
Vol. 15 - Num. 60
Originales
Lesiones no intencionales. Factores de riesgo en seguridad vial y práctica de actividades acuáticas en adolescentes de 13 a 18 años
Ana Fierro Urturia, Marta Esther Vázquez Fernándezb, M.ª Fe Muñoz Morenoc, M Alfaro Gonzálezd, Luis Rodríguez Molineroe, P García Gutiérrezf, Grupo de Educación para la Salud de la AEPap
aPediatra. CS Pisuerga. Arroyo de la Encomienda. Valladolid. España.
bPediatra. CS Arturo Eyries. Facultad de Medicina. Universidad de Valladolid. Valladolid. España.
cUnidad de Investigación Biomédica. Hospital Clínico Universitario de Valladolid. Valladolid. España.
dServicio de Pediatra. Hospital de Medina del Campo. Medina del Campo. Valladolid. España.
eServicio de Pediatría. Hospital Recoletas Campo Grande. Valladolid. España.
fPediatra. CS Aranda Norte. Aranda de Duero. Burgos. España.
Correspondencia: A Fierro. Correo electrónico: anfier99@gmail.com
Cómo citar este artículo: Fierro Urturi A, Vázquez Fernández ME, Muñoz Moreno MF, Alfaro González M, Rodríguez Molinero L, García Gutiérrez P, et al. Lesiones no intencionales. Factores de riesgo en seguridad vial y práctica de actividades acuáticas en adolescentes de 13 a 18 años. Rev Pediatr Aten Primaria. 2013;15:315-28.
Publicado en Internet: 04-12-2013 - Número de visitas: 40575
Resumen
Introducción: los accidentes o lesiones no intencionales constituyen un problema de salud pública por su prevalencia, morbimortalidad y elevados costes sanitarios. El conocimiento de los factores de riesgo de los accidentes ha permitido la elaboración de programas eficaces para su prevención y control.
Objetivo: conocer la prevalencia de las lesiones no intencionales que han precisado atención médica en el último año y analizar las conductas de riesgo en seguridad vial y actividades acuáticas en los adolescentes de la provincia de Valladolid (España), así como su relación con diversos factores.
Material y métodos: se realizó una encuesta a una muestra de 2412 escolares de 13 a 18 años de edad de la provincia de Valladolid durante el año 2012, con preguntas relacionadas con hábitos, comportamientos y conductas relacionadas con la salud. Se presentan los datos sobre accidentabilidad y factores de riesgo en seguridad vial y actividades acuáticas.
Resultados: la proporción de adolescentes que han sufrido algún accidente o lesión que requirió asistencia médica en el último año fue del 14%. Como factores de riesgo en la seguridad vial, destaca que el 81,5% refiere no usar el casco cuando monta en bicicleta, el 6% en moto y un 1,2% no se abrocha el cinturón de seguridad cuando va en coche. Detectamos varios factores de riesgo de accidentes en actividades acuáticas. Diversas variables sociodemográficas, económicas y conductas de riesgo se asocian al riesgo de accidentabilidad.
Conclusiones: encontramos en nuestro estudio factores de riesgo en la seguridad vial de los adolescentes y en la práctica de actividades acuáticas. Son necesarias medidas legislativas, campañas publicitarias y programas educativos en la escuela y en el medio sanitario, para reducir el riesgo de muerte y lesiones por accidentes en adolescentes.
Palabras clave
● Accidente ● Adolescencia ● Conductas de riesgoINTRODUCCIÓN
Los accidentes o lesiones no intencionales representan hoy día uno de los principales problemas en Salud Pública. Constituyen la primera causa de mortalidad en la población infantojuvenil en España y en los países de la Unión Europea, y son una importante causa de morbilidad y discapacidad que ocasiona elevados costes sanitarios1-5.
No solo repercuten en el aspecto sanitario con la necesidad que generan en cuanto a asistencia, sino que además los accidentes implican numerosos problemas de orden económico y social por las repercusiones familiares, sociales y los años potenciales de vida perdidos6.
Su origen es multifactorial, pues en él intervienen factores personales y ambientales. Entre los factores personales, destaca la influencia de la edad, siendo la adolescencia el grupo con más riesgo por sus propias características de inexperiencia, inestabilidad emocional, búsqueda de lo novedoso, impulsividad, ser fácilmente influenciables y con necesidad de mostrar sus habilidades ante los demás, entre otros4.
En ellos, los accidentes de tráfico constituyen el principal mecanismo lesivo, aunque no es despreciable el riesgo de intoxicaciones, ahogamientos, lesiones por armas de fuego, caídas y quemaduras5-7.
La mayoría de los accidentes y sus consecuencias negativas pueden evitarse con un enfoque preventivo social, educativo y sanitario, dirigido, en función de las edades, a padres, educadores y, sin duda alguna, a jóvenes y adolescentes con un potencial elevado en las conductas de riesgo.
El Informe mundial sobre prevención de las lesiones en los niños, elaborado conjuntamente por la Organización Mundial de la Salud (OMS) y UNICEF en 2006, reú ne todo el conocimiento actual acerca de los diversos tipos de lesiones en los niños y cómo evitarlos4,8.
En este artículo, se muestran los resultados de un estudio descriptivo de las situaciones de riesgo de accidentabilidad realizado en el marco de un proyecto más amplio de análisis de hábitos, comportamientos y conductas relacionadas con la salud, realizado en una muestra de estudiantes de 13 a 18 años de edad de la provincia de Valladolid (España) entre marzo y mayo del año 2012.
Los datos aportados en este estudio permiten identificar algunos comportamientos de riesgo relacionados con la seguridad vial y la práctica de actividades acuáticas de los adolescentes de nuestra provincia, así como su relación con diversos factores.
Conocer estos aspectos es imprescindible para poder diseñar estrategias preventivas eficaces, y el pediatra es uno de los profesionales más implicados en su problemática1,5,9-11.
MATERIAL Y MÉTODOS
Diseño
Se ha realizado un estudio descriptivo trasversal. La población de estudio han sido los adolescentes de 13 a 18 años de edad de la provincia de Valladolid, matriculados en centros educativos con 2.°, 3.° y 4.° de Enseñanza Secundaria Obligatoria (ESO) y 1.° y 2.° de Bachillerato LOGSE. De un total de 18 888 escolares se obtuvo una muestra de 2412 adolescentes. La selección de alumnos se realizó seleccionando aleatoriamente colegios (n=14) y después aulas, incluyendo a todos los estudiantes de las aulas seleccionadas.
El tamaño muestral se calculó para una proporción estimada del 50% y una precisión del 2,5% en un contraste bilateral, asumiendo un 10% de falta de respuestas, de donde resultaron 1566 alumnos. El número final de alumnos encuestados, una vez depurados los datos, fue de 2412 adolescentes escolarizados de 13 a 18 años.
