
Vol. 14 - Num. 55
Originales
Déficit de atención con hiperactividad. Perspectiva desde Atención Primaria
Amalia Pérez Payáa, A Lizondo Escudera, C García Lópeza, E Silgo Gauchea
aPediatra. CS de Catarroja. Valencia. España.
Correspondencia: A. Pérez. Correo electrónico: amperezp@comv.es
Cómo citar este artículo: Pérez Payá A., Lizondo Escuder A, García López C, Silgo Gauche E. Déficit de atención con hiperactividad. Perspectiva desde Atención Primaria. Rev Pediatr Aten Primaria. 2012;14:225-9.
Publicado en Internet: 19-09-2012 - Número de visitas: 20303
Resumen
Introducción: el déficit de atención con hiperactividad (TDAH) es un trastorno neuropsiquiátrico común en la infancia y en la adolescencia. Sin embargo, existen pocos estudios que muestren la situación actual de este trastorno desde la perspectiva del pediatra de Atención Primaria.
Material y métodos: a fecha de 1 de julio de 2011, fueron seleccionados los pacientes de edad comprendida entre 6 y 14 años de edad controlados en el centro de salud de Catarroja que presentaban el diagnóstico de TDAH. A partir de la historia clínica se procedió a la recogida de datos del paciente, de los profesionales involucrados en el diagnóstico, del tratamiento y del seguimiento.
Resultados: de los 2466 niños entre 6 y 14 años de edad registrados, 47 estaban diagnosticados de TDAH (1,9%). La mayoría de los pacientes fueron remitidos desde Pediatría de Atención Primaria para ser estudiados por Neuropediatría y/o Psiquiatría infantil. El tratamiento más extendido fue el metilfenidato (87%), seguido de atomoxetina (4%). Se realizaron exploraciones complementarias al 32% de los pacientes durante el seguimiento, para descartar otras causas de los síntomas. La existencia de comorbilidades asociadas fue similar a la encontrada en otros estudios. La evolución fue favorable en la mayoría de los pacientes en los que se registró la evolución (36%).
Conclusión: la prevalencia de TDAH encontrada en nuestra área ha sido baja, probablemente debido al diseño del estudio. Los pacientes son diagnosticados y tratados mayoritariamente por las especialidades de Neuropediatría y/o Psiquiatría infantil. Algunos de los pacientes son tratados por el pediatra de cabecera, tendencia que esperamos siga en aumento.
Palabras clave
● Atención Primaria ● Diagnóstico ● Prevalencia ● Trastorno por déficit de atención con hiperactividad ● TratamientoINTRODUCCIÓN
El déficit de atención con hiperactividad (TDAH) es un trastorno neuropsiquiátrico común en la infancia y en la adolescencia1. Su presencia tiene una gran repercusión sobre el desarrollo personal y el entorno familiar del paciente.
Al revisar los trabajos publicados sobre el TDAH, hemos encontrado diversos estudios de prevalencia del trastorno2,3, así como guías y recomendaciones de manejo de los pacientes4,5, pero no trabajos que informen sobre la realidad actual del estos niños, quiénes son los profesionales que los tratan, qué medicaciones toman y la evolución que han tenido.
El pediatra de Atención Primaria (AP), como profesional accesible y debido a su trato continuado con el niño y su familia, está en una posición privilegiada para implicarse en el diagnóstico y tratamiento de los niños con esta patología. Sin embargo, el diagnóstico y el manejo terapéutico de estos pacientes es una tarea compleja que precisa formación específica, experiencia en el uso de los fármacos y, lo que es más importante, tiempo suficiente en las consultas para realizar una entrevista con la duración y la tranquilidad necesarias. No obstante estas limitaciones, tratar a estos pacientes es un reto que resulta atractivo a muchos de los pediatras de AP.
