Vol. 14 - Num. 54
Originales
Hábitos de estilo de vida en adolescentes con sobrepeso y obesidad (Estudio Obescat)
Lefa S. Eddy Ivesa, I Moral Peláezb, C Brotons Cuixarc, Elisa de Frutos Gallegod, C Calvo Terradese, N Curell Aguilàf
aPediatra. Centre Mèdic Sant Ramon. Santa Coloma de Gramenet. Barcelona. España.
bDiplomada en Estadística. Unidad de investigación EAP Sardenya-IIB Sant Pau. Barcelona. España.
cEpidemiólogo. Unidad de investigación EAP Sardenya-IIB Sant Pau. Barcelona. España.
dPediatra. ABS Raval Nord. Barcelona. España.
ePediatra. ABS Albera Salut. Perelada. Girona. España.
fPediatra. Institut Dexeus. Barcelona. España.
Correspondencia: L S Eddy. Correo electrónico: lefaseddy@gmail.com
Cómo citar este artículo: Eddy Ives L S, Moral Peláez I, Brotons Cuixar C, de Frutos Gallego E, Calvo Terrades C, Curell Aguilà N. Hábitos de estilo de vida en adolescentes con sobrepeso y obesidad (Estudio Obescat). Rev Pediatr Aten Primaria. 2012;14:127-37.
Publicado en Internet: 06-07-2012 - Número de visitas: 31555
Resumen
Objetivo: evaluar la eficacia de una intervención educativa sobre hábitos de estilo de vida para reducir el índice de masa corporal en adolescentes.
Pacientes y métodos: ensayo clínico de un año de seguimiento realizado en 48 centros de Atención Primaria de Cataluña. Participaron 174 adolescentes entre 10 y 14 años con sobrepeso u obesidad; 87 aleatorizados al grupo intervención y 87 al grupo control. La intervención fue de carácter educativo (hábitos alimentarios y de ejercicio físico) y se realizó en la visita inicial, y a los 1, 3, 6, 9 y 12 meses de seguimiento. Variables de resultados: cambios en hábitos alimentarios y ejercicio físico, cambios en el índice de masa corporal (IMC) y en el perímetro abdominal.
Resultados: edad media 11,81 años (desviación estándar [DE]: 1,21) y 50% mujeres. Completaron el seguimiento 125 participantes (71,8%). Los Z-scores de IMC disminuyeron en ambos grupos (p < 0,001), de un valor medio inicial de 2,35 (DE: 0,46) a 2,06 (DE: 0,60). Los Z-scores de perímetro abdominal se redujeron en ambos grupos: en el grupo intervención de una media de 2,06 a 1,77, y en el grupo control de 2,06 a 1,82 (p < 0,001). La intervención educativa mejoró los hábitos alimentarios (aumento ingesta de fruta, disminución de dulces y de la ingesta de alimentos cuando se está aburrido). La actividad física disminuyó (p = 0,002).
Conclusiones: la intervención educativa fue efectiva para reducir el IMC y el perímetro abdominal en ambos grupos. Hubo mejoría en los hábitos alimentarios, pero no en la práctica de ejercicio.
Palabras clave
● Adolescencia ● Ejercicio físico ● Estudios de seguimiento ● Hábitos alimentarios ● Índice de masa corporal ● ObesidadINTRODUCCIÓN
La prevalencia de sobrepeso y obesidad se ha incrementado drásticamente en las tres últimas décadas, especialmente en países desarrollados. La prevalencia en España según el Estudio EnKid en población de 2 a 25 años es del 13,9% para obesidad y del 12,4% para sobrepeso1. Otros autores han reportado prevalencias similares de sobrepeso y obesidad2-5 y además se ha convertido en un problema de salud pública y es la enfermedad crónica más frecuente en la infancia6-8. Los adolescentes obesos corren el riesgo de continuar siéndolo en la edad adulta, desarrollando, además, otras enfermedades como son hipertensión arterial, hiperlipidemia, síndrome metabólico, diabetes mellitus tipo 2, enfermedad cardiovascular, hepatobiliar, cáncer y complicaciones psicosociales que pueden llegar a reducir la esperanza de vida9,10.
