
Vol. 25 - Num. 100
Original Papers
Tonsillopharyngitis and streptococcus, enemy or colonizer?
Celia Rasero Bellmunta, Germán Lloret Ferrándizb, Javier González de Diosc
aServicio de Pediatría. Hospital General Universitario Dr. Balmis. Alicante. España.
bServicio de Pediatría. Hospital General Universitario Dr. Balmis. ISABIAL-Instituto de Investigación Sanitaria y Biomédica. Alicante. España.
cServicio de Pediatría. Hospital General Universitario Dr. Balmis. Departamento de Pediatría. Universidad Miguel Hernández. ISABIAL-Instituto de Investigación Sanitaria y Biomédica. Alicante. España.
Correspondence: C Rasero. E-mail: celiarasero68@gmail.com
Reference of this article: Rasero Bellmunt C, Lloret Ferrándiz G, González de Dios J. Tonsillopharyngitis and streptococcus, enemy or colonizer? . Rev Pediatr Aten Primaria. 2023;25:e105-e111. https://doi.org/10.60147/c47a3ba2
Published in Internet: 14-11-2023 - Visits: 22252
Abstract
Introduction: the most frequent aetiology of acute pharyngitis (AP) is viral, and among the bacterial causes, Streptococcus pyogenes is a colonizer that cannot be overlooked in the healthy paediatric population. The aim of the study was to determine how the rapid streptococcal diagnostic test (RST) is used in paediatric emergency departments in order to optimize its use and reduce the overdiagnosis of acute streptococcal pharyngitis (SP) and antibiotic prescribing.
Material and methods: we collected retrospective data on the number of RSTs performed on patients managed in the paediatric emergency department of a tertiary care hospital between January 2022 and January 2023 (both included). We also collected data on the number of patients who underwent more than one RST and the time elapsed between tests.
Results: during the 13-month study period, a total of 1610 RSTs were performed (43% in children < 5 years). More than one RST was performed in 89 patients (53% in children < 5 years), and 40% of additional tests were performed within 40 days of the previous one.
Discussion: microbiological tests for S. pyogenes cannot differentiate between active infection and healthy carriage. Based on the findings of our study, there seems to be an inadequate use of RDTs; most tests are performed in children aged less than 5 years, in whom a streptococcal aetiology is less frequent and healthy carrier status predominates. This leads to overdiagnosis of acute SP, antibiotic overuse, adverse events and bacterial resistance.
Keywords
● Streptococcus pyogenes ● Acute pharyngitis ● Healthy carrier ● Rapid diagnostic testINTRODUCTION
Year 2023 opened with newspaper headlines underscoring the concern in society and public health administrations about invasive streptococcal disease. This stemmed from an alert issued in the United Kingdom1 on December 2, 2022, warning of an increase in the incidence of infections by Streptococcus pyogenes (group A beta-haemolytic Streptococcus pyogenes, GABHS): from 186 cases in week 46 to 851 cases the week the alert was issued. Among these infections, the predominant forms were those that are most common in the paediatric population, such as tonsillitis or scarlet fever. At the same time, there has been an increase in the frequency of invasive streptococcal disease in children aged less than 10 years, with an incidence of 2.3 cases per 100 000 children aged 1 to 4 years compared to a mean incidence of 0.5 cases in the pre-pandemic years (2017-2019) and 1.1 cases per 100 000 children aged 5 to 9 years compared to a mean incidence of 0.3 cases in the same time period in the pre-pandemic years (2017-2019). The main diseases caused by invasive GABHS infections are pneumonia, septic arthritis, necrotising fasciitis, sepsis and septic shock. The Sociedad Española de Infectología Pediátrica (SEIP, Spanish Society of Paediatric Infectious Diseases) invited our hospital to participate in a nationwide multicentre study to study these infections.
Streptococci are bacteria that may be haemolytic, which led Schötmuller and Brown to classify them according to whether they cause (complete haemolysis, β; incomplete haemolysis, α; no haemolysis, γ). Subsequent work by Lancefield has led to their classification based on the carbohydrates present in the cell wall (20 groups from A to H and from K to V).2 Group A streptococcus causes contagious infectious diseases that are common in the paediatric population, such as impetigo, cellulitis, necrotising fasciitis, suppurative complications (peritonsillar abscesses, lymphadenitis, otitis media, sinusitis), nonsuppurative complications (streptococcal glomerulonephritis, rheumatic fever, PANDAS syndrome) and, needless to say, streptococcal pharyngitis.
