
Vol. 15 - Num. 60
Original Papers
Unintentional injuries. Risk factors in road traffic safety and aquatic activity in 13 to 18 years old adolescents
Ana Fierro Urturia, Marta Esther Vázquez Fernándezb, M.ª Fe Muñoz Morenoc, M Alfaro Gonzálezd, Luis Rodríguez Molineroe, P García Gutiérrezf, Grupo de Educación para la Salud de la AEPap
aPediatra. CS Pisuerga. Arroyo de la Encomienda. Valladolid. España.
bPediatra. CS Arturo Eyries. Facultad de Medicina. Universidad de Valladolid. Valladolid. España.
cUnidad de Investigación Biomédica. Hospital Clínico Universitario de Valladolid. Valladolid. España.
dServicio de Pediatra. Hospital de Medina del Campo. Medina del Campo. Valladolid. España.
eServicio de Pediatría. Hospital Recoletas Campo Grande. Valladolid. España.
fPediatra. CS Aranda Norte. Aranda de Duero. Burgos. España.
Correspondence: A Fierro. E-mail: anfier99@gmail.com
Reference of this article: Fierro Urturi A, Vázquez Fernández ME, Muñoz Moreno MF, Alfaro González M, Rodríguez Molinero L, García Gutiérrez P, et al. Unintentional injuries. Risk factors in road traffic safety and aquatic activity in 13 to 18 years old adolescents. Rev Pediatr Aten Primaria. 2013;15:315-28.
Published in Internet: 04-12-2013 - Visits: 40577
Abstract
Introduction: unintentional injuries or accidents signify a public health issue due to their prevalence, morbidity, mortality and high health costs. Accident risk factors’ knowledge has allowed making efficient control and prevention programs.
Objective: evaluating the unintentional injuries needing medical assistance during the last year and assessing Valladolid adolescents’ road traffic safety and aquatic activity practice risk behaviors and their relationship with other factors.
Material and Methods: a survey with questions related to healthy habits, behaviors and conducts was conducted to a sample of 2412 students of 13 to 18 years old of Valladolid (Spain) during 2012. Data related with the risk of accident rate and risk factors on road traffic safety and aquatic activities.
Results: 14% of adolescents have suffered some kind of accident or injury that required medical assistance during the last year. Road traffic safety risk factors were: not using safety helmet when riding a bicycle in 81.5% of adolescents and 6% in the case of riding a motorbike, 1.2% of them do not fasten their seat belt in cars. A few risk factors are noticed in aquatic activities practice. Several sociodemographic and economic variables and risk behaviors are associated with the risk of accident.
Conclusions: our study identifies adolescents’ road traffic safety and aquatic activity practice’ risk factors. Legislative measures, publicity spots, educational programs in school and sanitary environment are required in order to reduce the adolescents’ risk of death and injuries in accidents.
Keywords
● Accident ● Adolescent ● Risk behaviorsINTRODUCTION
Accidents, or unintentional injuries, are one of the biggest issues in Public Healthcare nowadays. They are the leading cause of death in the child and adolescent population in Spain and the European Union, and they are an important source of morbidity and disability with elevated healthcare costs1-5.
Accidents not only impact the healthcare field by requiring services, but they also lead to a host of economic and social problems in families, society, and years of life lost6.
Their causes are multi-factorial, with individual and environmental factors at play. When it comes to individual factors, age has a marked influence, with adolescents being the group at highest risk due to their characteristic traits of inexperience, emotional instability, thrill-seeking, impulsivity, being easily influenced, and needing to show off their skills to their peers, among others4.
Traffic accidents are the main cause of injury in this group, although the risk posed by poisoning, drowning, firearm wounds, falls, and burns is also significant5-7.
Most accidents and their adverse consequences can be avoided with a preventative social, educational, and healthcare approach targeting, depending on the age, parents, educators, and needless to say youth and adolescents likely to engage in risk behaviours.
The World Report on Child Injury Prevention, developed jointly by the World Health Organization (WHO) and UNICEF and published in 2006, gathers all our current knowledge on the various types of child injuries and how to prevent them4-8.
This article presents the results of a descriptive study of situations involving a high risk for accidents, which was performed in the context of a broader project that studies health-related habits and behaviours in a sample of students aged 13 to 18 years in the province of Valladolid (Spain) between March and May of 2012.
The data contributed by this study helps identify some risk behaviours related to road safety and the practise of aquatic sports by adolescents in our province, as well as their relationship with various factors.
We need to know these aspects in order to design efficacious preventive strategies, and the paediatrician is one of the professionals with the highest involvement in the issue of unintentional injuries1,5,9-11.
MATERIALS AND METHODS
Design
We did a descriptive cross-sectional study. The population under study was adolescents aged 13 to 18 years in the province of Valladolid and attending school for the 2nd, 3rd, and 4th year of the Spanish compulsory secondary education (ESO) and 1st and 2nd years of post-compulsory schooling (Bachillerato) under the LOGSE system. We obtained a sample of 2412 adolescents out of the total 18,888 students. The students were selected by random selection of schools (n=14) and then classes, including all the students in those classes in the sample.
The sample size was calculated for an estimated proportion of 50% and a 2.5% significance level for bilateral hypothesis testing, assuming a 10% non-response rate, which resulted in 1566 students. The final number of surveyed students after data cleaning was of 2412 adolescents enrolled in school aged 13 to 18 years.
We made contact with the school administrators by phone and by mail and informed them of the objectives and contents of the study, and agreed on one or more days (not following a holiday) to carry out the survey in the months of March and May of 2012. Three schools refused to participate and did not give a clear reason for it. The schools notified the families of the students that they were going to be asked to participate in the survey, giving the families the chance to refuse with no repercussions.