Los expertos consideran que el aumento de la prevalencia no solo se debe a factores genéticos, sino a cambios en el estilo de vida (hábitos alimentarios y de ejercicio físico) asociados a un incremento de ingesta de calorías y un descenso del gasto energético11,12. Para mejorar la prevención y el control de la obesidad, es necesario trabajar con los adolescentes y sus familias ayudándoles a cambiar sus hábitos13-16.
La evaluación del sobrepeso y obesidad se realiza a través de la valoración del índice de masa corporal (IMC) (peso en kilos dividido entre la estatura en metros al cuadrado) y perímetro abdominal (PA), un parámetro indirecto de la distribución de grasa abdominal. Las consultas de Atención Primaria (AP) son el entorno idóneo para realizar promoción y prevención de la salud17, pero falta una clara evidencia de los beneficios de la educación sanitaria18-21.
El propósito de este estudio es determinar la eficacia de una intervención educativa para reducir el IMC en adolescentes de 10 a 14 años con sobrepeso u obesidad atendidos en centros de AP en Cataluña.
PACIENTES Y MÉTODOS
Ensayo clínico multicéntrico en adolescentes con obesidad o sobrepeso atendidos en consultas de AP en Cataluña, aprobado por el Comité Ético de Investigación Clínica del Institut d’Assistència Sanitaria (CEIC-IAS) y registrado en el International Standard Randomised Controlled Trial Register con el número ISRCTN35399598.
Criterios de inclusión: adolescentes 10-14 años de ambos sexos con sobrepeso (percentil del IMC entre 85-95 según edad y sexo) u obesidad (percentil del IMC > 95).
Criterios de exclusión: obesidad mórbida, obesidad secundaria, bulimia nerviosa, retraso mental, dificultades para comprender las recomendaciones, participación actual o reciente en otro ensayo clínico.
Tamaño muestra: asumiendo una desviación estándar (DE) del IMC de 2,5, un error alfa del 5%, una potencia del 80% y posible pérdida de casos del 1%, se necesita una muestra de 110 adolescentes por grupo para detectar una diferencia de 1 en el IMC entre grupos de estudio.
Reclutamiento: se explicaron los objetivos del estudio y se ofreció participar en él a todo adolescente que cumplía los criterios de inclusión y al acompañante respectivo (padres o tutores) que acudían a las consultas del pediatra de AP. En caso de aceptar participar se obtuvo el consentimiento informado y se aleatorizó al adolescente a uno de los grupos de estudio en base a una secuencia de números aleatorios previamente generada de forma centralizada desde la Unidad de Investigación participante en el estudio. En la visita inicial se recogieron datos sociodemográficos y clínicos. El estudio tuvo una duración de un año, completándose en diciembre de 2007.
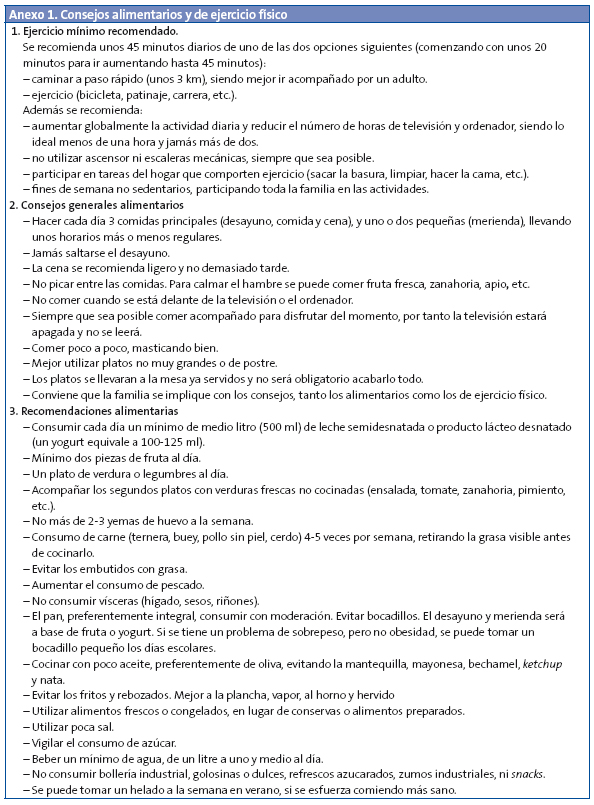
Intervención: los adolescentes del grupo intervención (GI) realizaron una visita inicial más otras cinco en los meses de seguimiento 1, 3, 6, 9 y 12. Los adolescentes del grupo control (GC) realizaron una visita inicial y una visita final al mes 12. En la intervención inicial se realizó educación sanitaria al adolescente en presencia de los padres o tutores para implicar a ambos, proporcionando por escrito consejos basado en recomendaciones nacionales e internacionales11,16,22 (Anexo 1).