Se contactó telefónicamente y por correo con los directores de los colegios y se les informó sobre los objetivos y contenidos del estudio, acordando uno o varios días (no precedidos de vacaciones) para la realización de la encuesta entre marzo y mayo de 2012. Tres colegios rehusaron participar sin dar una razón clara. Los colegios notificaron a las familias de los alumnos que se les iba a hacer participar en la encuesta, dando la opción de rechazarlo, sin consecuencias.
El equipo investigador fue el encargado de administrar la encuesta. En el 69% de la muestra se utilizó el cuestionario asistido por ordenador, y en el resto, el cuestionario en formato papel, principalmente por no disponer de suficiente número de ordenadores en las aulas de informática. Los datos informáticos quedaron automáticamente recogidos en la base de datos y los realizados en papel fueron introducidos manualmente en la misma.
Los alumnos seleccionados cumplimentaron los cuestionarios de forma personal, avisados previamente de la confidencialidad de los datos y de que no existiera comunicación entre ellos. La realización de la encuesta fue voluntaria, durante el horario escolar habitual. El tiempo aproximado utilizado para responder fue de 35-40 minutos. El diseño del proyecto fue aprobado por la Comisión de Investigación de la Gerencia de Atención Primaria del área Oeste de Valladolid.
Diseño
El cuestionario recogía, entre otras y además de preguntas relacionadas con el riesgo de accidentabilidad de los adolescentes, cuestiones sobre variables sociodemográficas, actividades durante el tiempo libre, rendimiento escolar, consumo de sustancias (tabaco, alcohol, drogas), conducta antisocial, experiencia sobre el maltrato y relaciones con los demás, alimentación y sexualidad, basadas en las recomendaciones de los programas internacionales12-14, nacionales15,16 y de distintas provincias y comunidades autónomas17-20.
Los principales indicadores analizados en relación con la accidentabilidad de los adolescentes fueron los siguientes:
- Alumnos que han tenido alguna lesión y han necesitado asistencia médica en los últimos 12 meses.
- Uso del cinturón cuando circulan en coche.
- Uso del casco cuando van en moto o en bicicleta.
- Conducción de vehículos bajo los efectos del alcohol o las drogas.
- Viajar en un vehículo conducido por alguien bajo los efectos del alcohol o las drogas.
- Preguntas sobre actividades acuáticas y prácticas de riesgo (saber nadar, tirarse de cabeza a la piscina, tirarse desde acantilados, meterse en el agua nada más comer y no tener en cuenta las indicaciones de los socorristas).
El estudio se realizó entre marzo y mayo de 2012.
Análisis estadístico
Las variables cuantitativas se presentan con los valores medios y el intervalo de confianza del 95% y las cualitativas según su distribución de frecuencias.
Para analizar la asociación entre los riesgos de accidentabilidad, las características sociodemográficas y los factores de riesgo, se ha utilizado el test Chi-cuadrado de Pearson. En el caso de que el número de celdas con valores esperados menores de 5 sean más de un 20%, se ha utilizado el test exacto de Fisher o el test razón de verosimilitud para variables con más de dos categorías.
Los datos han sido analizados con el programa estadístico SPSS®, versión 20.0, para Windows®. Los valores de p<0,05 han sido considerados estadísticamente significativos.
RESULTADOS
De los alumnos encuestados, fueron validadas 2412 encuestas; el 47,3% correspondía a mujeres, y el 52,7%, a varones. En relación con el curso, el 23,5% pertenecía a 2.° de la ESO; el 25,8%, a 3.° de la ESO; el 20,2%, a 4.° de la ESO; el 18,9%, a 1.° de Bachillerato, y el 11,6%, a 2.° de Bachillerato. La mayoría de los estudiantes procedía de colegios ubicados en el hábitat urbano (87,3%). El 95,5% pertenecía a un nivel socioeconómico medio o alto, según la estimación de la capacidad adquisitiva familiar mediante laFamily Affluence Scale (FAS)21.
Lesiones y accidentabilidad
En la Fig. 1 se describe la frecuencia de lesiones no intencionales y conductas de riesgo en seguridad vial.
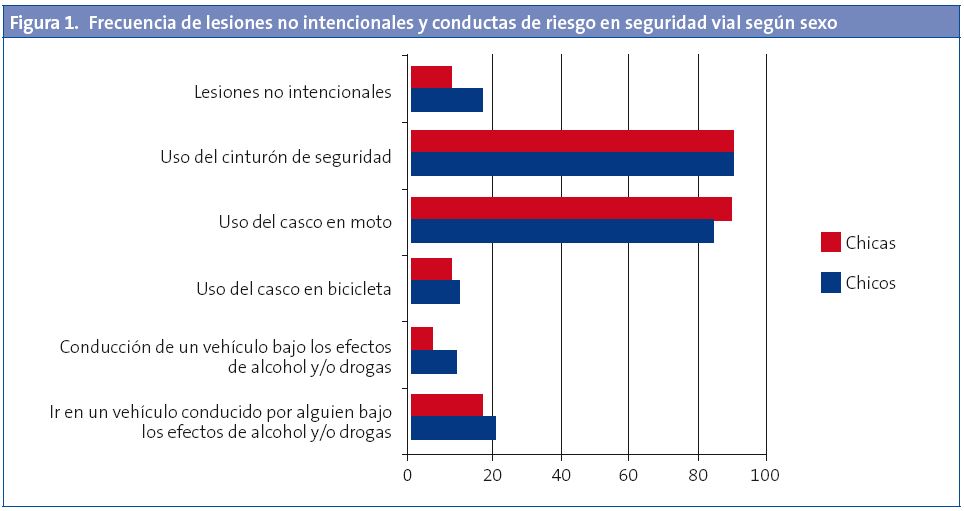
La proporción de niños que refirió haber sufrido algún accidente o lesión que requirió asistencia médica en los últimos 12 meses fue del 14%. Las causas referidas en mayor proporción (30%) fueron los accidentes traumatológicos (esguinces y fracturas), muchos de ellos ocasionados durante la práctica de deporte o caídas. Los accidentes de tráfico supusieron el 5,3%, diferenciados en automovilístico (2,9%), de bicicleta (1,7%), de moto (0,5%) y de monopatín (0,2%). Las heridas y contusiones supusieron el 2%. El 1,2% fue atendido por traumatismos craneoencefálicos.
Presentan una mayor accidentabilidad los varones, con un 17,5% frente al 10,2% de las mujeres, diferencia que resulta estadísticamente significativa (p<0,001). En el caso del curso, no se han encontrado diferencias.