The research team was in charge of administering the survey. A computer-assisted questionnaire was administered to 69% of the sample, and the rest did the survey in paper format, mainly because not enough computers were available in the computer rooms. The electronic data were automatically stored in the database, while the paper data were entered manually in the same database.
The participating students filled out the questionnaires individually, and were previously informed of the confidentiality of the data and asked not to communicate with each other during the survey. Taking the questionnaire was voluntary and it was done during regular school hours. The time used to fill out the questionnaire was approximately 35-40 minutes. The study design was approved by Comisión de Investigación de la Gerencia de Atención Primaria del Área Oeste [Research Board of the Management of Primary Care of the West Area] of Valladolid.
Questionnaire and fieldwork
The questionnaire included, among others and in addition to items pertaining to accident risk in adolescents, items on socio-demographic variables, leisure activities, academic performance, substance use (tobacco, alcohol, drugs), antisocial behaviour, experiences of abuse and relationships, nutrition, and sexuality, based on the recommendation of international12-14, national15,16 and province and autonomous community17-20 programmes.
The main indicators used in relation to the accident incidence rate of adolescents were the following:
- Students who sustained one or more injuries requiring medical care in the last 12 months.
- Use of the seat belt while travelling in a car.
- Use of a helmet while riding a motorcycle or bicycle.
- Driving under the influence of alcohol or drugs.
- Being an occupant in a vehicle driven by someone under the influence of alcohol or drugs.
- Questions about aquatic sports and high-risk activities (knowing how to swim, diving head-first into a pool, diving off cliffs, going into the water immediately after eating, and ignoring the indications given by life guards).
The study was done between March and May of 2012.
Statistical analysis
Quantitative variables are presented as mean values and a 95% confidence interval, and qualitative values as frequency distributions.
We used Pearson’s chi-square test to analyse the association between accident risk, socio-demographic characteristics, and risk factors. In those cases where the number of cells with expected values below 5 was over 20%, we used Fisher’s exact test or the likelihood-ratio test for variables with more than two categories.
We analysed the data with the SPSS® statistical software version 20.0 for Windows®. We considered p-values lower than 0.05 statistically significant.
RESULTS
For the total of participating students, 2412 questionnaires were considered valid; 47.3% of them were filled out by females, and 52.7% by males. When it came to academic year, 23.5% were filled out by 2nd year students of the ESO; 25.8% by 3rd year students of the ESO; 20.2% by 4th year students of the ESO; 18.9% by 1st year students of the Bachillerato, and 11.6% by 2nd year students of the Bachillerato. Most students were enrolled in schools located in an urban environment (87.3%), and 95.5% came from families with a middle to high socioeconomic status, with the affluence of the family estimated by means of theFamily Affluence Scale (FAS)21.
Injuries and accident incidence rates
Fig. 1 shows the frequency of unintentional injures and of risk behaviours concerning road traffic safety.
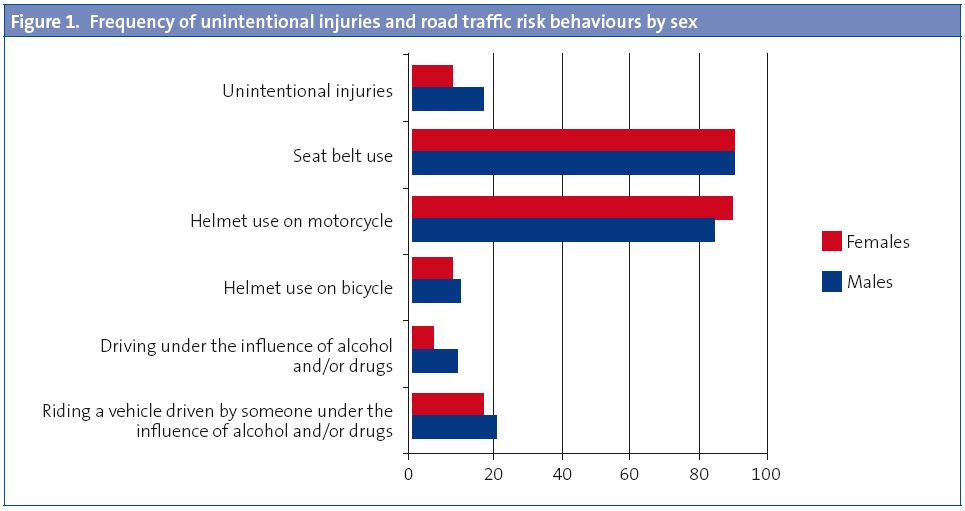
The proportion of children who reported having suffered an accident or injury requiring medical attention in the last 12 months was 14%. The causes reported most frequently (30%) were traumatic injuries (sprains and bone fractures), many of which were caused by falls or practicing sports. Traffic accidents were the cause of 5.3% of the injuries, categorised into car (2.9%), bicycle (1.7%), motorcycle (0.5%) and skateboard (0.2%) accidents. Wounds and concussions accounted for 2%, and 1.2% of the children received care for cranioencephalic trauma.
Males presented a higher accident incidence rate of 17.5% compared to females, at 10.2%, which was statistically significant (p<0.001). We found no difference between academic years.
Road traffic safety
- Use of the safety belt in the car: 93.9% of the adolescents reported using the safety belt regularly or always (93.9% of boys compared to 94.0% of girls) when travelling in a car; 4.9% reported putting it on sometimes (4.6% of boys versus 5.3% of girls), 1.2% did it rarely or never (1.4% of boys versus 0.6% of girls) (p = 0.048). We observed no statistically significant differences between academic years.
