
Vol. 25 - Num. 99
Original Papers
Use of antibiotics for treatment of acute pharyngitis in the province of Albacete
Carlos Marcilla Vázqueza, Juan Ríos Laordenb, Ángeles Lloret Callejoc, Francisco Tejada Cifuentesc, M.ª José Tirado Peláezc
aServicio de Pediatría. Complejo Hospitalario Universitario. Gerencia de Atención Integrada de Albacete. Albacete. España.
bPediatra. CS Zona VI. Gerencia de Atención Integrada de Albacete. Albacete. España.
cFarmacéutico de Atención Primaria. Gerencia de Atención Integrada de Albacete. Albacete. España.
Correspondence: C Marcilla. E-mail: carlos.marcilla11@gmail.com
Reference of this article: Marcilla Vázquez C, Ríos Laorden J, Lloret Callejo A, Tejada Cifuentes F, Tirado Peláez MJ. Use of antibiotics for treatment of acute pharyngitis in the province of Albacete . Rev Pediatr Aten Primaria. 2023;25:e85-e90. https://doi.org/10.60147/7207cc49
Published in Internet: 02-10-2023 - Visits: 13229
Abstract
Introduction: acute pharyngitis (AP) is one of the most prevalent diseases in the paediatric population and one of the leading causes of antibiotic prescribing in this age group.
Material and methods: observational and descriptive study of the use of antibiotics for treatment of AP. We included all children in our catchment area who received a prescription for antibiotics for treatment of AP in a 3 year period.
Results: a total of 53 995 cases of AP were diagnosed in the 3-year study period, out of which 33 426 (61.9%) were treated with antibiotics. In children aged less than 3 years, 10 901 cases of AP were diagnosed (20.2% of total cases of AP), of which 6494 were treated with antibiotics (59.6%).
We found that the most frequently prescribed antibiotics were beta-lactamase sensitive penicillins (phenoxymethylpenicillin, benzathine phenoxymethylpenicillin) and amoxicillin (60.3% of prescriptions in the first year, 60.9% in the second one and 66.8% in the third year), while other antibiotic classes were used less often: amoxicillin-clavulanic acid in 2475 cases (18.2%) in year 1 of the study, 1754 (17.7%) in year 2 and 1644 (16.6%) in year 3. Furthermore, we found a decrease in the use of macrolides: 2825 prescriptions (20.7%) the first year, 1933 (19.6%) the second year and 1419 (14.3%) the last year.
Conclusions: the use of amoxicillin-clavulanic acid and macrolides is significantly greater than would be expected given the low prevalence of Streptococcus pyogenes nasopharyngeal carriage or penicillin allergy in the paediatric population.
Keywords
● Acute pharyngitis ● Antibiotics ● Paediatric populationINTRODUCTION
In the paediatric population of Spain, there is a high consumption of systemic antibiotics at the community level.1 In fact, in 2019 Spain was the fifth country with the highest consumption of antibiotics in Europe, based solely on data for official prescriptions funded by the National Health System. 2 This excessive consumption is not particular to any age group, and the consumption is also high in the paediatric population.3
Acute pharyngitis (AP) is one of the most prevalent diseases in the paediatric age group and one of the main reasons for antibiotic prescribing in this subset of the population. To avoid overuse of antibiotics in the context of this disease, which in most cases has a viral aetiology, performance of antimicrobial testing is recommended, as basing the diagnosis exclusively in clinical features can lead to misdiagnosis in up to 20-25% of patients.4-6 The consensus document on the diagnosis and treatment of AP already highlighted the importance of microbiological testing (rapid streptococcal antigen detection [strep antigen] test or nasopharyngeal swab culture) in select patients who meet the criteria for probable streptococcal infection and who have not started antibiotherapy.7 The updated statement published in 2020 recommends microbiological testing in all patients and restricting empiric antibiotherapy based on the clinical features to situations in which microbiological testing is not available.4
The aim of our study was to assess the use of antibiotics and appropriateness of antibiotic prescribing in the catchment area of the Integrated Health Care Administration of Albacete (Spain) in children with a diagnosis of AP, stratifying the analysis by age group and comparing it to the most recent recommendations published in the updated version of the consensus document on the diagnosis and treatment of AP. The large sample size allowed us to make a critical analysis of the main aspects of inappropriate antimicrobial prescribing and use.
MATERIAL AND METHODS
We conducted an observational and descriptive study of medication use focused on the prescribing of antibiotics in the paediatric population served by the o Integrated Health Care Administration of Albacete.
