

Influencia del sexo y el tipo de escuela sobre los índices de sobrepeso y obesidad
Daniel Arriscado Alsinaa, José Joaquín Muros Molinab, Mikel Zabala Díazc, José M.ª Dalmau Torresa
aDepartamento de Ciencias de la Educación. Universidad de La Rioja. Logroño. España.
bDepartamento de Nutrición y Bromatología. Universidad de Granada. Granada. España.
cDepartamento de Educación Física y Deportiva. Universidad de Granada. Granada. España.
Correspondencia: D Arriscado. Correo electrónico: danielarriscado@hotmail.com
Cómo citar este artículo: Arriscado Alsina D, Muros Molina JJ, Zabala Díaz M, Dalmau Torres JM. Influencia del sexo y el tipo de escuela sobre los índices de sobrepeso y obesidad. Rev Pediatr Aten Primaria. 2014;16:e139-e146.
Publicado en Internet: 14-11-2014 - Número de visitas: 27408
Resumen
Introducción: el sobrepeso y la obesidad infantiles han pasado a ser, en las últimas décadas, una epidemia que afecta especialmente a los países desarrollados. Cada vez son más las repercusiones negativas sobre la salud que tienen relación con la obesidad infantil. El objetivo de este estudio fue determinar las prevalencias de sobrepeso y obesidad de una ciudad del norte de España, así como identificar los factores que influyen en la misma y la relación existente con la tensión arterial.
Material y métodos: el estudio se llevó a cabo sobre una muestra representativa compuesta por 329 escolares de sexto curso de primaria (11-12 años) de la ciudad de Logroño (La Rioja, España). Se obtuvieron datos sociodemográficos, tensión arterial, desarrollo madurativo, índice de masa corporal, perímetros de cadera y cintura, y pliegues de tríceps y subescapular.
Resultados: en todas las medidas antropométricas se encontraron diferencias significativas entre los normopesos y los sobrepesos/obesos. Las prevalencias de sobrepeso y obesidad, según referencias internacionales, fueron del 23,7 y el 3,3%, respectivamente. Estas prevalencias fueron mayores en niños y en alumnos de las escuelas públicas. Se encontraron relaciones significativas entre las variables antropométricas y la tensión arterial, tanto sistólica como diastólica.
Conclusiones: los índices de sobrepeso y obesidad fueron similares a los del conjunto de la nación, siendo los casos con mayor prevalencia los de alumnos de sexo masculino y los escolarizados en centros públicos.
Palabras clave
● Escuelas primarias ● Obesidad ● Presión arterial ● Sexo ● SobrepesoINTRODUCCIÓN
La obesidad es considerada una epidemia y uno de los grandes problemas del siglo XXI1, cuyas consecuencias podrían derivar en una disminución de la esperanza de vida2. En este sentido, son de especial interés los aumentos significativos sobre los porcentajes de sobrepeso y obesidad infantil que se han registrado en las últimas décadas en la mayoría de los países desarrollados y en vías de desarrollo3. En lo que a España se refiere, cabe destacar que es uno de los países con mayores índices de sobrepeso y obesidad infantil de Europa4, y, más concretamente, La Rioja posee una prevalencia de obesidad infantil ligeramente superior a la media nacional, con un 9,7%5. Estos informes resultan alarmantes en la medida en que se ha establecido una clara relación entre el exceso de peso en las primeras etapas de la vida con el mantenimiento de dicho exceso tanto en la adolescencia6 como en la edad adulta7.
