
Vol. 26 - Num. 101
Original Papers
Growth and pubertal development in girls adopted from Russia: 12-year follow-up
aPediatra. Centro de Pediatría y Adopción Internacional. Zaragoza. España.
Correspondence: G Oliván. E-mail: golivang@aragon.es
Reference of this article: Oliván Gonzalvo G. Growth and pubertal development in girls adopted from Russia: 12-year follow-up . Rev Pediatr Aten Primaria. 2024;26:45-51. https://doi.org/10.60147/43e0f65f
Published in Internet: 22-01-2024 - Visits: 16263
Abstract
Introduction: the objectives were to provide longitudinal data on growth and determine the age of thelarche and menarche in girls adopted from Russia.
Material and methods: prospective cohort study in 24 girls from Russia adopted in Spain in the 2002-2010 period, who were followed up for 12 years. The history of adverse childhood experiences was collected by reviewing pre-adoption medical records. We recorded standardised measurements of weight, height and head circumference and the age at thelarche and menarche. The mean values were compared with reference standards.
Results: Salient history: preterm birth (33.3%), low birth weight (41.7%), prenatal alcohol exposure (45.8%), abuse and neglect (54.2%). Initial evaluation: mean age, 3 years (standard deviation [SD] 1.6) years; weight z-score (z), −1.35; height z, −2.42; head circumference z −1.77. One year after adoption, there was significant catch-up growth in weight (z +0.68), height (z +0.98), and head circumference (z +0.76). Temporal trends in growth: no weight delay from age 7 years; height continued to recover until age 10 (z −0.40) and remained stable until age 15 (z −0.46); the delay was greater compared to weight at every timepoint. The mean age at onset of thelarche was 9.9 years (SD 0.8) with a height of 135.4 cm (z −0.43). The mean age at menarche was 11.9 years (SD 0.7) years, with a height of 147.6 cm (z −0.44).
Conclusions: the pattern of growth and development was characterized by severe delay in linear growth and a moderate delay in weight and head circumference at the time of adoption, rapid, significant and prolonged catch-up growth, acceleration of pubertal development with early thelarche and menarche and an incomplete recovery of linear growth.
Keywords
● Adoption ● Female ● Growth ● Menarche ● Russia ● ThelarcheINTRODUCTION
Growth is determined by endogenous factors (genetic, epigenetic, metabolic and neurohormonal) that interact throughout the process with a multitude of exogenous factors (diet, nutrition, hygiene, medical care, chronic diseases, emotional environment, psychosocial environment, stress, environmental factors, etc), so that, for the genetic potential not to be affected, all of these factors must interact appropriately and be correctly balanced.1
Internationally adopted children frequently have risk factors that can affect growth, chief among which are adverse prenatal exposures (drugs, alcohol, etc), intrauterine growth restriction, prematurity, emotional deprivation, abuse and neglect, stress, undernutrition and micronutrient deficiencies. In addition, stunted growth may have permanent effects, even if other aspects (nutrition, health, psychosocial environment, etc) improve later.2,3
Russia has been one of the main sending countries of foreign children adopted by Spanish families.4 There are few prospective studies on the growth in children adopted from Russia, and they usually have a short duration of followup, assessing growth delay on arrival to the receiving country and catch-up growth following adoption.5-10 After an exhaustive literature search, we did not find any prospective studies with a long-term followup.
The aim of this case series is to provide data on the longitudinal trends in growth and the age at onset of thelarche (Tanner stage II of puberty) and the age of menarche in girls adopted from Russia.
MATERIAL AND METHODS
We conducted a longitudinal, epidemiological, observational and descriptive study in a cohort of 24 girls adopted from Russia in Spain in the 2002-2010 period who were followed up for monitoring of growth and pubertal development in a specialised reference centre.
The initial cohort included 49 girls. Of these total, 19 girls were lost to followup for different reasons before menarche, and 6 girls were excluded due to diagnosis of diseases that could affect growth (2 with coeliac disease, 2 with foetal alcohol syndrome, 1 with hypothyroidism and 1 with growth hormone deficiency).
All the girls had been institutionalised in orphanages before adoption. We reviewed the pre-adoption medical records to collect data on the gestational age at birth, birth weight, prenatal exposure to alcohol and reasons for institutionalization.
