
Vol. 18 - Num. 72
Original Papers
Appropriateness of diagnosis and treatment of acute pharyngotonsillitis to current guidelines
Roi Piñeiro Péreza, Diego Hernández Martínb, Miguel Ángel Carro Rodríguezb, Esther Casado Verrierb, Resurrección Reques Cosmeb, Iván Carabaño Aguadoc
aServicio de Pediatría. Hospital Universitario General de Villalba. Collado Villalba. Madrid. España.
bServicio de Pediatría. Hospital General de Villalba. Collado Villalba. Madrid. España.
cSección de Gastroenterología, Hepatología y Nutrición Pediátrica. Servicio de Pediatría. Hospital Universitario 12 de Octubre. Madrid. España.
Correspondence: R Piñeiro. E-mail: roi.pineiro@quironsalud.es
Reference of this article: Piñeiro Pérez R, Hernández Martín D, Carro Rodríguez MA, Casado Verrier E, Reques Cosme R, Carabaño Aguado I. Appropriateness of diagnosis and treatment of acute pharyngotonsillitis to current guidelines. Rev Pediatr Aten Primaria. 2016;18:317-24.
Published in Internet: 23-11-2016 - Visits: 27968
Abstract
Introduction: acute tonsillopharyngitis (ATP) is one of the most common childhood diseases. The diagnosis and therapeutic management is simple. Further, a consensus document exists in Spain since 2011. The aim of this study is to analyze the appropriateness to consensus in a general hospital, where an author of the consensus document is working.
Patients and methods: a descriptive, cross-sectional, single-center and local study was conducted from January to December 2015. All children ≤ 14 years diagnosed as ATP in the Pediatric Emergency room were included. Clinical records and complementary tools were retrospectively studied.
Results: a total of 176 ATP were analyzed (52.3% girls). Clinical assessment was always performed by McIsaac score. After conducting culture or a rapid antigen-detection test, 46.5% of children received antibiotics. Selection of antimicrobials and prescribed doses were 100% adjusted to consensus. Dose ranges and duration of treatment were >85% appropriated. Only two of 17 pediatricians working on the hospital were responsible of inappropriate prescriptions.
Conclusions: appropriateness is higher than reported in other studies. Rational use of antibiotics could be improved through continuous and regular training by experts in pediatric infectious diseases. In addition, it is suggested to analyze inappropriate prescribers to select pediatricians that should receive specific training. In Spain, it is of primordial importance to adapt the prescribing of antibiotics to the scientific evidence.
Keywords
● Streptococcus pyogenes ● Antibiotics ● Children ● Pharyngitis ● TreatmentINTRODUCTION
The first Spanish national consensus document on the treatment and diagnosis of acute pharyngotonsillitis (APT) in children was published in 2011 through the collaboration of four scientific associations in the field of paediatrics.1 Its main purpose was to deliver a series of key points to paediatricians, paediatric intern resident physicians (MIR) and physicians caring for children. The document stated that there is a tendency to overdiagnose streptococcal APT due to its nonspecific symptoms, with the consequent prescription of unnecessary antibiotics. It also underscored that adapting the prescription of antibiotics to the current scientific evidence was an urgent priority in Spain.
In the past few years, several authors have investigated the appropriateness of antibiotic prescription in different paediatric primary care (PC) and specialty settings,2-6 including studies with a specific focus on APT in children 7-9 and adults.10,11 The findings of these studies vary depending on the year and setting under study. The development of consensus guidelines for the treatment of various paediatric infectious diseases has been associated with improvements in the theoretical knowledge of paediatricians in Spain2 and in the appropriateness of antibiotic treatment in countries like France5 or Italy,6 although improvements in the latter were not found in a small-scale study in adults conducted in Spain.11
The aim of this study was to analyse the appropriateness of APT diagnosis and treatment in children, based on the Spanish consensus guidelines,1 in a secondary hospital with particular interest in the appropriate management of APT, where one of the authors of the national consensus works.
PATIENTS AND METHODS
We conducted a local, single-centre, cross-sectional descriptive study. We performed a retrospective analysis of the discharge summaries and diagnostic tests performed in all children aged 14 years or less that received a diagnosis of APT in the Paediatric Emergency Department between January 1 and December 31, 2015.