Seguridad vial
- Uso del cinturón de seguridad en el coche: el 93,9% de los adolescentes refirió abrocharse el cinturón de seguridad habitualmente o siempre (el 93,9% de los chicos frente al 94,0% de las chicas) cuando iban en coche; a veces, un 4,9% (el 4,6% de los chicos frente al 5,3% de las chicas), y raramente o nunca el 1,2% (el 1,4% de los chicos frente al 0,6% de las chicas) (p=0,048). No se observaron diferencias significativas en relación al curso.
- Uso del casco en bicicleta y motocicleta: en la Tabla 1 se describen las respuestas sobre el grado de utilización del casco en bicicleta y motocicleta, diferenciadas por curso y sexo.
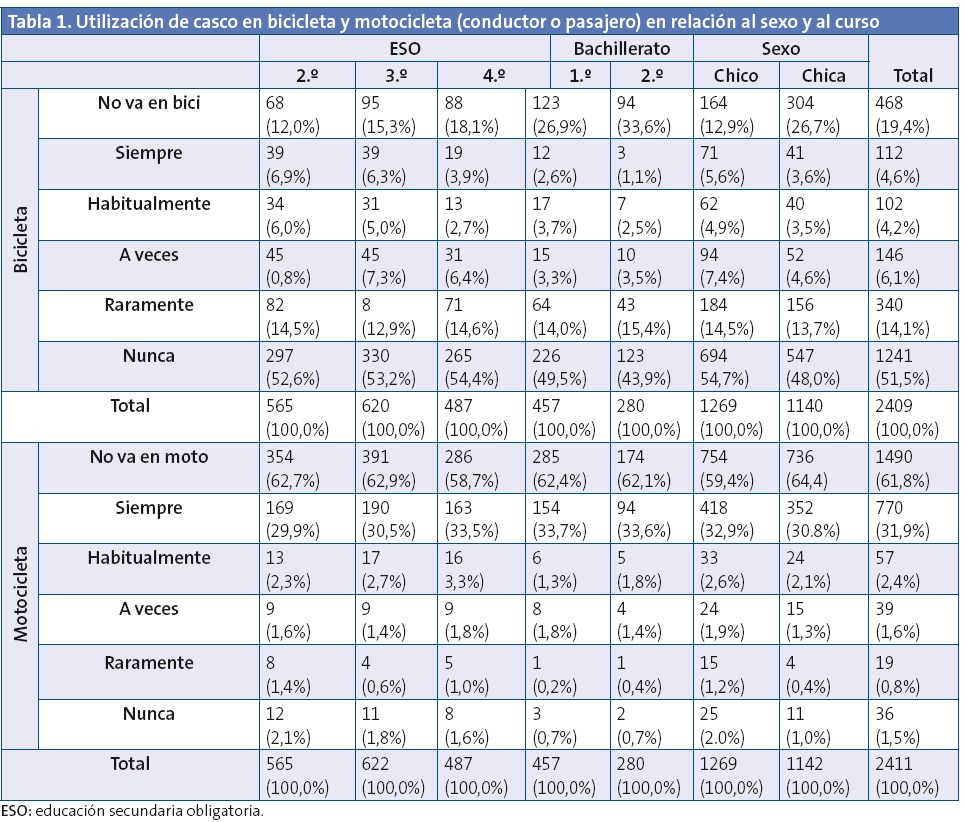
Se destacó el escaso uso del casco en bicicleta: un 81,5% de los adolescentes refirió utilizarlo raramente o nunca. El uso del casco en moto estaba más generalizado; sin embargo, el 6% declaró no utilizarlo nunca o casi nunca. Encontramos diferencias estadísticamente significativas en relación al sexo y al curso. Es mayor la proporción de chicas que no se pone el casco cuando va en bicicleta (p=0,009), mientras que son los chicos los que con más frecuencia no hacen uso de él cuando van en moto (p=0,01). El uso del casco en bicicleta es menor en los alumnos de 2.° Bachillerato (p<0,001).
Práctica de deportes acuáticos y actividades de riesgo en el agua
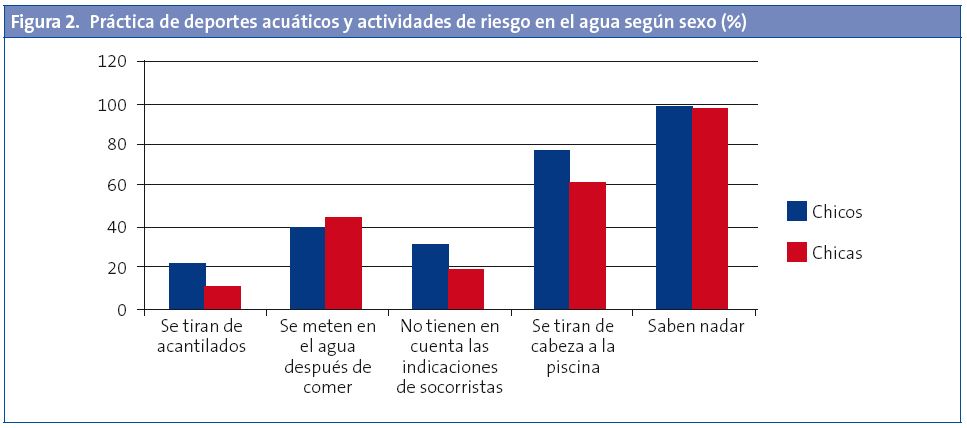
- Saber nadar:el 98,1% de los adolescentes sabe nadar, en proporción similar de chicos (98,3%) y chicas (97,8%). No hay diferencias estadísticamente significativas con respecto al curso.
- Actividades de riesgo: en general, las actividades de riesgo en el medio acuático son mayores en los chicos, presentando diferencias estadísticamente significativas en casi todos los casos. En el análisis según curso, solo presenta significación estadística la variable relacionada con meterse en el agua nada más comer, la única actividad de riesgo que es más frecuente en chicas.
- Acostumbra a tirarse de cabeza en la piscina el 69,2% (el 76,2% de los chicos y el 61,5% de las chicas) (p<0,001).
- A veces se ha tirado desde acantilados el 17,5% de los adolescentes (el 22,4% de los chicos y el 12% de las chicas) (p<0,001).
- Se mete en el agua nada más comer el 41,5% (el 39,1% de los chicos y el 44,3% de las chicas) (p=0,010). Los alumnos que lo realizan con mayor frecuencia son los de 2.° Bachillerato (45,5%) y 3.° ESO (45%), mientras que en menor medida lo hacen los de 2.° ESO (36,5%) (p=0,027).
- No tiene en cuenta las indicaciones de los socorristas cuando se mete en el mar el 25,6% de los adolescentes (el 31,5% de los chicos y el 19% de las chicas) (p<0,001).
En la Fig. 2 se describe la práctica de deportes acuáticas y actividades de riesgo según sexo.