En cada control se evaluó la adherencia a las recomendaciones realizadas inicialmente. En las visitas de inicio y final los participantes cumplimentaron un cuestionario de hábitos alimentarios y ejercicio físico.
Variable dependiente: evaluación del IMC y el Z-score asociado. Se calcularon los IMC Z-score utilizando los patrones de crecimiento publicados por la Organización Mundial de la Salud.
Variables independientes: el PA y el Z-score asociado, calculado utilizando los valores publicados en el Estudio EnKid1; hábitos alimentarios y de ejercicio físico, registrados en un cuestionario desarrollado específicamente para el estudio.
Análisis estadístico: se compararon los datos entre los grupos de estudio utilizando la prueba de χ2 en caso de tratar variables cualitativas y las pruebas t de Student para datos independiente o U de Mann-Whitney en caso de analizar variables cuantitativas dependiendo de si cumplían los criterios de aplicabilidad de las pruebas paramétricas o no. El cambio en la variable dependiente entre las visitas inicial y final según grupos de estudio se realizó utilizando el General Linear Model para medidas repetidas. Los datos se analizaron siguiendo el principio de intención de tratar. La significación estadística se considera para valores inferiores a 0,05. El análisis estadístico se realizó con el paquete estadístico SPSS® 15.0.
RESULTADOS
Se seleccionaron 211 adolescentes, de los cuales 37 (17,5%) fueron excluidos por no cumplir criterios de inclusión (Fig. 1).
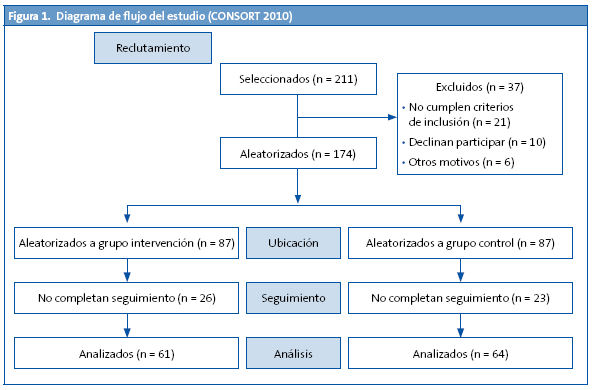
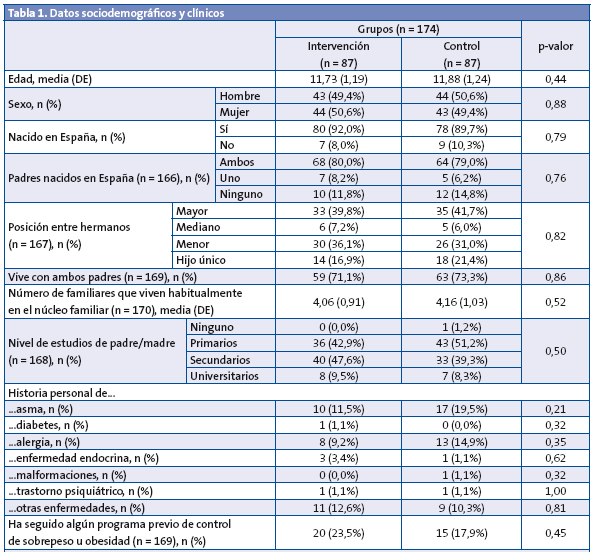
Por tanto, 174 participantes fueron aleatorizados completándose seguimiento en 125 (71,8%). La media de edad fue 11,81 (DE: 1,21); el 50% fueron mujeres (Tabla 1).