The sample comprised all children (0-14 years) who, during the 3-year study period, received a prescription for at least one antibiotic on account of an AP diagnosis. Subsequently, we made a descriptive analysis of the study variables after collecting the corresponding data from the electronic primary care health records system (Turriano) of the Department of Health of Castilla la Mancha (SESCAM). All data were coded for anonymisation.
We collected data on the following variables:
- Day of the week of prescription; month of prescription.
- Sex and date of birth of patient.
- Diagnosis: we used the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-MC) and the International Classification of Primary Care (ICPC) (Table 1).
- Antibiotic: we used the Anatomical Therapeutic Chemical Classification (ATC) System therapeutic subgroup code J01.
- Primary care centre.
| Table 1. Population data, group with acute pharyngitis and antibiotic use | ||||
|---|---|---|---|---|
| Year 1 | Year 2 | Year 3 | ||
| Population aged 0-14 years | Total | 38 857 | 38 303 | 38 299 |
| Received care for AP episode | 19 868 | 16 882 | 17 245 | |
|
Received care for AP episode and treated with ABX (% of total) (% of patients who received care for AP) |
13 633 (35.1%) (68.6%) |
9889 (25.8%) (58.6%) |
9904 (25.9%) (57.4%) |
|
| Population aged 0-3 years | Total | 6607 | 6192 | 6205 |
| Received care for AP episode | 2999 | 4026 | 3876 | |
|
Received care for AP episode and treated with ABX (% of total) (% of patients who received care for AP) |
2733 (45.4%) (91.1%) |
2187 (35.3%) (54.3%) |
1574 (25.4%) (40.6%) |
|
|
ABX: antibiotics; AP: acute pharyngitis. |
||||
The study was conducted in adherence to the principles of the Declaration of Helsinki and Organic Law on the Protection of Personal Data enacted on May 25, 2018. The study was approved by the Ethics Committee on Research with Medicines of our catchment area.
RESULTS
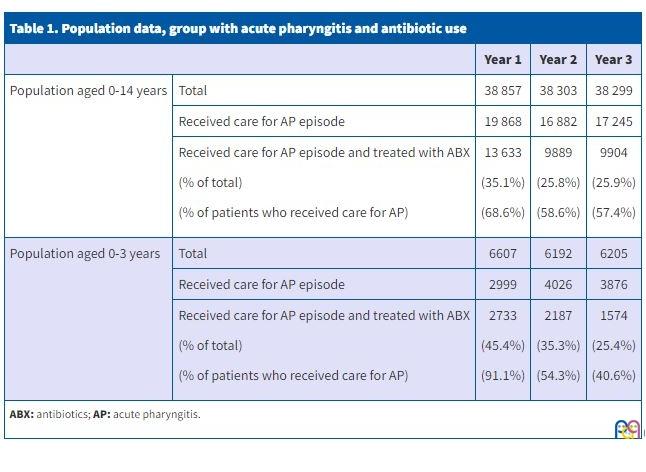
The population under study remained constant through the 3-year period, with 38 857 children aged 0-14 years in year 1 of the study and 38 299 the last year. The same was the case of the population aged less than 3 years: 6607 in year 1, 6192 in year 2 and 6205 in year 3.
The first year, 35.1% of the paediatric population received antibiotherapy for an AP episode, a percentage that subsequently decreased, to 25.8% in year 2 and 25.9% in year 3. A total of 53 995 episodes of AP were managed in the 3-year study period, with a fairly uniform distribution by year: 19 868 children in year 1, 16 882 in year 2 and 17 245 in year 3. Of the total cases of AP, 33 426 (61.9%) were treated with antibiotics. Analysing the case distribution by year, we did find significant differences, with a decreasing trend over the followup: in year 1, 13 633 (68.6%) of the cases were treated with antibiotics, compared to 9889 (58.6in year 2 and 9904 (57.4%) in year 3.
Focusing on children under 3 years, in whom AP is less frequent and the causative agent is usually viral, we found that a total of 10 901 cases of AP (20.2% of total paediatric AP cases) were managed during the study period: 2999 in year 1, 4026 in year 2 and 3876 in year 3. Of this total, 6494 (59.6%) were treated with antibiotics, and we found the same decreasing trend in the prescribing of antibiotics through the years: 2733 of cases treated in year 1 (91.1%), 2187 (54.3%) in year 2 and 1574 (40.6%) in year 3 (Table 1).