Factores asociados a conductas de riesgo en seguridad vial
Los factores sociodemograficos y conductas de riesgo que se asocian al no uso del casco cuando se va en moto o en bicicleta se exponen en la Tabla 2. Destaca la asociación de estas conductas de riesgo en seguridad vial con otros comportamientos de riesgo como el bajo rendimiento escolar, el consumo de tabaco, alcohol o drogas, la conductas antisociales (robar y hacer novillos), etc. Así como con factores sociodemográficos como la edad, el sexo y el nivel socioeconómico.
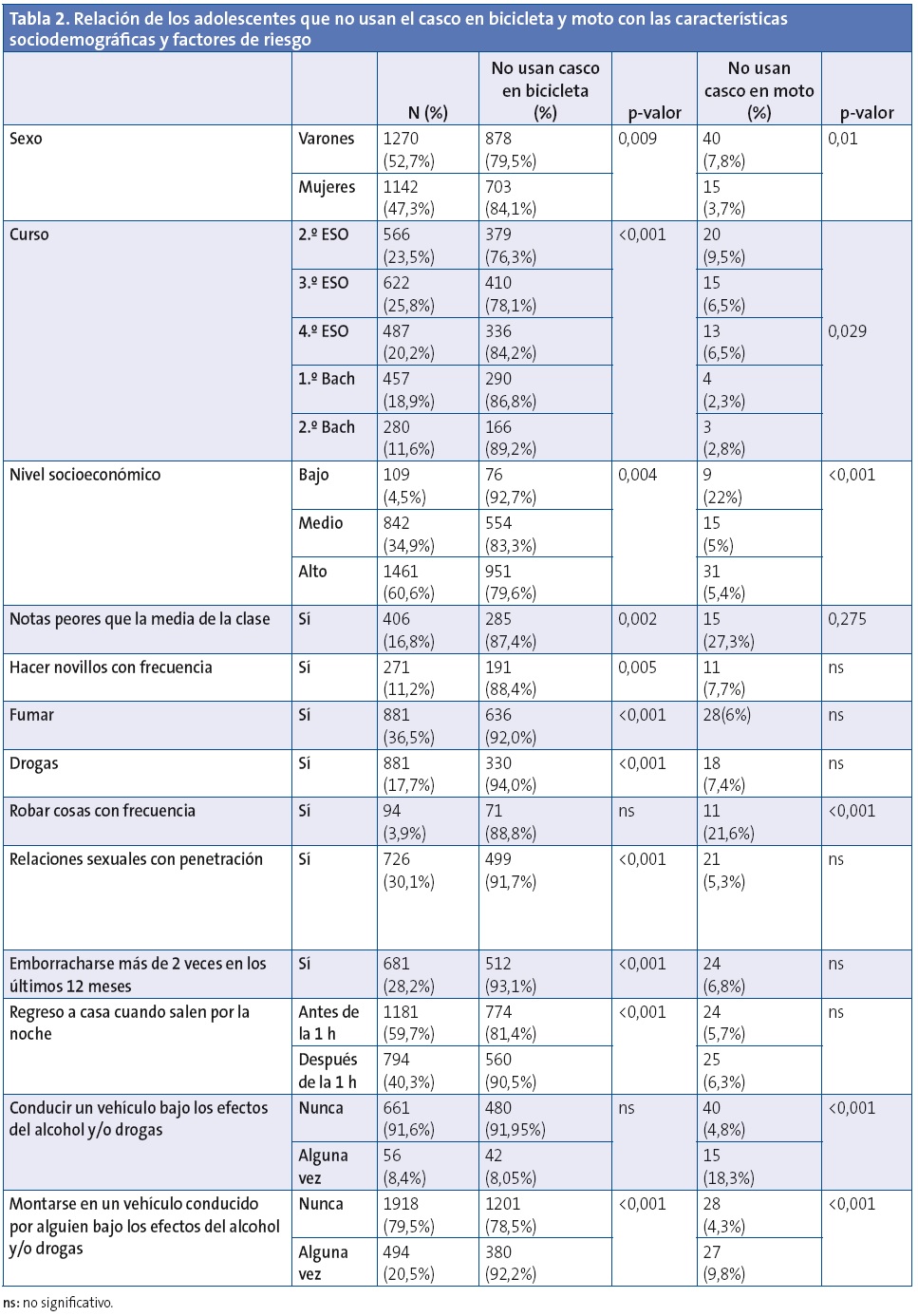
Otros dos aspectos que destacaron fueron la proporción de adolescentes (20,4%) que referían haberse montado en un vehículo conducido por una persona bajo los efectos del alcohol y/o las drogas, y los que declaraban haber conducido un vehículo (moto o coche) bajo los efectos de las drogas o alcohol (8,4%).
DISCUSIÓN
Las lesiones son una de las principales causas de muerte en los niños de todo el mundo. Son además un motivo importante de discapacidad y morbilidad, con secuelas duraderas e incluso permanentes, ya sean físicas, sensoriales o mentales2,6,11. Las lesiones no intencionales o accidentes representan casi el 90% de estos casos, y son la principal causa de muerte en los niños de 10 a 19 años.
Según los resultados encontrados por varios estudios internacionales, el problema de las lesiones se muestra particularmente preocupante en el caso de España, ya que se sitúa entre los países desarrollados con las cifras más altas de lesiones entre la población adolescente14,22. En nuestro país, los accidentes son la primera causa de muerte de 1 a 25 años, con tasas de incidencia que oscilan entre el 3,3/100 000 habitantes/año en edades comprendidas entre los 5 y los 14 años y el 30,1/100 000 habitantes/año de 15 a 25 años10,11. Aproximadamente el 1% de los accidentes son mortales.
Los resultados de nuestro estudio muestran que un 14% de los adolescentes refiere haber tenido alguna lesión que ha necesitado asistencia médica en el último año, dato similar al registrado por el Sistema de Vigilancia de Factores de Riesgo asociados a Enfermedades No Transmisibles en población juvenil (SIVFRENT-J) en los jóvenes de 15-16 años en 201020, e inferior al registrado al último estudio HBSC-2010 realizado en chicos y chicas españoles de 11 a 18 años (61,9%)14.
Destaca la mayor accidentabilidad en los varones, datos que concuerdan con otras investigaciones4,5,14,16,20.
Se han propuesto diversas teorías para explicar las diferencias en las tasas de lesiones por sexo23. Una de ellas es que los niños participan más en conductas de riesgo, tienen mayor grado de actividad física, realizan más deporte y se comportan de manera más impulsiva que las niñas.
Las causas referidas en mayor proporción (30%) fueron los accidentes traumatológicos (esguinces y fracturas), muchos de ellos ocasionados durante la práctica de deporte o caídas, como también refieren otros estudios, siendo la causa principal de lesiones no mortales4.
Las lesiones de tráfico constituyen la principal causa de discapacidad en niños y adolescentes de todo el mundo, siendo la principal causa de muerte para las edades comprendidas entre los 10 y los 19 años4.