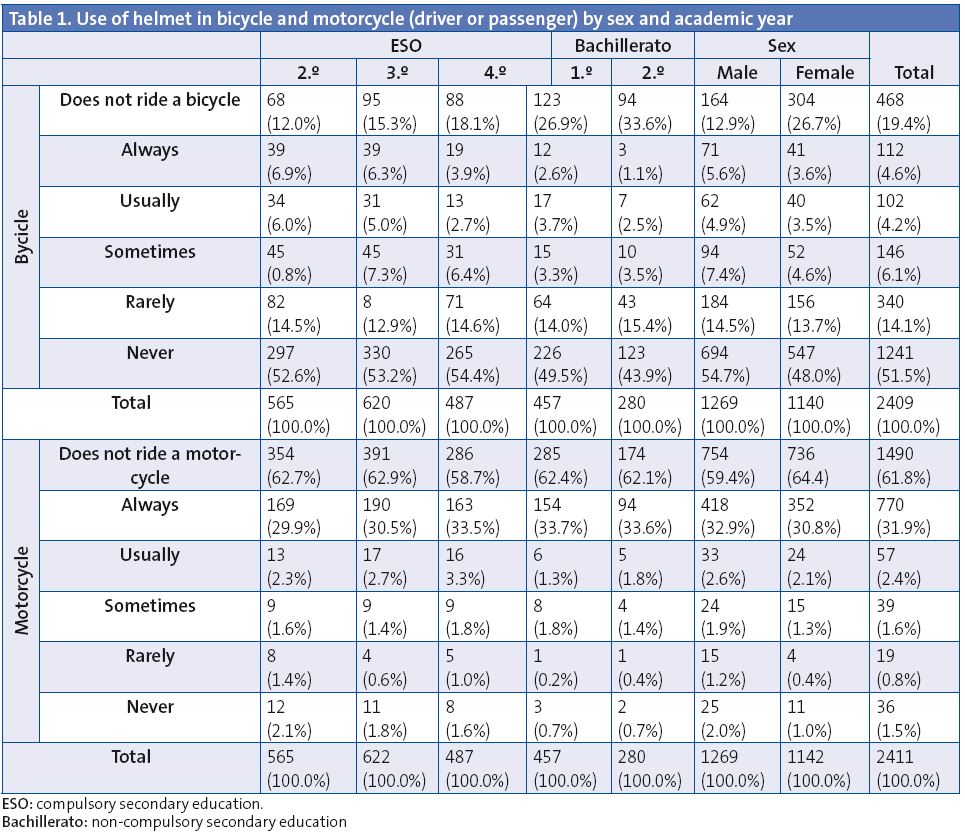
- Helmet use for bicycle and motorcycle riding: Table 1 describes the answers regarding the degree of helmet use for bicycle and motorcycle riding by sex and academic year.
- The low use of bicycle helmet was noteworthy: 81.5% of adolescents reported rarely or never using it. Helmet use for motorcycle riding was more widespread; still, 6% reported they never or rarely used it. We found statistically significant differences between sexes and academic years. There was a higher proportion of girls who did not use a helmet when riding a bicycle (p=0.009), while the frequency of boys who did not use a helmet for motorcycle riding was greater (p=0.01). The use of a helmet for bicycle riding was least frequent among 2nd year Bachillerato students (p<0.001).
Practice of aquatic sports and high-risk activities in water
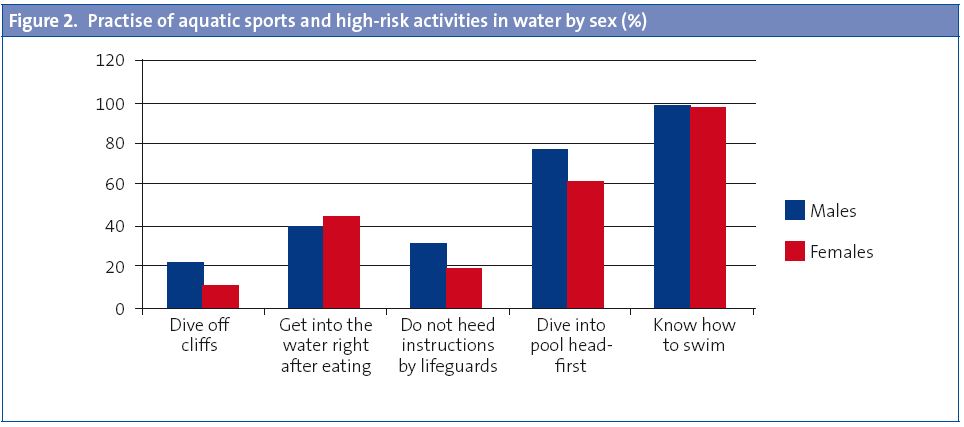
- Swimming:98.1% of the adolescents knew how to swim, in similar proportions for males (98.3%) and females (97.8%). We found no statistically significant differences between academic years.
- High-risk activities: broadly speaking, boys engaged more frequently in risky activities in the water, with statistically significant differences in almost every case. In the analysis by academic year, only the variable pertaining to getting into the water right after eating was statistically significant, which was also the only risk activity reported more frequently in girls.
- 69.2% usually dived into the pool head-first (76.2% of males and 61.5% of females) (p<0.001).
- 17.5% of the teenagers dived off cliffs sometimes (22.4% of boys and 12% of girls) (p<0.001).
- 41.5% reported going into the water right after eating (39.1% of boys and 44.3% of girls) (p=0.010). The students who did this most frequently were those in 2nd year of Bachillerato (45.5%) and 3rd year of the ESO (45%), while the ones who did it the least were in the 2nd year of the ESO (36.5%) (p=0.027).
- 25.6% of adolescents reported not heeding the indications of lifeguards when going into the sea (31.5% of boys and 19% of girls) (p<0.001).
Fig. 2 describes the practise of aquatic sports and risk activities by sex.