Cada vez son más los estudios que relacionan el sobrepeso en la infancia con un perfil lipídico menos saludable8, resistencia a la insulina y diabetes tipo 29 o dificultades psicosociales10. Además, favorece la incidencia del síndrome metabólico11, entendido este como un conjunto de factores de riesgo de enfermedad cardiovascular, entre los que se incluye la hipertensión arterial12. Diferentes estudios señalan los comportamientos sedentarios13, la falta de actividad física14, especialmente vigorosa15, y los hábitos de alimentación contemporáneos16, como los principales causantes de la acumulación excesiva de grasa. Sin embargo, dichos hábitos están a su vez condicionados por múltiples factores. Algunos de los más importantes son los determinantes sociodemográficos17, como el sexo, el nivel socioeconómico o el tipo de escuela al que se asiste. No obstante, también se han encontrado relaciones con el peso neonatal y el periodo de lactancia18, las características antropométricas de los progenitores y sus hábitos19, las horas de sueño20, los medios de comunicación21 u otros22. El estudio de estos factores resulta determinante de cara a elaborar programas de intervención eficaces.
Sin embargo, la mayoría de las investigaciones se han centrado en la población adolescente, siendo menor la bibliografía referente a estudios con niños más jóvenes. Además, los altos índices de obesidad infantil encontrados en nuestro país en los últimos años hacen preciso un continuo seguimiento que determine la eficacia de las actuaciones llevadas a cabo. De este modo, el objetivo de este estudio fue determinar los índices de prevalencia de sobrepeso y obesidad infantil de una población representativa de escolares de sexto de primaria (11-12 años) de Logroño. Además, se analizaron los factores sociodemográficos determinantes en el exceso de peso, así como la relación existente entre el mismo y la tensión arterial de los escolares.
MATERIAL Y MÉTODOS
Participantes
Se diseñó un estudio transversal con una muestra representativa de los alumnos escolarizados en sexto curso de Educación Primaria de la ciudad de Logroño (España). Los datos para ese intervalo de edad durante el curso 2011-2012 comprendían 1595 alumnos. Asumiendo un error del 5% y sobrestimando la participación en un 20%, la selección de los escolares se realizó a través de un muestreo aleatorio simple entre todos los centros educativos públicos y concertados de la ciudad, siendo la participación del 88,4% lo que supuso un total de 329 alumnos. La investigación se llevó a cabo durante la primavera de 2012 en cada una de las escuelas de la ciudad.
Todos los alumnos participaron de manera voluntaria y respetando el acuerdo sobre ética de investigación de Helsinki. Se solicitó el consentimiento informado de los padres o tutores de los alumnos. El Comité Ético de Investigación Clínica de La Rioja aprobó este estudio.
Datos sociodemográficos
Los propios participantes del estudio informaron mediante cuestionario de su sexo, fecha de nacimiento y país de origen. La clasificación de escuelas públicas o concertadas fue facilitada por la Consejería de Educación del Gobierno de La Rioja. El nivel socioeconómico y sociocultural de los alumnos se determinó en función de la información recogida en el Proyecto Educativo del centro al que asistían, dividiéndolo en las siguientes categorías: bajo, medio-bajo, medio, medio-alto y alto. No obstante, no se registraron alumnos con un nivel alto y se agruparon las categorías “bajo” y “medio-bajo”, dado el escaso número de escolares que se encontraban en la primera de ellas.
Medidas antropométricas
Todas las medidas antropométricas fueron tomadas siguiendo el protocolo establecido por la International Society for the Advancement of Kinanthropometry23 y por un único evaluador experimentado, acreditado como nivel II por la citada entidad.
El peso se determinó con una balanza SECA® (713, Hamburg, Alemania), con una precisión de 0,1 kg. Para la talla se empleó un tallímetro Holtain® (Holtain Ltd., Dyfed, Reino Unido), con una precisión de un milímetro. A partir de estos datos, se calculó el índice de masa corporal (IMC) como el peso dividido por la altura al cuadrado (kg/m2). El sobrepeso y la obesidad fueron definidos de acuerdo a los criterios internacionales24.
Los perímetros de cintura y cadera fueron medidos con una cinta de acero flexible Lufkin® (Lufkin W606 PM, Michigan, EE. UU.) de 0,1 cm de precisión. Posteriormente, se calculó el cociente entre cintura y cadera.