La tasa mundial de mortalidad por traumatismos causados por accidentes de tráfico aumenta con la edad, lo que refleja la evolución del uso de las vías públicas en función de la edad, en menores como pasajeros de vehículos y peatones, posteriormente como ciclistas, motociclistas y por último como conductores.
En España, los accidentes de tráfico son la primera causa de muerte entre los 15 y los 35 años, tal como se detalla en los últimos datos analizados por el Centro de Epidemiología (CNE) del Instituto Carlos III del Ministerio de Sanidad y Consumo24. El descenso progresivo de la tasa de mortalidad por esta razón en los últimos años24,25 ha hecho que pase al tercer lugar en los niños y niñas de 5 a 14 años y en las mujeres de 25 a 34 años, lo cual indica que las medidas llevadas a cabo para su prevención están siendo eficaces.
La distribución porcentual del número de fallecidos, en función de modo de desplazamiento en el tramo de edad de 15 a 17 años, según datos de la Dirección General de Tráfico (DGT) de 2011, fue del 41% en ciclomotor, 31% en turismo, 10% como peatones, 7% en moto,7% en bicicleta y 4% en otras circunstancias26.
Las revisiones científicas realizadas demuestran la eficacia en reducir la morbimortalidad por accidente de tráfico con la utilización de los sistemas de retención infantil, el uso del cinturón de seguridad y el uso del casco en bicicletas, motos y ciclomotores. Por otra parte, las pruebas existentes en la actualidad en otros países desarrollados demuestran que las leyes aumentan la utilización del casco, cuyo uso reduce el riesgo de lesiones craneofaciales y muerte1,4,27-29,32.
El uso del cinturón de seguridad ha aumentado de forma progresiva en los últimos años hasta un 88,6% de los conductores en el año 2011, según datos del Road Safety Annual Report 201125. Sin embargo, el 22% de los fallecidos usuarios de turismo no utilizaba el cinturón de seguridad en las vías interurbanas, y en las vías urbanas este porcentaje fue casi del 41%.
En nuestro estudio, el 93,9% de los encuestados refirió usar el cinturón de seguridad habitualmente o siempre, coincidiendo estos resultados con los de otros estudios realizados también en población adolescente17,20; sin embargo, la no utilización del mismo por el 6,1% de los adolescentes hace que siga siendo necesario promover su uso a todas las edades.
A pesar del descenso en las cifras de mortalidad globales, las víctimas por accidente de motocicleta aumentaron entre 2003 y 2009, aunque se aprecia una tendencia descendente en los dos últimos años. Sin embargo, el ciclomotor es el tipo de vehículo en el que ha habido más fallecidos, heridos graves y heridos leves en la franja entre 15 y 17 años25,26.
Para entender mejor la alta incidencia de lesiones de tráfico en la adolescencia española hay que tener en cuenta que España ocupa una posición destacada en lo que se refiere al uso de vehículos de dos ruedas. La normativa española autoriza a obtener la licencia para conducir ciclomotores (50 cc) a partir de los 15 años desde diciembre de 2010, el permiso de conducir motocicletas de hasta 125 cc, a partir de los 16, y los permisos para motocicletas de mayor cilindrada y para automóviles, a partir de los 18 años30,31.
Por otro lado, teniendo en cuenta los datos estadísticos de accidentalidad, algunos estudios de la DGT señalan el menor porcentaje de uso del casco como uno de los factores que explican la alta siniestralidad registrada en el grupo de jóvenes conductores de ciclomotor (14-17 años de edad). Según cifras de 2011, el 19% de los usuarios de ciclomotor fallecidos no utilizaba casco en carretera y el 16% en zona urbana. En el caso de las motocicletas, los fallecidos en carretera no utilizaban casco en el 2% de los casos, mientras que en zona urbana ese porcentaje se eleva al 15%26.
La utilización del casco disminuye el riesgo y la gravedad de los traumatismos un 72% aproximadamente y reduce el riesgo de defunción hasta un 39%, según la velocidad de la motocicleta4.
Un 10,1% de los adolescentes de nuestro estudio declaró no utilizar el casco en la moto nunca o casi nunca, datos comparables a los de otras investigaciones17,26,33 e inferiores a los registrados en el 2011 en la Comunidad de Madrid en alumnos de 4.° de la ESO (35,2%)20.
El uso de a bicicleta ha experimentado un incremento en los últimos años, tanto en los países europeos como en EE. UU., siendo utilizada para realizar diversas actividades como la recreativa o la deportiva, y como medio de transporte o de trabajo. Es utilizada principalmente en las calles, que es donde se ocasionan con mayor frecuencia los accidentes. Sin embargo, esta actividad no está exenta de riesgos, ya que es causante de muchos accidentes que pueden ocasionar lesiones graves con secuelas importantes e incluso la muerte.
A nivel mundial, en su manual sobre cascos de motociclistas y ciclistas, la OMS indica que aproximadamente dos terceras partes de las lesiones graves de ciclistas que requieren hospitalización y tres cuartas partes de las muertes ocurridas en ciclistas son consecuencia de traumatismos craneales. Casi el 25% de las lesiones cerebrales significativas en menores de 15 años se debe a los accidentes con bicicleta4.
Además de las lesiones craneales, las lesiones musculoesqueléticas y las producidas en órganos internos son también causas importantes de mortalidad relacionada con la bicicleta.
Aunque los accidentes se dan mayoritariamente en la zona urbana, los fallecidos se producen principalmente en carretera, siendo varones más del 90% de los ciclistas fallecidos.
En nuestro país, el número de ciclistas fallecidos entre 2001 y 2010 se redujo un 33%, si bien entre los años 2009 y 2010 aumentó un 20%. Sin embargo, en el caso de los lesionados se ha producido un notable incremento en los últimos diez años26,29.
Según la revisión internacional realizada por el estudio Cochrane, las lesiones de la cabeza son responsables de alrededor de tres cuartos de todas las muertes de ciclistas implicados en colisiones, y los cascos proporcionan una reducción entre el 63 y el 88% de las lesiones graves en la cabeza (cuero cabelludo y cráneo) y el cerebro para todas las edades de ciclistas. Por otra parte, los cascos proporcionan el mismo nivel de protección en caso de colisiones con implicación de vehículos a motor que en el caso de otras causas1,4,27.
Pese a ello, la gran mayoría de los usuarios de bicicletas, incluidos los niños, no utilizan el caso o lo usan de manera inadecuada.
En nuestro estudio, una altísima proporción de adolescentes refiere no usar el casco nunca o casi nunca (81,3%), datos que poco han variado del estudio realizado en el año 2005 en Guipúzcoa33 y similar al estudio realizado en la Comunidad de Madrid en 200920. Destacamos en nuestro estudio el mayor número de mujeres que no utilizan el casco cuando montan en bicicleta mientras que son los varones los que menos lo utilizan en la moto, factores a tener en cuenta al realizar las medidas preventivas en seguridad vial.