Este estudio trata de aclarar la situación actual del TDAH en nuestra área asistencial. Se trata de un estudio de observación, que recoge datos epidemiológicos y clínicos relevantes de la historia clínica de los pacientes, proporcionando una base para una actitud más intervencionista por parte de los pediatras de de nuestro centro de salud (CS).
MATERIAL Y MÉTODOS
El CS de Catarroja se encuentra en un municipio de la Horta Sud cercano a la ciudad de Valencia. La plantilla incluye a cuatro pediatras y se trabaja con historias clínicas informáticas. El programa informático utilizado (Abucasis), que es el proporcionado por la Conselleria de Sanidad Valenciana, utiliza los diagnósticos de la clasificación de enfermedades CIE-9.
Criterios de inclusión: para determinar los pacientes hemos seleccionado los niños con los diagnósticos activos, a fecha de 01 de julio de 2011, de CIE-9-314 (síndrome hipercinético infantil), CIE-9-314.9 (síndrome hipercinético no especificado), CIE-9-314.2 (trastorno hipercinético de la conducta), CIE-9-314.00 (trastorno por déficit de atención sin hiperactividad) y CIE-9-314.01 (trastorno por déficit de atención con hiperactividad).
Variables: sobre la base de estos diagnósticos, hemos revisado las historias clínicas para recoger los siguientes datos: fecha de nacimiento, remitente, fecha de diagnóstico, profesional, exploraciones complementarias practicadas, presencia de comorbilidad, si el paciente recibe apoyo psicológico y cómo ha evolucionado el niño.
Como remitente hemos considerado a la persona que demanda la atención médica: padres o centro escolar, maestro o gabinete psicopedagógico; como fecha de diagnóstico, la fecha en la que por primera vez aparece el diagnóstico de TDAH en la historia clínica; profesional es quien realiza el diagnóstico e indica medicación o hace el seguimiento terapéutico: neuropediatra, paidopsiquiatra, psicólogo clínico o pediatra. Las comorbilidades registradas han sido la neurológica y la psiquiátrica. En cuanto a la evolución, se ha considerado buena si en la historia había referencia a mejores resultados escolares o mejor comportamiento.
RESULTADOS
Este estudio muestra 47 niños con los diagnósticos anteriormente indicados. Atendemos a 4873 niños, de los cuales 2466 tienen edades entre 6 y 14 años. Esta última cifra es la que se ha utilizado para calcular la prevalencia, que es del 1,9%. Las edades de los niños en el momento del diagnóstico tenían un rango de 2 a 13 años, con una media de ocho años (desviación estándar: 2,5). El número de niños fue 39 y el de niñas ocho.
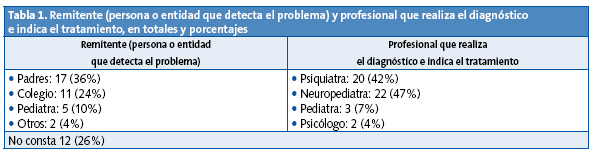
En la Tabla 1 se muestran los remitentes y los profesionales, en números absolutos y en porcentaje. En el caso de los remitentes había 12 niños (26% del número inicial) en cuya historia clínica no constaba el remitente.
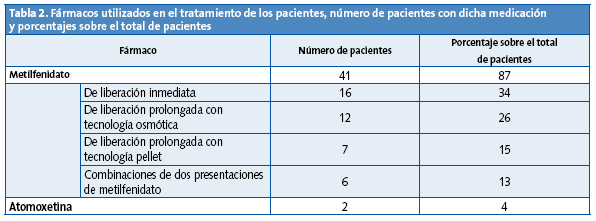
En la Tabla 2 se muestran los tratamientos farmacológicos que siguen los pacientes en la última visita documentada. Solo dos de los pacientes han recibido únicamente terapia psicológica, el resto ha tomado o toma medicación. Varios de ellos han cambiado de compuesto farmacológico a lo largo de su curso evolutivo.