Se midieron los pliegues cutáneos de tríceps y subescapular con un plicómetro Holtain® (Holtain Ltd., Crosswell, Reino Unido), con una precisión de 0,2 mm y una presión constante de 10 g/mm2. El porcentaje de masa grasa se estimó mediante las ecuaciones de Slaugther25.
Maduración sexual
El nivel de maduración sexual fue determinado por investigadores entrenados, del mismo sexo que el alumno y a través de dos procedimientos diferentes:
- Por un lado, los niños autoevaluaron su estado madurativo identificando su desarrollo genital y vello púbico, mientras que las niñas hicieron lo propio con su desarrollo mamario y vello púbico. De este modo, todos los escolares determinaron el estadio madurativo en que se encontraban según la metodología descrita por Tanner26.
- Por otro lado, se estableció la “edad al pico de crecimiento”, un método más objetivo de hallar el nivel de desarrollo mediante ecuaciones que toman como referencia la edad cronológica, el sexo y una serie de medidas antropométricas27.
Presión arterial
Los niveles de presión arterial sistólica (PAS) y diastólica (PAD) se determinaron mediante un esfigmomanómetro aneroide Riester® (Minimus III, Jungingen, Alemania) calibrado y un estetoscopio. Las medidas se realizaron con los alumnos en sedestación, tras más de cinco minutos de reposo previo y con un brazalete adaptado al tamaño del brazo, tal y como indican las recomendaciones internacionalmente aceptadas para la valoración en niños28.
Personal titulado y experimentado fue el responsable de tomar la PAS y PAD en los dos brazos de cada uno de los participantes. Se registraron las medidas en milímetros de mercurio (mmHg).
Análisis estadístico
Las variables cuantitativas se presentan con la media y su desviación típica, mientras que las cualitativas según su distribución de frecuencias.
La asociación de las variables cualitativas se analizó mediante el test Chi-cuadrado de Pearson. En el caso de que el número de celdas con valores esperados menores de cinco fuera mayor de un 20%, se utilizó el test exacto de Fisher o el test Razón de verosimilitud para variables con más de dos categorías.
La normalidad de los datos fue analizada usando el test de Kolmogorov-Smirnov y, en el caso de muestras pequeñas (n<30), el test de Shapiro-Wilk. Las comparaciones de los valores cuantitativos se realizó mediante la prueba T de Student o el ANOVA de un factor para muestras independientes según si el número de grupos a comparar fue de dos o de más de dos. Estas pruebas fueron aplicadas para variables con distribución normal, el resto fueron analizadas mediante las pruebas U de Mann-Whitney y Kruskal Wallis, respectivamente.
Dentro del ANOVA de un factor se utilizó la prueba robusta para la igualdad de medias de Welch y, como pruebas a posteriori, la prueba de Bonferroni o la de Tamhane, en función de si las varianzas de los grupos a comparar eran iguales o no.
Los datos fueron analizados con el programa estadístico IBM-SPSS® versión 20,0 para Windows®. El nivel de significación se estableció en 0,05.
RESULTADOS
Los resultados del estudio reflejan las características antropométricas de una muestra representativa de escolares de 11-12 años de Logroño. La edad, el desarrollo madurativo, la presión arterial y las características antropométricas en función del sexo, y la presencia o no de sobrepeso u obesidad, se recogen en la Tabla 1. Según el tipo de centro, no se encontraron diferencias significativas en ningún parámetro a excepción de la edad, ligeramente superior en los alumnos de la escuela pública (11,8±0,4 años frente a 11,7±0,4 años). En lo referente a la nacionalidad, se dieron diferencias significativas entre los alumnos españoles y extranjeros, que constituían el 17,3% de la muestra, en los siguientes parámetros: edad (11,7±0,3 años frente a 12,0±0,5 años), desarrollo de Tanner (estadio 2,3±0,6 frente a estadio 2,7±0,7), edad al pico de crecimiento (-2,5±0,4 años frente a -2,3±0,5 años) y talla (149,3±6,7 cm frente a 151,0±8,3 cm).