Acute pharyngitis (AP) is one of the most frequent reasons for medical visits and inappropriate antibiotic use in paediatric care.3 Its aetiology is most frequently (approximately 75-80% of cases) and the rest are caused by bacterial agent, predominantly GABHS (responsible for 3-7% of total cases of AP in children aged less than 2 years, 5-10% in children aged 2-3 years, 30-40% in children aged 4-13 years and 5-10% in children aged more than 14 years). This bacterial agent causes mild and self-limited AP episodes, with a seasonal pattern (outbreaks in late autumn to early spring), and presenting symptoms that include sore throat of abrupt onset, headache, nausea, vomiting and abdominal pain, and characteristic clinical signs including fever, scarlatiniform rash, tonsillar redness, swelling or exudate, petechiae in the soft palate, a red and swollen uvula and unilateral cervical enlarged lymph nodes (> 1 cm) tender to the touch. The diagnosis of acute streptococcal pharyngitis (SP)3,4 must be based on a positive microbiological test result in the presence of signs and symptoms compatible with infection by GABHS and the absence of signs and symptoms of viral infection. Therefore, the diagnosis of acute SP rests on three pillars: compatible symptoms, compatible signs and a positive microbiological test result.
There are, essentially, two types of microbiological tests for the diagnosis of acute SP: culture and rapid diagnostic tests (rapid strep test, RST).5 Culture is the gold standard of diagnosis, as it offers a high sensitivity and specificity, but its use is limited. Rapid tests are used more commonly, with detection based on the extraction in acid media of carbohydrate antigens present in the plasma membrane (on which the Lancefield classification is based), and offers a sensitivity of 85% and a specificity of 95%, so that a positive result is interpreted as GABHS being the causative agent of AP in the patient (in the presence of compatible signs and symptoms) or GABHS carriage (presence of the infectious agent in the absence of clinical signs or symptoms of disease). Neither of these 2 microbiological methods can differentiate between acute infection and carrier status. In addition, RSTs may yield a false positive result in patients with acute SP tested soon after completion of an antibiotherapy course (for a period estimated to last a month following completion), because there may be remnants of antigen in the pharynx of the patient.
It is known that in children, the proportion of healthy carriers of GABHS during outbreaks may be as high as 50%, with a proportion of up to 20% in schoolchildren.4,6 Furthermore, the healthy carrier status may persist for months, although the probability of transmission and the risk of poststreptococcal glomerulonephritis or rheumatic fever are very low. Approximately 15% of individuals with acute SP become asymptomatic carriers after treatment.6 In addition, the presence of Streptococcus milleri, a commensal bacterium that expresses antigen A, may give rise of false positive results in RSTs.5 The frequency of healthy carrier status decreases with increasing age,7 with a proportion of approximately 66% in children under 5 years, 45% in children aged 5-17 years and 16% in individuals aged more than 17 years. This is an essential factor to consider in the decision to perform a rapid test for, depending on the child’s age, the probability of healthy carriage will be greater or smaller, which in turn affects the validity of the test.
In this framework, the relevant clinical question is whether microbiological tests (culture, RST) are detecting active infection as opposed to colonization of the pharynx by streptococcus and, consequently, whether patients who are carriers of GABHS and have a viral or a bacterial infection caused by a different agent are given inappropriate treatment. In light of this, the primary objective of our study was to assess the use of RSTs in the paediatric emergency department of Hospital General Universitario Dr. Balmis (a tertiary care hospital in the province of Alicante, Spain) in order to optimise the use of this resource and reduce the overdiagnosis of acute SP and the overuse of antibiotic treatment (and the associated adverse events, bacterial drug resistance and increase in health care costs). The secondary objective was to adapt the AP diagnosis algorithm proposed by the Asociación Española de Pediatría (AEP, Spanish Association of Pediatrics) in 2011 based on the clinical experience and results obtained in our paediatric emergency department.
MATERIAL AND METHODS
We collected retrospective data on the number of RSTs and the age of the patients in whom they were performed for the period ranging from January 2022 to January 2023 (both included). These data correspond to all the patients aged less than 15 years managed at the paediatric emergency department of Hospital General Universitario Dr. Balmis. We also collected data stratified by age group on the number of patients in whom more than one RST had been performed and the time elapsed between successive rapid tests.