La práctica de deportes acuáticos es otra causa frecuente de accidentes, siendo el ahogamiento una de las principales causas de muerte en niños y adolescentes.
La tasa mundial de ahogamiento mortal en la niñez es de 7,2 por 100 000 habitantes, aunque varía considerablemente según las regiones. El 28% de todas las defunciones de los niños por lesiones no intencionales se debe al ahogamiento. Las tasas de muerte por ahogamiento más elevadas corresponden a los niños menores de cinco años, y el valor máximo de todos los grupos de edad corresponde a los niños de uno a cuatro años. Se observa otro pico más pequeño al final de la adolescencia4.
El ahogamiento de los adolescentes suele producirse en masas de agua libre mientras realizan actividades relacionadas con la natación, la navegación o cualquier otra actividad recreativa. Habitualmente, los adolescentes y preadolescentes saben nadar, o al menos tienen nociones, pero la mayoría piensa que nada mejor de lo que realmente lo hace, y entonces no valora adecuadamente las corrientes, las profundidades del agua y su propio estado físico.
La mayoría de los accidentes suceden en lugares no supervisados, como ríos, diques y estanques, como resultado de lesiones producidas por zambullirse en áreas de escasa profundidad o con objetos flotantes o sumergidos, golpes contra el fondo de la piscina, saltos desde el trampolín, o bien al nadar bajo los efectos del alcohol u otras drogas.
Los comportamientos arriesgados ocupan uno de los primeros lugares entre las causas de ahogamiento accidental, en particular en los adolescentes. El consumo de alcohol se ha asociado a una proporción de defunciones de adolescentes y adultos en el curso de actividades de recreo acuáticas que oscila entre el 25 y el 50%. El alcohol influye en el sentido del equilibrio, en la coordinación y en el juicio, y la exposición al sol y al calor agrava sus efectos aumentando su riesgo de ahogamiento en el caso de que se encuentren en una situación difícil4.
En general, los adolescentes que se ahogan estaban en compañía de uno o varios amigos de edad similar que no se dieron cuenta de sus dificultades o que no pudieron socorrerlos. Los adultos suelen estar ausentes, y es posible que los adolescentes presionen a sus compañeros para que adopten conductas arriesgadas, como el consumo de alcohol. El riesgo de ahogamiento aumenta proporcionalmente a la tasa de alcoholemia.
Los datos mundiales indican que el ahogamiento mortal es más frecuente en los niños que en las niñas. La mayor diferencia entre sexos en las tasas de mortalidad por ahogamiento se encuentra en el grupo de 15 a 19 años, siendo 2,4 veces mayor en los chicos que en las chicas4. Los niños afrontan un mayor riesgo de ahogamiento que las niñas debido a su mayor exposición a entornos donde hay agua y a que adoptan con mayor frecuencia comportamientos arriesgados, en particular en el caso de los adolescentes.
En España, según datos del CNE del Instituto Carlos III, en el año 2010 la tasa de mortalidad por ahogamiento en ambos sexos fue del 0,67/100 000 habitantes/año en el grupo de 15 a 24 años, con una tasa del 1,22/100 000 habitantes/año para los varones y 0,09/100 000 habitantes/año las mujeres24.
En nuestro estudio, a pesar de que casi todos los adolescentes refieren saber nadar (98,1%), es importante la proporción de ellos que adoptan prácticas de riesgo en el medio acuático, como tirarse de cabeza a la piscina, tirarse por acantilados y no obedecer las indicaciones de los socorristas, siendo estas prácticas también más frecuentes en chicos. Las chicas, sin embargo, se meten con más frecuencia en el agua después de comer.
Diferentes investigaciones han informado de que las lesiones están relacionadas con otras conductas de riesgo en la adolescencia, como el uso de sustancias, el absentismo escolar y la participación frecuente en la actividad física14. La comprensión de los factores que contribuyen a la aparición de lesiones entre los jóvenes es fundamental para el desarrollo de intervenciones para controlar y evitar lesiones graves y muerte.
El alcohol aparece como factor en un tercio de los accidentes mortales en los que intervienen adolescentes, alterando la capacidad de conducción, por lo general con concentraciones sanguíneas inferiores a las que producen el mismo efecto en adultos. Además, otros factores, tales como un error del conductor, un menor uso de los cinturones de seguridad, la distracción (uso del teléfono móvil u otros dispositivos electrónicos...), la fatiga y la presencia de otros pasajeros adolescentes, aumentan la gravedad de los choques en los que participan conductores adolescentes. Dichos comportamientos de riesgo se ven a menudo exacerbados por la presión de iguales, sobre todo en el caso de los chicos, por lo que la probabilidad de lesiones por tráfico es mucho mayor en ellos, incrementándose también las diferencias con la edad4.
Conducir después del consumo de sustancias psicoactivas es un hecho frecuente en España, alcanzando un porcentaje del 17% de los conductores españoles. Aparte del alcohol (7%), casi un 11% de conductores conducen tra haber consumido alguna sustancia (drogas de abuso) que puede afectar a la capacidad para una conducción segura, entre las que se encuentran el cannabis y la cocaína como las dos sustancias más frecuentemente halladas. Estos datos proceden del proyecto europeo DRUID (Driving Under Influence of alcohol and Drug), concluido en 201134.
En nuestro estudio, el 8,4% de los adolescentes que refiere haber conducido un vehículo (coche o moto) declara que lo ha hecho bajo los efectos del alcohol y/o las drogas, y un 20,4% se ha montado en un vehículo (coche o moto) conducido por otra persona que estaba bajo los efectos del alcohol y/o las drogas, en proporción similar a otras encuestas18. En ambas situaciones, la adopción de estas conductas de riesgo fue mayor en los varones, situación también observada en otros estudios4.
Encontramos otros factores asociados al mayor riesgo de accidentabilidad, adolescentes pertenecientes a nivel socioeconómico bajo, el menor nivel de estudios de los padres, adolescentes con peor rendimiento escolar, hacer novillos en la escuela, conductas antisociales como robar con frecuencia cosas y consumo de alcohol y otras sustancias adictivas.
Recomendaciones en la prevención de lesiones y accidentes de tráfico
Las lesiones pueden prevenirse o controlarse. La adopción de medidas específicas para la seguridad vial dirigidas a adolescentes adoptadas en otros países ha revelado una reducción significativa de la morbimortalidad asociada la conducción de vehículos por adolescentes. Entre estas medidas se encuentran:
- Programas de concesión gradual de permiso de conducción en etapas de aprendizaje con restricciones temporales en la conducción sin supervisión, la conducción de noche y la conducción con pasajeros jóvenes.