- Inclusion criteria: children aged 14 years or less with a working diagnosis coded with the in-house scheme of the hospital, which is based on the International Classification of Diseases, 10th version (ICD-10), as “acute pharyngitis”, “acute tonsillitis”, “scarlet fever” or “strep throat”.
- Exclusion criteria: 1) patients with incorrectly coded diagnoses that, upon review of the discharge summary, we considered not to be cases of APT or scarlet fever with APT; 2) interval of less than a week between two or more diagnoses of APT or scarlet fever in a single patient, in which case the data was grouped into a single episode, and 3) episodes diagnosed as scarlet fever with no associated APT.
We collected data for the following variables: sex; age; working diagnosis; date of diagnosis; discharging physician, prior history of antibiotic use; McIsaac score,12 performance or lack thereof of a rapid antigen detection test (RADT) for streptococcus and its results if applicable; prescription of one or more antibiotics at discharge and, when prescribed, the selected antibiotic, its dosage, interval between doses and duration of treatment; and presence of complications in the six months following diagnosis.
We made a descriptive analysis of qualitative variables by calculating their relative frequencies. There were no quantitative data, as temporal variables were grouped into ranges. Comparison analysis was done by means of the χ2 test or Fisher’s exact test for expected frequencies of less than 5. We conducted the statistical analysis with SPSS® version 22.0.
RESULTS
In 2015, the hospital received 20 996 visits to the paediatric emergency department. Of this total, 199 were coded as APT or scarlet fever. Twenty-three were excluded based on the established criteria: nine episodes of scarlet fever without APT, seven due to inappropriate coding and seven second or third visits due to a single disease process in a period of less than seven days.
We eventually analysed 176 cases of APT (0.84% of the total emergency visits). Of this total, 22 manifested with scarlatiniform rash combined with symptoms of APT; 52.3% in girls; 23.9% in patients aged less than 3 years (median age, 4.5 years). We did not find any significant differences between seasons (P = 0.23).
In the 134 children aged 3 years of less, the clinical assessment was done by means of the McIsaac score, which was 2 or greater in 88.1%. A streptococcal RADT was requested in 72.4%. Table 1 shows the association between the request for rapid testing and the clinical assessment. Rapid testing was requested for 81.4% of children with a McIsaac score of 2 or more. In 75% of the children with a score of 2 or greater in which culture and RADT were not requested, the reason was that they were already being treated with antibiotics without prior microbiological testing. Within this subset, 75% had been prescribed antibiotics in primary care and 25% in private clinics. Furthermore, antibiotic treatment was inappropriate in 42% of cases (three children given azithromycin and two given amoxicillin-clavulanic acid).

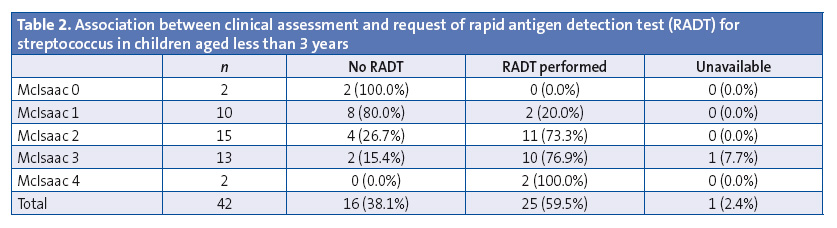
Out of the 42 cases in children aged less than 3 years, rapid testing was requested in 59.5%. Although the consensus guidelines do not call for using the McIsaac criteria in this age group,1 we decided to use this scale to determine the characteristics of cases in which RADT was requested (Table 2). Rapid testing was requested in 83.3% of cases with a score of 2 or greater.
Of the total of 122 RADTs requested, 68 (55.7%) had positive results. Cultures were not performed in any of the cases that tested positive. When it came to cases with a negative RADT result, culture was requested if there was a strong clinical suspicion of streptococcal APT with a McIsaac score of 3 or greater, and culture was also requested in two other cases because RADT was not available; eight out of twenty-seven cultures (29.6%) were positive, all of them for group A beta-haemolytic streptococci (GABHS). There were no Group C or G isolates. Rapid antigen testing in children with McIsaac scores of 3 or greater had a positive predictive value of 70%.