RESULTS
In the paediatric emergency department of our hospital, 1610 RSTs were performed during the 13-month period under study, corresponding to approximately 4% of the total number of patients treated in that period. Of the total, 688 tests (43%) were carried out in children under 5 years of age and 922 (the remaining 57%) in children aged 5 to 14 years. Table 1 presents the age distribution of the patients in whom the RSTs were performed.
| Table 1. Age distribution of the total number of RST performed in the paediatric emergency department of the Hospital General Universitario Dr. Balmis (January 2022-January 2023) | ||
|---|---|---|
| Age | RSTs (n) | Percentage of total RSTs performed |
| <3 years | 217 | 13% |
| 3-4 years | 237 | 15% |
| 4-5 years | 234 | 15% |
| 5-6 years | 222 | 13% |
| 6-7 years | 145 | 9% |
| 7-8 years | 125 | 8% |
| 8-9 years | 82 | 5% |
| 9-10 years | 63 | 4% |
| 10-11 years | 63 | 4% |
| 11-12 years | 66 | 4% |
| 12-13 years | 53 | 3% |
| 13-14 years | 43 | 3% |
| 14-15 years | 60 | 4% |
| TOTAL | 1610 | 100% |
| RST: rapid strep test. | ||

On the other hand, more than one RST was done in a total of 89 patients, of who 53% were aged less than 5 years. As can be seen in Table 2, the percentage of successive tests performed decreased with increasing patient age. About 40% of these additional RSTs were carried out within 40 days.
| Table 2. Frequency of patients in whom more than one RST was performed and time elapsed between tests, stratified by age (January 2022-January 2023) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age | Number of patients with >1 RST | Days elapsed between successive RSTs | ||||||||
| 1 day | 2 days | 3 days | 4 days | 5-14 days | 15-21 days | 21-40 days | >40 days | Total performed within 40 days (percentage) | ||
| <3 years | 10 | 0 | 1 | 1 | 0 | 2 | 0 | 1 | 5 | 5 (50%) |
| 3-4 years | 22 | 0 | 1 | 0 | 0 | 2 | 1 | 3 | 15 | 7 (31%) |
| 4-5 years | 15 | 1 | 3 | 0 | 2 | 0 | 0 | 1 | 8 | 7 (41%) |
| 5-6 years | 17 | 1 | 2 | 0 | 1 | 1 | 1 | 3 | 8 | 9 (53%) |
| 6-7 years | 6 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 5 | 1 (16%) |
| 7-8 years | 6 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 5 | 1 (16%) |
| 8-9 years | 4 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 2 | 2 (50%) |
| 9-10 years | 3 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 2 | 1 (33%) |
| 10-11 years | 2 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 (50%) |
| 11-12 years | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0< | 0 | 0 (0%) |
| 12-13 years | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 (0%) |
| 13-14 years | 2 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 (50%) |
| 14-15 years | 2 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 (50%) |
| Total (percentage) | 89 (100%) | 4 (5%) | 9 (10%) | 1 (1%) | 3 (3%) | 7 (8%) | 3 (3%) | 9 (10%) | 53 (60%) | 36 (40%) |
| RST: rapid strep test. | ||||||||||

DISCUSSION
It is well known that the most frequent aetiology of AP is viral, in which the symptoms and signs are not easy to differentiate from those of bacterial infection. And we know that the diagnosis and treatment of acute SP requires a microbiological test positive for GABHS. However, as we mentioned above, the microbiological tests currently available for detection GABHS cannot differentiate active infection from carrier status. As a result, the use of RSTs without the correct selection of patients in which these tests are appropriate in paediatric emergency departments and primary care centres may lead to overdiagnosis of acute SP.
On one hand, the combination of clinical signs and symptoms has been used for the development of several clinical prediction rules (Centor, McIsaac, FeverPAIN, Attia) meant to estimate the que probability of Infection of bacterial aetiology based on the resulting score. These rules have been used for the prescription of empirical antibiotherapy when patients meet a certain set of criteria, since the probability of bacterial cause is considered 'high enough' to initiate antibiotic treatment in such cases. This approach omits the third pillar for the diagnosis of acute SP noted above, which is the positive microbiological test result. Another aspect worth highlighting in regard to the use of clinical prediction rules, which may be even more important, is the application of these instruments to identify probable cases of acute SP and thus select patients in whom performance of microbiological tests is indicated. Reviewing the evidence available to date, it is reasonable to conclude that microbiological tests for diagnosis of GABHS should be performed in patients who have compatible signs and symptoms in the absence of manifestations suggestive of viral infection.
