
Vol. 16 - Num. 61
Documento de consenso
Calendario de vacunaciones de la Asociación Española de Pediatría: recomendaciones 2014
David Moreno Péreza, FJ Álvarez Garcíab, J Arístegui Fernándezc, M.ª José Cilleruelo Ortegad, JM Corretger Rauet, Nuria García Sánchezf, Ángel Hernández Merinog, Teresa Hernández-Sampelayo Matosh, M Merino Moina, L Ortigosa del Castilloi, J Ruiz-Contreras, Comité Asesor de Vacunas de la Asociación Española de Pediatría
aInfectología Pediátrica e Inmunodeficiencias. Unidad de Gestión Clínica de Pediatría. Hospital Materno-Infantil. Hospital Regional Universitario de Málaga. Grupo de Investigación IBIMA. Facultad de Medicina. Universidad de Málaga. Málaga. España.
bPediatra. CS de Llanera. Departamento de Medicina. Universidad de Oviedo. Asturias. España.
cUnidad de Infectología Pediátrica. Hospital Universitario de Basurto. Departamento de Pediatría. Facultad de Medicina de la Universidad del País Vasco (UPV/EHU). Bilbao. España.
dServicio de Pediatría. Hospital Universitario Puerta de Hierro-Majadahonda. Facultad de Medicina. Universidad Autónoma de Madrid. Madrid. España.
fPediatra. CS Delicias Sur. Zaragoza. España.
gPediatra de Atención Primaria. Madrid. Vocal del Comité Asesor de Vacunas de la AEP. España.
hServicio de Pediatría. Hospital General Universitario Gregorio Marañón. Facultad de Medicina. Universidad Complutense de Madrid. Madrid. España.
iServicio de Pediatría. Hospital Universitario Ntra. Sra. de Candelaria. Facultad de Medicina. Universidad de La Laguna. Tenerife. España.
Correspondencia: D Moreno. Correo electrónico: dmp.malaga@gmail.com
Cómo citar este artículo: Moreno Pérez D, Álvarez García FJ, Arístegui Fernández J, Cilleruelo Ortega MJ, Corretger Rauet JM, García Sánchez N, et al. Calendario de vacunaciones de la Asociación Española de Pediatría: recomendaciones 2014. Rev Pediatr Aten Primaria. 2014;16:13-20.
Publicado en Internet: 10-02-2014 - Número de visitas: 64410
RECOMENDACIONES 2014
El Comité Asesor de Vacunas de la Asociación Española de Pediatría (CAV-AEP) actualiza anualmente el calendario de vacunaciones teniendo en cuenta tanto aspectos epidemiológicos, como de seguridad, efectividad y eficiencia de las vacunas. Estas recomendaciones van dirigidas a pediatras, médicos de familia, personal de enfermería, matronas, familiares de los niños y, en general, a todas aquellas personas interesadas en disponer de una información actualizada sobre la vacunación en la edad pediátrica.
El presente calendario para 2014 (Tabla 1) sigue incluyendo grados de recomendación. Se han considerado como vacunas sistemáticas aquellas que el CAV-AEP estima que todos los niños en España deberían recibir de forma universal; como recomendadas las que presentan un perfil de vacuna sistemática en la edad pediátrica y que el CAV-AEP considera deseable que todos los niños reciban, pero cuya prioridad, por razones de coste-efectividad, se establece en función de las posibilidades económicas de su financiación pública; y dirigidas a grupos de riesgo aquellas que se consideran indicadas para individuos en situaciones ambientales o personales que incrementen la probabilidad de presentar las enfermedades para las que van dirigidas o de sufrir formas más graves si las padeciesen, o bien porque tengan una enfermedad de base que pueda agravarse o desestabilizarse si contraen la infección.