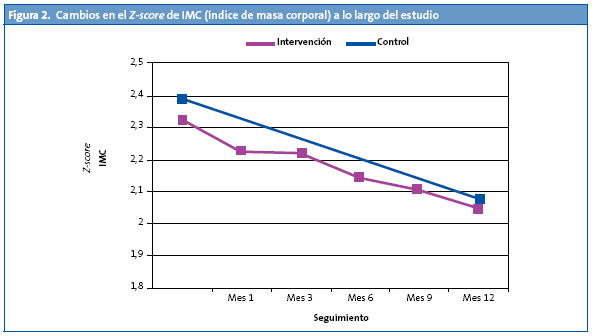
El porcentaje de sobrepeso al inicio era del 26,4%, y el de obesidad del 73,6%. Al final del estudio, un 5,6% de los adolescentes alcanzó un peso normal. Hubo incremento de casos con sobrepeso y descenso de casos con obesidad (34,4 y 60%, respectivamente). El IMC se redujo de una media de 26,25 kg/m2 (DE: 2,70) a 25,99 kg/m2 (DE: 3,02), sin diferenciarse significativamente ambos grupos. Los Z-scores IMC se redujeron significativamente (p = 0,001) pasando de un valor medio inicial de 2,35 (DE: 0,46) a 2,06 (DE: 0,60), lo que significó una reducción aproximado del 12% (Fig. 2).
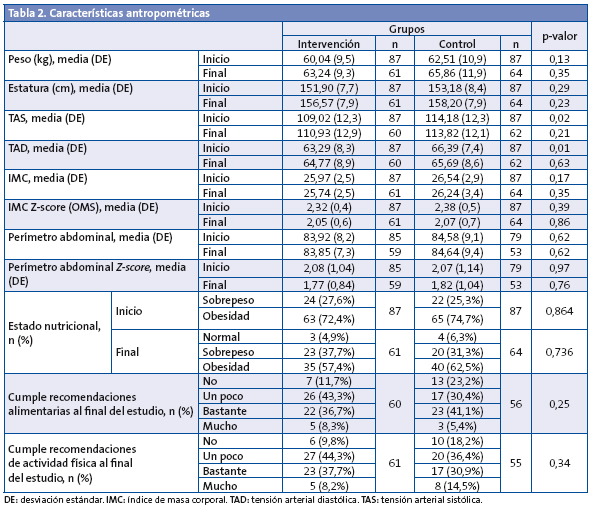
El PA no varió a lo largo del tiempo (p = 0,72) en ninguno de los grupos (p = 0,60). Pero el Z-score del PA se redujo significativamente (p < 0,001) en ambos grupos de forma similar (p = 0,63): en el GI, de una media de 2,08 (DE: 1,04) a 1,77 (DE: 0,84); y en el GC, de una media de 2,07 (DE: 1,14) a 1,82 (DE: 1,04) (Tabla 2).
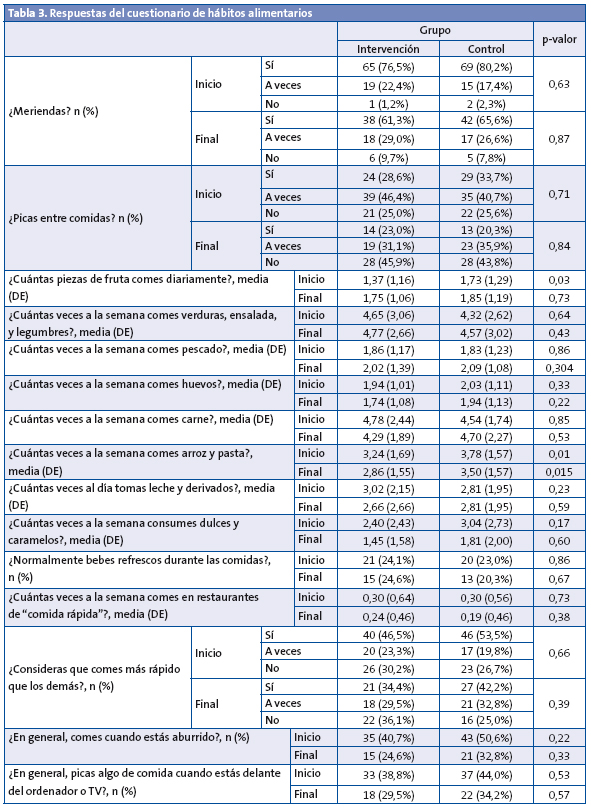
La adherencia a los consejos alimentarios y sobre actividad física fue mayor en el GI que en el GC (88,3 frente a 76,8% y 90,2 frente a 81,8%, respectivamente), sin diferenciarse significativamente ambos grupos. Al inicio del estudio, el GC consumía diariamente más piezas de fruta (p = 0,028) y semanalmente más pasta y arroz (p = 0,010), con la misma tendencia en el consumo de este último al final del estudio (p = 0,015) (Tabla 3).