The height, weight and head circumference (HC) were measured and recorded following the standardised protocol in the initial evaluation on arrival and in follow-up visits conducted every 6 months and annually for 12 years, always by the same health care provider. Weight was measured with a Seca 708 stand-up scale and stadiometer (max 200 kg, accurate to 0.1 kg), a GC-1104 baby scale (max 20 kg; accurate to 10 g), Seca infantometer (max 100 cm) for children aged less than 3 years and a flexible non-elastic tape measure (in mm). The anthropometric measurements were entered in an Excel spreadsheet to calculate the mean, standard deviation (SD) and body mass index (BMI = kg/m2).
Families were instructed on how to identify thelarche and menarche with the purpose of carrying out an additional anthropometric evaluation at those time points. We entered the ages at thelarche and menarche in an Excel spreadsheet also used to calculate the corresponding mean and SD values.
Patients underwent the procedures in the study protocol after obtaining the informed consent of their legal guardians. The data were recorded and used in adherence to Organic Law 3/2018 on the protection of personal data and the upholding of digital rights currently in force in Spain.
We used the WHO Anthro 2.0 (0-5 years) and WHO AnthroPlus (5-19 years) software11 to compare the mean anthropometric values obtained in our study with the child growth reference standards developed by the World Health Organization (WHO), calculating the corresponding z-scores and percentiles for age and sex. These software applications do not allow calculation of the z score and percentile of the head circumference from age 5 years or of the weight from age 10 years. According to the WHO standards, z-scores of less than −2 correspond to severe delay, while z-scores between −1 and −2 correspond to moderate delay and abnormally low z-scores greater −1 to mild delay. We defined significant catch-up as an increase in the z-score of a given parameter greater than +0.5 in a one-year period.12
RESULTS