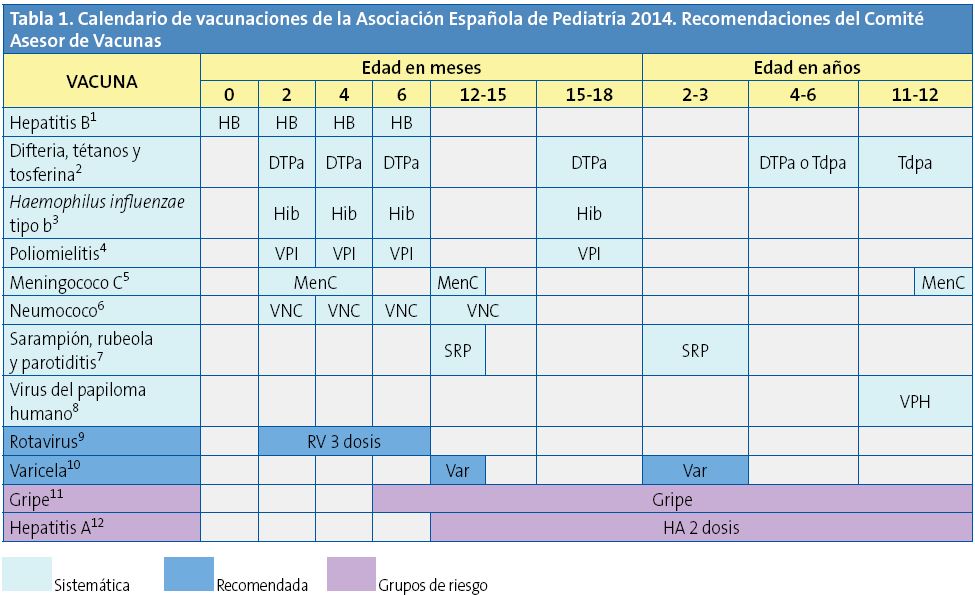
(1) Vacuna antihepatitis B (HB). 3 dosis según 3 pautas equivalentes: 0, 1, 6 meses o 0, 2, 6 meses o 2, 4, 6 meses, todas adecuadas para hijos de madres seronegativas (HBsAg-), siendo las 2 primeras pautas también adecuadas para hijos de madres portadoras del virus de la hepatitis B (HBsAg+). Estos últimos recién nacidos (madres HBsAg+) recibirán en las primeras 12 horas de vida la 1.ª dosis de vacuna y 0,5 ml de inmunoglobulina antihepatitis B, la 2.ª dosis de vacuna a la edad de 1 o 2 meses y la 3.ª dosis a los 6 meses de vida. Si la serología materna fuera desconocida deberá administrarse la 1.ª dosis de vacuna en las primeras 12 horas de vida e investigar la serología inmediatamente y, si resultara positiva, administrar 0,5 ml de inmunoglobulina antihepatitis B en la 1.ª semana de vida (preferentemente en las primeras 72 horas de vida). La administración de 4 dosis de vacuna HB es aceptable en niños vacunados de la 1.a dosis monocomponente al nacer, seguida de 3 dosis de vacuna hexavalente a los 2, 4 y 6 meses de edad. Los niños y adolescentes no vacunados recibirán, a cualquier edad, 3 dosis según la pauta 0, 1, 6 meses.
(2) Vacuna frente a la difteria, el tétanos y la tosferina acelular (DTPa/Tdpa). 6 dosis: primovacunación con 3 dosis de vacuna DTPa; refuerzo a los 15-18 meses (4.ª dosis) con DTPa; a los 4-6 años (5.ª dosis) con DTPa o con el preparado de baja carga antigénica de difteria y tosferina (Tdpa) y a los 11-12 años (6.ª dosis) con Tdpa.
(3) Vacuna conjugada frente al Haemophilus influenzae tipo b (Hib). 4 dosis: primovacunación a los 2, 4, 6 meses y refuerzo a los 15-18 meses (4.ª dosis).
(4) Vacuna antipoliomielítica inactivada (VPI). 4 dosis: primovacunación con 3 dosis y refuerzo a los 15-18 meses (4.ª dosis).
(5) Vacuna conjugada frente al meningococo C (MenC). 3 o 4 dosis de vacuna conjugada monovalente (esquema 1 o 2+1+1), con la siguiente pauta: 1 o 2 dosis entre los 2 y 11 meses de edad, otra dosis a los 12 meses de edad y otra dosis final a los 12 años. La pauta para los lactantes de 2 a 4 meses de edad, con 1 o 2 dosis, dependerá del preparado vacunal que se utilice.
(6) Vacuna conjugada frente al neumococo (VNC). 4 dosis: las 3 primeras a los 2, 4, 6 meses con un refuerzo entre los 12 y 15 meses de edad (4.ª dosis).
(7) Vacuna frente al sarampión, la rubeola y la parotiditis (SRP). 2 dosis de vacuna sarampión-rubeola-parotiditis (triple vírica). La 1.ª a los 12 meses, y la 2.ª a los 2-3 años de edad, preferentemente a los 2 años.
(8) Vacuna frente al virus del papiloma humano (VPH). Solo para niñas. 2 o 3 dosis entre los 11 y los 12 años. La tetravalente con pauta 0, 2, 6 meses y la bivalente con pauta de 2 dosis (0 y 6 meses) para niñas entre 9 y 14 años, y pauta de 3 dosis (0, 1, 6 meses) si 15 años o más.
(9) Vacuna frente al rotavirus (RV). 3 dosis de vacuna frente al rotavirus: a los 2, 4, 6 meses o a los 2, 3, 4 meses. La pauta ha de iniciarse entre las 6 y las 12 semanas de vida y debe completarse antes de las 32 semanas de edad.
(10) Vacuna frente a la varicela (Var). 2 dosis: la 1.ª a los 12 meses (es aceptable a los 12-15 meses) y la 2.ª a los 2-3 años de edad, preferentemente a los 2 años. En pacientes susceptibles fuera de las edades anteriores, vacunación con 2 dosis con un intervalo de, al menos, 1 mes.