In our study, nearly half of the RSTs (43%) were performed in children under 5 years and, as we noted above, in this age group the prevalence of healthy GABHS carrier status is estimated at 66% and streptococcus is estimated to cause 3-10% of AP cases; while in the 5-14 years group the prevalence of carrier status for this pathogen is estimated at 45% and 30-40% of cases of AP have a streptococcal aetiology. Therefore, in our paediatric emergency department, in the period under study, more tests were performed in age groups in which the proportion of healthy carrier status for GABHS is greater and the frequency of a streptococcal aetiology in AP less frequent, which reflects an inadequate use of the tests, as it was not appropriate given the epidemiological context of the patient. There is a high probability that this led to overdiagnosis of acute SP in children under 5 years.
On the other hand, the repetition of the RST in 89 patients (43% in children under 5 years and 50% within 40 days), knowing that they could give false positive results after the completion of antibiotherapy or indicate carrier status, suggests that the repetition of these tests can be dispensed with.
Having said this, we would like to make clear that RST is a tool that can support the presumptive diagnosis of acute SP, and that it should be performed prior to initiating antibiotic treatment. The ease of use, rapid turnaround and wide availability of RSTs in paediatric emergency departments and primary care settings facilitate their use, but may also lead to their overuse. The RST should be performed based on a high suspicion of a bacterial aetiology and interpreted taking into account the possibility of false positives (especially in children under 5 years). This approach may raise concerns about underdiagnosing acute SP, but it is important to remember that this disease is mild and self-limiting and that it rarely causes suppurative and non-suppurative complications in our area.
The findings presented in this article are subject to the limitations of retrospective descriptive studies. However, they provide valuable information on the pattern of use of RSTs in patients with manifestations of AP in the paediatric emergency care setting of a tertiary care hospital. And, in light of all of the above, we propose optimising the use of RSTs and cultures in our paediatric emergency department to reduce the overdiagnosis of PSA, health care costs and the emergence of antibiotic resistance. We propose that clinical criteria (symptoms and signs of bacterial and viral infection), as interpreted by the clinician in the context of each specific case, be used to determine whether the performance of microbiological tests is indicated, for which clinical prediction rules may be helpful to the paediatrician, but not required.
All of the above is summarized in the algorithm presented in Figure 1, which is an adaptation of the one proposed by the AEP4 based on up-to-date scientific evidence and the analysis of clinical data from the paediatric emergency department of our hospital. The first modification is that, given the high prevalence of healthy carriers in children under 5 years of age, we established this age as the cut-off point. Thus, the paediatric population with AP symptoms would be divided into <5 years and 5-15 years age groups, instead of <3 years and 3-15 years. Another modification concerns patients aged 5-15 years, in whom, if symptoms are predominantly indicative of a viral aetiology in the opinion of the clinician, it would not be necessary to use the Centor score modified by McIsaac while, on the other hand, if they present with any symptom suggestive of a bacterial aetiology, this score should be used, and considering the fulfilment of at least 3 criteria necessary for the performance of a RST (since fulfilment of 2 criteria, such as age 3-14 years and a temperature >38 °C, would likely result in the performance of the test in a majority of patients visiting the emergency department, whether the reason for the visit is AP or not).