The relevant history in the cohort of girls adopted from Russia was: preterm birth (33.3%), low birth weight (41.7%), documented prenatal exposure to alcohol (45.8%), abuse/neglect (54.2%) and abandonment at birth (45.8%).
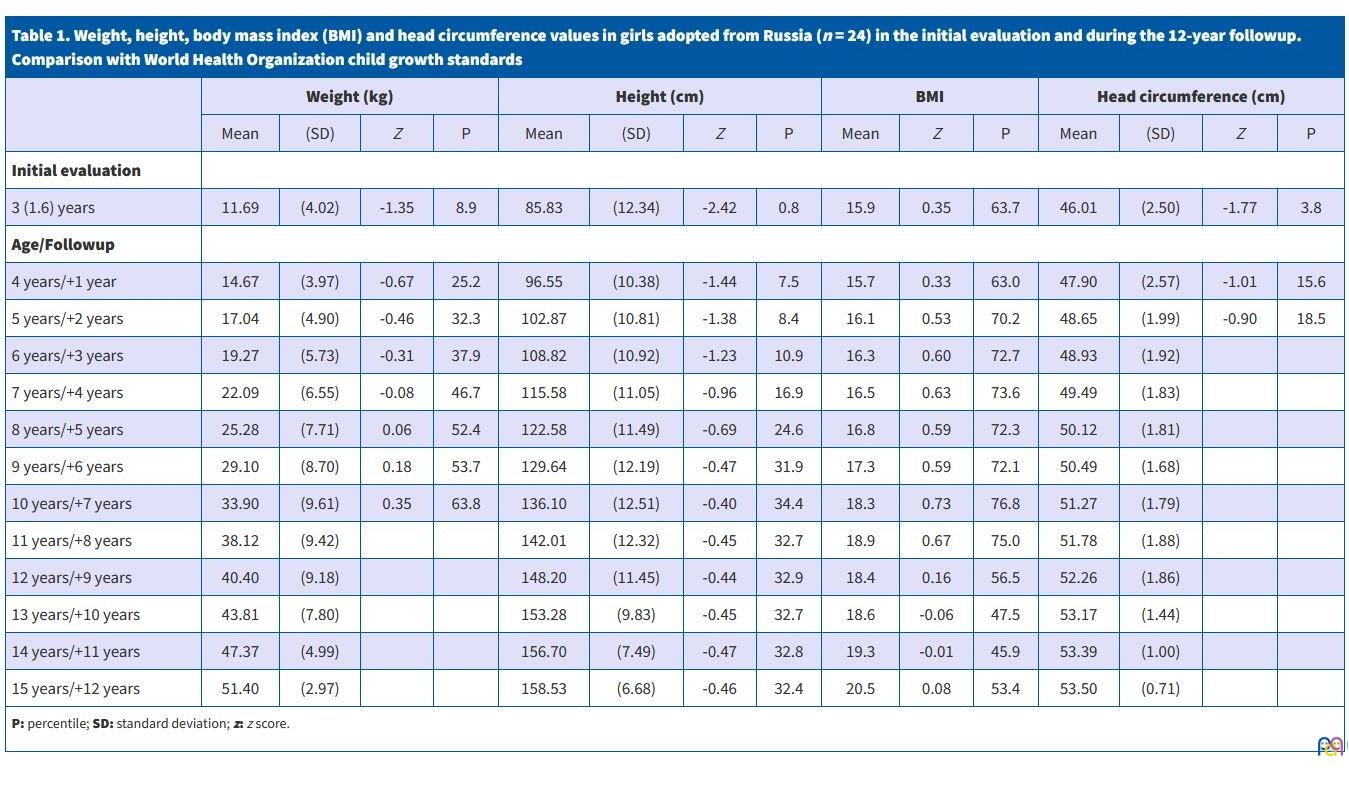
Table 1 presents the anthropometric values obtained in the initial evaluation after adoption and in the annual follow-up visits and their comparison with the WHO child growth standards. Figure 1 shows the temporal trends in the height and BMI z scores relative to the WHO child growth standards.
| Table 1. Weight, height, body mass index (BMI) and head circumference values in girls adopted from Russia (n = 24) in the initial evaluation and during the 12-year followup. Comparison with World Health Organization child growth standards | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Weight (kg) | Height (cm) | BMI | Head circumference (cm) | ||||||||||||
| Mean | (SD) | Z | P | Mean | (SD) | Z | P | Mean | Z | P | Mean | (SD) | Z | P | |
| Initial evaluation | |||||||||||||||
| 3 (1.6) years | 11.69 | (4.02) | -1.35 | 8.9 | 85.83 | (12.34) | -2.42 | 0.8 | 15.9 | 0.35 | 63.7 | 46.01 | (2.50) | -1.77 | 3.8 |
| Age/Followup | |||||||||||||||
| 4 years/+1 year | 14.67 | (3.97) | -0.67 | 25.2 | 96.55 | (10.38) | -1.44 | 7.5 | 15.7 | 0.33 | 63.0 | 47.90 | (2.57) | -1.01 | 15.6 |
| 5 years/+2 years | 17.04 | (4.90) | -0.46 | 32.3 | 102.87 | (10.81) | -1.38 | 8.4 | 16.1 | 0.53 | 70.2 | 48.65 | (1.99) | -0.90 | 18.5 |
| 6 years/+3 years | 19.27 | (5.73) | -0.31 | 37.9 | 108.82 | (10.92) | -1.23 | 10.9 | 16.3 | 0.60 | 72.7 | 48.93 | (1.92) | ||
| 7 years/+4 years | 22.09 | (6.55) | -0.08 | 46.7 | 115.58 | (11.05) | -0.96 | 16.9 | 16.5 | 0.63 | 73.6 | 49.49 | (1.83) | ||
| 8 years/+5 years | 25.28 | (7.71) | 0.06 | 52.4 | 122.58 | (11.49) | -0.69 | 24.6 | 16.8 | 0.59 | 72.3 | 50.12 | (1.81) | ||
| 9 years/+6 years | 29.10 | (8.70) | 0.18 | 53.7 | 129.64 | (12.19) | -0.47 | 31.9 | 17.3 | 0.59 | 72.1 | 50.49 | (1.68) | ||
| 10 years/+7 years | 33.90 | (9.61) | 0.35 | 63.8 | 136.10 | (12.51) | -0.40 | 34.4 | 18.3 | 0.73 | 76.8 | 51.27 | (1.79) | ||