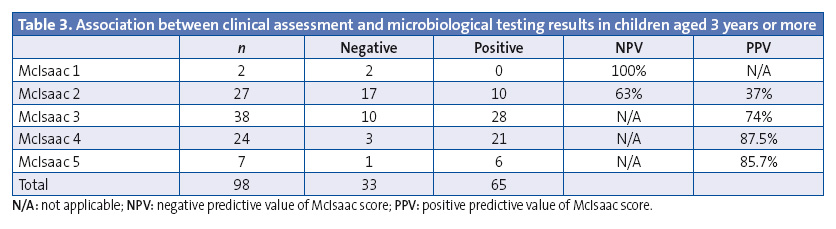
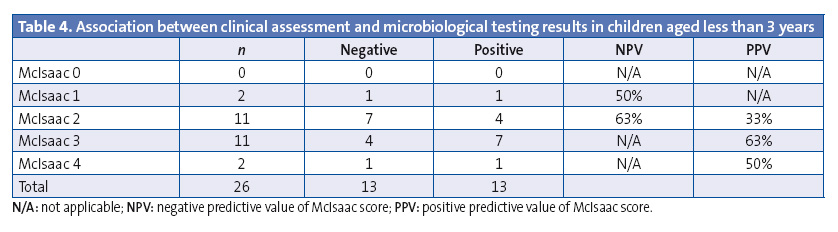
We analysed the association between positive results in microbiological tests (RADT or culture) and the McIsaac score (Tables 3 and 4). Our analysis shows that there is no cut-off point in the McIsaac score that would be appropriate for deciding to initiate antibiotic therapy based on clinical data,1 which the consensus document advises against.
Of the 176 children in the study, 82 (46.5%) received antibiotics: 64.6% phenoxymethylpenicillin, 33% amoxicillin, 1.2% benzathine penicillin G and 1.2% josamycin (due to a known beta-lactam allergy). Therefore, 100% of prescribed antibiotherapy was appropriate based on the consensus.1 In fourteen children, antibiotherapy was initiated despite negative RADT results based on the judgment of the physician in charge. In the eight cases in which culture results were negative, the family was advised to discontinue antibiotic treatment.
The dosage adhered to the consensus guidelines1 in 100% of the cases, too. As for the prescribed duration of oral antibiotherapy, it was 10 days in 85.2% of the children, in adherence to consensus guidelines.1 Other prescriptions were for eight days (12.3%) or seven days (2.5%). When we analysed the intervals between doses, we found that the prescriptions were inappropriate in nine cases (11.1%), with administration of penicillin or amoxicillin every eight hours as opposed to every twelve. We found that inappropriate schedules were prescribed by only two physicians in the department. The rate of complications (local suppurative and nonsuppurative) was 0%.
DISCUSSION
Acute pharyngotonsillitis is one of the most frequent diseases in childhood. Its aetiology is usually viral. The approach to its diagnosis and management is simple and has been established in a consensus document.1 Rapid antigen detection testing should be available in Spain, both in PC and specialty settings, and clinical manifestations must guide paediatricians in ordering microbiological tests, but not in the decision to prescribe antibiotics. However, the medical literature shows that the clinical management of APT diverges significantly from evidence-based recommendations.
According to the results of a survey conducted in Spain13 and published in 1999, 47.3% of physicians believed that GABHS was the most frequent causative agent of APT, and only 20.5% believed that APT most frequently had a viral aetiology. Furthermore, among the latter, one third reported that they would prescribe antibiotics even if they thought the cause was viral. Thus, the results of a study published by Ochoa7 in 2003 that analysed 1716 cases of APT in eleven paediatric emergency departments in Spain come as no surprise. Antibiotic treatment was prescribed in 80.9% of the cases, but RADT or culture was only requested in nine children (0.5%). Of all children aged more than 3 years, 75.9% received antibiotics. Of all prescriptions, 22.8% were classified as treatment of choice (penicillin, or other antibiotics in patients with hypersensitivity to beta-lactam agents), 22.4% as alternative treatments (amoxicillin) and 54.8% as inappropriate (not indicated, or use of other antibiotics in patients with no history of beta-lactam allergy).