Al inicio, el 3,4% de los adolescentes no desayunaba, reduciéndose a un 0,8% al finalizar.
En el GI, entre el inicio y el final del estudio, hubo un aumento del consumo de fruta (p = 0,010), un descenso del consumo de leche y derivados (p = 0,028), y un aumento del porcentaje de adolescentes que comían solos (al inicio un 3,2%, al final un 12,9%; p = 0,031). En el GC, cabe destacar el descenso del consumo de comida rápida (p = 0,039). Sin distinción de grupo, los datos a destacar entre inicio y final fueron: descenso del porcentaje de niños que comen más deprisa que los demás (p = 0,018); descenso del porcentaje de niños que comen cuando están aburridos (p = 0,000); aumento del consumo de fruta (p = 0,006) y verdura (p = 0,026); y descenso del consumo de golosinas (p = 0,003).
En cuanto al uso recreativo de pantallas (televisión, videojuegos, ordenador), al inicio la media era 137,63 (DE: 102,38) minutos/día, y deporte 210,19 (DE: 179,03) minutos/semana, sin diferencias significativas entre ambos grupos. Al final del estudio, la media era 138,12 (DE: 120,89) minutos/día y 190,82 (DE: 164,26) minutos/semana, datos sin registrarse diferencias estadísticamente significativas.
Los datos sociodemográficos no mostraron diferencias significativas entre grupos (Tabla 1). El 90% había nacido en España, el 79,5% con ambos padres españoles y el 72,2% vivía con ambos padres. El nivel de formación de la mayoría de los padres se situaba entre estudios primarios y secundarios. Cabe destacar, entre otros datos, una historia familiar de obesidad de un 48,85%, y que el 20,7% había seguido un programa previo de control de peso.
DISCUSIÓN
En ambos grupos, GI y GC, los Z-scores IMC y PA se redujeron significativamente sin diferencias significativas entre ambos, produciéndose al final del estudio un incremento del porcentaje de adolescentes con sobrepeso en relación con los de obesidad. Nuestra hipótesis era que el GI tendría mayor reducción del IMC, ya que en ese grupo se trabajó intensamente en motivar e implicar a la familia, factor importante para lograr adherencia a los consejos educativos24,25. Tres posibles explicaciones son: primero, el efecto Hawthorne26: todos los pacientes sabían que participaban en un ensayo clínico; segundo, la posible influencia de diferentes iniciativas desde el Ministerio de Sanidad y Consumo para el control del sobrepeso (Proyecto NAOS)16, y tercero, el GC recibió una intervención inicial que podría haber tenido su impacto. Un estudio australiano donde el GC fue remitido a una lista de espera de 12 meses y a su vez recibió un folleto sobre hábitos saludables en general, mostró unos resultados similares reduciendo de forma significativa su Z-score IMC, al igual que los dos GI, pero a diferencia del Estudio Obescat no redujeron su Z-score PA27.
Un punto fuerte del Estudio Obescat fue que era un estudio multicéntrico en toda Cataluña, lo que proporciona validez externa al estudio. Pero al mismo tiempo esto podría considerarse un punto débil, al dificultar reuniones periódicas aconsejables para asegurar una metodología de investigación homogénea de los investigadores, hecho subsanado con el soporte on line.
Hubo una pérdida elevada de casos (38,2%) que podría explicarse en parte porque varios pediatras fueron transferidos de su inicial centro de salud a otro. Hay autores que reportan un porcentaje aún mayor de pérdida de casos a los 12 meses (43-47%)28,29. En la revisión Cochrane30 de 2009, con 54 estudios basados en intervenciones educativas, la pérdida de casos variaba entre un 7 y un 43%.
En dicha revisión, la mayoría de las intervenciones fueron llevadas a cabo en atención sanitaria nivel 2 y 3, según el modelo Kaiser. Nuestra intervención se llevó a cabo en AP (nivel 1), donde primero conviene realizarlo en busca de efectividad que evite acudir a los niveles 2-3. También, muchos de los trabajos para prevenir sobrepeso y obesidad son realizados en el entorno escolar, impidiendo trabajar con las familias e implicarlos con los hábitos de una alimentación sana y ejercicio físico regular31-33. Por tanto, otro punto fuerte del Estudio Obescat fue llevarlo a cabo en AP.