| 11 years/+8 years | 38.12 | (9.42) | 142.01 | (12.32) | -0.45 | 32.7 | 18.9 | 0.67 | 75.0 | 51.78 | (1.88) | ||||
| 12 years/+9 years | 40.40 | (9.18) | 148.20 | (11.45) | -0.44 | 32.9 | 18.4 | 0.16 | 56.5 | 52.26 | (1.86) | ||||
| 13 years/+10 years | 43.81 | (7.80) | 153.28 | (9.83) | -0.45 | 32.7 | 18.6 | -0.06 | 47.5 | 53.17 | (1.44) | ||||
| 14 years/+11 years | 47.37 | (4.99) | 156.70 | (7.49) | -0.47 | 32.8 | 19.3 | -0.01 | 45.9 | 53.39 | (1.00) | ||||
| 15 years/+12 years | 51.40 | (2.97) | 158.53 | (6.68) | -0.46 | 32.4 | 20.5 | 0.08 | 53.4 | 53.50 | (0.71) | ||||
|
P: percentile; SD: standard deviation; z: z score. |
|||||||||||||||
| Figure 1. Height and body mass index (BMI) z scores in girls adopted from Russia (n = 24) during the 12-year followup. Comparison with World Health Organization child growth standards |
|---|
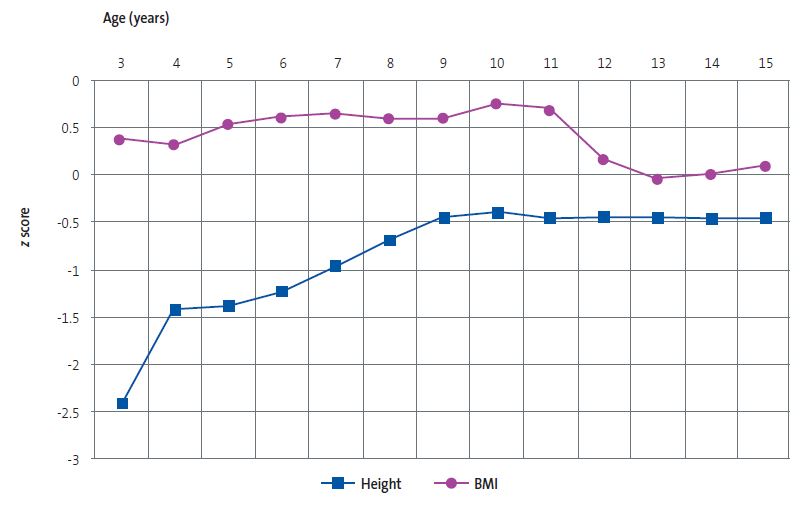 |
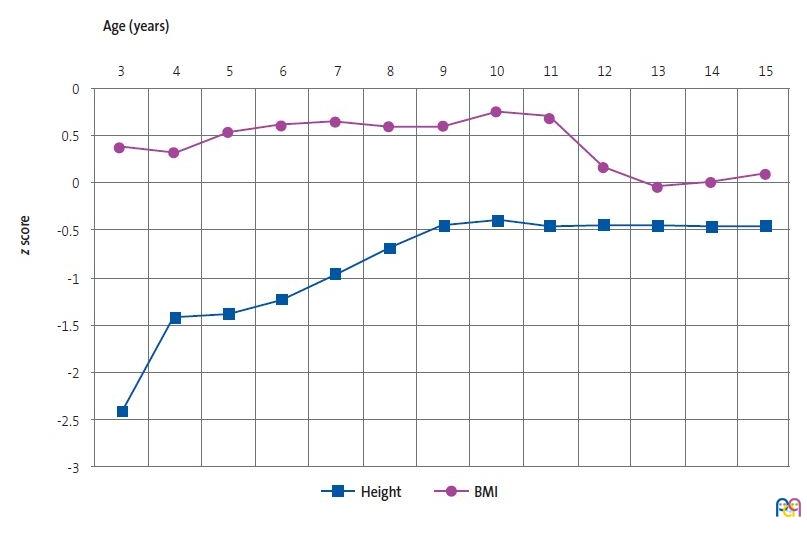
Weight: in the initial evaluation, 75% of the cohort exhibited moderate delay and the rest severe delay; one year after adoption, there had been significant catch-up growth (z increase +0.68); during the followup, mild delay persisted through age 7 years, after which there were no more delays in weight gain. Height: in the initial evaluation 58.3% of the cohort exhibited severe delay and the rest moderate delay; one year after adoption, there had been significant catch-up growth (z increase +0.98); during the followup, the catch-up growth persisted through age 10 years, and moderate linear growth delay persisted through age 6 years; from age 10 to 15 years, linear growth remained stable, with persistent mild delay. BMI: throughout the followup, the delay in linear growth was greater compared to the delay in weight. Head circumference: in the initial evaluation, 66.7% of the cohort exhibited moderate delay and the rest severe delay; one year after adoption, there had been significant catch-up growth (z increase +0.76); at age 5 years, there was still a mild delay.
