the alternative is much more daunting.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation with the preparation and publication of this article.
FUNDING
The Paediatrics Department of the Universidad de Valladolid applied funds received from Ágora Estudios de Mercado for recording the data in this study.
ABBREVIATIONS: ESO, compulsory secondary education; HIV, human immunodeficiency virus; STD, sexually transmitted disease.
REFERENCES
- Resultados de la Encuesta Nacional de Salud Sexual 2009. Ministerio de Sanidad y Política Social [on line] [consulted on 12/06/2015]. Available in www.msps.es/organizacion/sns/planCalidadSNS/docs/v5_presentacion_ResultadosENSS_16dic09.pdf
- Calatrava M, López-Del Burgo C, de Irala J. Factores de riesgo relacionados con la salud sexual en los jóvenes europeos. Med Clin (Barc). 2012;138:534-40.
- Rodríguez-Carrión J, Traverso Blanco CI. Conductas sexuales en adolescentes de 12 a 17 años de Andalucía. Gac Sanit. 2012;26:519-24.
- Junta de Castilla y León. Portal de Educación [on line] [consulted on 01/07/2012]. Available in www.educa.jcyl.es/es/informacion/estadistica-ensenanza-universitaria/curso-2010-2011
- Casal J, Mateu E. Tipos de muestreo. Rev Epidemiol Med Prev. 2003;1:3-7.
- Pérez López C. Muestreo estadístico. Conceptos y problemas resueltos. Madrid: Pearson Educación; 2005.
- García-Vega E, Menéndez Robledo E, García Fernández P, Rico Fernández R. Influencia del sexo y del género en el comportamiento sexual de una población adolescente. Psicothema. 2010;22:606-12.
- López F, Carcedo R, Fernández Rouco N, Blázquez MI, Kilani A. Diferencias sexuales en la sexualidad adolescente: afectos y conductas. An Psicología. 2011;27:791-9.
- Bermúdez MP, Teva I, Buela-Casal G. Influencia de variables sociodemográficas sobre los estilos de afrontamiento, el estrés social y la búsqueda de sensaciones sexuales en adolescentes. Psicothema. 2009;21:220-6.
- Calafat A, Juan M, Becoña E, Mantecón A. Qué drogas se prefieren para las relaciones sexuales en contextos recreativos. Adicciones. 2008;20:37-48.
- Calafat A, Juan M, Becoña E, Mantecón A, Ramón A. Sexualidad de riesgo y consumo de drogas en el contexto recreativo. Una perspectiva de género. Psicothema. 2009;21:227-33.
- Begoña Iglesias E, López-Durán A, Fernández del Río E, Martínez Pradeda U, Osorio López J, Fraga Ares J, et al. Borracheras, conducción de vehículos y relaciones sexuales en jóvenes consumidores de cocaína y éxtasis. Adicciones. 2011;23:205-18.
- Lomba L, Apóstolo J, Mendes F. Consumo de drogas, alcohol y conductas sexuales en los ambientes recreativos nocturnos de Portugal. Adicciones. 2009;21:309-26.
- Castaño Pérez GA, Arango Tobon E, Morales Mesa S, Rodríguez Bustamante A, Montoya Montoya C. Consumo de drogas y prácticas sexuales de los adolescentes de la ciudad de Medellin (Colombia). Adicciones. 2012;24:347-54.
- López-Amorós M, Schiaffino A, Moncada A, Pérez G. Factores asociados al uso autodeclarado de la anticoncepción de emergencia en la población escolarizada de 14 a 18 años de edad. Gac Sanit. 2010;24:404-9.
- González E, Molina T, Montero A, Martínez V. Factores familiares asociados al inicio sexual temprano en adolescentes consultantes en un centro de salud sexual y reproductiva en Santiago de Chile. Rev Med Chile. 2013;141:313-9.
- Ruiz-Canela M, López-del Burgo C, Carlos S, Calatrava M, Osorio A, de Irala J. Familia, amigos y otras fuentes de información asociadas al inicio de las relaciones sexuales en adolescentes de El Salvador. Rev Panam Salud Pública. 2012;31:54-61.
- Espada JP. Validación de una escala de conocimiento sobre el VIH y otras infecciones de transmisión sexual en población adolescente. Aten Primaria. 2014;46:558-65.
- Sierra JC, Vallejo-Medina P, Santos-Iglesias P, Lameiras Fernández M. Validación del Massachusetts General Hospital-Sexual Functioning Questionnaire (MGH-SFQ) en población española. Aten Primaria. 2012;44:516-26.
- Carpintero E, Fuertes A. Validación de la versión en español del “Sexual Opinion Survey” (SOS). Cuadernos de Medicina Psicosomática. 1994;31:52-61.