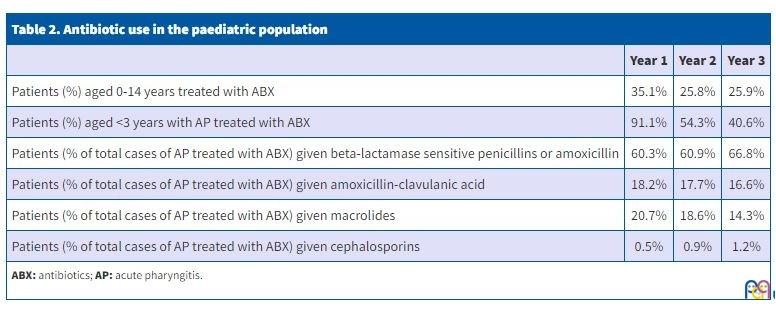
When it came to the selection of the antibiotic for treatment of AP, we found an increase in the prescribing of beta-lactamase sensitive penicillins (including phenoxymethylpenicillin and benzathine phenoxymethylpenicillin) and amoxicillin at the end of the study period, from 60.3% and 60.9% in years 1 and 2, respectively, to 66.8% in year 3. The most frequently used antibiotic was amoxicillin: 6725 cases in year 1 (81.4% of total cases treated with beta-lactamase sensitive penicillins or amoxicillin), 4760 (79%) in year 2 and 4916 (74.3%) in year 2. In contrast, the number of cases treated with amoxicillin-clavulanic acid relative to the total cases treated with antibiotics decreased through the 3-year period: 2475 (18.2%) in year 1, 1754 (17.7%) in year 2 and 1644 (16.6%) in year 3. Considering the use of this antibiotic in relation to the total number of diagnosed cases of AP, we found that amoxicillin-clavulanic acid was used to treat 12.5% in year 1, 10.4% in year 2 and 9.5% in year 3.
Similarly, there was a marked decrease in the treated cases of AP that were treated with macrolides: 2825 (20.7%) in year 1, 1933 (19.6%) in year 2 and 1419 (14.3%) in year 3. The use of this group of drugs relative to the overall diagnosed cases of AP was also considerable, as 14.2% of total cases of AP in year 1 were treated with macrolides, a percentage that decreased the two following years to 11.5% and 8.2%. Among the macrolides, azithromycin was the most frequently used antibiotic: in 2797 of treated cases in year 1 (99% of total cases treated with macrolides), 1905 (98.6%) in year 2 and 1405 (99%) in year 3.
The use of cephalosporins for treatment of AP was lower compared to the groups discussed above. They were used in only 95 of treated cases in year 1 (0.7%), 159 in year 2 (1.6%) and 201 in the last year (2%). In relation to the total cases of AP, the percentage treated with cephalosporins is all but negligible: 0.5% of diagnosed cases of AP in the first year under study were treated with cephalosporins, 0.9 % in year 2 and 1.2 % in year 3. The most frequently used cephalosporins were cefuroxime and cefixime: 82 cases treated in year 1 (86.3% of cases treated with cephalosporins), 142 (89.3%) in year 2 and 188 (93.5%) in year 3 (Table 2).
| Table 2. Antibiotic use in the paediatric population | |||
|---|---|---|---|
| Year 1 | Year 2 | Year 3 | |
| Patients (%) aged 0-14 years treated with ABX | 35.1% | 25.8% | 25.9% |
| Patients (%) aged <3 years with AP treated with ABX | 91.1% | 54.3% | 40.6% |
| Patients (% of total cases of AP treated with ABX) given beta-lactamase sensitive penicillins or amoxicillin | 60.3% | 60.9% | 66.8% |
| Patients (% of total cases of AP treated with ABX) given amoxicillin-clavulanic acid | 18.2% | 17.7% | 16.6% |
| Patients (% of total cases of AP treated with ABX) given macrolides | 20.7% | 18.6% | 14.3% |
| Patients (% of total cases of AP treated with ABX) given cephalosporins | 0.5% | 0.9% | 1.2% |
|
ABX: antibiotics; AP: acute pharyngitis. |
|||
DISCUSSION
Acute pharyngitis is a disease manifesting with inflammation of the pharyngeal and/or tonsillar mucosa, and its aetiology is most frequently viral. Among the bacterial causative agents, the most common is Streptococcus pyogenes, responsible for 30-40% of AP cases in children aged more than 3 years. At younger ages, the proportion of cases with a bacterial aetiology decreases to 10-14%.7-9 Analysing the results of our study, the proportion of patients with a diagnosis of AP who received antibiotherapy was consistent with the prevalence of infection by Streptococcus pyogenes described in the paediatric population aged more than 3 years (35.1% in the first year, with a decrease in the 2 subsequent years to 25.8% and 25.9%). This decrease may be explained by the introduction in 2018 of the rapid streptococcal antigen detection test in primary care centres, which allows the treatment of patients with confirmed infection, which prevents inappropriate treatments resulting from the use of clinical rules in up to one third of patients.4,10,11 The proportion of patients aged less than 3 years seeking care for AP who are treated with antibiotics is disproportionally high, of up to an unacceptable 91.1% in the first year of life, with a significant descent to the 54.3% and 40.6% in the next two years, which is still far higher than would be expected for this age group.