The mean age at thelarche was 9.9 years (SD 0.8). In the corresponding follow-up visit, the mean weight was 33.4 kg [z 0.33, 62.8th percentile], the mean height 135.4 cm [z -0.43, 33.4th percentile] and the mean BMI was 18.2 [z 0.72, 76.5th percentile]. The mean age at menarche 11.9 years (SD 0.7). In the corresponding visit, the mean weight was 40.2 kg, the mean height 147.6 cm [z −0.44, 32.8th percentile] and the mean BMI was 18.5 [z 0.22, 58.7th percentile]. The mean peak height velocity between thelarche and menarche was 12.2 cm, and the mean additional linear growth from menarche through age 15 years was 10.9 cm. None of the girls showed signs of pubertal development before age 7 years. In 2 girls, thelarche occurred between ages 7 and 8 years. One girl experienced menarche between ages 9 and 10 years.
DISCUSSION
Longitudinal measurements of weight, height and head circumference are a simple method for growth assessment and a useful indicator of child development and health.11,12 Russia is a vast country in which the genetic growth potential varies between geographical regions and socioeconomic levels. Martinchik et al13 compared mean values of weight, height and BMI in the paediatric population of Russia applying the WHO child growth standards. The analysis of the z scores of anthropometric measurements showed that the largest differences corresponded to mean high positive BMI z values in children aged 0 to 6 years. The authors concluded that the WHO child growth standards should be used to assess growth and nutritional status in Russian children.
Growth stunting is a common finding in children adopted from Russia. Studies suggest this could be attributed to factors such as undernutrition, stress and psychosocial deprivation prior to adoption.4-10 The drastic change that takes place after adoption generally results in significant catch-up growth, 5-7,9,10 but this can also accelerate pubertal development.14,15 The pathophysiological mechanisms underlying this association are unclear and probably involve a variety of endogenous and exogenous factors.3,16
Meta-analyses and regression studies in children adopted from Russia have determined that low birth weight, prenatal alcohol exposure, more severe undernutrition at the time of adoption and late adoption are independent predictors of a lower height z score in the initial evaluation after adoption and that early adoption, a greater initial growth delay and a larger energy intake after adoption are associated with better and more complete catch-up growth.5,7-9
Observational studies in internationally adopted girls have shown that late adoption, a greater degree of undernutrition at the time of adoption and rapid catch-up growth are associated with early onset of puberty and earlier menarche.3,14-17
In the analysed cohort of girls adopted from Russia, the prevalence of preterm birth, low birth weight and undernutrition in the initial evaluation were 8, 7 and 9 times greater, respectively, compared to the general paediatric population of Russia.18 The documented prevalence of prenatal alcohol exposure was higher compared to the prevalence reported in institutionalised Russian children19 and the mean age at adoption was twice greater compared to other studies of children adopted from Russia.7-9
When it came to linear growth, the mean height z score in the initial evaluation was half that reported by other researchers.8-10 Despite the significant catch-up linear growth in the first year after adoption and the sustained catch-up through age 10 years, coinciding with the age at thelarche, from this point on linear growth stabilised, and the mean height at age 15 years was 3.2 cm smaller compared to the WHO11 and Russian13 child growth standards.