(11) Vacuna antigripal (Gripe). Vacunación anual de pacientes con factores de riesgo y sus convivientes (mayores de 6 meses). 1 dosis en mayores de 9 años; entre 6 meses y 9 años se administrarán 2 dosis la 1.ª vez, con un intervalo de 1 mes y en los años siguientes, si persiste el factor de riesgo, vacunación anual con 1 dosis.
(12) Vacuna antihepatitis A (HA). 2 dosis, con un intervalo de 6-12 meses, a partir de los 12 meses de edad. Vacunación de pacientes con indicación por viajes internacionales a países con endemicidad intermedia o alta, o por pertenecer a grupos de riesgo.
Los calendarios de vacunaciones tienen que ser dinámicos y adaptarse a los cambios epidemiológicos que vayan surgiendo. Teniendo en cuenta los últimos cambios en la epidemiología de las enfermedades, las nuevas publicaciones sobre eficacia, efectividad y seguridad de las diferentes vacunas, así como de los cambios recientes de las fichas técnicas de algunos preparados vacunales, el CAV-AEP hace hincapié en las siguientes recomendaciones:
- Hepatitis B: se recomienda que se realice en el primer año de vida con 3 o 4 dosis, en forma de preparado comercial monocomponente o hexavalente. En niños mayores no vacunados se aplicarán 3 dosis de vacuna monocomponente, con la pauta 0, 1 y 6 meses.
- Difteria-tétanos-tosferina-poliomielitis-Haemophilus influenzae tipo b: se recomienda la primovacunación con DTPa-VPI-Hib-HB a los 2, 4 y 6 meses, siendo aceptable el empleo de la vacuna hexavalente o de la pentavalente más la vacuna monocomponente de hepatitis B. Se puede valorar adelantar la primera dosis a las 6 semanas de vida. El refuerzo con DTPa-VPI-Hib debe realizarse a los 15-18 meses, con un refuerzo posterior con DTPa o Tdpa a los 4-6 años y con Tdpa a los 11-12 años. Se recomienda la vacunación con Tdpa a la embarazada a partir de la semana 27 de gestación, y a los miembros del entorno familiar de los recién nacidos (estrategia del nido), especialmente de la madre, no previamente vacunada en el embarazo, en el puerperio inmediato.
- Meningococo C: se cambia la pauta de vacunación frente al meningococo C, pasando de un esquema 2+1 a un esquema de 3 o 4 dosis de vacuna conjugada monovalente (esquema 1 o 2+1+1), con la siguiente pauta: 1 o 2 dosis entre los 2 y los 11 meses de edad, otra dosis a los 12 meses de edad y otra dosis final a los 12 años. La pauta para los lactantes de 2 a 4 meses de edad, con 1 o 2 dosis, dependerá del preparado vacunal que se utilice.
- Neumococo: se recomienda vacunar frente al neumococo de forma sistemática a todos los niños menores de 5 años, como la mejor medida para la prevención de la enfermedad neumocócica en la infancia, siendo la vacuna neumocócica conjugada 13-valente (VNC13) la que mejor cobertura proporciona frente a los serotipos neumocócicos circulantes en España. También se hace hincapié en la necesidad de vacunar a todos los niños entre 5 y 17 años que padecen inmunodepresión u otras situaciones de riesgo (Tabla 2).
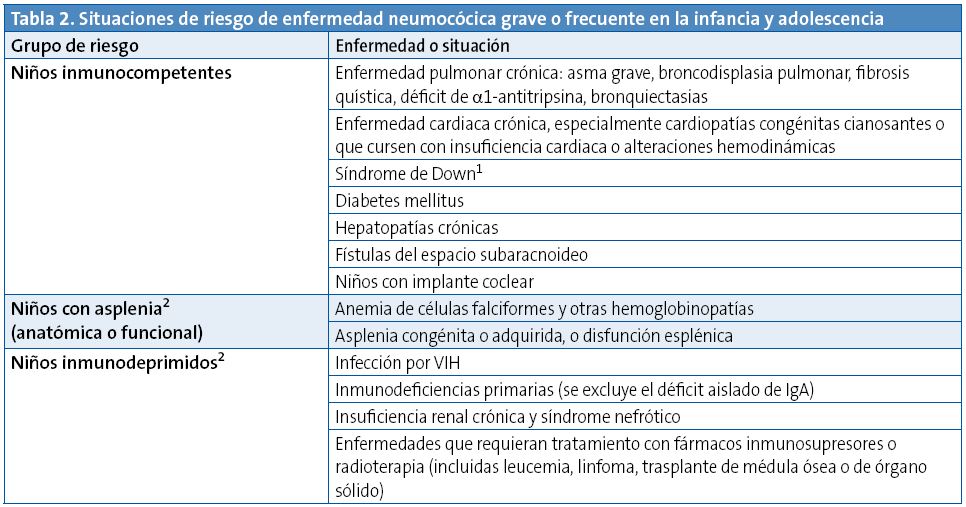
1. En el caso de documentación de alguna inmunodeficiencia de alto riesgo para ENI, seguir las recomendaciones de los niños inmunodeprimidos.