Se realizaron exploraciones complementarias a 15 de los niños (32% del total), estas fueron: ocho electroencefalogramas, seis estudios neurofisiológicos (mapeo cerebral y potenciales evocados auditivos y visuales), dos determinaciones del cociente intelectual, una resonancia nuclear magnética y una tomografía axial computarizada cerebral.
En cuanto a las comorbilidades neurológicas o psiquiátricas, venían reflejadas en la historia de 23 (49%) de los pacientes: ansiedad en un paciente, agresividad en dos, síndrome de La Tourette en uno, enuresis en uno, cefalea en uno, trastorno del lenguaje en cuatro, trastorno de la lectoescritura en tres, epilepsia en tres y fracaso escolar en seis. Diez (21%) pacientes recibían apoyo psicológico: seis acudían a un gabinete psicopedagógico, uno era tratado por la psicóloga del centro de salud mental infantil, dos habían hecho el entrenamiento de memoria COGME y uno terapia neurofeedback. Con respecto a la evolución de los niños, tenemos datos de 17 pacientes (36%): 12 tenían buena evolución, 2 intermedia y 3 mala.
DISCUSIÓN
En primer lugar, cabe destacar la falta de datos del estudio, ya que, debido a su carácter retrospectivo, solo hemos podido valorar los datos que aparecen en la historia clínica, en algunos casos muy escasos.
Tratándose de niños diagnosticados tiempo atrás, el pediatra, con la sospecha diagnóstica y de acuerdo con los padres, remitía al paciente al neuropediatra o al psiquiatra, que eran quienes emitían el diagnóstico definitivo. En este apartado hay que referir que existe bastante presión por parte de los padres para que el niño sea remitido al que ellos denominan “especialista”.
También hay pacientes que se acercan a la consulta de AP pública cuando ya han sido diagnosticados en la medicina privada con el objeto de solicitar las recetas (con descuento) correspondientes a los fármacos prescritos. En estos casos, la información acerca del paciente es muy restringida y puede aumentar erróneamente el número de pacientes con medicación.
En cuanto a la prevalencia encontrada, es más baja que la referida en la literatura médica2. Esto se explica por el hecho de que no es un estudio diseñado para conocer prevalencia, sino un estudio de observación de los niños que acuden a nuestra consulta espontáneamente.
Las edades al diagnóstico y la diferencia entre los sexos sí corresponden a lo reportado6,7.
En cuanto al profesional que efectúa el diagnóstico, se reparte casi por igual entre el neuropediatra y el psiquiatra infantil. En nuestro centro hay una Unidad de Salud Mental Infantil, con la que tenemos una relación muy cercana, por lo que con frecuencia remitimos al psiquiatra si no hay sospecha de alguna alteración neurológica que precise ser valorada por el neurólogo.
Hay tres pacientes que han sido diagnosticados y tratados por el propio pediatra, reflejo de la tendencia actual de que sea el pediatra de AP el haga el diagnóstico y el seguimiento de estos pacientes8.
Las medicaciones administradas son en su mayoría derivados del metilfenidato, en sus diversas presentaciones; como segunda opción terapéutica se encuentra la atomoxetina, y hemos encontrado dos niños que únicamente son tratados con psicoterapia por la psicóloga clínica.
Las exploraciones complementarias realizadas no han sido muy numerosas, de acuerdo con las recomendaciones actuales, en las que no se recomienda la realización sistemática de exploraciones complementarias9, salvo que la anamnesis o la exploración física lo indiquen. Se han efectuado exploraciones neurofisiológicas que, al no ser solicitadas por nosotros, suponemos que entran dentro de las actitudes diagnósticas de los especialistas implicados.
Las comorbilidades encontradas son similares a las reflejadas en la literatura10, destacan el fracaso escolar y las alteraciones del lenguaje y de la lectoescritura como alteraciones predominantes. Tres pacientes tienen epilepsia concomitante y, de ellos, dos siguen tratamiento farmacológico para el TDAH, ya que no está contraindicado.