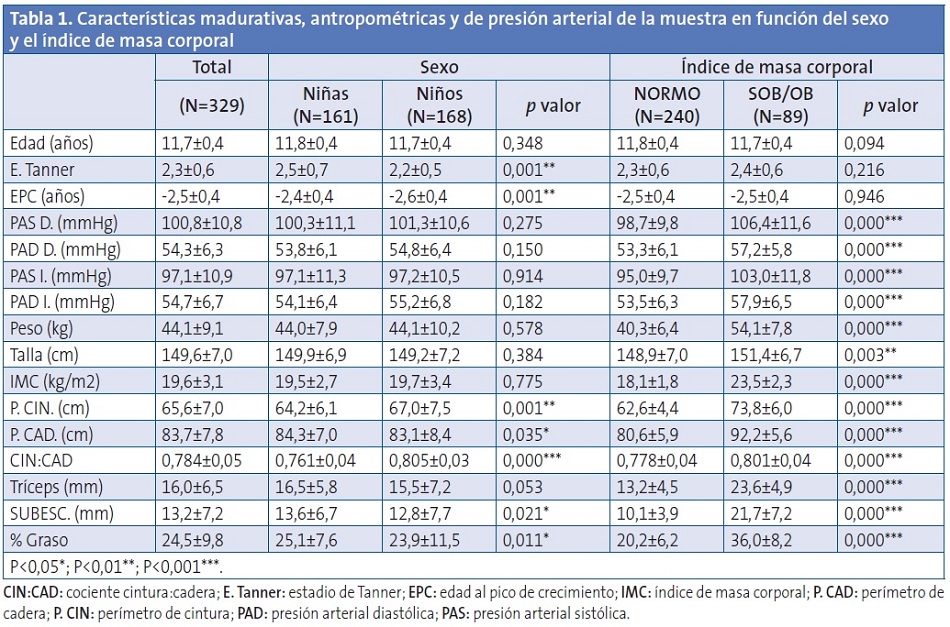
En función del sexo, existieron diferencias significativas en el desarrollo de Tanner (estadio 2,5±0,7 en niñas por estadio 2,2±0,5 en niños), la edad al pico de crecimiento (-2,4±0,4 años frente a -2,6±0,4 años), el perímetro de cintura (64,2±6,1 cm frente a 67,0±7,5 cm), el perímetro de cadera (84,3±7,0 cm frente a 83,1±8,4 cm), el cociente cintura:cadera (0,8±0,1 frente a 0,8±0,0), el pliegue subescapular (13,6±6,7 mm frente a 12,8±7,7 mm) y el porcentaje de grasa (25,1±7,6% frente a 23,9±11,5%), siendo todos los valores superiores para el género femenino, excepto el perímetro de la cintura. Según las directrices de la International Diabetes Federation para niños de 10 a 16 años29, y tomando como referencia las tablas del estudio nacional EnKid30, únicamente un 0,6% de las niñas y un 4,8% de los niños presentaron valores de riesgo de síndrome metabólico en función de su perímetro de cintura.
Según la clasificación en “normopeso” y “sobrepeso-obeso”, se encontraron diferencias significativas en todas las variables antropométricas y en los valores de presión arterial, obteniendo valores más altos el grupo compuesto por niños con sobrepeso u obesos en todos los casos. En este sentido, se registraron relaciones significativas (p<0,01) entre las variables antropométricas y la tensión arterial, tanto para la PAS como para la PAD y tanto en niños como en niñas. Las mayores correlaciones se dieron entre la PAS y el peso (r=0,42 en el brazo derecho y r=0,43 en el izquierdo), el perímetro de cintura (r=0,40 y r=0,38) y el IMC (r=0,33 a 0,35).