| Figure 1. Algorithm of the Asociación Española de Pediatría (AEP) adapted for the diagnosis of acute pharyngitis* |
|---|
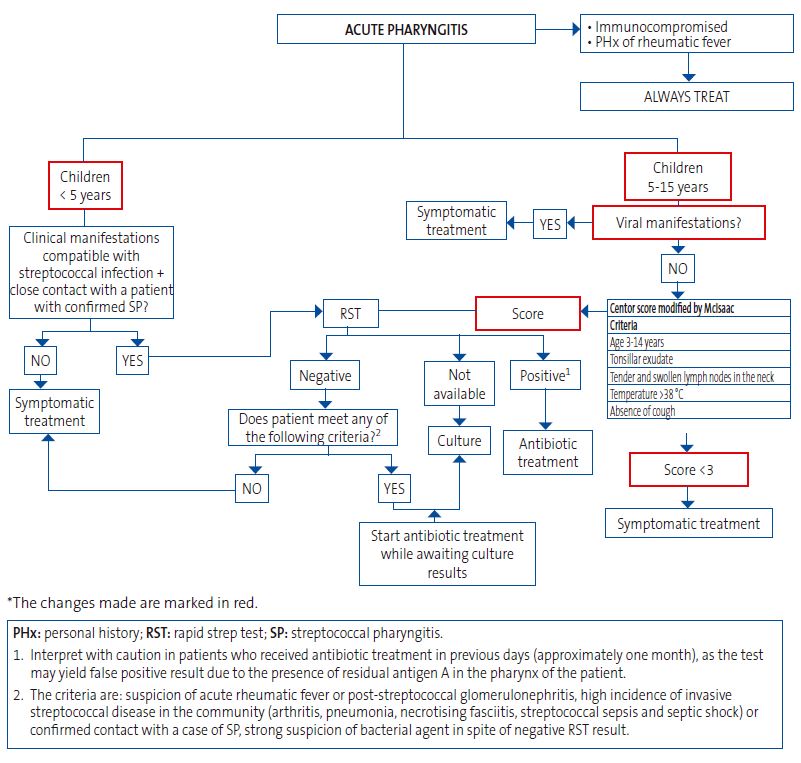 |

The objective is to make appropriate use of rapid tests for detection of GABHS in the pharynx and tonsils, preventing their inappropriate and excessive use, for which it is important to keep in mind that in many cases, GABHS is a colonizer and, much less frequently, a pathogenic foe calling for treatment. For, with the exception of occasional public health alerts, like the one mentioned at the beginning of this article, it is important to keep in mind this balance between the colonizer and foe roles of GABHS in approaching its diagnosis and management in adherence to good clinical practice.8
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
AUTHORSHIP
All authors contributed equally to the development of the published manuscript.
ABBREVIATIONS
AEP: Asociación Española de Pediatría · AP: acute pharyngitis · SP: streptococcal pharyngitis · GABHS: group A beta-haemolytic Streptococcus pyogenes · RST: rapid strep test · SEIP: Sociedad Española de Infectología Pediátrica.
REFERENCES
- Sociedad Española de Infectología Pediátrica. Alerta sobre infecciones invasivas graves por Streptococcus pyogenes. 2022 [online] [accessed 02/03/2023]. Available at www.aeped.es/sites/default/files/alerta_igas-seip_v1.1.pdf
- Bush LM, Vazquez-Pertejo MT. Streptococcal infections. MSD Manual. Professional version [online] [accessed 02/03/2023]. Available at www.msdmanuals.com/professional/infectious-diseases/gram-positive-cocci/streptococcal-infections
- García C. Utilidad del test rápido de detección de antígeno estreptocócico (TRDA) en el abordaje de la faringoamigdalitis aguda en pediatría. Grupo de Patología Infecciosa de la Asociación Española de Pediatría de Atención Primaria. In: AEPap [online] [accessed 02/03/2023]. Available at www.aepap.org/grupos/grupo-de-patologia-infecciosa/contenido
- Piñeiro R, Hijano F, Alvez F, Fernández A, Silva JC, Pérez C, et al. Documento de consenso sobre el diagnóstico y tratamiento de la faringoamigdalitis aguda. An Pediatr (Barc). 2011;75: 342.e1-13. https://doi.org/1016/j.anpedi.2011.07.015
- Hijano F, Piñeiro R, Orden B. Técnicas de detección rápida del antígeno estreptocócico. Guía-ABE. 2012 [online] [accessed 02/03/2023]. Available at www.guia-abe.es/files/pdf/Guia-ABE_RST_estreptococo_v.1_2012.pdf
- Hernández-Aguilera V, Sánchez l, Romao A, Panacci A, Avellaneda J, Rodríguez-Leo C, et al. Estreptococos betahemolíticos y factores asociados al estado de portador asintomático, en escolares de dos municipios del estado Aragua, Venezuela. Comunidad y Salud. 2017;16:9-21.
- Romero A, Requena M, Martínez E, Ladera M, Jeri R. Prevalencia de portadores asintomáticos de Streptococcus pyogenes y Streptococcus pneumoniae en estudiantes del primer año de la Facultad de Odontología de la USMP. Revista KIRU. 2009;6:84-7.
- González de Dios J. Evidencia científica y Medicina de la adolescencia: el camino a la Medicina apropiada. In: Medicina de la Adolescencia. Atención Integral. Madrid: Editorial Ergón; 2019. p. 63-8.