
Vol. 25 - Num. 98
Original Papers
Hashimoto's thyroiditis: clinical and biochemical manifestations and their association with autoimmune and non-autoimmune diseases
Ana Laura Bahena Garcíaa, Sofía Elizondo Benetb, Héctor Eliud Arriaga Cázaresc, Samantha Garza Fuentesa
aDepartamento de Endocrinología Pediátrica. Unidad Médica de Alta Especialidad #25. Nuevo León. México.
bDepartamento de Pediatría. Unidad Médica de Alta Especialidad #25. Nuevo León. México.
cDepartamento de Investigación. Unidad Médica de Alta Especialidad #21. Nuevo León. México.
Correspondence: S Elizondo. E-mail: sofia.elizondob@gmail.com
Reference of this article: Bahena García AL, Elizondo Benet S, Arriaga Cázares HE, Garza Fuentes S. Hashimoto's thyroiditis: clinical and biochemical manifestations and their association with autoimmune and non-autoimmune diseases . Rev Pediatr Aten Primaria. 2023;25:137-44.
Published in Internet: 12-06-2023 - Visits: 50814
Abstract
Introduction: Hashimoto thyroiditis is the most frequent cause of thyroid dysfunction in children, with an incidence of 1 to 2%. This autoimmune disease is usually associated with other pathologies. The objective of the study was to determine whether Hashimoto thyroiditis (clinical or biochemical) is associated with other diseases in paediatric patients, and to establish guidelines for early detection and treatment.
Material and methods: we conducted a cross-sectional observational and descriptive study over a 15-year period in patients with Hashimoto thyroiditis aged less than 15 years managed by Specialty Care Unit #25 in a north-eastern region in Mexico. We analysed variables such as the familial clustering or history of thyroid, autoimmune or malignant disease, sex, age, reason for seeking medical care, thyroid function at diagnosis and the presence of autoimmune and non-autoimmune comorbidities.
Results: the sample included 110 patients. The most frequent reason for seeking care at the time of diagnosis was the chance detection of TSH elevation. Eighty percent had onset with overt biochemical hypothyroidism. Twenty-six percent of patients had an associated non-thyroid autoimmune disease, most frequently type 1 diabetes mellitus, found in 18%, followed by others such as vitiligo, systemic lupus erythematosus and Addison disease. Obesity was the most frequent non-autoimmune comorbidity.
Conclusions: paediatric patients with Hashimoto thyroiditis are at high risk of non-thyroid autoimmune disease, chiefly type 1 diabetes mellitus. We found that male paediatric patients with Hashimoto thyroiditis were at high risk of having non-thyroid autoimmune disease.
Keywords
● Adolescent ● Autoimmune thyroiditis ● Child ● Chronic lymphocytic thyroiditis ● HypothyroidismINTRODUCTION
Hashimoto thyroiditis, also known as chronic autoimmune thyroiditis (CAT) or chronic lymphocytic thyroiditis, is the most frequent cause of acquired hypothyroidism and goitre in children and adolescents. Its prevalence in children is of 1 to 2%, and it is more frequent in girls and in puberty.1
The term thyroiditis is defined as evidence of “intrathyroidal lymphocytic infiltration” with or without follicular damage. Two types of CAT cause persistent hypothyroidism: Hashimoto disease (goitrous form) and atrophic thyroiditis (without goitre). Both are characterised by circulating thyroid autoantibodies and varying degrees of thyroid dysfunction, differing only by the presence or absence of goitre.2 Chronic autoimmune thyroiditis can be suspected in the presence of goitre, even if there are no signs or symptoms of thyroid dysfunction. Among symptomatic patients, the most frequent manifestations are goitre and growth delay.3 It may also be an incidental finding in medical check-ups or in the management of children with autoimmune comorbidities: type 1 diabetes,4,5 coeliac disease6 and vitiligo.7,8 It may also be present in children with chromosomal abnormalities, such as Turner, Down or Klinefelter syndrome, with rheumatic diseases, such as systemic lupus erythematosus,9,10 and metabolic diseases,11 such as type 2 diabetes,12 among others.