2. Pacientes de alto riesgo: deben seguir recomendaciones de vacunación antineumocócica específicas (ver texto).
- Sarampión, rubeola y parotiditis (triple vírica): se mantiene la norma general de vacunación que comprende la administración de 2 dosis, recomendando la primera a los 12 meses y la segunda a los 2-3 años de edad, preferentemente a los 2 años. En caso necesario, un intervalo mínimo de 4 semanas entre ellas asegura una correcta inmunización. Se reafirma asimismo la necesidad de alcanzar y mantener altas coberturas vacunales, para conseguir inmunidad de grupo y propiciar la eliminación de las enfermedades que previene.
- Papilomavirus humano: se recomienda la vacunación sistemática de todas las niñas de 11-12 años, como forma de prevención del cáncer cervical y de lesiones precancerosas del tracto genital en la mujer. Puede realizarse tanto con el preparado bivalente como tetravalente. Además de la pauta clásica de 3 dosis, recientemente se ha aprobado la pauta de 2 dosis (0, 6 meses) para niñas de 9 a 14 años con el preparado bivalente. Es preciso un gran esfuerzo de todos los profesionales sanitarios para incrementar las coberturas vacunales actuales.
- Rotavirus: la vacunación frente al rotavirus, dadas la morbilidad y la elevada carga sanitaria, es recomendable en todos los lactantes, con el preparado pentavalente actualmente disponible en España. Se recomienda la administración de 3 dosis. La primera se administra entre las 6 y las 12 semanas de edad. El intervalo mínimo entre dosis es de 4 semanas. Las 3 dosis deben ser administradas antes de las 32 semanas de edad. Puede administrarse al mismo tiempo que las otras vacunas del calendario.
- Varicela: la vacunación universal frente a la varicela iniciada en el segundo año de vida es una estrategia efectiva, y se solicita la inmediata disponibilidad pública de las dos vacunas existentes en España, reclamando el derecho a la prescripción y el derecho de los niños sanos a poder ser vacunados. Se recomienda la administración de la vacuna frente a la varicela a todos los niños con 2 dosis: una primera dosis a los 12 meses, y una segunda dosis a los 2-3 años, preferentemente a los 2 años.
- Gripe: se recomienda la vacunación anual en la infancia y la adolescencia en: a) grupos de riesgo: niños a partir de los 6 meses de edad y adolescentes en determinadas situaciones o enfermedades de base; b) niños sanos a partir de los 6 meses de edad y adolescentes sanos que convivan con pacientes de riesgo; y c) adultos en contacto con niños y adolescentes incluidos en los grupos de riesgo. Es especialmente importante la vacunación antigripal anual de todos los profesionales sanitarios.
- Hepatitis A: se recomienda la vacuna en ciertas situaciones de riesgo con 2 dosis, con un intervalo de, al menos, 6 meses entre ellas. Debe valorarse su administración en niños mayores de 12 meses que acuden a guardería.
La vacuna frente al meningococo B, recientemente autorizada, abre un capítulo de esperanza en la prevención de esta enfermedad. En espera de próximos estudios nacionales e internacionales se recomienda, por el momento, para el control de brotes epidémicos y se insiste en el deseo de que sea comercializada libremente en las oficinas de farmacia.
Se puede ampliar información de todos los aspectos comentados en el artículo publicado en el número de enero de 2014 de la revista Anales de Pediatría1 y en la web del CAV-AEP (www.vacunasaep.org).
POSICIONAMIENTO DEL CAV-AEP SOBRE EL CALENDARIO COMúN DE VACUNACIONES DEL MINISTERIO PARA 2014
En la actualidad, no hay diferencias epidemiológicas en las enfermedades inmunoprevenibles entre las diferentes comunidades autónomas (CC. AA.), con la posible excepción de la hepatitis A en Ceuta y Melilla, que justifiquen la existencia de calendarios de vacunaciones distintos2. El CAV-AEP estima que es necesario un esfuerzo colectivo de todos los agentes sanitarios y políticos implicados en la toma de decisiones sobre el diseño y la financiación del calendario de vacunaciones para los niños residentes en España y sigue ofreciendo su colaboración para la consecución de este sensato objetivo, y en este sentido hemos manifestado nuestra oposición al nuevo calendario común propuesto por el Consejo Interterritorial en marzo de 2013 y modificado posteriormente en diciembre de 20133 por considerarlo una propuesta que ahonda en los problemas de implantación de un calendario único en las CC. AA. y porque es insuficiente para conseguir la mejor y mayor protección de todos los niños españoles, al no contemplar la incorporación de nuevas vacunas sistemáticas, ni siquiera con un plan de futuro cuando mejoren las circunstancias económicas.
Consideramos que sería deseable que se hiciera un esfuerzo económico colectivo por parte de las CC. AA. y por el Ministerio que permitiera la financiación de un calendario sistemático completo, y no de mínimos, para los niños españoles. Se recomienda la lectura del argumentario completo que conforma el posicionamiento de este comité acerca de la implantación del calendario común del Ministerio de Sanidad, recientemente publicado en el número de enero de la revista Anales de Pediatría4.