Los consejos Obescat fueron útiles para mejorar diversos hábitos alimentarios, pues el consumo de fruta aumentó de forma significativa en el GI, pero como contrapartida hubo un descenso en el consumo de leche y derivados. También se logró un descenso significativo del consumo de golosinas y dulces en ambos grupos. Los hábitos negativos modificados positivamente fueron: descenso en el porcentaje de adolescentes que “picaban” comida cuando estaban aburridos, que picaban entre comidas, y que tenían el hábito de comer más deprisa que los demás. Por tanto, el asesoramiento Obescat les ayudó a tomar conciencia de su relación no saludable con la comida.
Tal como se esperaba, ya que era una muestra de adolescentes con sobrepeso y obesidad, las encuestas mostraron al inicio del estudio unos hábitos de actividad física no deseables: pasaban más de dos horas diarias delante de pantallas, mientras que solo practicaban una media de 30 minutos diarios de actividad física. La Academia Americana de Pediatría recomienda no más de dos horas diarias de televisión de calidad34 y un mínimo de una hora diaria de actividad física15,35,36. A diferencia de los consejos sobre alimentación, los consejos Obescat sobre actividad física no consiguieron cambios positivos. Una posible explicación es que los padres tienen cierto grado de control sobre lo que comen sus hijos, ya que ellos habitualmente compran y cocinan la comida, pero es más difícil que controlen el tiempo que su hijo adolescente practica deporte y actividad física en general. Por tanto, para cambiar los hábitos de ejercicio físico, hay que trabajar sobre todo con el adolescente.
CONCLUSIONES
Una intervención basada en consejos sobre el estilo de vida ha demostrado ser eficaz para reducir el IMC. El Estudio Obescat ha aportado una mejoría en los hábitos alimentarios, pero no en los de actividad física. Por tanto, cuando se realiza el asesoramiento con el adolescente es necesario trabajar más sobre la importancia del ejercicio físico; y cuando se realiza con los padres, hacer énfasis en la importancia de limitar el tiempo del uso recreativo de pantallas. Conviene seguir investigando para perfilar mejor la frecuencia ideal para realizar controles que proporcione efectos beneficiosos a largo plazo.
AGRADECIMIENTOS
Comité directivo: L. Eddy (coordinación), J. M. Bofarull, C. Brotons, N. Calvo, I. Cercós, E. de Frutos, M. A. Diéguez, M. D. Folch, A. M. López-Lorite, I. Moral, E. Olmos, M. A. Peix, P. Plaja, F. Sabate.
Investigadores Obescat: G. Aloy, M. C. Calvo, M. Calvo, C. Campillo, D. Canadell, R. Cortés, M. P. Cortés, N. Curell, M. Domingo, A. Elettrico, G. Fajó, O. Fernández, E. Fortea, M. Gámez, J. García-Lop, A. C. García-López, P. E. García-Pellegri, A. García-Serradell, A. Gatell, L. Gay, M. Giribet, M. González-García, M. Gotzens, A. Harb, J. Jove, J. Molina, V. Morales, A. Moreno, L. Orsola-Santos, E. Orsola-Lecha, C. Palasí, D. Panadés, M. Payola, M. T. Pérez-Vidal, G. Perkal, P. Ramírez, E. Reverter, A. M. Ristol, M. T. Rodríguez-Avilés, P. Ruiz-Cuevas, M. Sánchez-Bonet, L. Sanz, I. Sau, A. Serrano, J. M. Soler, C. Teixidó, A. Valeri, M. Vicente, H. Villena, X. Viñallonga, C. R. Young.
Nuestro agradecimiento a los participantes del Estudio Obescat, a los padres y al personal de campo y laboratorio.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
Financiación: IX Premio de Investigación Nutribén 2007. Datos parciales de este estudio se han presentado en forma de comunicación en el XVIII Symposium Club de Pediatría Social en Barcelona, 7-8 de marzo de 2008, en la 15.ª Reunió Anual de la Societat Catalana de Pediatria en Berga, 16-17 de mayo de 2008, en el 2nd Congress of the European Academy of Paediatrics-EAP en Niza, 24-28 de octubre de 2008 y en el XX Congreso de la Sociedad Española de Medicina de la Adolescencia en Salou, 23-24 de abril de 2010; también en forma de póster en el XXII Congreso Nacional de la Sociedad Española de Pediatría Extrahospitalaria y Atención Primaria en Tenerife, 16-19 de octubre de 2008.