Its aetiology is multifactorial and involves genetic, environmental and endogenous factors in the development of autoimmunity. Up to 30% of affected individuals may have a family history of autoimmune thyroid disease, highlighting the importance of genetic predisposition to the disease, especially in the paediatric age group, in which genetic factors may be involved in up to 80% of cases.13 Some of the possible environmental factors are a high iodine intake, selenium deficiency, exposure to tobacco smoke or other pollutants, infectious disease or stress. The level of thyroid-stimulating hormone (THS) has been suggested as a possible marker of cardiometabolic risk.14
The association between chronic inflammation and the development of cancer is well known. If thyroid nodules are detected, they need to be evaluated to rule out malignancy. Chronic lymphocytic thyroiditis may make it difficult to arrive to the correct diagnosis, as it has cytological features that may give rise to indeterminate or conflicting results.15 It is important to recognise the overall shift in the spectrum of histotypes and underlying molecular alterations common in paediatric thyroid cancer, as it may directly influence diagnostic test selection and therapeutic recommendations.16
The aim of our study was to identify the most frequent comorbidities in paediatric patients with Hashimoto thyroiditis and determine their association with other autoimmune and non-autoimmune diseases to allow the development of guidelines for early diagnosis in the future.
MATERIAL AND METHODS
We conducted a cross-sectional observational and descriptive study of patients with a diagnosis of Hashimoto thyroiditis aged less than 15 years managed at the Speciality Care Unit #25 of Monterrey, Nuevo León, Mexico, in the 2006-2021 period. The study was approved by the local clinical research ethics committee.
We recruited patients by consecutive sampling, including all who were eligible. We collected data from the health records of patients aged less than 15 years with a diagnosis of Hashimoto thyroiditis who had complete records and positive thyroid peroxidase antibody test results. We excluded patients lost to followup or with a diagnosed chromosomal abnormality. We analysed different variables, such as sex, age, the reason for seeking care and thyroid function at the time of diagnosis, the presence of comorbidities and the hereditary/family history of thyroid disease, autoimmune or malignant, and of other autoimmune diseases.
We used measures of central tendency, such as the median for qualitative variables and the mean for quantitative variables. In the inferential analysis, we compared categorical data by means of the chi-square test and Fisher exact test, and considered p values of less than 0.05 statistically significant. Lastly, we calculated odds ratios (ORs).
RESULTS
We analysed 123 health records, of which 110 met the inclusion criteria (Table 1). Of this total, 84 (77%) corresponded to female patients. The median age at diagnosis was 10 years. Sixty patients (55%) were aged 4 to 10 years. The most frequent reason for seeking care was a chance findings of TSH elevation, followed by manifestations compatible with thyroid disease, such as weight gain, delayed growth or puberty and/or constipation (31% of patients).