Las diferencias entre los valores de presión arterial para ambos brazos fueron de 5,4±3,8 mmHg para la PAS y de 4,0±4,2 mmHg para la PAD, con valores máximos de 15 mmHg, comunicados por nueve escolares en el caso de la PAS y por ocho en el de la PAD. Además, según la International Diabetes Federation29, únicamente a dos alumnos (menos de un 1%), uno obeso y otro con sobrepeso, se les detectó hipertensión arterial.
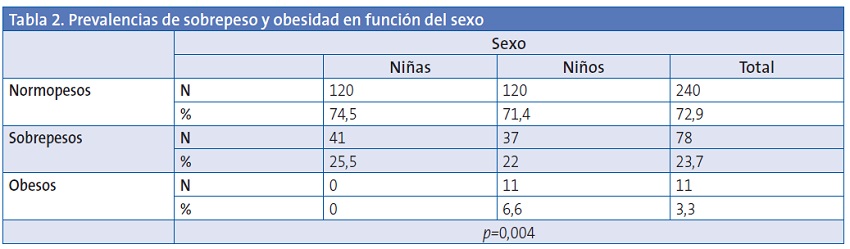
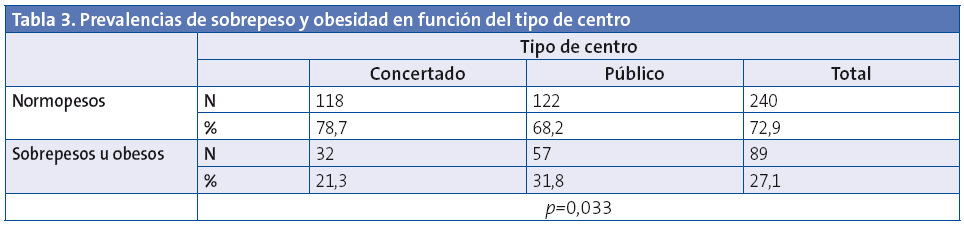
La Tabla 2 refleja la distribución de niños y niñas en normopesos, sobrepesos y obesos. A pesar de que los porcentajes son similares en los grupos de normopesos y sobrepesos, no hubo ninguna mujer obesa, mientras que el 6,5% de los hombres sí lo fue. Siguiendo con el análisis de los factores determinantes sobre el exceso de peso, la Tabla 3 nos indica que el tipo de centro también es un aspecto influyente, siendo la prevalencia de alumnos sobrepesos y obesos en las escuelas concertadas menor que en las públicas (odds ratio [OR]=0,58). No existieron diferencias significativas en relación a la nacionalidad, el nivel socioeconómico o el nivel sociocultural de los alumnos.
DISCUSIÓN
Los resultados indicaron que tanto el sexo como el tipo de escuela influyen sobre la prevalencia de sobrepeso y obesidad, encontrándose que el hecho de ser niño está relacionado con un mayor riesgo de ser obeso, de la misma manera que asistir a un colegio público se asocia con mayores posibilidades de padecer sobrepeso u obesidad en niños escolarizados en sexto curso. En relación al sexo, a pesar de que el porcentaje de normopesos fue ligeramente superior en las niñas, se observaron grandes diferencias en la presencia de obesidad. Aunque una tendencia similar se había encontrado anteriormente a nivel nacional en jóvenes de 10 a 14 años5, con una tasa de obesidad del 4,3% en chicos y del 3,0% en chicas, cabe destacar que en la muestra del estudio ninguna chica padecía obesidad.
Por otro lado, se obtuvieron diferencias significativas en función del tipo de escuela, siendo menores los porcentajes de alumnos sobrepesos u obesos en los centros concertados con respecto a los públicos (OR=0,58). Dada la relación que encontramos entre el tipo de escuela y el nivel socioeconómico (p=0,000), es posible que estos resultados manifiesten una notable diferencia entre la red pública y concertada en nuestra región, ya que la misma tendencia se encontró en estudios previos31, pero con valores menos acusados (OR=0,85). Sin embargo, nuestros resultados no mostraron diferencias en función del nivel socioeconómico de los escolares, aunque este no se valoró de forma individual. En una importante revisión17, se encontraron relaciones inversas entre el nivel económico y la adiposidad en el 42% de los artículos analizados, mientras que no fue así en el 27%.