CALENDARIOS O PAUTAS DE VACUNACIóN DE RESCATE PARA NIñOS Y ADOLESCENTES CON VACUNACIóN INCOMPLETA
En muchas ocasiones, es necesario vacunar a niños que no han recibido vacunas previamente o que no han seguido un calendario de vacunaciones de forma regular, lo han iniciado tardíamente, lo han interrumpido o han sido vacunados en sus países de origen con una pauta diferente a la indicada en España. En todos estos niños se debe realizar una adaptación al calendario de vacunación de nuestro país. Se han elaborado unas tablas para orientar en la realización de pautas de vacunación de rescate en niños y adolescentes con inmunización incompleta (Tablas 3 a 5) que conllevan cambios con respecto a las de 2013.
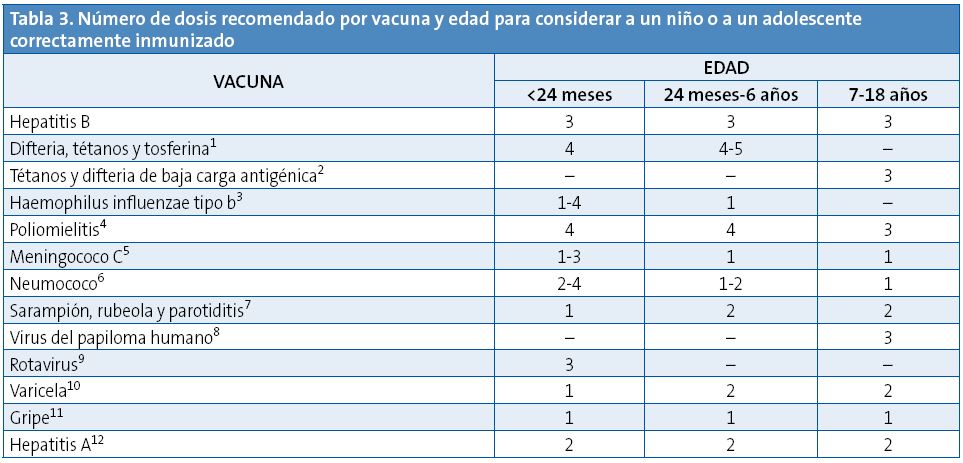
Esta tabla indica el número de dosis necesarias, según la edad, para los niños y los adolescentes con el calendario de vacunación incompleto o que comienzan la vacunación tardíamente. No se ha de reiniciar una pauta de vacunación si ya se han administrado dosis previas, sino completarla independientemente del intervalo máximo transcurrido desde la última dosis. Las reacciones adversas se deben notificar a las autoridades sanitarias.
(1) Vacuna frente a la difteria, el tétanos y la tosferina acelular (DTPa). La 5.ª dosis de DTPa o Tdpa no es necesaria si la 4.ª dosis de DTPa se administró con 4 o más años. La DTPa se puede administrar hasta los 6 años. La Tdpa, con componentes de difteria y tosferina de baja carga antigénica, está autorizada desde los 4 años de edad.
(2) Vacuna frente al tétanos y la difteria de baja carga antigénica (Td). En niños de 7 años o más administrar la vacuna de tétanos-difteria de baja carga antigénica. En las dosis de refuerzo, una vez completada la primovacunación, se recomienda utilizar la vacuna Tdpa.
(3) Vacuna conjugada frente al Haemophilus influenzae tipo b (Hib). Número de dosis según edad de inicio: 4 en menores de 6 meses; 3 entre 7-11 meses; 2 entre 12-14 meses; 1 entre 15 meses y 5 años.
(4) Vacuna antipoliomielítica inactivada (VPI). Solo si la 3.ª dosis se administró antes de los 4 años de edad se requerirá una 4.ª dosis.
(5) Vacuna conjugada frente al meningococo C (MenC). Según edad: 1 o 2 dosis, según preparado vacunal, en menores de 12 meses con 1 de refuerzo en el 2.º año de vida y otra de refuerzo en la adolescencia a los 12 años; 1 dosis en los vacunados a partir de los 12 meses de edad con 1 dosis de refuerzo en la adolescencia.
(6) Vacuna conjugada frente al neumococo (VNC). Número de dosis según edad de inicio: 4 en menores de 6 meses; 3 entre 7-11 meses; 2 entre 12-23 meses; entre 24 y 59 meses: 1 de Prevenar 13® (1 o 2 en grupos de riesgo, ver texto) y 2 de Synflorix®; entre 5 y 17 años 1 dosis de Prevenar 13® en grupos de riesgo (ver texto). Synflorix® está autorizada hasta los 5 años y Prevenar 13® hasta la edad adulta, sin límite de edad.
(7) Vacuna frente al sarampión, la rubeola y la parotiditis (SRP). 2.ª dosis a partir de los 2-3 años de edad.