| Table 1. General characteristics of 110 paediatric patients given a diagnosis of Hashimoto thyroiditis over a 15-year period | |
|---|---|
| Variable | Frequency, n (%) |
|
Mean age Median age |
9.9 years 10 years |
|
Sex Female Male |
85 (77) 25 (23) |
|
Reason for consultation Chance finding of TSH elevation Goitre Short stature Other manifestations of thyroid disease |
41 (37) 26 (24) 9 (8) 34 (31) |
|
Thyroid status at diagnosis Euthyroidism Subclinical hypothyroidism Overt hypothyroidism Hyperthyroidism |
15 (14) 19 (17) 75 (68) 1 (1) |
|
Autoimmune comorbidities None Type 1 diabetes SLE Vitiligo Addison disease |
82 (74) 20 (18) 1 (1) 6 (5) 2 (2) |
|
Non-autoimmune comorbidities None Obesity Thyroid cancer Metabolic syndrome |
79 (72) 17 (15) 9 (8) 5 (5) |
|
Family history None Autoimmune thyroid disease Other thyroid disease Thyroid cancer Other autoimmune disease |
86 (78) 4 (4) 15 (13) 3 (3) 2 (2) |
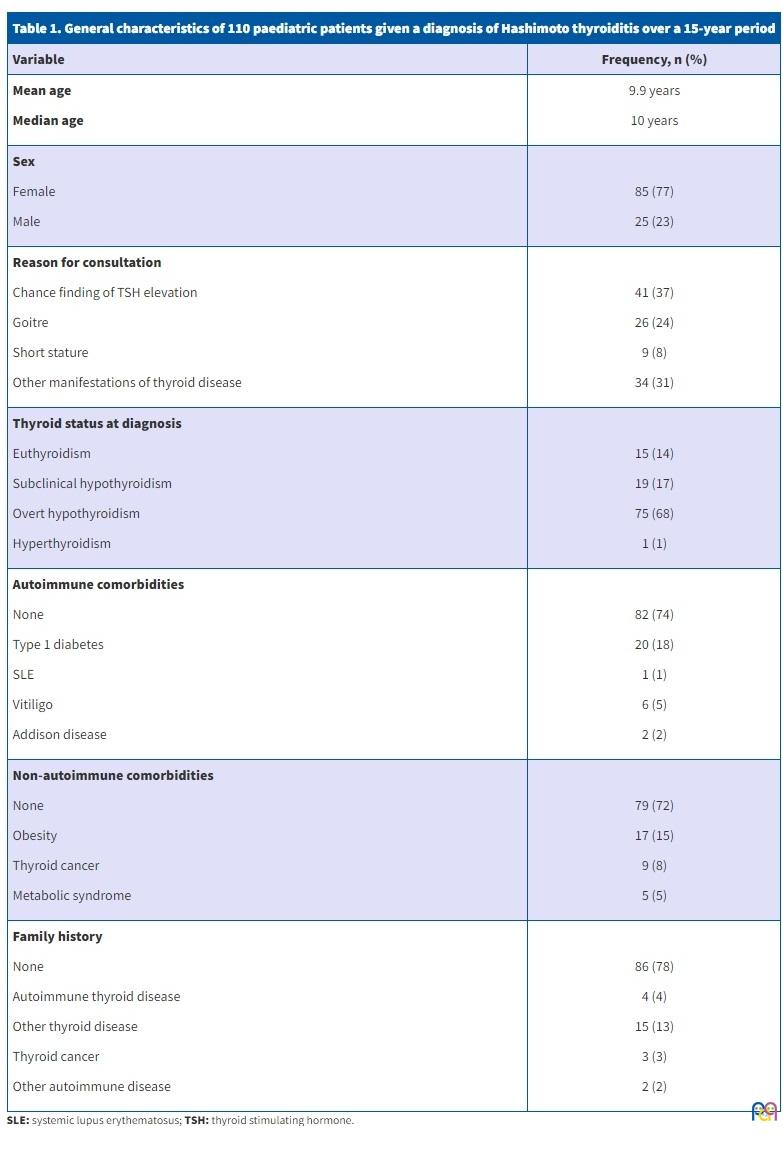
The most frequent biochemical profile at diagnosis was overt hypothyroidism, found in 75 (68%) of the patients, followed by subclinical hypothyroidism in 17%. Biochemical hyperthyroidism was only found in 1 patient. Most patients did not have a known relevant family/hereditary history of disease. Thirteen percent had a family history in first-degree relatives of non-autoimmune thyroid disease, 4% of autoimmune thyroid disease and 2%, of non-thyroidal autoimmune disease. In addition, 3% had a history of thyroid cancer.
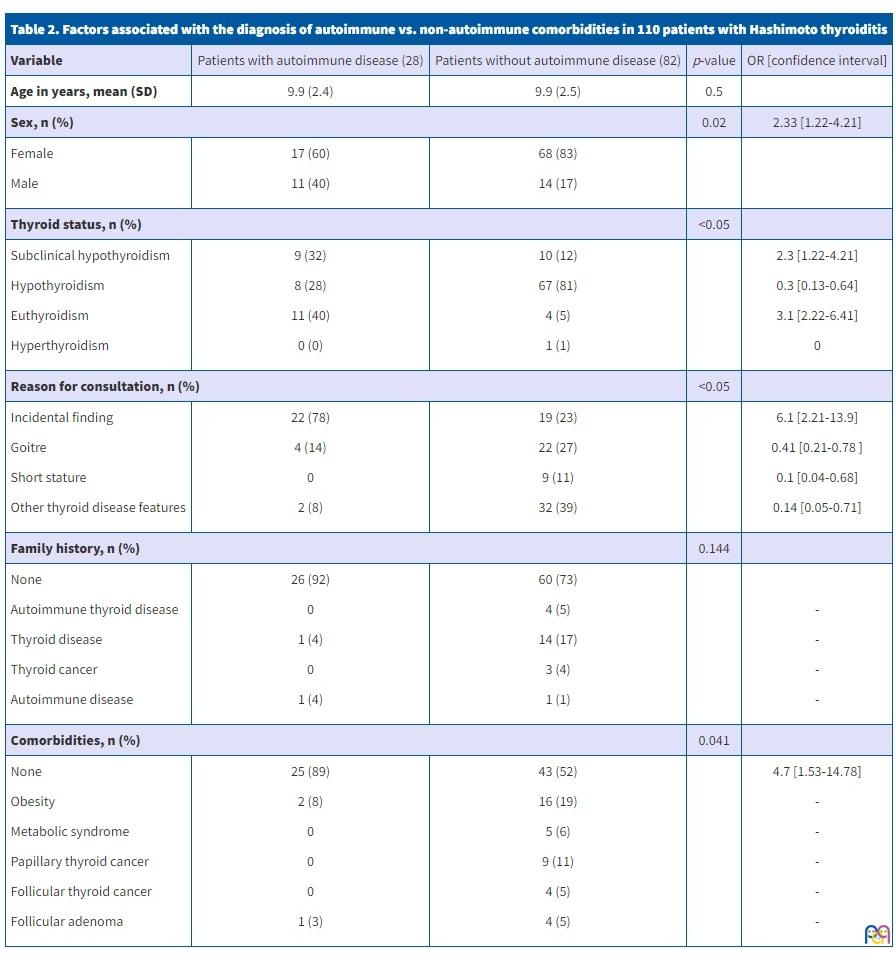
As regards autoimmune comorbidities in the sample of patients with Hashimoto thyroiditis, we found that 28 (26%) had another autoimmune disease. The most prevalent one was type 1 diabetes mellitus, present in 20 patients (18%). When it came to non-autoimmune comorbidities, obesity was the most frequent, present in 15%, while 8% had thyroid cancer. We divided patients into 2 categories: those who had an autoimmune comorbidity and those who did not; Table 2 presents the results of the comparative analysis. We did not find a significant difference in age between patients with and without autoimmune comorbidities, with a mean age of 9.9 years. When it came to sex, we found that out of the 85 female patients in the sample, 20% had another autoimmune disease, while of the 25 male patients, 44% had an autoimmune comorbidity (p = 0.02). In the group without autoimmune comorbidities, 81% of patients presented with overt hypothyroidism in the biochemistry panel performed at diagnosis of Hashimoto disease(p ≤0.05). On the other hand, 40% of patients with autoimmune comorbidities had normal thyroid function at diagnosis(p ≤0.001).
| Table 2. Factors associated with the diagnosis of autoimmune vs. non-autoimmune comorbidities in 110 patients with Hashimoto thyroiditis | ||||
|---|---|---|---|---|
| Variable | Patients with autoimmune disease (28) | Patients without autoimmune disease (82) | p-value | OR [confidence interval] |
| Age in years, mean (SD) | 9.9 (2.4) | 9.9 (2.5) | 0.5 | |
| Sex, n (%) | 0.02 | 2.33 [1.22-4.21] | ||
|
Female Male |
17 (60) 11 (40) |
68 (83) 14 (17) |
||
| Thyroid status, n (%) | <0.05 | |||