Nuestro estudio estableció que el 23,7% de los escolares padece sobrepeso y el 3,3% obesidad. En los últimos años, se han realizado investigaciones similares con muestras de escolares no representativas de otras ciudades de España como, por ejemplo, Oviedo32, obteniendo porcentajes de obesidad del 8,4%. Dado que ambas poblaciones se ubican en el Norte de España, las diferencias podrían deberse a la no representatividad de la muestra o al mayor margen de edad de la población allí estudiada. Sin embargo, dos son las grandes investigaciones a nivel nacional en este sentido: el estudio EnKid33, que, en la franja de edad de 10-13 años, mostró unos porcentajes de sobrepeso y obesidad del 22 y el 5%, respectivamente; y la última Encuesta de Salud Nacional realizada en nuestro país5, que reveló unos porcentajes del 19,2% de sobrepeso y el 3,7% de obesidad en la población de 10-14 años. En ambos casos se puede observar que los porcentajes de niños con sobrepeso y obesidad fueron similares a los del estudio realizado, lo que indica una estabilización de los porcentajes en los últimos años. No obstante, dichos porcentajes siguen siendo muy elevados, ya que más del 25% de los escolares de 11-12 años de la ciudad padece sobrepeso u obesidad, lo que resulta especialmente grave si se tienen en cuenta las consecuencias negativas que esto implica sobre la salud presente y futura de los mismos. No se debe olvidar que los países del sur de Europa, entre los que se encuentra España, comunicaron prevalencias de obesidad infantil entre el 6 y el 19%, cifras muy lejanas al 2-4% de los países del norte22.
En lo que a porcentaje de grasa se refiere, Williams34 estableció como valores de corte saludables el 25% en niños y el 30% en niñas. En la muestra estudiada, el 35% de los niños y el 27% de las niñas superaron los citados porcentajes de grasa. En una investigación llevada a cabo en EE. UU.35, la media de grasa corporal para el grupo de edad estudiado fue de 18,6% y de 23,1% para niños y niñas, respectivamente. En ambos casos por debajo de los resultados obtenidos en nuestra muestra. En función del sexo, las niñas presentaron mayor porcentaje de grasa, como ya se había constatado anteriormente6.
En cuanto a la presión arterial, encontramos relaciones significativas entre todas las medidas antropométricas (excepto el cociente cintura:cadera) y la presión arterial, tanto sistólica como diastólica, lo cual ya había sido descrito en una investigación realizada sobre niños y adolescentes chinos2. En la misma, la presión arterial aumentaba entre 1,4 y 4,1 mmHg por cada incremento de la desviación estándar del peso, IMC y talla. No obstante, el estudio más semejante, por edad cronológica y localización de la muestra, es el European Youth Heart Study12, en el que se valoraron la presión y las medidas antropométricas de niños europeos de nueve y diez años. En dicho estudio, las relaciones significativas entre antropometría y presión arterial se dieron especialmente con la PAS (r=0,21 con IMC, r=0,29 con perímetro de cintura). Aunque nuestros resultados mostraron mayores coeficientes de correlación, lo cual puede deberse a la edad superior de la muestra, las asociaciones fueron igualmente superiores con la PAS, tanto en niños como en niñas. No obstante, cabe destacar que solo dos alumnos padecían hipertensión (menos de un 1% de la población) y que ninguno reportó diferencias entre ambos brazos de más de 15 mmHg en la medida de la presión arterial, lo que podría ser indicador de riesgo vascular36.