Beta-lactamase sensitive penicillins (including phenoxymethylpenicillin and benzathine phenoxymethylpenicillin) and amoxicillin are the antimicrobials used most frequently for treatment of AP, used in 60.3% to 66.8% of cases. Oral penicillin is the first-line antibiotic agent for treatment of streptococcal AP, and amoxicillin is the alternative of choice. Both of these antibiotics have a narrow spectrum of activity, are safe and effective and achieve rapid improvement of symptoms, prevent complications of disease and shorten the infectious period.4,12,13 Therefore, their use was appropriate, and these were the antibiotics used most frequently to treat AP, although we may consider it lower than would be expected given the low incidence of penicillin allergy in the paediatric population (ranging from 1.7% to 5.2%, in which case treatment with cephalosporins or macrolides would be indicated), first-line treatment failure or carrier status.4,14
Amoxicillin-clavulanic acid was used to treat 9.5% to 12.5% of patients with a diagnosis of AP, depending on the year. This antibiotic should be reserved for patients with first-line treatment failure, known carrier status and patients with any of the following characteristics: personal or family history of rheumatic fever, recurrent outbreaks of AP or invasive Streptococcus pyogenes group A infection in the family, institutionalization in residential facility, living with an immunosuppressed individuals or patients in whom tonsillectomy is considered as a treatment of last resort. Given that the prevalence of carriage in children is 12%, the percentage of patients treated with amoxicillin-clavulanic acid was greater than should be expected, especially considering that in such cases there are other valid alternatives, such as clindamycin or azithromycin, to name a few.4,7,15,16
The use of cephalosporins amounted to 0.7 to 2% of patients treated with antibiotics, figures that are to be expected given that 1.7 to 5.2% of the paediatric population is allergic to penicillin.14 However, when it came to the use of cephalosporins, the choice of antibiotic was often inappropriate, with an excessive use of second- and third-generation cephalosporins (chiefly cefuroxime and cefixime, which were used in more than 85% of AP cases treated with cephalosporins). First-generation cephalosporins are the treatment of choice in children with delayed-type hypersensitivity to penicillin/amoxicillin, of which cefadroxil is considered most appropriate in most guidelines on account of its good tolerability and narrower spectrum of activity.4,12,17,18
The most significant type of inappropriate antimicrobial use identified in our study may been the high use of macrolides (8.2% to 14.2% of cases of AP were treated with this class of antibiotics, amounting to 14.3% to 20.7% of the cases of AP treated with antibiotics). This overuse greatly exceeds what would be expected based on the low prevalence of penicillin hypersensitivity reactions, as noted in the previous paragraph.14 Macrolides should be used exclusively in patients with immediate or anaphylactic reactions to beta-lactam antibiotics.4,7,12,17 Azithromycin was the most frequently used macrolide (more than 98% of cases treated with macrolides in the 3-year study period), which was also a significant form of inappropriate antimicrobial use given that in recent years there has been an increase in the prevalence of group A beta-haemolytic Streptococcus strains resistant to macrolides, which, while still below 10% overall, may be much higher for emm type strains. These are resistant only to 14- and 15-membered ring macrolides, of which azithromycin is one, so the best option in allergic patients are 16-membered ring macrolides, such as josamycin and diacetyl-midecamycin.4,19
After retrieving the data for 2017, an educational intervention that targeted the health care professionals in the catchment area was implemented in the form of a course, offered several times, reviewing the indications for antibiotherapy for management of AP and the appropriate selection of antibiotics based on the characteristics of the patient (first-line treatment failure, carrier status or penicillin allergy). While we observed a subsequent decrease in the use of antibiotics and more appropriate prescribing of these drugs (greater use of amoxicillin or beta-lactamase sensitive penicillins and decreased use of amoxicillin-clavulanic acid and macrolides), we cannot attribute this improvement completely to the educational intervention, although the findings do reinforce the need for this type of activities and the surveillance of indicators of antibiotic use.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation or publication of this article.
AUTHOR CONTRIBUTIONS
All authors contributed equally to the manuscript.