Factors associated to risk-taking behaviours in road traffic safety
Socio-demographic factors and risk-taking behaviours associated to not using a helmet when riding a bicycle or motorcycle are shown in Table 2. There is a notable association of these risk-taking behaviours as regards road safety and other risk behaviours such as low academic performance, alcohol, drug, or tobacco use, antisocial behaviours (stealing and school absenteeism), etc. There are also socio-demographic factors, such as age, sex, and socio-economic status.
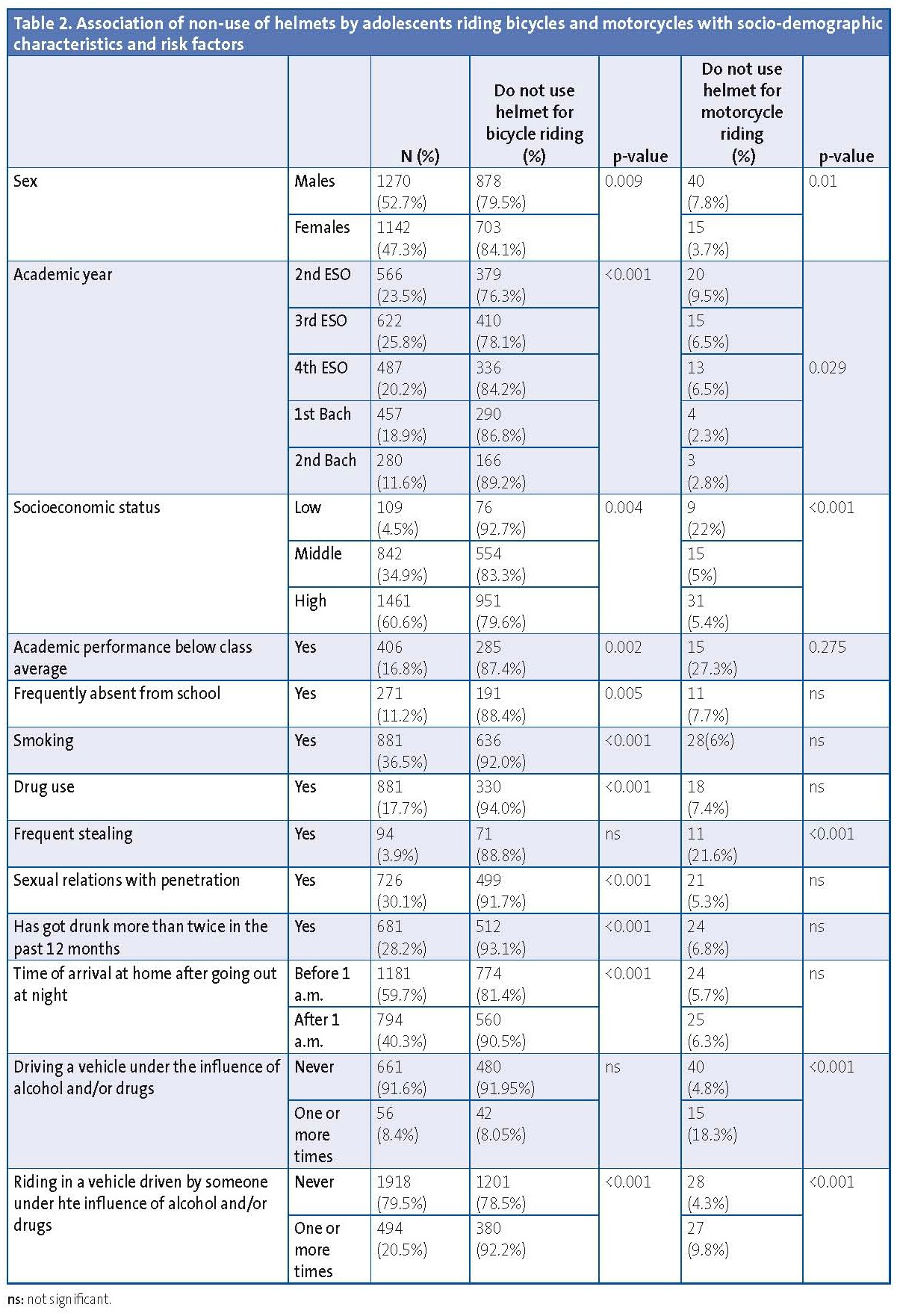
Another two aspects that stood out were the proportion of adolescents (20.4%) who reported having been occupants in vehicles driven by a person under the influence of alcohol and/or drugs, and the proportion who reported having driven a vehicle (motorcycle or car) under the influence of drugs or alcohol (8.4%).
DISCUSSION
Injuries are one of the leading causes of death in children across the world. They are also a significant source of morbidity and disability, with long-lasting and even life-long physical, sensory, or mental sequelae 2,6,11. Unintentional injuries or accidents represent nearly 90% of these cases, and they are the leading cause of death in persons aged 10 to 19 years.
According to the results of various international studies, the issue of injuries is particularly worrisome in Spain, as it is one of the developed countries with the highest rates of injury among the teenage population14,22. In Spain, accidents are the leading cause of death from 1 to 25 years of age, with incidence rates that range from 3.3/100 000 inhabitants/year in the 5-14 years age range, and 30.1/100 000 inhabitants/year in the 15-25 year age group10,11. Approximately 1% of accidents are fatal.
The results of our study show that 14% of adolescents report having had an injury requiring medical attention in the last year, a figure similar to the one recorded by the Surveillance System for Risk Factors associated to Non-Transmissible Diseases in the Juvenile Population (SIVFRENT-J) in youth 15-16 years old in 201020, and lower than the one reported in the last HBSC-2010 study on Spanish boys and girls ages 11 to 18 years (61.9%)14.
We ought to note the higher accident incidence rate in males in our study, in agreement with the data of other studies4,5,14,16,20.
Several theories have been proposed to account for the differences in accident incidence rates between sexes23. One of them is that boys engage in risk-taking behaviours more frequently, do more physical activity and sports, and tend to behave more impulsively than girls.