ABREVIATURAS: AP: Atención Primaria • DE: desviación estándar • GC: grupo control • GI: grupo intervención • IMC: índice de masa corporal • PA: perímetro abdominal.
BIBLIOGRAFÍA
- Serra Majem L, Ribas Barba L, Aranceta Bartrina J, Pérez Rodrigo C, Saavedra Santana P, Peña Quintana L. Obesidad infantil y juvenil en España. Resultados del Estudio enKid (1998-2000). Med Clin (Barc). 2003;121:725-32.
- Moreno LA, Mesana MI, Fleta J, Ruiz JR, González-Gross M, Sarría A, et al. The AVENA Study Group. Overweight, Obesity and Body Fat Composition in Spanish Adolescents. Ann Nutr Metab. 2005;49:71-6.
- Albañil MR, Sánchez-Martín M, De la Torre M, Olivas Domínguez A, Sánchez Méndez M, Sanz Cuesta T. Prevalencia de obesidad a los 14 años en cuatro consultas de atención primaria. Evolución desde los dos años. An Pediatr (Barc). 2005;63:39-44.
- Edwards KL, Cade JE, Ransley JK, Clarke GP. A cross-sectional study examining the pattern of childhood obesity in Leeds: affluence is not protective. Arch Dis Child. 2010;95:94-9.
- Singh GK, Kogan MD, van Dyck PC. Changes in State-Specific Childhood Obesity and Overweight Prevalence in the United States From 2003 to 2007. Arch Pediatr Adolesc Med. 2010;164(7):598-607.
- Dietz WH. Overweight in childhood and adolescence. N Engl J Med. 2004;350:855-7.
- Merrick J, Birnbaum L, Kandel I, Morad M. Obesity and adolescence. A public health concern. Int J Adolesc Med Health. 2004;16:387-8.
- Caprio S, Genel M. Confronting the Epidemic of Childhood Obesity. Pediatrics. 2005;115:494-5.
- Duelos Marcos M, Escribano Ceruelo E, Muñoz Velasco F. Obesidad. Rev Pediatr Aten Primaria. 2009;11 Supl 16:s239-s257.
- Sociedad Española para el Estudio de la Obesidad (SEEDO). Consenso SEEDO’2000 para la evaluación del sobrepeso y la obesidad y el establecimiento de criterios de intervención terapéutica. Med Clin (Barc). 2000;115:587-97.
- Han JC, Lawlor DA, Kimm SYS. Childhood Obesity. Lancet. 2010;375:1737-48.
- Maffeis C. Aetiology of overweight and obesity in children and adolescents. Eur J Pediatr. 2000:159 (Suppl 1);S35-S44.
- Barlow SE and the Expert Committee. Expert Committee Recommendations Regarding the Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity: Summary Report. Pediatrics. 2007;120:S164-S192.
- Grupo de trabajo de la guía sobre la prevención y el tratamiento de la obesidad infantojuvenil. Centro Cochrane Iberoamericano, coordinador. Guía de Práctica Clínica sobre la Prevención y el Tratamiento de la Obesidad Infantojuvenil. Madrid: Plan de Calidad para el Sistema Nacional de Salud del Ministerio de Sanidad y Política Social. Agència de’Avaluació de Tecnologia i Recerca Mèdiques; 2009. Guía de práctica clínica: AATRM Nº 2007/25.
- Estrategia para la Nutrición, Actividad Física y Prevención de la Obesidad (Naos). Invertir la tendencia de la Obesidad. Ministerio de Sanidad y Consumo (2005). [En línea] [consultado el 22/09/2011]. Disponible en www.naos.aesan.msc.es/naos/ficheros/investigacion/publicacion1estrategianaos.pdf
- Reinehr T, Schmidt C, Toschke AM, Andler W. Lifestyle intervention in obese children with non-alcoholic fatty liver disease: 2-year follow-up study. Arch Dis Child. 2009;94:437-42.
- Lama RA, Alonso A, Gil-Campos M, Leis R, Martínez V, Moráis López A, et al. Obesidad Infantil. Recomendaciones del Comité de Nutrición de la Asociación Española de Pediatría. Parte I. Prevención. Detección Precoz. Papel del pediatra. An Pediatr (Barc). 2006;65:607-15.