As for pubertal development, the mean age at thelarche (9.9 years) and menarche (11.9 years) was lower compared to the reference populations of the WHO (menarche 12.8 years)20, Russian (menarche 13.2 years)20 and Spanish (thelarche 10.7 years; menarche 12.6-12.9 years) growth standards.21,22
In the comparison to other cohorts of internationally adopted girls in Spain, girls adopted from Russia exhibited earlier pubertal development than girls adopted from China (thelarche 10.1 years; menarche 12.2 years)23 and later puberty compared to those adopted from Ukraine (thelarche 9.1 years; menarche 11.2 years).24 It is worth noting that Chinese girls were adopted at a significantly earlier age (1.3 years) and that they had been infrequently exposed to adverse exogenous factors, while Ukrainian girls had been adopted at an older age (3.9 years) and the proportion exposed to adverse exogenous factors was similar to the proportion found in the cohort of Russian girls.
Although we could not determine the underlying pathophysiological mechanisms, the pattern of growth and pubertal development observed in the cohort of girls adopted from Russia suggested that, in addition to endogenous factors (one of the limitations of the study was the lack of data on the height and pubertal development of the biological parents), various adverse exogenous factors could have been present in a high proportion of adopted Russian girls as well as the history of late adoption. The interaction of these factors could explain the significant delay in growth observed at the time of adoption, the rapid and persistent catch-up growth, the acceleration of pubertal development with thelarche and menarche at early ages and the incomplete recovery of linear growth.
CONCLUSION
In this case series of girls adopted from Russia, the longitudinal trends in growth and development trends were characterised by severe linear growth delay and moderate delay in weight and head circumference at the time of adoption, rapid, significant and prolonged catch-up growth, accelerated pubertal development with early thelarche and menarche and incomplete height recovery.
CONFLICTS OF INTEREST
The author has no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS
BMI: body mass index · P: percentile · SD: standard deviation · WHO: World Health Organization
REFERENCES
- Hermanussen M, Erofeev S, Scheffler C. The socio-endocrine regulation of human growth. Acta Paediatr. 2022;111(11):2077-81. https://doi.org/10.1111/apa.16504
- Miller BS, Spratt EG, Himes JH, Condon D, Summer A, Papa CE, et al. Growth failure associated with early neglect: pilot comparison of neglected US children and international adoptees. J Pediatr Endocrinol Metab. 2014;28(1-2):111-5. https://doi.org/10.1515/jpem-2014-0231
- Mason P, Narad C. Long-term growth and puberty concerns in international adoptees. Pediatr Clin North Am. 2005;52(5):1351-68. https://org/10.1016/j.pcl.2005.06.016
- Oliván Gonzalvo G. Adopción en la Federación Rusa y Europa del Este: problemas de salud y recomendaciones médicas [Adoption in the Russian Federation and Eastern Europe: health problems and medical recommendations]. Rev Pediatr Aten Primaria. 2006;8(30):265-81.
- Judge S. Developmental recovery and deficit in children adopted from Eastern European orphanages. Child Psychiatry Hum Dev. 2003;34(1):49-62. https://doi.org/10.1023/a:1025302025694
- Pomerleau A, Malcuit G, Chicoine JF, Seguin R, Belhumeur C, Germain P, et al. Health status, cognitive and motor development of young children adopted from China, East Asia and Russia across the first six months after adoption. Journal of Applied Developmental Psychology. 2005;29(5):445-57. https://doi.org/10.1177/0165025050020625
- Van Ijzendoorn MH, Bakermans-Kranenburg MJ, Juffer F. Plasticity of growth in height, weight, and head circumference: meta-analytic evidence of massive catch-up after international adoption. J Dev Behav Pediatr. 2007;28(4):334-43. https://doi.org/10.1097/DBP.0b013e31811320aa
- Miller BS, Kroupina MG, Iverson SL, Mason P, Narad C, Himes JH, et al. Auxological evaluation and determinants of growth failure at the time of adoption in Eastern European adoptees. J Pediatr Endocrinol Metab. 2009;22(1):31-9. https://doi.org/10.1515/JPEM.2009.22.1.31
- Miller BS, Kroupina MG, Mason P, Iverson SL, Narad C, Himes JH, et al. Determinants of catch-up growth in international adoptees from eastern europe. Int J Pediatr Endocrinol. 2010;2010:107252. https://doi.org/10.1155/2010/107252
- Palacios J, Román M, Camacho C. Growth and development in internationally adopted children: extent and timing of recovery after early adversity. Child Care Health Dev. 2011;37(2):282-8. https://doi.org/10.1155/2010/107252
- World Health Organization. Child Growth Standards. The WHO Anthro Software. 2023 [online] [accessed 16/01/2024]. Available at www.who.int/tools/child-growth-standards/software
- Wit JM, Boersma B. Catch-up growth: definition, mechanisms, and models. J Pediatr Endocrinol Metab. 2002;15 Suppl 5:1229-41.