|
Subclinical hypothyroidism Hypothyroidism Euthyroidism Hyperthyroidism |
9 (32) 8 (28) 11 (40) 0 (0) |
10 (12) 67 (81) 4 (5) 1 (1) |
2.3 [1.22-4.21] 0.3 [0.13-0.64] 3.1 [2.22-6.41] 0 |
|
| Reason for consultation, n (%) | <0.05 | |||
|
Incidental finding Goitre Short stature Other thyroid disease features |
22 (78) 4 (14) 0 2 (8) |
19 (23) 22 (27) 9 (11) 32 (39) |
6.1 [2.21-13.9] 0.41 [0.21-0.78 ] 0.1 [0.04-0.68] 0.14 [0.05-0.71] |
|
| Family history, n (%) | 0.144 | |||
|
None Autoimmune thyroid disease Thyroid disease Thyroid cancer Autoimmune disease |
26 (92) 0 1 (4) 0 1 (4) |
60 (73) 4 (5) 14 (17) 3 (4) 1 (1) |
- - - - |
|
| Comorbidities, n (%) | 0.041 | |||
|
None Obesity Metabolic syndrome Papillary thyroid cancer Follicular thyroid cancer Follicular adenoma |
25 (89) 2 (8) 0 0 0 1 (3) |
43 (52) 16 (19) 5 (6) 9 (11) 4 (5) 4 (5) |
4.7 [1.53-14.78] - - - - - |
|
DISCUSSION
Nearly half of all individuals with Hashimoto thyroiditis have a family history of autoimmune thyroid disease, but in our study this history was only present in 4% of included patients. Studies conducted in Denmark found a concordance of 55% in monozygotic twins compared to 3% in dizygotic twins.17 It has also been associated with certain chromosomal abnormalities, such as Down syndrome or Turner syndrome. On the other hand, some environmental factors are also believed to contribute to its aetiology, such as excessive intake of iodine, viral infections, stress, exposure to radiation and certain drugs such as amiodarone, lithium or some anticonvulsants.18
Hashimoto thyroiditis is more prevalent in female individuals, with a female-to-male ratio of approximately 2 to 10:1, and usually has onset in puberty. However, although its incidence is lower in the paediatric population, it is considered the most common cause of acquired hypothyroidism in children and adolescents, with a prevalence of 1-2%.19 The prevalence of Hashimoto thyroiditis is greater in patients with type 1 diabetes, 20% of who test positive for thyroid antibodies and 5% of who exhibit TSH elevation. It may also be present in the context of autoimmune polyglandular syndrome: it is found in 10% of patients with type 1 in association with mucocutaneous candidiasis, hypoparathyroidism and adrenal insufficiency caused by changes in the AIRE gene (autoimmune regulator), or patients with type 2 (Schmidt syndrome), in whom it tends to develop in adolescence in association with diabetes mellitus, with or without adrenal insufficiency.20
The most common symptoms of hypothyroidism are fatigue, cold intolerance, constipation, and menstrual irregularities. Children may present with pubertal delay or, in cases of severe longstanding hypothyroidism, precocious puberty. Other possible findings are bradycardia, delayed reflexes and myxoedema of the face and extremities. Hypothyroidism causes poor linear growth, and, if undiagnosed, may negatively affect the final adult height.21 However, hypothyroidism is rarely the cause of weight gain. In fact, excessive weight gain is associated with a mild elevation of thyrotropin (5 to 10 mIU/l) that normalises when the excess weight is lost.22