- Moore H, Summerbell CD, Greenwood DC, Tovey P, Griffiths J, Henderson M, et al. Improving management of obesity in primary care: cluster randomised trial. BMJ. 2003;327:1085.
- Wilfley DE, Tibbs TL, Van Buren DJ, Reach KP, Walker MS, Epstein LH, et al. Lifestyle Interventions in the Treatment of Childhood Overweight: A Meta-Analytic Review of Randomized Controlled Trials. Health Psychol. 2007;26 (5):521-32.
- Summerbell CD, Ashton V, Campbell KJ, Edmunds L, Kelly S, Waters E, et al. Interventions for treating obesity in children. Cochrane Database of Systematic Reviews 2003;(3):CD001872.
- Gibson LJ, Peto J, Warren J M, dos Santos Silva I. Lack of evidence on diets for obesity for children: a systematic review. Int J Epidemiol. 2006;35 (6):1544-52.
- Daniels SR, Arnett DK, Eckel RH, Gidding SS, Hayman LL, Kumanyika S, et al. Overweight in Children and Adolescents: Pathophysiology, Consequences, Prevention, and Treatment. Circulation. 2005:111;1999-2012.
- De Onis M, Onyango A, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. 2007;85: 661-668.
- West F, Sanders MR, Cleghom GJ, Davies PS. Randomised clinical trial of a family-based lifestyle intervention for childhood obesity involving parents as the exclusive agents of change. Behav Res Ther. 2010;48:1170-9.
- Story MT, Neumark-Stzainer DR, Sherwood NE, Holt K, Sofka D, Trowbridge FL, et al. Management of Child and Adolescent Obesity: Attitudes, Barriers, Skills, and Training Needs Among Health Care Professionals. Pediatrics. 2002;110:210-4.
- McCarney R, Warner J, Iliffe S, van Haselen R, Griffin M, Fisher P. The Hawthorne Effect: a randomised, controlled trial. BMC Med Res Methodol. 2007;7:30.
- Golley RK, Magarey AM, Baur LA, Steinbeck KS, Daniels LA. Twelve-Month Effectiveness of a Parent-led, Family-Focused Wight-Management Program for Prepubertal Children: A Randomized, Controlled Trial. Pediatrics. 2007;119;517-25.
- Díaz RG, Esparza-Romero J, Moya-Camarena SY, Robles-Sardín AE, Valencia ME. Lifestyle Intervention in Primary Care Settings Improves Obesity Parameters among Mexican Youth. J Am Diet Assoc. 2010;110:285-90.
- Savoye M, Shaw M, Dziura J, Tamborlane WV, Rose P, Guandalini C, et al. Effects of a Weight Management Program on Body Composition and Metabolic Parameters in Overweight Children. A Randomized Controlled Trial. JAMA-2007;297:2697-704.
- Oude Luttikhuis H, Baur L, Jansen H, Shrewsbury VA, O'Malley C, Stolk RP, et al. Interventions for treating obesity in children. Cochrane Database of Systematic Reviews. 2009;(1):CD001872.
- Robertson W, Friede T, Blissett J, Rudolf MC, Wallis M, Stewart-Brown S. Pilot of “Families for Health”: community-based family intervention for obesity. Arch Dis Child. 2008:93:921-6.
- Epstein LH, Valoski A, Wing RR, McCurley J. Ten-year outcomes of behavioural family-based treatment for childhood obesity. Health Psychol. 1994;13:373-83.
- Heinberg LJ, Kutchman EM, Berger NA, Lawhun SA, Cuttler L, Seabrook RC, et al. Parent involvement is associated with early success in obesity treatment. Clin Pediatr (Phila). 2010;49(5):457-65.
- American Academy of Pediatrics, Committee on Public Education. Children, adolescents, and television. Pediatrics. 2001;107:423-6.
- Active Healthy Living: Prevention of Childhood Obesity Through Increased Physical Activity Council on Sports Medicine and Fitness and Council on School Health. Pediatrics. 2006;117(5):1834-42.
- Lau DC, Douketis JD, Morrison KM, Hramiak IM, Sharma AM, Ur E, for the members of the Obesity Canada Clinical Practice Guidelines Expert Panal. 2006 Canadian CPG on the management and prevention of obesity in adults and children. CMAJ. 2007;176 (Suppl 8):S1-13.