The most frequently reported causes of injury were traumatic accidents (sprains and bone fractures, 30%), many of which occurred while playing sports or as a result of falls, as is reported in other studies. They were the leading cause of non-fatal injuries4.
Traffic-related injuries are the leading cause of disability in children and adolescents worldwide, and they are the leading cause of death for the 10 to 19-year-old age group4.
The worldwide mortality rate for road traffic-related traumatic injuries increases with age, which reflects the evolution of the use of public roads as a function of age in minors, who go from being pedestrians and vehicle occupants, to being cyclists and motorcyclists, and eventually drivers.
In Spain, road traffic accidents are the leading cause of death between the ages of 15 and 35 years, as described in the last set of data analysed by the National Centre of Epidemiology (CNE) of the Instituto Carlos III of the Ministry of Health24. The progressive decrease in the road traffic mortality rates in recent years24,25 has made it drop to the third leading cause of death in boys and girls 5 to 14 years of age, and in women 25 to 34 years old, which means that the measures that have been implemented to prevent these deaths are in fact working.
The percentage distribution of the number of deaths according to road use type in the 15 to 17-year-old age group is, according to the 2011 data of the Dirección General de Tráfico (Directorate General of Traffic, DGT), 41% moped, 31% automobile, 10% pedestrians, 7% motorcycle, 7% bicycle, and 4% other circumstances26.
The scientific reviews that have been done show that child restraint systems, seat belt use, and the use of helmets in bicycles and motorcycles are efficacious in reducing road traffic accident morbidity and mortality rates. On the other hand, current research in other developed countries show that legislation results in increased helmet use, which in turn results in a lowered risk for facial and head injuries and death1,4,27-29,32.
Seat belt use has increased progressively in recent years to up to 88.6% of drivers in 2011, according to the data of the 2011 Road Safety Annual Report 25. Still, 22% of people killed in car collisions were not using the seat belt in interurban roads, and this percentage rose to nearly 41% in urban roads.
In our study, 93.9% of those surveyed reported using the seat belt regularly or always, results in accordance to those found in other studies on the adolescent population17,20; notwithstanding, the fact that the seat belt was not used by 6.1% means that we still need to promote its use in every age group.
Despite the overall decrease in mortality rates, the number of motorcycle accident deaths increased between 2003 and 2009, although we have observed a decreasing trend in the past two years. Still, the moped is the type of vehicle associated to the greatest number of deaths, severe injuries, and mild injuries in the 15 to 17 years age group25,26.
To better understand the high road-traffic injury incidence rate in the Spanish adolescent population, we need to keep in mind that Spain ranks high in the use of two-wheeled vehicles. As of December 2010, under Spanish legislation it is possible to obtain a moped driving permit starting at 15 years of age, a permit to drive motorcycles with engines up to 125cc from 16 years of age, and permits for more powerful motorcycles and automobiles from age 1830,31.
On the other hand, considering the statistical data on accident rates, some studies of the DGT point at the lower percentage of helmet use as one of the factors that account for the high mortality rate among young moped riders (14-17 years of age). According to data from 2011, 19% of the deceased moped riders did not use a helmet in interurban roads, and 16% did not use it in urban roads. When it came to motorcycles, 2% of those killed in interurban roads did not use a helmet, with this percentage rising to 15% for urban roads26.
Using a helmet decreases the risk and severity of injuries by approximately 72% and decreases the risk of death by as much as 39%, depending on the motorcycle speed4.
In our study, 10.1% of adolescents reported never or rarely using a helmet when riding a motorcycle, data that are comparable to those of other studies17,26,33 and with rates lower than those found in the 2011 study of 4th year students of the ESO in the Madrid Region (35.2%)20.
There has been an increase in the use of bicycles in recent years, both in European countries and in the United States, with bicycles being used for various activities such as recreation, sports, transportation, or work. They are mainly used in roads, which is where accidents happen most frequently. However, this practise is not risk-free, as it is the cause of many accidents that may result in severe injuries with significant sequelae or even death.
In its manual on bicycle and motorcycle helmets, the WHO notes that globally about two thirds of hospital admissions due to severe injuries of cyclists and three quarters of deaths of injured cyclists are from head injuries. Nearly 25% of the severe brain injuries in children younger than 15 years are due to bicycle accidents4.
In addition to head injuries, musculoskeletal and internal organ injuries are also important causes of bicycle-related deaths.
Although most accidents take place in an urban environment, fatalities occur mainly in interurban roads, with males accounting for over 90% of deceased cyclists.
In our country, the number of cyclists killed between 2001 and 2010 dropped by 33%, although it increased by 20% between 2009 and 2010. Still, there has been a marked increase in the number of injured cyclists in the past ten years26,29.
According to the international review done by the Cochrane group, head trauma accounts for about three quarters of all collision-related bicyclist deaths, and helmet use results in a decrease of 63% to 88% of severe head injuries (scalp and skull) and brain injuries for all age groups. Furthermore, helmets provide the same level of protection in case of collision with motor vehicles as in accidents due to other causes1,4,27.
This notwithstanding, most bicycle users, including children, do not use a helmet or use it inappropriately.
In our study, a very high proportion of adolescents reported never or seldom using helmets (81.3%), data which differ little from the 2005 study done in Guipuzcoa33 and also similar to those in the study done in the Madrid Region in 200920. We ought to note that our study showed a greater number of females who did not use a helmet when riding a bicycle, while males tended to use helmets less frequently for motorcycle riding, factors that need to be taken into account in the design of preventive road safety measures.
The practise of aquatic sports was another frequent cause of accidents, with drowning being one of the leading causes of death in children and adolescents.