CONCLUSIONES
Los resultados indicaron que los índices de sobrepeso y obesidad en escolares de la ciudad de Logroño fueron similares a la media del país en la última década, siendo los casos con mayor prevalencia los de alumnos de género masculino y los escolarizados en centros públicos. La elevada prevalencia pone de manifiesto la necesidad de programas de intervención que deberían enfocarse hacia estos grupos de mayor riesgo.
FINANCIACIÓN
El estudio fue parcialmente financiado por el Instituto de Estudios Riojanos del Gobierno de La Rioja mediante “Resolución n.º 55, de fecha de 20 de agosto de 2012 de la Gerente del Instituto de Estudios Riojanos por la concesión de ayudas para estudios científicos de temática riojana del año 2012”.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS: IMC: índice de masa corporal • mmHg: milímetros de mercurio • OR: odds ratio • PAD: presión arterial diastólica • PAS: presión arterial sistólica.
BIBLIOGRAFÍA
- Blair SN. Physical inactivity: The biggest public health problem of the 21st century. Br J Sports Med. 2009;43:1-2.
- Ma J, Wang Z, Dong B, Song Y, Hu P, Zhang B. Quantifying the relationships of blood pressure with weight, height and body mass index in Chinese children and adolescents. J Paediatr Child Health. 2012;48:413-8.
- Wang Y, Lobstein T. Worldwide trends in childhood overweight and obesity. Int J Pediatr Obes. 2006;1:11-25.
- Lobstein T, Frelut M. Prevalence of overweight among children in Europe. Obes Rev. 2003;4:195-200.
- Encuesta Nacional de Salud 2011-2012. Madrid: Instituto Nacional de Estadística. Ministerio de Sanidad, Servicios Sociales e Igualdad; 2012.
- Brouwer SI, Stolk RP, Liem ET, Lemmink KA, Corpeleijn E. The role of fitness in the association between fatness and cardiometabolic risk from childhood to adolescence. Pediatr Diabetes. 2013;14:57-65.
- Freedman DS, Mei Z, Srinivasan SR, Berenson GS, Dietz WH. Cardiovascular risk factors and excess adiposity among overweight children and adolescents: The Bogalusa Heart Study. J Pediatr. 2007;150:12-7.
- Bell LM, Curran JA, Byrne S, Roby H, Suriano K, Jones TW, et al. High incidence of obesity co-morbidities in young children: A cross-sectional study. J Paediatr Child Health. 2011;47:911-7.
- Weiss R, Dziura J, Burgert TS, Tamborlane WV, Taksali SE, Yeckel CW, et al. Obesity and the metabolic syndrome in children and adolescents. N Engl J Med. 2004;350:2362-74.
- Zhou l, Wen SW, He G. Self-esteem situation and relative factor for obese and overweight children. Am J Epidemiol. 2011;173:S125.
- Brambilla P, Lissau I, Flodmark C, Moreno LA, Widhalm K, Wabitsch M, et al. Metabolic risk-factor clustering estimation in children: To draw a line across pediatric metabolic syndrome. Int J Obes (Lond). 2007;31:591-600.
- Ruiz JR, Ortega FB, Loit HM, Veidebaum T, Sjöström M. Body fat is associated with blood pressure in school-aged girls with low cardiorespiratory fitness: The European Youth Heart Study. J Hypertens. 2007;25:2027-34.
- Mitchell JA, Mattocks C, Ness AR, Leary SD, Pate RR, Dowda M, et al. Sedentary behavior and obesity in a large cohort of children. Obesity (Silver Spring). 2009;17:1596-602.
- Butte NF, Puyau MR, Adolph AL, Vohra FA, Zakeri I. Physical activity in non overweight and overweight Hispanic children and adolescents. Med Sci Sports Exerc. 2007;39:1257-66.
- Dencker M, Thorsson O, Karlsson MK, Lindén C, Eiberg S, Wollmer P, et al. Daily physical activity related to body fat in children aged 8-11 years. J Pediatr. 2006;149:38-42.