- Limitar la conducción en autovías a una velocidad de 80 km/hora.
- Restricción de la tasa de alcoholemia permitidas de 0-0,02 g/dl para conductores menores de 21 años.
- Restricciones relativas al uso de teléfonos móviles, incluso aquellos que cuentan con dispositivos de manos libres.
- Elevación de la edad legal mínima para consumir alcohol a los 21 años.
- Medidas legislativas sobre la obligatoriedad del uso de cascos homologados a los usuarios de bicicletas, ciclomotores y motocicletas acompañadas de campañas de concienciación del público.
- Realizar campañas de información y concienciación que expliquen la protección que ofrecen los equipamientos de seguridad en motoristas (cascos, espalderas, botas y coderas de calidad) y fomenten su uso cotidiano.
Estrategias de prevención durante las actividades acuáticas
Deben adaptarse a las circunstancias y los lugares, y usar enfoques multifacéticos en la medida de lo posible:
- Los cursos de natación y la enseñanza de las aptitudes necesarias para la supervivencia en el agua son uno de los componentes importantes en los programas de prevención.
- Mejorar las siguientes capacidades cognitivas relacionadas con las actividades en el agua: reconocimiento de los riesgos; conocimiento de los límites personales, incluidos los relacionados con la natación; capacidad de resistir la presión de los compañeros para participar en actividades para las cuales se carece de las aptitudes necesarias.
- Disuadir a los adolescentes de consumir alcohol cuando practiquen deportes acuáticos y limitar cualquier tipo de publicidad que estimule el uso de alcohol a bordo de embarcaciones, así como la venta de alcohol en lugares donde se realicen actividades recreativas acuáticas.
- Proponer a los niños y adolescentes lugares para nadar que sean seguros a la par que atractivos. Socorristas convenientemente formados y equipados presentes en los lugares y los momentos en los que los adolescentes tienden a congregarse. En las zonas rurales, poner a disposición de los adolescentes y los niños lugares seguros para nadar, para evitar que se reúnan en lugares peligrosos, como los canales de riego, las canteras y otras zonas con masas de agua libre.
Conclusiones
Encontramos factores de riesgo en la seguridad vial de los adolescentes de nuestra provincia, como son el no uso del cinturón de seguridad, la no utilización del casco en moto, un alto porcentaje del no uso del casco en bicicleta, el consumo de alcohol y/o drogas durante la conducción y los factores de riesgo en la práctica de las actividades acuáticas.
Son necesarias medidas legislativas, campañas publicitarias y programas educativos en la escuela y en el medio sanitario para reducir el riesgo de muerte y lesiones por accidentes en adolescentes.
FINANCIACIÓN
Este trabajo ha sido financiado por la Asociación Española de Pediatría de Atención Primaria (AEPap).
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS: CNE: Centro de Epidemiología • DGT: Dirección General de Tráfico • ESO: Enseñanza Secundaria Obligatoria • OMS: Organización Mundial de la Salud.
BIBLIOGRAFÍA
- Esparza Olcina MJ. Prevención de lesiones infantiles por accidente de tráfico. Asociación Española de Pediatría de Atención Primaria: Recomendaciones PrevInfad/PAPPS [en línea] [actualizado en junio de 2011; consultado el 10/08/2013]. Disponible en www.aepap.org/previnfad/accidentes_trafico.htm
- Sociedad Española de Medicina de Familia y Comunitaria (semFYC). Estudio sobre accidentes infantiles atendidos en los Centros de Salud. Sociedad Española de Medicina de Familia y Comunitaria y Fundación MAPFRE. 2010 [en línea] [consultado el 10/10/2013]. Disponible en www.fundacionmapfre.org/fundacion/es_es/prevencion-salud-medio-ambiente/publicaciones-y-estudios/estudios/prevencion/accidentes-infantiles.jsp
- World Health Organization Regional Office for Europe. Matching the lowest injury mortality rate could save half a million lives per year in Europe. WHO/Europe Fact sheet 26 June 2006 [en línea] [consultado el 10/10/2013]. Disponible en www.euro.who.int/en/what-we-do/health-topics/disease-prevention/violence-and-injuries/facts-and-figures/matching-the-lowest-injury-mortality-rate-could-save-half-a-million-lives-per-year-in-europe2
- Peden M, Oyegbite K, Ozanne-Smith J, Hyder AA, Branche C, Rahman A, et al. World report on child injury prevention. World Health Organization. 2008 [en línea] [consultado el 10/10/2013]. Disponible en http://whqlibdoc.who.int/publications/2008/9789241563574_eng.pdf
- Da Cuña Vicente R.Accidentes en niños asistidos por el Servicio de emergencias sanitarias de Castilla y León. Epidemiología y análisis cronobiológico de 10.933 casos. Tesis doctoral. Valladolid; 2012.
- Hanfling MJ, Gill AC. Overview of Pediatric injury prevention: epidemiology; history; application. UpTDate. 30, Abril, 2008 [en línea]. Disponible en www.uptodate.com
- Fraga A, Fraga G, Stanley C, Constantini T, Coimbra R. Children at danger: injury fatalities among children in San Diego County. Eur J Epidemiol. 2010;25(3):211-17.
- World Health Organization. Child and adolescent injury prevention: a WHO plan of action 2006-2015. Geneva: WHO 2006 [en línea] [consultado el 10/10/2013]. Disponible en http://whqlibdoc.who.int/publications/2006/9241593385_eng.pdf
- Sethi D, Racioppi F, Baumgarten I, Vida P. Injuries and violence in Europe. Why they matter and what can be done. Copenhagen, Denmark: World Health Organization Regional Office for Europe; 2006 [en línea] [consultado el 10/10/2013]. Disponible en www.euro.who.int/__data/assets/pdf_file/0005/98762/E88037.pdf
- Rivara FP, Grossman D. Control de las lesiones. En: Nelson (ed.). Tratado de Pediatría, 18.ª ed. Barcelona: Elsevier; 2009. p. 366-74.
- Pou J, Luaces C. Accidentes infantiles. Intoxicaciones. En: Cruz M (ed.). Manual de Pediatría, 2.ª ed. Madrid: Ergón; 2008. p. 1095-101.