The world’s rate of death by drowning in childhood is of 7.2 per 100 000 people, although it varies considerably from region to region. Drowning is the cause of 28% of deaths due to unintentional injuries in children. The highest rates of death by drowning correspond to children younger than five years, with the maximum frequency falling in the 1-4 year old age group. There is another small peak in late adolescence4.
Adolescent drowning usually happens in natural bodies of water while they practise recreational activities related to swimming, sailing, and others. Adolescents and pre-adolescents usually know how to swim or know the basics, but most of them think that they swim better than they actually do, and thus do not make an accurate assessment of currents, the depth of the water, and their own physical state.
Most accidents take place in unsupervised places, such as rivers, dams, and ponds, and result from diving in areas that are shallow or have floating or underwater objects, hitting the bottom of a pool, diving from a springboard, or swimming under the influence of alcohol or other drugs.
Risk-taking behaviours constitute one of the leading causes of accidental drowning, especially among adolescents. Alcohol use has been associated to a proportion of adolescent and adult deaths in the course of water recreation that ranges from 25 to 50%. Alcohol influences balance, coordination, and judgment, and sun and heat exposure heighten its effects, increasing the risk of drowning if difficulties arise4.
Usually, teenagers who end up drowning are with one or more friends of similar age who do not realise they are in trouble or are unable to rescue them. Adults are usually absent and it is possible that adolescents pressure their peers to engage in risk-taking behaviours, such as alcohol consumption. The risk of drowning increases as blood alcohol levels rise.
Worldwide data show that fatal drowning is more frequent in boys than in girls. The biggest differences in drowning death rates between sexes occur in the 15 to 19 years age group, where it is 2.4 times higher in males than in females4. Boys are at a higher risk for drowning than girls because they are more exposed to environments where there is water and engage in risk behaviours more frequently, especially in the case of adolescents.
According to the CNE (National Centre of Epidemiology) of the Instituto Carlos III, in 2010 the drowning death rate for both sexes in Spain was of 0.67/100 000 inhabitants/year and in the 15-24 year age group the rate was of 1.22/100 000 inhabitants/year for males and 0.09/100 000 inhabitants/year for females24.
It is important to note that in our study, though most adolescents reported knowing how to swim (98.1%), a great proportion engaged in high-risk activities in the water, such as diving head-first into the pool, cliff diving, and disregarding the directions of lifeguards, all of them found more frequently in boys. The girls, however, went into the water right after eating more frequently.
Different studies have reported that injuries are associated to other risk behaviours in adolescence, such as substance use, school absenteeism, and frequent participation in physical activity14. Understanding the factors that contribute to the occurrence of injuries in young people is key to developing interventions to control and prevent severe injuries and death.
Alcohol appeared as a factor in one third of the fatal accidents in which adolescents were involved, impairing the ability to drive, and usually with blood alcohol concentrations lower than those with similar effects in adults. Furthermore, other factors, such as a mistake by the driver, the less frequent use of safety belts, being distracted (use of mobile phones or other electronic devices), fatigue, and the presence of other adolescent occupants, increase the severity of the crashes involving adolescent drivers. These behaviours are often exacerbated by peer pressure, especially when it comes to boys, so the probability of traffic-related injuries is much higher in this group, which also shows greater differences between age groups4.
Driving under the influence of psychoactive substances is a frequent behaviour in Spain, found in up to 17% of Spanish drivers. In addition to alcohol (7%), nearly 11% of drivers drive after having consumed some substance (illicit drugs) which may impair the ability to drive safely, with cannabis and cocaine being the two most commonly found drugs. These data come from the European project DRUID (Driving Under Influence of alcohol and Drugs), which concluded in 201134.
In our study, 8.4% of adolescents who reported driving a vehicle (car or motorcycle) stated that they have done it under the influence of alcohol and/or drugs, and 20.4% has been an occupant in a vehicle (car or motorcycle) driven by another person who was under the influence of alcohol and/or drugs, proportions that were similar to those found in other surveys18. Males engaged more frequently in both risk behaviours, a fact that has also been observed in other studies4.
We found additional factors associated to a higher accident risk, such as having low socio-economic status, parents having a lower level of education, adolescents with poor academic performance, school absenteeism, antisocial behaviours such as frequent stealing, and the consumption of alcohol and other addictive substances.
Recommendations for the prevention of injuries and traffic accidents
Injuries can be prevented or controlled. The specific measures for road safety targeting adolescents implemented in other countries have led to a significant decrease in the morbidity and mortality rates associated to adolescent motor vehicle driving. Among these measures are:
- Introducing graduated driver licensing systems with distinct learning stages that set restrictions on unsupervised driving, driving at night, and driving with young passengers.
- Setting speed limits of 80 km/hour in highways.
- Lowering blood alcohol concentration limits for drivers younger than 21 years to 0 0-0.02 g/dl.
- Restricting the use of mobile phones, including those used with hands-free devices.
- Raising the legal minimum drinking age to 21 years.
- Implementing legislation making the use of approved helmets mandatory for bicycle, moped, and motorcycle riders, accompanied by public awareness campaigns.
- Education and awareness campaigns explaining the protection offered by safety gear in motorcycle riders (quality helmets, back protectors, boots, and elbow pads) and promoting their daily use.
Preventive strategies for water recreation
They must be adjusted to circumstances and location, and use multifaceted approaches whenever possible:
- Swimming courses and teaching the necessary skills to survive in the water are a key component in prevention programmes.
- Improving the following cognitive skills associated to aquatic sports: ability to identify hazards, recognition of personal limits, including knowledge of one’s swimming skills; ability to resist peer pressure to participate in activities for which one lacks the necessary skills.
- Discourage adolescents from consuming alcohol when practicing water recreational activities and restrict any kind of advertising that may induce alcohol consumption in boats, as well as the sale of alcohol in places where water recreation takes place.