The laboratory findings include high levels of TSH, low levels of free thyroxine (T4) and/or presence of thyroid peroxidase (TPO) antibodies or thyroglobulin (Tg) antibodies. Although elevation of TSH is considered pathognomonic of Hashimoto thyroiditis, it is important to be aware that elevation of this marker can be secondary to other conditions, including obesity, infection and excessive iodine intake. In addition, there have been reports of patients with overt disease but normal laboratory findings.23 On the other hand, 10 to 15% of the general population tests positive for TPO antibodies in the absence of clinically significant symptoms. Due to this ambiguity, the evaluation often includes additional assessment of the thyroid by grey scale ultrasound. Historically, the characteristic appearance of Hashimoto thyroiditis on ultrasound is the presence of hypoechoic areas and a heterogenous echotexture. However, this “moth-eaten” appearance is only present in approximately a third of affected children.24
Comparing our results to the previous literature, we found a predominance of female patients, which was in agreement with previous findings, with a female-to-male ratio of 3.3:1. The mean age at diagnosis was 9.9 years, younger than reported in other studies. In a study conducted in Argentina, the female-to-male ratio was 2:1 and the mean age 11 years, while a study conducted in Turkey found a sex ratio of 6:1, and diagnosis occurring most frequently between 12 and 14 years of age.25 In 37% of patients, thyroiditis was a chance finding stemming from detection of high levels of TSH, 26 while only 24% of cases were diagnosed due to the presence of goitre, similar to the findings of previous studies.27,28
As regards the initial thyroid status of the patients, overt hypothyroidism was documented in 68% of patients at diagnosis, a high percentage compared to a study conducted in Argentina in which subclinical hypothyroidism was detected in 55% and overt hypothyroidism in 10.5%.3 This could be explained in part by a delay in diagnosis in Mexico due to a lack of access to health care services in a large proportion of the population. In Mexico, nearly 33 million inhabitants are not affiliated to any health care system.29 Another possible factor could be the low frequency of identified cases in the family compared to other studies.3,20 Hyperthyroidism was detected in only one patient, in contrast to a study conducted in Costa Rica in which 42%, nearly half of paediatric patients with Hashimoto thyroiditis, had hyperthyroidism.30 We found that the most frequent biochemical profile in the patients given a diagnosis of non-thyroidal autoimmune diseases was euthyroidism: 40% of them had normal thyroid function, compared to overt hypothyroidism in 80% of patients who did not have non-thyroidal autoimmune diseases (p <0.001). A study conducted in Italy in more than 500 patients found a normal thyroid status in 69% of patients who had a non-thyroidal autoimmune comorbidity.31
As regards the comorbidities found in patients with chronic lymphocytic thyroiditis, the most frequent one was type 1 diabetes, in 18% of patients, followed by obesity in 15%, thyroid cancer in 8% and vitiligo in 5%. Approximately 45% of the patients did not have any known comorbidity, autoimmune or not.