(8) Vacuna frente al virus del papiloma humano (VPH). Solo para niñas. 2 o 3 dosis entre los 11 y los 12 años de edad. El Consejo Interterritorial la recomienda a los 14 años de edad.
(9) Vacuna frente al rotavirus (RV). 3 dosis de vacuna frente al rotavirus (RotaTeq®). La pauta se puede iniciar entre las 6 y las 12 semanas de edad y debe completarse antes de las 32 semanas de edad.
(10) Vacuna frente a la varicela (Var). 2.ª dosis a partir de los 2-3 años de edad.
(11) Vacuna antigripal (Gripe). 1 dosis anual de vacuna antigripal inactivada a partir de los 6 meses de edad. La primera vez que se vacune a menores de 9 años se administrarán 2 dosis con un intervalo de, al menos, un mes.
(12) Vacuna antihepatitis A (HA). 2 dosis, con un intervalo de 6-12 meses, a partir de los 12 meses de edad.
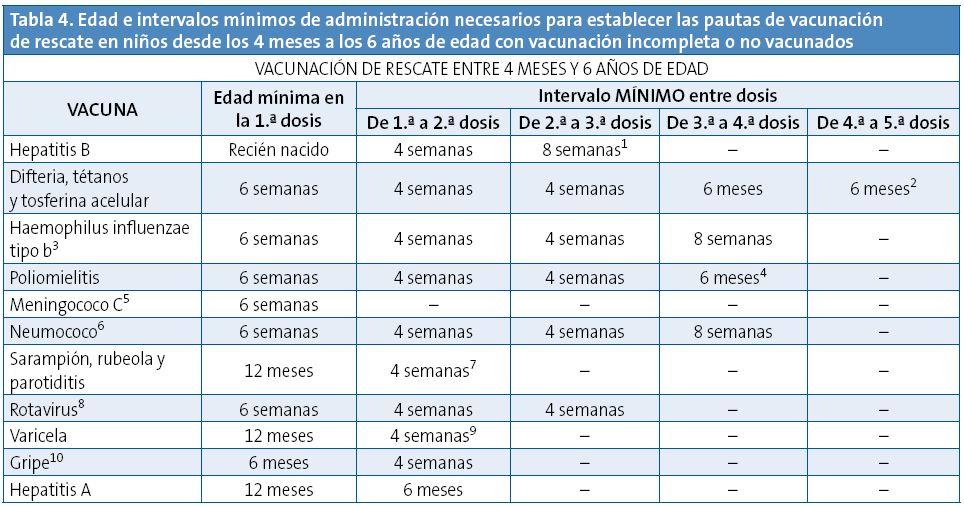
Esta tabla indica los intervalos mínimos entre las dosis para los niños con calendarios incompletos o que comienzan la vacunación tardíamente. No se ha de reiniciar una pauta de vacunación si ya se han administrado dosis previas, sino completarla independientemente del intervalo máximo transcurrido desde la última dosis. Las reacciones adversas se deben notificar a las autoridades sanitarias.
(1) Vacuna antihepatitis B (HB). La 3.ª dosis se administrará, al menos, 4 meses después de la 1.ª y nunca antes de los 6 meses de edad. En caso de haberse administrado 1 dosis de vacuna monocomponente tras el nacimiento también será aceptable administrar 3 dosis adicionales como vacuna hexavalente; la última dosis siempre a los 6 o más meses de edad.
(2) Vacuna frente a la difteria, el tétanos y la tosferina acelular (DTPa/Tdpa). El intervalo mínimo entre la 3.ª y la 4.ª dosis de DTPa es de 6 meses, pero si se aplica la 4.ª dosis a los 4 o más meses se considerará válida. La 5.ª dosis de DTPa o Tdpa no es necesaria si la 4.ª de DTPa se administró con 4 o más años de edad.
(3) Vacuna conjugada frente al Haemophilus influenzae tipo b (Hib). Todas las dosis antes de los 12 meses se administrarán con, al menos, 4 semanas de intervalo. Si la 1.ª dosis de la serie se administra entre los 12 y los 14 meses, las 2 dosis se separarán 8 semanas. Si la 1.ª dosis se administra a partir de los 15 meses solo es necesaria 1 dosis. La 4.ª dosis solo se administrará en caso de haber recibido 3 dosis en los primeros 12 meses de vida.
(4) Vacuna antipoliomielítica inactivada (VPI). Solo si la 3.ª dosis se administró antes de los 4 años de edad se requerirá una 4.ª dosis, separada por 6 meses de la anterior.
(5) Vacuna conjugada frente al meningococo C (MenC). Se precisan 1 o 2 dosis en el primer año de vida (a los 2 y 4 meses o a los 4 meses), según el preparado vacunal. A partir de los 12 meses se precisa 1 dosis en el 2.º año de vida y 1 dosis en la adolescencia a los 12 años de edad.