- Provide children and adolescents with swimming sites that are both safe and attractive. Post properly trained and equipped lifeguards in places where adolescents tend to congregate and at the times they tend to do so. In rural areas, make safe swimming areas available to children and adolescents to prevent them from gathering in dangerous places such as irrigation channels, quarries, and other areas with natural bodies of water.
Conclusions
We identified risk factors for road safety in the adolescent population of our province, such as not using safety belts, not using a helmet when riding a motorcycle, a high percentage of minors who did not use helmets when riding bicycles, alcohol or substance use and driving, and risk factors in the practise of aquatic sports.
Legislation, advertising campaigns, and educational programmes in schools and the healthcare field are needed to decrease the risk of death and injury due to accidents in adolescents.
FUNDING
This work has been funding by the Spanish Association of Primary Care Paediatrics (AEPap)
CONFLICT OF INTERESTS/span>
The authors declare having no conflict of interests in relation to the preparation and publication of this paper.
ABBREVIATIONS: CNE: National Centre of Epidemiology • DGT: Directorate General of Traffic • ESO: Compulsory Secondary Education • WHO: World Health Organization.
BIBLIOGRAPHY
- Esparza Olcina MJ. Prevención de lesiones infantiles por accidente de tráfico. Asociación Española de Pediatría de Atención Primaria: Recomendaciones PrevInfad/PAPPS [on line] [updated in June 2011; consulted on 10/08/2013]. Available in www.aepap.org/previnfad/accidentes_trafico.htm
- Sociedad Española de Medicina de Familia y Comunitaria (semFYC). Estudio sobre accidentes infantiles atendidos en los Centros de Salud. Sociedad Española de Medicina de Familia y Comunitaria y Fundación MAPFRE. 2010 [on line] [consulted on 10/10/2013]. Available in www.fundacionmapfre.org/fundacion/es_es/prevencion-salud-medio-ambiente/publicaciones-y-estudios/estudios/prevencion/accidentes-infantiles.jsp
- World Health Organization Regional Office for Europe. Matching the lowest injury mortality rate could save half a million lives per year in Europe. WHO/Europe Fact sheet 26 June 2006 [on line] [consulted on 10/10/2013]. Available in www.euro.who.int/en/what-we-do/health-topics/disease-prevention/violence-and-injuries/facts-and-figures/matching-the-lowest-injury-mortality-rate-could-save-half-a-million-lives-per-year-in-europe2
- Peden M, Oyegbite K, Ozanne-Smith J, Hyder AA, Branche C, Rahman A, et al. World report on child injury prevention. World Health Organization. 2008 [on line] [consulted on 10/10/2013]. Available in http://whqlibdoc.who.int/publications/2008/9789241563574_eng.pdf
- Da Cuña Vicente R.Accidentes en niños asistidos por el Servicio de emergencias sanitarias de Castilla y León. Epidemiología y análisis cronobiológico de 10.933 casos. Tesis doctoral. Valladolid; 2012.
- Hanfling MJ, Gill AC. Overview of Pediatric injury prevention: epidemiology; history; application. UpTDate. 30, Abril, 2008 [on line]. Available in www.uptodate.com
- Fraga A, Fraga G, Stanley C, Constantini T, Coimbra R. Children at danger: injury fatalities among children in San Diego County. Eur J Epidemiol. 2010;25(3):211-17.
- World Health Organization. Child and adolescent injury prevention: a WHO plan of action 2006-2015. Geneva: WHO 2006 [on line] [consulted on 10/10/2013]. Available in http://whqlibdoc.who.int/publications/2006/9241593385_eng.pdf
- Sethi D, Racioppi F, Baumgarten I, Vida P. Injuries and violence in Europe. Why they matter and what can be done. Copenhagen, Denmark: World Health Organization Regional Office for Europe; 2006 [on line] [consulted on 10/10/2013]. Available inwww.euro.who.int/__data/assets/pdf_file/0005/98762/E88037.pdf
- Rivara FP, Grossman D. Control de las lesiones. En: Nelson (ed.). Tratado de Pediatría, 18.ª ed. Barcelona: Elsevier; 2009. p. 366-74.
- Pou J, Luaces C. Accidentes infantiles. Intoxicaciones. En: Cruz M (ed.). Manual de Pediatría, 2.ª ed. Madrid: Ergón; 2008. p. 1095-101.