In our study, nearly half of male patients had a second autoimmune disease, while this was only the case in one fifth of female patients, a difference that was statistically significant with a p-value of 0.02. This could be related to the fact that in school-aged children and adolescence, the prevalence of autoimmune diseases tends to be greater in the male sex, contrary to the trend observed in the adult age group.31
CONCLUSION
Paediatric patients with Hashimoto thyroiditis are at high risk of having non-thyroid autoimmune disease, chiefly type 1 diabetes mellitus. It is important for clinicians to be knowledgeable of these diseases and detect them in a timely manner, as early treatment of both diseases will improve their control and the health of the patient. A majority of patients with associated non-thyroidal autoimmune disease had normal thyroid gland function at the time of diagnosis of Hashimoto thyroiditis. We found that in the paediatric age group, male patients were at higher risk of developing non-thyroidal autoimmune disease.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article. The study did not receive any form of funding.
AUTHORSHIP
Author contributions: study conception and design (ALBG, HEAC), data collection (ALBG), data analysis and interpretation (ALBG, HEAC), manuscript draft (ALBG, SEB, HEAC, SGF). All authors reviewed the results and approved the final version of the manuscript.
ABBREVIATIONS
CAT: chronic autoimmune thyroiditis · Tg: thyroglobulin · TPO: thyroid peroxidase · TSH: thyroid stimulating hormone · T4: thyroxine
REFERENCES
- Hanley P, Lord K, Bauer AJ. Thyroid disorders in children and adolescents. JAMA Pediatr. 2016;170(10):1008-19.
- Cappa M, Bizzarri C, Crea F. Autoimmune thyroid diseases in children. J Thyroid Res. 2010;2011:675-703.
- Gómez E, Nso Roca AP, Juste M, Cortés E. Enfermedad de Hashimoto en una cohorte de 29 niños y adolescentes. Epidemiología, evolución y comorbilidad a corto y largo plazo. Arch Argent Pediatr. 2018;116(1):56-8.
- Korzeniowska K, Ramotowska A, Szypowska A, Szadkowska A, Fendler W, Kalina Faska B, et al. How does autoimmune thyroiditis in children with type 1 diabetes mellitus influence glycemic control, lipid profile and thyroid volume? J Pediatr Endocrinol Metab. 2015;28(3-4):275-8.
- Bárová H, Perusicová J, Hill M, Sterzl I, Vondra K, Masek Z. Anti-GAD-positive patients with type 1 diabetes mellitus have higher prevalence of autoimmune thyroiditis than anti-GAD-negative patients with type 1 and type 2 diabetes mellitus. Physiol Res. 2004;53(3):279-86.
- Husby S, Koletzko S, Korponay Szabó IR, Mearin ML. Phillips A, Shamir R. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. 2012;54(1):136-60.
- Fallahi P, Elia G, Ragusa F, Ruffilli I, Camastra S, Giusti C, et al. The aggregation between AITD with rheumatologic, or dermatologic, autoimmune diseases. Best Pract Res Clin Endocrinol Metab. 2019;33(6):101372.
- Liu M, Murphy E, Amerson EH. Rethinking screening for thyroid autoimmunity in vitiligo. J Am Acad Dermatol. 2016;75(6):1278-80.
- Merino Muñoz R, Remesal Camba A, Murias Loza S. Lupus eritematoso sistémico. An Pediatr Contin. 2013;11(2):89-97.
- Klionsky J, Antonelli M. Thyroid disease in lupus: an updated review. ACR Open Rheumatol. 2020;2(2):74-8.
- Brenta G, Fretes O. Dyslipidemias and hypothyroidism. Pediatr Endocrinol Rev. 2014;11(4):390-9.
- Nishi M. Diabetes mellitus and thyroid diseases. Diabetol Int. 2018;9(2):108-12.
- Saranac l, Zivanovic S, Bjelakovic B, Stamenkovic H, Novak M, Kamenov B. Why is the thyroid so prone to autoimmune disease? Horm Res Paediatr. 2011;75(3):157-65.