In 2005, Herranz14 designed a survey addressed to primary care paediatricians in Madrid. Of all respondents, 23.6% stated that they would always prescribe antibiotics for the treatment of APT, and 40.2% that they would prescribe them often. In 2010, Durán et al3 analysed 100 randomly selected cases of APT in a paediatric emergency department in Barcelona. Rapid antigen testing was performed in 60 cases and was positive in 41.7%. Thirty-six percent of patients with APT received antibiotics (11% amoxicillin-clavulanic acid, and 30% without prior microbiological testing). In 2012, Fernández et all8 studied 563 cases of APT in the paediatric emergency departments of five hospitals and 80 PC clinics. The study did not collect data on microbiological confirmation. The appropriateness of antibiotic treatment had not improved compared to that observed by Ochoa,7 as it was prescribed to 75.5% of the children (78.3% of children aged < 3 years). Antibiotherapy was considered the treatment of choice in 43.3% (penicillin or amoxicillin, or other antibiotics justified by allergy) and inappropriate in 56% (not indicated or with selection of other antibiotics in the absence of a history of allergy).
In 2014, Malo et all4 analysed 40 806 cases of APT in PC settings in Aragón. Antibiotic treatment was prescribed in 75% and considered appropriate in 67% of cases. Amoxicillin-clavulanic acid was prescribed in 25% of cases. The authors acknowledged that paediatricians in this autonomous community did not routinely order RADT. Another relevant study conducted in 2014 was the one by Fierro et al9 in 25 health care centres with the analysis of 52 658 cases of APT. The authors found that 50% of inappropriate prescriptions came from one group of providers, specifically from 8% of 222 prescribing physicians. The authors proposed that interventions targeting specific physicians could improve adherence to evidence-based recommendations. It is apparent that even when clinical guidelines are available, some physicians do not put them into practice. The identification of these professionals and the implementation of measures to correct inappropriate practices could improve antibiotic use in Spain.
There is evidence that consensus guidelines have some impact. This is the case in France,5 where a clinical guideline for the treatment of acute otitis media was published in 2011. Empirical treatment with amoxicillin-clavulanic acid dropped by 28.4% and with cefpodoxime proxetil by 34.3%. However, there was no reduction in the overall percentage of otitis cases treated with antibiotics. A study in Italy had similar findings.6 In Spain, Rico-Ferreira et al11 recently found evidence of non-adherence to clinical guidelines in the treatment of APT in adults, and emphasised the need to implement measures to minimise this problem, to perform qualitative studies to understand the underlying reasons for the inappropriate prescription of antibiotics, and to develop warning systems in electronic health records as an intervention on physicians who are more prone to making inappropriate prescriptions. Similarly, Malo et al4 stated the need to promote continuing education and make health care providers more aware of their responsibility as prescribers. They also proposed involving parents in the process, dispelling false and widespread myths regarding respiratory diseases and the benefits of antibiotic treatment.
The inappropriate prescription of antibiotics stands against the theoretical knowledge of paediatricians, as demonstrated by the results of the ABES survey on the empirical use of antibiotics in children in Spain.2 A total of 1214 paediatricians completed the survey, of who 96% chose penicillin or amoxicillin as the first-line treatment for APT of probable bacterial aetiology, while 3.6% chose amoxicillin-clavulanic acid and only 0.4% chose azithromycin. The authors themselves remarked that one of the limitations of the study was that the questionnaire assessed the selection of antibiotics within a closed set of options, rather than actual antibiotic prescription. They also mentioned a potential selection bias that would result from the recruitment method, as the willingness to complete an electronic survey could be associated with a specific paediatrician profile. At any rate, there seemed to be a clear discrepancy between theoretical knowledge and antibiotic prescribing practices when it came to APT.
The main limitation in our study is that we reviewed electronic health records retrospectively, so it is possible that some features were not properly documented in the discharge summaries. Furthermore, culture was not performed in all cases with a negative RADT, so it is possible that actual cases of streptococcal APT were missed. However, this showed adherence to the consensus guidelines,1 which only recommend culture in cases with a negative RADT if there is a high clinical suspicion of streptococcal involvement or in the presence of risk factors. Another limitation was the sample, which was smaller compared to other studies, and recruited from a single centre.