- Butte NF, Christiansen E, Sorensen TI. Energy imbalance underlying the development of childhood obesity. Obesity (Silver Spring). 2007;15:3056-66.
- Shrewsbury V, Wardle J. Socioeconomic status and adiposity in childhood: A systematic review of cross-sectional studies 1990-2005. Obesity (Silver Spring). 2008;16:275-84.
- Olstad DL, McCargar L. Prevention of overweight and obesity in children under the age of 6 years. Appl Physiol Nutr Metab. 2009;34:551-70.
- Brophy S, Rees A, Knox G, Baker J, Thomas NE. Child fitness and father’s BMI are important factors in childhood obesity: A school based cross-sectional study. PLoS One. 2012;7:e36597.
- Bell JF, Zimmerman FJ. Shortened nighttime sleep duration in early life and subsequent childhood obesity. Arch Pediatr Adolesc Med. 2010;164:840-5.
- Council on Communications and Media, Strasburger VC. Children, adolescents, obesity, and the media. Pediatrics. 2011;128:201-8.
- Ahrens W, Pigeot I, IDEFICS Consortium. Idefics study - Obesity prevalence and risk factors in European children. Am J Epidemiol. 2011;173:S280.
- Stewart A, Marfell-Jones M, Olds T, de Ridder H. International standards for anthropometric assessment. New Zealand: ISAK, Lower Hutt; 2011.
- Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000;320:1240-3.
- Slaughter MH, Lohman TG, Boileau RA, Stillman PJ, Van Loan MD, Bembem DA. Skinfolds equations for estimation of body fatness in children and youth. Hum Biol. 1988;60:709-23.
- Tanner JM, Whitehouse RH. Clinical longitudinal standards for height, weight, height velocity and stages of puberty. Arch Dis Child. 1976;51:170-9.
- Mirwald RL, Baxter-Jones AD, Bailey DA, Beunen GP. An assessment of maturity from anthropometric measurements. Med Sci Sports Exerc. 2002;34:689-94.
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114:555-76.
- Zimmet P, Alberti GK, Kaufman F, Tajima N, Silink M, Arslanian S, et al. The metabolic syndrome in children and adolescents - an IDF consensus report. Pediatr Diabetes. 2007;8:299-306.
- Serra L, Aranceta J, Ribas L, Sangil M, Pérez C. Crecimiento y desarrollo: dimensión alimentaria y nutricional. En: Serra L, Aranceta J (eds.). Crecimiento y desarrollo. Estudio EnKid, Krece Plus. Vol. 4, Barcelona: Masson; 2003. p. 45-54.
- Moreno LA, Tomás C, González-Gross M, Bueno G, Pérez-González JM, Bueno M. Micro-environmental and socio-demographic determinants of childhood obesity. Int J Obes Relat Metab Disord. 2004;28:S16-20.
- Martín JJ, Hernández LS, González MG, Méndez CP, Rey Galán C, Guerrero SM. Trends in childhood and adolescent obesity prevalence in Oviedo (Asturias, Spain) 1992-2006. Acta Paediatr. 2008;97:955-8.
- Aranceta J, Serra L, Foz M, Moreno B, Barbany M, Bellido D, et al. Prevalence of obesity in Spain. Med Clin (Barc). 2005;125:460-6.
- Williams DP, Going SB, Lohman TG, Harsha DW, Srinivasan SR, Webber LS, et al. Body fatness and risk for elevated blood pressure, total cholesterol, and serum lipoprotein ratios in children and adolescents. Am J Public Health. 1992;82:358-63.
- Laurson KR, Eisenmann JC, Welk GJ. Body fat percentile curves for US children and adolescents. Am J Prev Med. 2011;41:S87-92.
- Clark CE, Taylor RS, Shore AC, Ukoumunne OC, Campbell JL. Association of a difference in systolic blood pressure between arms with vascular disease and mortality: A systematic review and meta-analysis. Lancet. 2012;379:905-14.