- Chang YC, Hua SC, Chang CH, Kao WY, Lee HL, Chuang LM, et al. High TSH level within Normal Range Is Associated with Obesity, Dyslipidemia, Hypertension, Inflammation, hypercoagulability, and the metabolic syndrome: a novel cardiometabolic marker. J Clin Med. 2019;8(6):817.
- Silva de Morais N, Stuart J, Guan H, Wang Z, Cibas ES, Frates MC, et al. The impact of Hashimoto Thyroiditis on thyroid nodule cytology and risk of thyroid cancer. J Endocr Soc. 2019;3(4):791-800.
- Paulson V, Rudzinski ER, Hawkins DS. Thyroid cancer in the pediatric population. Genes (Basel). 2018;10(9):723.
- Brix TH, Hegedüs l, Gardas A, Banga JP, Nielsen CH. Monozygotic twin pairs discordant for Hashimoto's thyroiditis share a high proportion of thyroid peroxidase autoantibodies to the immunodominant region A. Further evidence for genetic transmission of epitopic 'fingerprints'. Autoimmunity. 2011;44(3):188-94.
- Duntas LH. Environmental factors and autoimmune thyroiditis. Nat Clin Pract Endocrinol Metab. 2008;4:454-60.
- Casto C, Pepe G, Li Pomi A, Corica D, Aversa T, Wasniewska M. Hashimoto's thyroiditis and Graves' disease in genetic syndromes in pediatric age. Genes (Basel). 2021;12(2):222.
- Núñez Almache O, Del Aguila Villar C, Chávez E, Espinoza O, Pinto P, Calagua M, et al. Progresión clínica de la tiroiditis autoinmune en niños y adolescentes atendidos en el Instituto Nacional de Salud del Niño. An Fac Med. 2015;76(4):325-31.
- Hanley P, Lord K, Bauer AJ. Thyroid disorders in children and adolescents: a review. JAMA Pediatr. 2016;170(10):1008-19.
- Pacifico l, Anania C, Ferraro F, Andreoli GM, Chiesa C. Thyroid function in childhood obesity and metabolic comorbidity. Clin Chim Acta. 2012;413(3- 4):396-405.
- Mincer DL, Jialal I: Hashimoto thyroiditis. In: StatPearls. Treasure Island, FL; 2023 [online] [accessed 11/04/2023]. Available at www.ncbi.nlm.nih.gov/books/NBK459262/
- Decker T, Schnittka E, Stolzenberg l, Yalowitz J. Shear-Wave Elastography for the Diagnosis of Pediatric Hashimoto's Thyroiditis: A systematic review and meta-analysis. Cureus. 2023;15(2):e35490.
- Dündar B, Boyaci A, Sangün O, Dündar N. Hashimoto thyroiditis in children and adolescents: evaluation of clinical and laboratory findings. Turk Arch Ped. 2011;46:309-13.
- Crisafulli G, Gallizzi R, Aversa T, Salzano G, Valenzise M, Wasniewska M, et al. Thyroid function test evolution in children with Hashimoto's thyroiditis is closely conditioned by the biochemical picture at diagnosis. Ital J Pediatr. 2018;44(1):22.
- De Luca F, Santucci S, Corica D, Pitrolo E, Romeo M, Aversa T. Hashimoto's thyroiditis in childhood: presentation modes and evolution over time. Ital J Pediatr. 2013;39:8.
- Tang S, Yang M, Zhang D, Tong YJ, Xin Y. Clinical characteristics and follow-up of 19 children with Hashimoto's thyroiditis aged below 3 years: a single-center retrospective analysis. Front Endocrinol (Lausanne). 2021;12:737527.
- Censo de Población y Vivienda. 2020 [online] [accessed 11/04/2023]. Available at www.inegi.org.mx/contenidos/programas/ccpv/2020/doc/Censo2020_Principales_resultados_EUM.pdf
- Acevedo G, Mejía J, Gil M, Astudillo E, Gómez J, Valencia A, et al. Características clínicas y paraclínicas de pacientes pediátricos con tiroiditis autoinmune en una institución especializada de Cali, Colombia. Rev Méd Univ Costa Rica. 2020;14(2):13-22.
- Ruggeri RM, Trimarchi F, Giuffrida G, Certo R, Cama E, Campennì A, et al. Autoimmune comorbidities in Hashimoto’s thyroiditis: different patterns of association in adulthood and childhood/adolescence. Eur J Endocrinol. 2017;176(2):133-41.