- Brooks F, Van der Sluijs W, Klemera E, Morgan A, Magnusson J, Gabhainn SC, et al. Young People’s Health in Great Britain and Ireland. Findings from the Health Behaviour in School-Aged Children Study 2006. HBSC International Coordinating Centre. Child and Adolescent Health Research Unit (CAHRU) The Moray House School of Education. The University of Edinburgh. St Leonard's Land. Holyrood Road. Edinburgh EH8 8AQ. Scotland, UK [on line] [consulted on 10/10/2013]. Available in www.nuigalway.ie/hbsc/documents/2009_young_peoples_health_in_gb__ireland.pdf
- University of California. Adolescent Questionnaire. California Health Interview Survey. CHIS 2009 [on line] [consulted on 10/10/2013]. Available in www.chis.ucla.edu
- World Health Organization Regional Office for Europe. Health Behaviour in School-aged Children (HBSC) study: international report from the 2009/2010 survey. Copenhagen, WHO Regional Office for Europe, 2012 (Health Policy for Children and Adolescents, No. 6) [on line] [consulted on 10/10/2013]. Available in www.euro.who.int/__data/assets/pdf_file/0003/163857/Social-determinants-of-health-and-well-being-among-young-people.pdf
- Ministerio de Sanidad, Política Social e Igualdad. Encuesta nacional de salud de España 2006. Ministerio de Sanidad, Política Social e Igualdad en Portal estadístico del SNS [on line] [consulted on 10/10/2013]. Available in www.msssi.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2006.htm
- Moreno-Rodríguez C, Muñoz Tinoco V, Pérez Moreno PJ, Sánchez Queija I, Granado Alcon MC, Ramos Valverde P, et al. Desarrollo adolescente y salud. Resultados del estudio HBSC 2006 con chicos y chicas españoles de 11-17 años. Madrid: Ministerio de Sanidad, Política Social e Igualdad 2008 [on line] [consulted on 10/10/2013]. Available in http://grupo.us.es/estudiohbsc/index.php/es/publicaciones/libros/libros-nacionales
- Nebot M, Pérez A, García-Continente X, Ariza C, Espelt A, Pasarín M, et al. Informe FRESC 2008. Resultats principals. Barcelona: Agència de Salut Pública de Barcelona, 2010 [on line] [consulted on 10/10/2013]. Available in www.aspb.cat/quefem/docs/Informe_FRESC_resultats2008.pdf
- Ministerio de Sanidad y Consumo. Secretaría General de Sanidad. Delegación del Gobierno para el Plan Nacional sobre Drogas. Encuesta Estatal sobre Consumo de Drogas entre Estudiantes de Enseñanza Secundaria de 14 a 18 años (ESTUDES), 2006-2007. Ministerio de Sanidad, Política Social e Igualdad en Plan Nacional sobre Drogas [on line] [consulted on 10/10/2013]. Available in www.pnsd.msc.es/Categoria2/observa/pdf/Estudes2006-2007.pdf
- Schiaffino A, Moncada A, Martín A. Estudi EMCSAT 2008. Conductes de salut de la població adolescent de Terrassa, 1993-2008. Ajuntament de Terrassa: Servei de Salut Comunitària, Desembre 2009.
- Servicio epidemiología Comunidad de Madrid. Hábitos de salud en la población juvenil de la Comunidad de Madrid, 2010. Resultados del sistema de vigilancia de factores de riesgo asociados a enfermedades no transmisibles en población juvenil (SIVFRENT-J), 2010. Boletín Epidemiológico de la Comunidad de Madrid. 2011;17(4):3-38.
- Boyce W, Torsheim T, Currie C, Zambon A. The Family Affluence Scale as a measure of national wealth: Validation of an adolescent self-report measure. Soc Indic Res. 2006;78:473-87.
- World Health Organization Regional Office for Europe. European Detailed Mortality Database. Copenhague: WHO Regional Office for Europe [on line] [updated in September 2013; consulted on 10/10/2013]. Available in http://data.euro.who.int/dmdb/
- Graine MA. Sex differences, effects of sex-stereotype conformity, age and internalization on risk-taking among pedestrian adolescents. Saf Sci. 2009;47:1277-83.
- Instituto Carlos III. Estadísticas de mortalidad por causas en España 2003-2011. Instituto Carlos III: Servicios Científico-Técnicos: Epidemiología: Mortalidad [on line] [consulted on 10/08/2013]. Available in www.isciii.es/ISCIII/es/contenidos/fd-servicios-cientifico-tecnicos/fd-vigilancias-alertas/mortalidad-cne.shtml
- International Traffic Safety Data and Analysis Group. Road Safety Annual Report 2011. IRTAD Annual Report OECD/ITF 2012 [on line] [consulted on 10/08/2013]. Available in www.dgt.es/was6/portal/contenidos/documentos/seguridad_vial/estudios_informes/11IrtadReport.pdf
- Dirección General de Tráfico. Las principales cifras de la siniestralidad vial. España 2011. Dirección General de Tráfico: Seguridad vial: Estadística e indicadores [on line] [consulted on 10/08/2013]. Available in www.dgt.es/portal/es/seguridad_vial/estadistica/publicaciones/princip_cifras_siniestral/
- Thompson DC, Rivara F, Thompson R. Helmets for preventing head and facial injuries in bicyclists. Cochrane Database Sys Rev. 2000;(2):CD001855.
- Coleman P, Munro J, Nicholl J, Harper R, Kent G, Wild D. The effectiveness of interventions to prevent accidental injury to young persons aged 15-24 years: a review of the evidence. Sheffield: University of Sheffield, School of Health and Related Research, Medical Care Research Unit. 1996 [on line] [consulted on 10/08/2013]. Available in www.crd.york.ac.uk/CRDWeb/ShowRecord.asp?View=Full&ID=11996008507#.UkHu6DbIaCo
- Monclús J. Instituto de seguridad vial-Fundación MAPRE. Casco de ciclistas. Trabajo realizado con la colaboración y supervisión de la Fundación MAPFRE; 2013.
- Suelves JM. Lesiones no intencionadas en la infancia y la adolescencia: rompiendo el tópico de la mala suerte. Barcelona: Observatorio de Salud de la Infancia y la Adolescencia del Hospital Sant Joan de Déu; 2009 [on line] [consulted on 10/08/2013]. Available in http://faros.hsjdbcn.org/adjuntos/285.1-Informe_Faros_2_Cast.pdf
- Seguí-Gómez M, López-Váldés FJ. Recognizing the importance of injury in other policy fórums: The case of motorcycle licensing policy in Spain.Inj Prev. 2007;13(6):429-30.
- Macpherson A, Spinks A. Bicycle helmet legislation for the uptake of helmet use and prevention of head injuries. Cochrane Database Syst Rev 2007;(2):CD005401.
- Gorrotxategi Gorrotxategi P, Gonález Conde L, Ibarguren Aguirre O. Utilización del casco en bicicleta y motocicleta. An Pediatr (Barc). 2005;62:338-9.
- Hargutt V, Krüger HP, Knoche A. Driving under the influence of alcohol, illicit drugs and medicines. Risk estimations from different methodological approaches. DRUID. Project co-funded by the European Commission with the Sixth Framework program. DELIVERABLE 1.3.1 (2011).