
Vol. 25 - Num. 98
Original Papers
Short lingual frenulum: results of an intervention to improve continuity of care
Sara Monserrat Proaño Landazuria, Jesús Vicente Redondo Sedanoa, M.ª Eunate Martí Carrerab, M.ª Rosario Azcutia Gómezc, Andrés Gómez Frailea, M.ª Dolores Delgado Muñoza
aServicio de Cirugía Pediátrica. Hospital Universitario 12 de Octubre. Madrid. España.
bServicio de Cirugía Plástica. Hospital Universitario 12 de Octubre. Madrid. España.
cDirección Continuidad Asistencial. Hospital Universitario 12 de Octubre. Madrid. España.
Correspondence: JV Redondo. E-mail: jesusredondosedano@gmail.com
Reference of this article: Proaño Landazuri SM, Redondo Sedano JV, Martí Carrera ME, Azcutia Gómez MR, Gómez Fraile A, Delgado Muñoz MD. Short lingual frenulum: results of an intervention to improve continuity of care . Rev Pediatr Aten Primaria. 2023;25:131-5.
Published in Internet: 26-04-2023 - Visits: 16715
Abstract
Introduction: we created an informative triptych about short lingual frenulum/ ankyloglossia (SLF/A) to avoid discrepancy in the referral criteria of patients to the pediatric plastic surgery consultation from primary care (PC). The main objective is to analyze the impact of this intervention on the referrals to specialized care (SC).
Material and methods: the information was sent to the primary care professionals attached to the health area of our hospital. We performed a retrospective analysis of the referrals to SC in the 2 years prior sending the information. We compared these results with the prospective analysis of the consultations attended in the year after sending the triptych.
Results: we analyzed 874 consultations. 59.6% of them were attended prior sending the information. 61.9% of the referrals adjusted to the proposed criteria for lingual frenotomy, observing a significant reduction in the wrongly referred patients between the compared periods of time (41.8% vs 32.6%). We also found a significant reduction in the number of patients with no functional problem associated to the SLF (34.4% vs 23.3%).
Conclusions: our informative triptych about SLF/ ankyloglossia has adjusted referrals from PC to the proposed criteria for lingual frenotomy in our hospital.
Keywords
● Ankiloglossia ● Care continuity ● Lingual frenotomy ● Short lingual frenulumINTRODUCTION
Lingual frenulum (LF) complaints have become one of the most frequent reasons for consultation in the Paediatric Plastic Surgery Unit (PPSU) of the Hospital 12 de Octubre (Madrid, Spain). This fact is consistent with the tendency toward overdiagnosis noted by several publications in recent years, and is not supported by the clinical evidence currently available on the subject.1,2
In our case, the increase in the number of evaluated patients was associated with an increase in the frequency of referral from primary care (PC). However, in many cases the criteria for referral to surgical services differ from the criteria applied in the unit to determine the indication of frenotomy, which compromises continuity of care and the quality of care perceived by referred parties.3,4
In an attempt to homogenize the information provided at different levels of care, the PPSU team developed an informational trifold brochure summarising the current scientific evidence on the health problems associated with a short lingual frenulum (SLF) and specifying the criteria applied in our unit for the performance of frenotomy.
The primary objective of our study was to analyse the referrals to our related to SFL/ankyloglossia (SLF/A) made from the PC level, and the subsequent management of the patient at the specialty care (SC) level. We also assessed the impact of the distribution of the informational brochure on the quality of subsequent referrals.
MATERIAL AND METHODS
Health education contents were disseminated in the form of a trifold brochure that focused on the following aspects:
- Difference between short lingual frenulum and ankyloglossia.
- Functional limitations associated with ankyloglossia.
- Type of surgical treatment offered and description of surgical procedures.
- Indications for surgical intervention (frenotomy). Based on the current evidence, the criteria applied to determine eligibility for surgical intervention were:
- Patient aged less than 4 months with SLF and breastfeeding difficulties that do not improve with conservative management.4,5 In this case, frenotomy is performed at the office without general anaesthesia.1,6
- Patient aged more than 4 years with SLF and speech articulation problems, preferably with a previous evaluation by a speech therapist. Frenotomy is performed in the surgical theatre under sedation.7
- Patient of any age with SLF and oral/dental health problems, such as difficulty cleaning the mouth and teeth or placing orthodontic devices.8
The contents and wording of the brochure were reviewed by the Quality Assurance unit of the hospital. The trifold brochure was distributed among PC professionals in centres within the catchment area of our hospital with the collaboration of the Care Continuity Team of our hospital.
To assess the concordance of the criteria for referral to SC from PC with the criteria proposed by professionals in the PPSU, we conducted a retrospective review of the consultations related to SLF/A by patients referred from PC managed in the 2 years preceding the dissemination of the educational brochure (period A). We compared the resulting data with the same information, collected prospectively, on the consultations made the year following the distribution of the informational brochure (period B).
The following were considered referral criteria that did not fit the indications proposed by the PPSU: patients with functional impairment without evident SLF; patients with SLF without associated functional impairment; patients with breastfeeding difficulties aged more than 4 months or infants aged less than 4 months who were not breastfed; and patients with pronunciation problems aged less than 3.5 years and/or those in whom the speech impairment occurred in the context of a broader language delay that had not been assessed by the pertinent specialists.