ABBREVIATIONS
AP: acute pharyngitis
REFERENCES
- Albañil MR. Plan Nacional de Resistencia a Antibióticos. Form Act Pediatr Aten Prim. 2016;9: 56-9.
- European Centre for Disease Prevention and Control. Antimicrobial consumption in the EU/EEA, annual epidemiological report for 2019. Stockholm: ECDC; 2020:4-9 [online] [accessed 14/09/2023]. Available at www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-consumption-europe-2019
- Malo S, Bjerrum l, Feja C, Lallana MJ, Poncel A, Rabanaque MJ. Prescripción antibiótica en infecciones respiratorias agudas en Atención primaria. An Pediatr. 2014;82:412-6.
- Piñeiro R, Álvez F, Baquero F, Cruz M, De la Flor i Bru J, Fernández A, et al. Actualización del documento de consenso sobre el diagnóstico y tratamiento de la faringoamigdalitis aguda. An Pediatr (Barc). 2020;93(3):206e.1-206e.8.
- Gerber M, Shulman S. Rapid diagnosis of pharyngitis caused by group A Streptococci. Clin Microbiol Rev. 2004;17:571-80.
- Fine A, Nizet V, Mandl K. Large-Scale validation of the Centor and McIsaac scores to predict Group A streptococcal pharyngitis. Arch Intern Med. 2012;172:847-52.
- Piñeiro R, Hijano F, Álvez F, Fernández A, Silva JC, Pérez C, et al. Documento de consenso sobre el diagnóstico y tratamiento de la faringoamigdalitis aguda. An Pediatr (Barc). 2011;75(5):342e.1-342e.13.
- Álvez Ginzález F. Faringitis estreptocócica en niños menores de 2 años. An Pediatr (Barc). 2008;68:525-39.
- Shaikh N, Leonard E, Martin J. Prevalence of streptococcal pharyngitis and streptococcal carriage in children: a metaanalysis. Pediatrics. 2010;126:557-64.
- Ochoa Sangrador C, Andrés de Llano JM. Los síntomas y signos clínicos no son suficientemente válidos para diagnosticar la faringitis estreptocócica. Evid Pediatr. 2012;8:23.
- Le Marechal F, Martinot A, Duhamel A, Ptuvost I, Dubos F. Streptococcal pharyngitis in children: a meta-analysis of clinical decision rules and their clinical variables. BMJ Open. 2013;3(3):e001482.
- Shulman ST, Bisno AL, Clegg HV, Gerber MA, Kaplan EL, Lee G, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55:1279-82.
- Van Driel ML, De Sutter AI, Habraken H, Thorning S, Christiaens T. Different antibiotic treatments for group A streptococcal pharyngitis. Cochrane Database Syst Rev. 2016;9.CD004406.
- Baquero F, Michavila A, Suárez Rodríguez A, Hernandez A, Martínez Campos l, Calvo C, et al. Documento de consenso de la Sociedad Española de Infectología Pediátrica, Sociedad Española de Inmunología Clínica y Alergia Pediátricas, Asociación Española de Pediatría de Atención Primaria y Sociedad Española de Pediatría Extrahospitalaria y Atención Primaria sobre antibioterapia en alergia a penicilina o Amoxicilina. An Pediatr (Barc) 2017;86:99.e1-99.e9.
- Oliver J, Malliya Wadu E, Pierse N, Moreland NJ, Williamson DA, Baker MG. Group A Streptococcus pharyngitis and pharyngeal carriage: A meta-analysis. PLoS Negl Trop Dis. 2018;12(3):e0006335.
- Shulman ST, Tanz RR, Dale JB, Beall B, Kabat W, Kabat K, et al. Seven-year surveillance of north american pediatric group A streptococcal pharyngitis isolates. Clin Infect Dis. 2009;49:78-84.
- Pichichero M. Treatment and prevention of streptococcal pharyngitis. 2019 [online] [accessed 14/09/2023]. Available at https://sso.uptodate.com/contents/treatment-and-prevention-of-streptococcal-pharyngitis-in-adults-and-children
- Campagna JD, Bond MC, Schabelman E, Hayes BD. The use of cephalosporins in penicillin-allergic patients: a literature review. J Emerg Med. 2012;42:612-20.
- Calle Miguel l, Pérez Méndez C, Miguel Martínez MD, Lombraña Álvarez E, García García E, Solís Sánchez G. Cambios evolutivos en las tasas y fenotipos de resistencia de Streptococcus pyogenes en una población pediátrica de Asturias, España (2005-2015). Rev Esp Quimioter. 2017;30:90-5.