En cuanto al tratamiento psicológico como complemento al farmacológico y apoyo psicopedagógico, aparece en las historias clínicas en pocos pacientes (21%). Probablemente se trate de un defecto en la cumplimentación de la historia y este se lleve a cabo en más ocasiones de las referidas.
Por último, la evolución de los pacientes, al menos a corto plazo, ha sido satisfactoria en la mayoría de los casos. De nuevo nos encontramos con el problema de la falta de datos, ya que la evolución está registrada en pocas historias.
CONCLUSIONES
En nuestra área, el TDAH está diagnosticado y tratado por una variedad de profesionales. Los pediatras nos estamos implicando progresivamente en su diagnóstico y seguimiento. Las características de los pacientes parecen ajustarse a los datos de epidemiología referidos; los tratamientos administrados y la evolución también se ajustan a las revisiones al respecto.
La falta de datos en las historias clínicas ha sido el principal problema detectado en el estudio.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS: AP: Atención Primaria • CS: centro de salud • TDAH: trastorno por déficit de atención con hiperactividad.
BIBLIOGRAFÍA
- American Psychiatric Association. DSM-IV TR. Manual diagnóstico y estadístico de los trastornos mentales-IV. Texto revisado. Barcelona: Masson; 2001.
- Cardo E, Servera M, Llobera J. Estimation of the prevalence of attention deficit hyperactivity disorder among the standard population on the island of Majorca. Rev Neurol. 2007;44:10-4.
- Rodríguez Molinero L, López JA, Garrido M, Sacristán AM, Martínez MT. Estudio psicométrico-clínico de prevalencia y comorbilidad del trastorno por déficit de atención con hiperactividad en Castilla y León (España). Rev Pediatr Aten Primaria. 2009;11:251-70.
- Grupo de trabajo de la Guía de Práctica Clínica sobre el Trastorno por Déficit de Atención con Hiperactividad (TDAH) en Niños y Adolescentes. Fundació Sant Joan de Déu, coordinador. Guía de Práctica Clínica sobre el trastorno por Déficit de Atención con Hiperactividad (TDAH) en Niños y Adolescentes. Plan de Calidad para el Sistema Nacional de Salud del Ministerio de Sanidad, Política Social e Igualdad. Agència d’Informació, Avaluació i Qualitat (AIAQS) de Cataluña, 2010. Guías de Práctica Clínica en el SNS. AATRM Nº 2007/18.
- Rubió Badía J, Mena Pujol B, Murillo Abril B. El pediatra y la familia de un niño con TDAH. Rev Pediatr Aten Primaria. 2006;8 Supl 4:S199-216.
- Criado Alvarez JJ, Romo Barrientos C. Variability and tendencies in the consumption of methylphenidate in Spain. An estimation of the prevalence of attention deficit hyperactivity disorder. Rev Neurol. 2003;37(9):806-10.
- Boneti M, Clavenne A. The epidemiology of psychotropic drug use in children and adolescents. Int Rev Psichiatry. 2005;17(3)181-8.
- Subcommittee on Attention-Deficit/Hyperactivity Disorder, Steering Committee on Quality Improvement and and Management. ADHD: Clinical Practice Guideline for the Diagnosis, Evaluation and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. Pediatrics. 2011;128(5):1007-22.
- Subcommitee on Attention-Deficit/Hyperactivity Disorder and Committee on Quality Improvement. Clinical practical guideline: diagnosis and evaluation of the child with Attention-Deficit/Hyperactivity Disorder. American Academy of Pediatrics. Pediatrics. 2000;105:1158-70.
- Jensen PS, Martin D, Cantwell DP. Comorbidity in ADHD: implications for research, practice and DSM-V. J Am Acad Child Adolesc Psychiatry. 1997;36(8):1065-86.