The statistical analysis was conducted with the statistical software package SPSS. Due to the nature of the study, it was not necessary to obtain informed consent.
RESULTS
We analysed 874 appointments. Of this total, 521 (59.6%) corresponded to period A and 353 (40.4%) to period B. The mean age at the time of referral to SC was 25.5 ± 36 meses. Referrals were made by the PC physician in 95.5% cases (835).
Overall, the referrals conformed to the criteria proposed by the PPSU in 541 patients (61.9%). Thus, inappropriate referrals corresponded to 38.1% of the total (333 appointments). Comparing both periods, we found a 9.2% decrease in the referrals that did not match the criteria proposed by the PPSU (41.8% in period A vs. 32.6% in period B), a difference that was statistically significant (p = 0.006).
The distribution of the inappropriate reasons for referral was the following: 261 (78.4%) patients had SLF, but no associated functional impairment; 37 (11.1%) children were referred due to speech articulation problems, but it was before the age frenotomy would be indicated or the problem was associated with a language delay that had yet to be assessed by other specialists; 35 (10.5%) were infants referred due to breastfeeding problems after age 4 months or who did not breastfeed at all; and 4 (1.2%) patients were not found to have a SLF on examination.
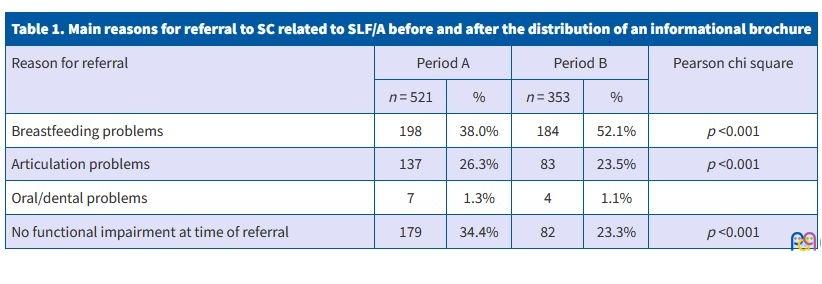
Breastfeeding problems were the most frequent reason for referral (382 cases; 43.7%), followed by patients with SLF that was not associated with functional impairment at the time of assessment in SC (261 cases; 29.9%) and patients with speech articulation problems (220 patients; 25.2%). Table 1 presents the distribution of patients by the reason for referral to SC in each of the periods under study. The results show a statistically significant reduction in the referral of patients without functional impairment associated with SLF (34.4% in period A vs. 23.3% in period B).
| Table 1. Main reasons for referral to SC related to SLF/A before and after the distribution of an informational brochure | |||||
|---|---|---|---|---|---|
| Reason for referral | Period A | Period B | Pearson chi square | ||
| n = 521 | % | n = 353 | % | ||
| Breastfeeding problems | 198 | 38.0% | 184 | 52.1% | p <0.001 |
| Articulation problems | 137 | 26.3% | 83 | 23.5% | p <0.001 |
| Oral/dental problems | 7 | 1.3% | 4 | 1.1% | |
| No functional impairment at time of referral | 179 | 34.4% | 82 | 23.3% | p <0.001 |
There were 653 patients (74.7%) who underwent surgical intervention. Out of this total, 116 (17.8%) did not meet the criteria for surgical intervention established in the protocol proposed by the PPSU. The most frequent types of patient in this subset were infants who had no latching problems (86; 74.2%) and patients in whom frenotomy was performed taking advantage of another surgery (22; 19%). Out of the percentage of operated patients, 45.5% were operated in period A and 18.5% in period B, with a statistically significant decrease in the latter (p <0.001).
DISCUSSION
The interest in health problems associated with SLF has increased significantly in the past decade. 1,4 In spite of it, there is significant controversy regarding the functional limitations associated with it and considerable heterogeneity in the diagnosis and treatment protocols applied by health care professionals.3,5,7-10 This is most pronounced between the different levels of care and calls for the development of strategies to facilitate continuity of care.
The perceived discrepancies between the criteria for treatment applied at the PPSU and the referrals from PC related to SFL motivated the development of an informational brochure to standardise management within our health care area. The key concept was the distinction between the anatomical feature and functional impairment, that is, between SLF and ankyloglossia, as the indications of surgery are based on the presence of symptoms as opposed to abnormal morphology.1,6
In this regard, the dissemination of the trifold brochure achieved a significant reduction in the number of patients without evident functional limitation associated to SLF referred to our unit. The reduction of this type of referrals was one of our main goals, as the decision not to perform surgery often went against the expectations of the caregivers in bringing the child to the unit.