- Martinchik AN, Baturin AK, Keshabyants EE, Peskova EV. Ретроспективная оценка антропометрических показателей детей России в 1994–2012 гг. по новым стандартам ВОЗ. [Retrospective assessment of anthropometric measurements of children in Russia 1994–2012 according to the new WHO standards]. Pediatria n.a. G.N. Speransky. 2015;94(1):156-60. https://doi.org/10.15690/pf.v13i4.1608
- Dominé F, Parent AS, Rasier G, Lebrethon MC, Bourguignon JP. Assessment and mechanism of variations in pubertal timing in internationally adopted children: a developmental hypothesis. Eur J Endocrinol. 2006;155(1):S17-S25. https://doi.org/10.1530/eje.1.02252
- Teilmann G, Petersen JH, Gormsen M, Damgaard K, Skakkebaek NE, Jensen TK. Early puberty in internationally adopted girls: hormonal and clinical markers of puberty in 276 girls examined biannually over two years. Horm Res. 2009;72(4):236-46. https://doi.org/10.1159/000236085
- Stagi S, Papacciuoli V, Boiro D, Maggioli C, Ndambao NN, Losi S, et al. Auxological and endocrinological features in internationally adopted children. Ital J Pediatr. 2020;46(1):82. https://doi.org/10.1186/s13052-020-00832-5
- Proos LA, Hofvander Y, Tuvemo T. Menarcheal age and growth pattern of Indian girls adopted in Sweden. I. Menarcheal age. Acta Paediatr Scand. 1991;80(8-9):852-8. https://doi.org/10.1111/j.1651-2227.1991.tb11960.x
- Oliván-Gonzalvo G. Prevalencia de prematuridad, bajo peso al nacimiento y desnutrición en la infancia temprana en niños rusos asignados para adopción internacional [Prevalence of prematurity, low birth weight and malnutrition in early childhood in Russian children assigned for international adoption]. An Pediatr (Engl Ed). 2019;91(3):214-5. https://doi.org/10.1016/j.anpedi.2019.04.011
- Miller LC, Chan W, Litvinova A, Rubin A, Tirella l, Cermak S. Medical diagnoses and growth of children residing in Russian orphanages. Acta Paediatr. 2007;96(12):1765-9. https://doi: 10.1111/j.1651-2227.2007.00537.x
- Wang Y, Adair l. How does maturity adjustment influence the estimates of overweight prevalence in adolescents from different countries using an international reference? Int J Obes Relat Metab Disord. 2001;25(4):550-8. https://doi.org/10.1038/sj.ijo.0801580
- Ferrández Longás A, Baguer l, Labarta JI, Labena C, Mayayo E, Puga B, et al. Longitudinal study of normal Spanish children from birth to adulthood: anthropometric, puberty, radiological and intellectual data. Pediatr Endocrinol Rev. 2005;2(Suppl 4):425-53.
- Carrascosa A, Yeste D, Moreno-Galdó A, Gussinyé M, Ferrández Á, Clemente M, et al. Crecimiento puberal de 1.453 niños sanos según la edad de inicio de la pubertad. Estudio longitudinal de Barcelona [Pubertal growth of 1.453 healthy children according to age at pubertal growth spurt onset. The Barcelona longitudinal growth study]. An Pediatr (Engl Ed). 2018;89(3):144-52. https://doi.org/10.1016/j.anpedi.2017.11.018
- Oliván-Gonzalvo G. Crecimiento y desarrollo puberal en niñas adoptadas de China: seguimiento de 15 años [Growth and pubertal development in girls adopted from China: 15-year follow-up]. An Pediatr (Engl Ed). 2023;99(2):136-8. https://doi.org/10.1016/j.anpedi.2023.03.006
- Oliván Gonzalvo G. Adopted children from Ukraine: health outcomes on arrival and long-term. IAR Jr Clnc Res. 2022;2(2):1-8.