Despite these limitations, the findings of our case series reflect an excellent adherence to the consensus.1 Only 46.3% of the children were treated with antibiotics, in all cases following microbiological testing. The selected antimicrobials were appropriate in 100% of those treated. When it came to the duration of treatment and the intervals between doses, adherence exceeded 85%. Inappropriate prescriptions were only made by two of the seventeen physicians that staffed our hospital’s paediatric emergency department in 2015.
As for the aetiology of APT, GABHS was responsible for 48.5% of cases in children aged 3 years or more, a proportion that similar although slightly higher than those described in the literature, and for 31% of cases in children aged less than 3 years, which was significantly higher than what has been previously reported.1 Clearly, we cannot determine how many of the positive results may have corresponded to carriers, but in the presence of symptoms compatible with APT, a positive result ought to be interpreted as causative of disease, and based on current evidence, initiation of targeted antibiotic treatment is recommended.1
These data evince three distinct situations, to which we propose different solutions. First of all, there is the situation that was already discussed by Malo4 and Rico-Ferreira.11 It is very likely that interventions in continuing education and awareness-raising on the use of antibiotics would be more successful if they directly targeted specific physicians compared to consensus guidelines addressed to all paediatricians. It goes without saying that consensus guidelines must continue to establish the standards to be followed in Spain, but as a theoretical basis of what must and must not be done, and recognizing that many physicians will not read them and that these are the physicians on which intervention is needed. Identifying physicians that make inappropriate prescriptions is easier now through the review of electronic health records. This is a simple task that should be performed by PC coordinators, paediatrics department chiefs and the competent authorities to improve the use of antibiotics in APT in Spain. This is a feasible objective and, considering the current level of adherence, one that ought to be a priority.
Secondly, our department does not stand out because all its paediatricians are experts in paediatric infectious diseases and in antibiotic stewardship. Instead, one of the writers of the aforementioned consensus document1 is part of the team and regularly educates the department staff on the appropriate management of APT in children. The results of our series demonstrate that it is possible to achieve excellence in the management of this disease. Paediatric infectious disease specialists in each hospital or health care area would be tasked with the continuing education of their own colleagues. Such a measure could also considerably improve the use of antimicrobials.
Thirdly, one of the salient findings of our study was that streptococcus was the causative agent in 31% of children aged less than 3 years. The consensus1 mentions that in this age group, streptococcal APT amounts to less than 10% of the cases, and that rheumatic fever is extremely rare in developed countries. The decision to prescribe antibiotic treatment should be made on a case-to-case basis and only if there are clinical manifestations compatible with streptococcal disease. However, the possibility of invasive disease by GABHS, while rare, is well documented in newborns, infants and toddlers, with a mortality that ranges between 2% and 8%. Although risk factors for developing invasive disease have been described in the literature, cases have also been published that were not associated with any of these predisposing factors.15 Given the potential severity of invasive disease by GABHS, perhaps it would be better to call for a more active search for this microorganism in children aged less than 3 years, guided by clinical scores similar to the one proposed by McIsaac,12 who already adjusted the Centor criteria for age with the purpose of not basing decisions on the diagnosis and treatment of these patients on the personal judgment of each paediatrician, since there is evidence that this results in an unjustified increase in antibiotic prescription.
In summary, we present data on the adherence to consensus guidelines on the diagnosis and treatment of APT1 in a secondary level hospital, which show better results compared to those reported by other case series. One possible explanation is the ongoing and periodic education provided by one of the physicians in the department, who is an expert in the management of this pathology and one of the authors of the national consensus. Furthermore, we propose a potential solution to the inappropriate use of antibiotics for the treatment of APT in Spain that focuses on analysing inappropriate prescriptions and providing specialised training to specific physicians. Last of all, we propose the possibility of revising the 2001 consensus as pertains the diagnosis and treatment of APT in children aged less than 3 years.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS: APT: acute pharyngotonsillitis · ICD-10: International Statistical Classification of Diseases and Related Health Problems, 10th version · GABHS: group A beta-haemolytic streptococcus · PC: Primary Care · MIR: resident intern physician · RADT: rapid antigen detection test.