In most cases, these referrals were made with the notion that frenotomy could be a prophylactic measure against the future development of articulation problems. We ought to highlight that the literature on the subject does not support this indication, first, because it is difficult to predict which patients with SLF will go on to develop speech problems, and secondly, because the main complication of frenotomy performed at an early age is the recurrence of tongue tie, so that surgery could actually create a problem that the patient may not have experienced otherwise.2,3,8
As regards speech difficulties, it is important to consider certain aspects before referring the patient to SC: age (speech articulation matures at around 3.5-4 years), ethnicity and socio-educational environment, the co-occurrence of a developmental language disorder (in which case, the initial approach should be to carry out an appropriate evaluation of the patient, so that frenotomy would not be the first step to take) and the possibility of having the patient evaluated by a speech therapist first.2
When it comes to breastfeeding, the main reason for referral, the symptoms that improves most significantly after frenotomy is nipple pain with latching. Breastfeeding is a multifactorial process (positioning, maternal experience, shape of baby’s mouth, nipple anatomy, etc), and therefore it is important that all these aspects be assessed by an experienced lactation consultant before planning the surgery, as the latter may not resolve the problem.1,4,6
In recent years, new functional deficits have been associated with SLF. They include swallowing problems, palate/mandible deformity or obstructive sleep apnoea. The current evidence does not show a consistent association, so caution must be exerted regarding the recommendation of frenotomy in relation to these problems and the information that is given to parents at the primary care level.2,5,7
Lastly, analysing the management in clinical practice, we found that a large number of patients had undergone surgery for indications that may not have been appropriate based on the protocol proposed by the clinicians of the unit. which the indication of surgery was not clear based on the protocol had undergone frenotomy. Authors agree that in most cases inappropriate surgical intervention involves performance of frenotomy in infants without breastfeeding difficulties, in whom the relative simplicity of the procedure contributes to the inclination to perform the surgery. The decrease in the relative frequency of inappropriate interventions between the 2 study periods suggests an attitude shift toward greater adherence to the proposed protocol and caution not to convey contradictory messages.
CONCLUSION
The diffusion of an informational trifold brochure on SLF/A was associated with changes in the patterns of referral from PC to the proposed criteria for frenotomy in the PIMCU of our hospital. High-quality prospective studies are required to establish diagnosis and treatment protocols for the management of SLF/A at different levels of care.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article. The study did not require any form of external funding. Partial results of the study were presented at the LIX Congress of the Sociedad de Cirugía Pediátrica (Paediatric Surgery Society), held in Porto, Portugal, in May 2022. The results presented in this article complement those presented at the congress.
AUTHORSHIP
Author contributions: study design, data collection and manuscript writing (SMPL), research team coordination, study design, writing of manuscript and informational trifold brochure and critical revision of the manuscript draft (JVRS), study design, writing of manuscript and informational trifold brochure and critical revision of manuscript draft (MEMC, MDDM), revision of the manuscript and informational brochure drafts, distribution of the informational brochure among primary care professionals (MRAG), critical revision of manuscript draft (AGF).
ABBREVIATIONS
LF: lingual frenulum · PC: primary care · PPSU: paediatric plastic surgery unit · SC: specialty care · SLF/A: short lingual frenulum/ankyloglossia.
REFERENCES
- Costa Romero M, Esinola Docio M, Paricio Talayero JM, Díaz Gómez NM. Ankyloglossia in breastfeeding infants. An update. Arch Argent Pediatr. 2021;119:e600-e609.
- Salt H, Claessen M, Johnston T, Smart S. Speech production in young children with tongue-tie. Int J Pediatr Otorhinolaryngol. 2020;134:110035.
- Walsh J, Tunkel D. Diagnosis and Treatment of Ankyloglossia in Newborns and Infants: A Review. JAMA Otolaryngol Neck Surg. 2017;143:1032.
- Hill R. Implications of Ankyloglossia on Breastfeeding. MCN Am J Matern Nurs. 2019;44:73-9.
- Messner AH, Walsh J, Rosenfeld RM, Schwartz SR, Ishman SL, Baldassari C, et al. Clinical Consensus Statement: Ankyloglossia in Children. Otolaryngol Neck Surg. 2020;162:597-611.
- Colombari GC, Mariusso MR, Ercolin LT, Mazzoleni S, Stellini E, Ludovichetti FS. Relationship between Breastfeeding Difficulties, Ankyloglossia, and Frenotomy: A Literature Review. J Contemp Dent Pract. 2021;22:452-61.
- Calvo-Henríquez C, Neves SM, Branco AM, Lechien JR, Reinoso FB, Rojas XM, et al. Relationship between short lingual frenulum and malocclusion. A multicentre study. Acta Otorrinolaringol Esp. 2022;73:177-83.
- Frenectomy for the Correction of Ankyloglossia: A Review of Clinical Effectiveness and Guidelines [online]. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2016 Jun 15. PMID: 27403491.
- Barberá Pérez PM, Sierra Colomina M, Deyanova Alyosheva N, Plana-Fernández M, Lalaguna Mallada P. Prevalence of ankyloglossia in newborns and impact of frenotomy in a Baby-Friendly Hospital. Bol Méd Hosp Infant México. 2021;78:6405.
- González Jiménez D, Costa Romero M, Riaño Galán I, González Martínez MT, Rodríguez Pando MC, Lobete Prieto C. Prevalencia de anquiloglosia en recién nacidos en el Principado de Asturias. An Pediatr (Barc). 2014;81:115-9.