- Brooks F, Van der Sluijs W, Klemera E, Morgan A, Magnusson J, Gabhainn SC, et al. Young People’s Health in Great Britain and Ireland. Findings from the Health Behaviour in School-Aged Children Study 2006. HBSC International Coordinating Centre. Child and Adolescent Health Research Unit (CAHRU) The Moray House School of Education. The University of Edinburgh. St Leonard's Land. Holyrood Road. Edinburgh EH8 8AQ. Scotland, UK [en línea] [consultado el 10/10/2013]. Disponible en www.nuigalway.ie/hbsc/documents/2009_young_peoples_health_in_gb__ireland.pdf
- University of California. Adolescent Questionnaire. California Health Interview Survey. CHIS 2009 [en línea] [consultado el 10/10/2013]. Disponible en www.chis.ucla.edu
- World Health Organization Regional Office for Europe. Health Behaviour in School-aged Children (HBSC) study: international report from the 2009/2010 survey. Copenhagen, WHO Regional Office for Europe, 2012 (Health Policy for Children and Adolescents, No. 6) [en línea] [consultado el 10/10/2013]. Disponible en www.euro.who.int/__data/assets/pdf_file/0003/163857/Social-determinants-of-health-and-well-being-among-young-people.pdf
- Ministerio de Sanidad, Política Social e Igualdad. Encuesta nacional de salud de España 2006. Ministerio de Sanidad, Política Social e Igualdad en Portal estadístico del SNS [en línea] [consultado el 10/10/2013]. Disponible en www.msssi.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2006.htm
- Moreno-Rodríguez C, Muñoz Tinoco V, Pérez Moreno PJ, Sánchez Queija I, Granado Alcon MC, Ramos Valverde P, et al. Desarrollo adolescente y salud. Resultados del estudio HBSC 2006 con chicos y chicas españoles de 11-17 años. Madrid: Ministerio de Sanidad, Política Social e Igualdad 2008 [en línea] [consultado el 10/10/2013]. Disponible en http://grupo.us.es/estudiohbsc/index.php/es/publicaciones/libros/libros-nacionales
- Nebot M, Pérez A, García-Continente X, Ariza C, Espelt A, Pasarín M, et al. Informe FRESC 2008. Resultats principals. Barcelona: Agència de Salut Pública de Barcelona, 2010 [en línea] [consultado el 10/10/2013]. Disponible en www.aspb.cat/quefem/docs/Informe_FRESC_resultats2008.pdf
- Ministerio de Sanidad y Consumo. Secretaría General de Sanidad. Delegación del Gobierno para el Plan Nacional sobre Drogas. Encuesta Estatal sobre Consumo de Drogas entre Estudiantes de Enseñanza Secundaria de 14 a 18 años (ESTUDES), 2006-2007. Ministerio de Sanidad, Política Social e Igualdad en Plan Nacional sobre Drogas [en línea] [consultado el 10/10/2013]. Disponible en www.pnsd.msc.es/Categoria2/observa/pdf/Estudes2006-2007.pdf
- Schiaffino A, Moncada A, Martín A. Estudi EMCSAT 2008. Conductes de salut de la població adolescent de Terrassa, 1993-2008. Ajuntament de Terrassa: Servei de Salut Comunitària, Desembre 2009.
- Servicio epidemiología Comunidad de Madrid. Hábitos de salud en la población juvenil de la Comunidad de Madrid, 2010. Resultados del sistema de vigilancia de factores de riesgo asociados a enfermedades no transmisibles en población juvenil (SIVFRENT-J), 2010. Boletín Epidemiológico de la Comunidad de Madrid. 2011;17(4):3-38.
- Boyce W, Torsheim T, Currie C, Zambon A. The Family Affluence Scale as a measure of national wealth: Validation of an adolescent self-report measure. Soc Indic Res. 2006;78:473-87.
- World Health Organization Regional Office for Europe. European Detailed Mortality Database. Copenhague: WHO Regional Office for Europe [en línea] [actualizado en septiembre de 2013; consultado el 10/10/2013]. Disponible en http://data.euro.who.int/dmdb/
- Graine MA. Sex differences, effects of sex-stereotype conformity, age and internalization on risk-taking among pedestrian adolescents. Saf Sci. 2009;47:1277-83.
- Instituto Carlos III. Estadísticas de mortalidad por causas en España 2003-2011. Instituto Carlos III: Servicios Científico-Técnicos: Epidemiología: Mortalidad [en línea] [consultado el 10/08/2013]. Disponible en www.isciii.es/ISCIII/es/contenidos/fd-servicios-cientifico-tecnicos/fd-vigilancias-alertas/mortalidad-cne.shtml
- International Traffic Safety Data and Analysis Group. Road Safety Annual Report 2011. IRTAD Annual Report OECD/ITF 2012 [en línea] [consultado el 10/08/2013]. Disponible en www.dgt.es/was6/portal/contenidos/documentos/seguridad_vial/estudios_informes/11IrtadReport.pdf
- Dirección General de Tráfico. Las principales cifras de la siniestralidad vial. España 2011. Dirección General de Tráfico: Seguridad vial: Estadística e indicadores [en línea] [consultado el 10/08/2013]. Disponible en www.dgt.es/portal/es/seguridad_vial/estadistica/publicaciones/princip_cifras_siniestral/
- Thompson DC, Rivara F, Thompson R. Helmets for preventing head and facial injuries in bicyclists. Cochrane Database Sys Rev. 2000;(2):CD001855.
- Coleman P, Munro J, Nicholl J, Harper R, Kent G, Wild D. The effectiveness of interventions to prevent accidental injury to young persons aged 15-24 years: a review of the evidence. Sheffield: University of Sheffield, School of Health and Related Research, Medical Care Research Unit. 1996 [en línea] [consultado el 10/08/2013]. Disponible en www.crd.york.ac.uk/CRDWeb/ShowRecord.asp?View=Full&ID=11996008507#.UkHu6DbIaCo
- Monclús J. Instituto de seguridad vial-Fundación MAPRE. Casco de ciclistas. Trabajo realizado con la colaboración y supervisión de la Fundación MAPFRE; 2013.
- Suelves JM. Lesiones no intencionadas en la infancia y la adolescencia: rompiendo el tópico de la mala suerte. Barcelona: Observatorio de Salud de la Infancia y la Adolescencia del Hospital Sant Joan de Déu; 2009 [en línea] [consultado el 10/08/2013]. Disponible en http://faros.hsjdbcn.org/adjuntos/285.1-Informe_Faros_2_Cast.pdf
- Seguí-Gómez M, López-Váldés FJ. Recognizing the importance of injury in other policy fórums: The case of motorcycle licensing policy in Spain.Inj Prev. 2007;13(6):429-30.
- Macpherson A, Spinks A. Bicycle helmet legislation for the uptake of helmet use and prevention of head injuries. Cochrane Database Syst Rev 2007;(2):CD005401.
- Gorrotxategi Gorrotxategi P, Gonález Conde L, Ibarguren Aguirre O. Utilización del casco en bicicleta y motocicleta. An Pediatr (Barc). 2005;62:338-9.
- Hargutt V, Krüger HP, Knoche A. Driving under the influence of alcohol, illicit drugs and medicines. Risk estimations from different methodological approaches. DRUID. Project co-funded by the European Commission with the Sixth Framework program. DELIVERABLE 1.3.1 (2011).