REFERENCES
- Piñeiro Pérez R, Hijano Bandera F, Álvez González F, Fernández Landaluce A, Silva Rico JC, Pérez Cánovas C, et al. Documento de consenso sobre el diagnóstico y tratamiento de la faringoamigdalitis aguda. An Pediatr (Barc). 2011;75:342.e1-342.e13.
- Piñeiro Pérez R, Calvo Rey C, Medina Claros AF, Bravo Acuña J, Cabrera García L, Fernández-Llamazares CM, et al. Uso empírico de antibióticos en niños en España. Resultados de una Encuesta Pediátrica Nacional 2012 (Estudio ABES). An Pediatr (Barc). 2013;79:32-41.
- Durán Fernández-Feijóo C, Marqués Ercilla S, Hernández-Bou S, Trenchs Sainz de la Maza V, García García JJ, Luaces Cubells C. Calidad de la prescripción antibiótica en un servicio de urgencias pediátrico hospitalario. An Pediatr (Barc). 2010;73:115-20.
- Malo S, Bjerrum L, Feja C, Lallana MJ, Poncel A, Rabanaque MJ. Prescripción antibiótica en infecciones respiratorias agudas en Atención Primaria. An Pediatr (Barc). 2015;82:412-6.
- Levy C, Pereira M, Guedj R, Abt-Nord C, Gelbert NB, Cohen R, et al. Impact of 2011 French guidelines on antibiotic prescription for acute otitis media in infants. Med Mal Infect. 2014;44:102-6.
- Palma S, Rosafio C, Del Giovane C, Patianna VD, Lucaccioni L, Genovese E, et al. The impact of the Italian guidelines on antibiotic prescription practices for acute otitis media in a paediatric emergency setting. Ital J Pediatr. 2015;41:37.
- Ochoa Sangrador C, Vilela Fernández M, Cueto Baelo M, Eiros Bouza JM, Inglada Galiana L, Grupo Español de Estudio de los Tratamientos Antibióticos. Adecuación del tratamiento de la faringoamigdalitis aguda a la evidencia científica. An Pediatr (Barc). 2003;59:31-40.
- Fernández González N, Herrero-Morín JD, Solís Sánchez G, Pérez Méndez C, Molinos Norniella C, Pardo de la Vega R, et al. Variabilidad e idoneidad en el tratamiento antimicrobiano de las faringoamigdalitis agudas pediátricas en Asturias, España. Arch Argent Pediatr. 2012;110:207-13.
- Fierro JL, Prasad PA, Localio AR, Grundmeier RW, Wasserman RC, Zaoutis TE, etal. Variability in the diagnosis and treatment of group a streptococcal pharyngitis by primary care pediatricians. Infect Control Hosp Epidemiol. 2014;35:S79-85.
- Lázaro A, Ochoa C, Inglada L, Eiros JM, Martínez A, Vallano A, et al. Practice variation and appropriateness study of antimicrobial therapy for acute pharyngotonsillitis in adults. Enferm Infecc Microbiol Clin. 1999;17:292-9.
- Rico-Ferreira P, Palazón-Bru A, Calvo-Pérez M, Gil-Guillén VF. Nonadherence to guidelines for prescribing antibiotic therapy to patients with tonsillitis or pharyngotonsillitis: a cross-sectional study. Curr Med Res Opin. 2015;31:1319-22.
- McIsaac WJ, Kellner JD, Aufricht P, Vanjaka A, Low DE. Empirical validation of guidelines for the management of pharyngitis in children adults. JAMA. 2004;291:1587-95[Erratum en JAMA. 2005;294:2700].
- Ripoll Lozano MA, Orero González A, Prieto Prieto J. Etiología y tratamiento de elección de las infecciones respiratorias en Atención Primaria. Opinión de los médicos. Aten Primaria. 1999;23:296-300.
- Herranz Jordán B, Pérez Martín C. Encuesta sobre prescripción de antibióticos en infecciones respiratorias pediátricas. Rev Pediatr At Prim. 2005;28:19-40.
- Plana Fernández M, López Gil A, Gomà Brufau AR, Solé Mira E, Bringué Espuny X. Enfermedad invasiva por Streptococcus pyogenesen lactante sano de 38 días. An Pediatr (Barc). 2007;66:540-1.