(6) Vacuna conjugada frente al neumococo (VNC). Todas las dosis antes de los 12 meses se administrarán con, al menos, 4 semanas de intervalo. Si la vacuna se administra entre los 12 y 24 meses las 2 dosis se separarán 8 semanas. Si la 1.ª dosis se administra con más de 24 meses solo es necesaria 1 dosis con Prevenar 13® y 2, separadas por 8 semanas, con Synflorix®, salvo grupos de riesgo que precisan 2 con cualquier preparado. En niños de 5 o más años no es necesaria la vacunación, salvo en grupos de riesgo en los que se debe aplicar 1 dosis de Prevenar 13®. La 4.ª dosis solo se administrará en caso de haber recibido 3 dosis en el primer año. La vacuna polisacarídica 23-valente está indicada en mayores de 2 años con enfermedades que aumentan el riesgo de infección por el neumococo; el intervalo respecto de la última dosis de vacuna conjugada frente al neumococo será de 8 semanas. Synflorix® está autorizada hasta los 5 años y Prevenar 13® hasta la edad adulta, sin límite de edad.
(7) Vacuna frente al sarampión, la rubeola y la parotiditis (SRP). Administrar la 2.ª dosis a los 2-3 años, preferentemente a los 2 años. A partir de los 12 meses de edad se considera correctamente vacunado si se administran 2 dosis separadas por, al menos, 4 semanas.
(8) Vacuna frente al rotavirus (RV). Pentavalente (RotaTeq®) 3 dosis, la última antes de las 32 semanas de edad.
(9) Vacuna frente a la varicela (Var). Administrar la 2.ª dosis a los 2-3 años, preferentemente a los 2 años junto a la vacuna triple vírica (el mismo día o separadas, al menos, por 1 mes). El intervalo mínimo entre ambas dosis de varicela es de 4 semanas aunque se recomienda, en menores de 13 años, un intervalo de 6 a 12 semanas.
(10) Vacuna antigripal (Gripe). Solo se administrarán 2 dosis, separadas por 4 semanas, en menores de 9 años en la primera temporada en que reciban la vacuna antigripal.
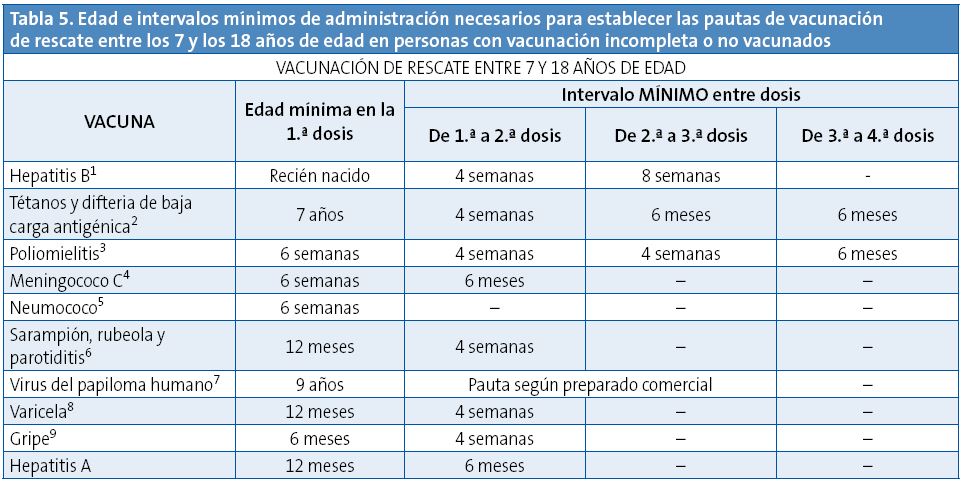
Esta tabla indica los intervalos mínimos entre las dosis para los niños y los adolescentes con calendarios incompletos o que comienzan la vacunación tardíamente. No se ha de reiniciar una pauta de vacunación si ya se han administrado dosis previas, sino completarla independientemente del intervalo máximo transcurrido desde la última dosis. Las reacciones adversas se deben notificar a las autoridades sanitarias.
(1) Vacuna antihepatitis B (HB). En mayores de 7 años no vacunados 3 dosis con la pauta 0, 1, 6 meses. La 3.ª dosis se administrará, al menos, 4 meses después de la 1.ª dosis.
(2) Vacuna frente al tétanos y la difteria de baja carga antigénica (Td). A partir de los 7 años utilizar la vacuna de tétanos-difteria de baja carga antigénica (Td). Para las dosis de refuerzo, una vez completada la primovacunación, se recomienda utilizar la vacuna tétanos-difteria-tosferina acelular de baja carga antigénica (Tdpa). Los vacunados con 1 dosis de DTP antes de los 12 meses de edad recibirán, si continúan la vacunación después de los 7 años, 2 dosis adicionales de Td para completar su primovacunación y una de Tdpa de refuerzo. Los vacunados con 1 dosis de DTP o Td después de los 12 meses, si continúan la serie a partir de los 7 años, completarán su primovacunación con 2 dosis de Td, con un intervalo de 6 meses entre ambas. Para que un adulto se considere completamente inmunizado frente al tétanos debe haber recibido, al menos, 5 dosis de vacunas con toxoide tetánico en su vida, por lo que, tras la primovacunación con 3 dosis, deberá recibir 2 dosis de refuerzo separadas preferentemente por 10 años, aunque el intervalo mínimo entre ellas es de 1 año, una de ellas con Tdpa.
(3) Vacuna antipoliomielítica inactivada (VPI). En mayores de 7 años no vacunados 3 dosis. En caso de haber recibido la 3.ª dosis antes de los 4 años se recomienda administrar una 4.ª dosis, al menos, 6 meses después de la 3.ª.
(4) Vacuna conjugada frente al meningococo C (MenC). En mayores de 7 años no vacunados, si tiene menos de 10 años aplicar 1 dosis seguida de otra a partir de los 10 años y con una separación mínima entre las 2 de 6 meses. Si tiene 10 o más años solo es necesaria 1 dosis.
(5) Vacuna conjugada frente al neumococo. Prevenar 13® está autorizada hasta la edad adulta, sin límite de edad. Todos los grupos de riesgo no vacunados recibirán 1 dosis de esta vacuna y a las 8 semanas 1 dosis de la vacuna polisacarídica 23-valente. Si ya hubieran recibido una dosis de la vacuna 23-valente, podrán recibir 1 dosis de Prevenar 13® separada por, al menos, 8 semanas de la 23-valente puesta. Los grupos de alto riesgo recibirán una 2.ª dosis y última de vacuna 23-valente a los 5 años de la 1.ª dosis.
(6) Vacuna frente al sarampión, la rubeola y la parotiditis (SRP). En mayores de 7 años no previamente vacunados, 2 dosis. Si vacunado con 1 dosis previa de sarampión monocomponente, administrar 2 dosis de SRP. Si vacunado con 1 dosis previa de SRP, administrar una 2.ª dosis.
(7) Vacuna frente al virus del papiloma humano (VPH). Solo para niñas. La edad mínima de administración para la 1.ª dosis es de 9 años. Administrar siempre que sea posible la serie según pauta del preparado comercial correspondiente: Gardasil® 0, 2, 6 meses; Cervarix® pauta de 2 dosis (0 y 6 meses) para niñas entre 9 y 14 años, y pauta de 3 dosis (0, 1, 6 meses) si 15 años o más. Gardasil® recomienda que la 2.ª dosis debe ser administrada, al menos, 1 mes después de la 1.ª dosis y la 3.ª dosis, al menos, 3 meses después de la 2.ª dosis; la 3.ª dosis deberá administrarse no antes de los 6 meses de la 1.ª, pero si han pasado 4 o más meses de la 1.ª dosis se considerará válida. Las 3 dosis deben ser administradas dentro de un periodo de 1 año. Cervarix® recomienda que la 2.ª dosis se administre entre 1 y 2,5 meses tras la 1.ª dosis y la 3.ª dosis entre 5 y 12 meses después de la 1.ª dosis.
(8) Vacuna frente a la varicela (Var). 2 dosis con un intervalo mínimo de 4 semanas en pacientes no previamente vacunados. En menores de 13 años se ha recomendado un intervalo de 6-12 semanas entre ambas dosis y en mayores de 13 años, 4 a 8 semanas.
(9) Vacuna antigripal (Gripe). Solo se administrarán 2 dosis, separadas por 4 semanas, en menores de 9 años en la primera temporada en que reciban la vacuna antigripal.
CONFLICTO DE INTERESES
En la publicación original se expone de forma detallada1.
ABREVIATURAS: CAV-AEP: Comité Asesor de Vacunas de la Asociación Española de Pediatría • CC. AA.: comunidades autónomas.
BIBLIOGRAFÍA
- Moreno-Pérez D, álvarez García FJ, Arístegui Fernández J, Cilleruelo Ortega MJ, Corretger Rauet JM, García Sánchez N, et al.; en representación del Comité Asesor de Vacunas de la Asociación Española de Pediatría. Calendario de vacunaciones de la Asociación Española de Pediatría: recomendaciones 2014. An Pediatr (Barc). 2014;80:55.e1-55.e37.
- Calendarios de vacunación de las ciudades y comunidades autónomas españolas. Web de la Asociación Española de Pediatría de Atención Primaria [en línea] [consultado el 18/01/2014]. Disponible en www.aepap.org/vacunas/calendarios-espanoles
- Consejo Interterritorial del Sistema Nacional de Salud. Calendario común de vacunación infantil; enero de 2014 [en línea] [consultado el 18/01/2014]. Disponible en www.msssi.gob.es/ciudadanos/proteccionSalud/vacunaciones/docs/CalendarioVacunacion2014.pdf
- Arístegui Fernández J, Moreno-Pérez D. El calendario de vacunación común de mínimos para España: posicionamiento del CAV-AEP. An Pediatr (Barc). 2014;80:1-5.