
Vol. 24 - Num. 95
Original Papers
Sensitivity of the Panbio COVID-19 rapid antigen detection test in primary care
Ana M.ª Alonso Rubioa, Mercedes Garrido Redondob, M.ª Rosario Bachiller Luquec, M.ª Luisa Vega Gutiérrezc, Cristina García de Riverad, Beatriz Liras Muñoze, Teresa Palencia Ercillaf, Mónica Sanz Fernándezg, M.ª Jesús Alonso Ballesterosh, M.ª Fe Muñoz Morenoi, Paula Borregón Garridoj
aPediatra. CS Covaresa-Parque Alameda. Valladolid. España.
bPediatra. CS La Tórtola. Valladolid. España.
cPediatra. CS Pilarica. Valladolid. España.
dPediatra. CS Rondilla. Valladolid. España.
ePediatra. CS Cuéllar. Cuellar. Segovia. España.
fPediatra. CS Cuellar. Cuellar. Segovia. España.
gPediatra. CS Pisuerga. Arroyo de la Encomienda. Valladolid. España.
hPediatra. CS Medina del Campo. Valladolid. España.
iPediatra. Unidad de Apoyo a la Investigación. Hospital Clínico Universitario. Valladolid. España.
jEstudiante de Medicina. Facultad de Medicina. Universidad de Valladolid. Valladollid. España.
Correspondence: AM Alonso . E-mail: alonsoam04@hotmail.com
Reference of this article: Alonso Rubio AM, Garrido Redondo M, Bachiller Luque MR, Vega Gutiérrez ML, García de Rivera C, Liras Muñoz B, et al. Sensitivity of the Panbio COVID-19 rapid antigen detection test in primary care . Rev Pediatr Aten Primaria. 2022;24:e283-e289.
Published in Internet: 21-09-2022 - Visits: 12234
Abstract
Introduction and objectives: primary care paediatricians need reliable rapid diagnostic techniques (RDTs) to prevent the spread of coronavirus disease 19 (COVID-19) through early and effective screening while awaiting a vaccine. The objective of this study was to evaluate the sensitivity (Sen) of the Abbott laboratory SARS-CoV-2 Panbio antigen test, newly introduced in primary care, in both adults and children (symptomatic and asymptomatic contacts) in comparison to the polymerase chain reaction (PCR) test.
Sample and methods: the study included 591 patients (222 aged less than 14 years) from 7 primary care centres; of who 249 were symptomatic and 342 asymptomatic contacts. We calculated the Sen and specificity (Spe) with their 95% confidence intervals (CIs). We assessed the independence of the two results with the McNemar test.
Results: the Sen of the test within 5 days from onset was 81% in adults (95% CI, 66.16-96.34) and 80% in children (95% CI: 34.94-100). In contacts, we assessed the Sen within 5 days, in adults (68%; 95% CI: 51.13- 86.37), in 5 to 9 days (85%) and in children (66%; 95% CI: 30.31-100). The most frequent source of exposure were household contacts (52% of the cases). The Spe was 100% in every case.
Conclusions: the Panbio SARS-CoV-2 rapid antigen test can be useful for diagnosis in adults and children within 5 days of onset, and from days 5 to 9 in contacts of confirmed COVID 19 cases. Further studies are required for adequate interpretation of the latter result.
Keywords
● COVID-19 ● Point-of-care diagnostics ● Primary care ● SARS-CoV-2INTRODUCTION
Early diagnosis of coronavirus disease 2019 (COVID-19) at the primary care level is important to prevent the spread of the SARS-CoV-2 virus through early and effective screening followed by quasi-immediate isolation. To achieve this goal, we need reliable rapid diagnostic tests (RDTs).1-4 The aim of this study was to assess the sensitivity (Sen) of the Panbio COVID-19 antigen test (Abbott Diagnostic GmbH, Jena, Germany), an immunochromatography assay, upon its introduction in primary care centres within a few days of the onset of symptoms or exposure to a positive case compared to in-hospital testing with polymerase chain reaction (PCR) in both children and adults. Several studies have found that antigen test results correlate more strongly to PCR than viral culture, which would make the infection more probable.5,6
MATERIAL AND METHODS
Participants
Seven primary care centres in the provinces of Valladolid and Segovia (Spain) participated in the study in October and November of 2020. The study included patients with symptoms compatible with COVID-19 and asymptomatic contacts for whom a PCR test had been ordered. We excluded samples if the results were inconclusive, there were problems during their collection or if the patient had a known history of positive PCR test (2%) or positive IgG antibody test (7.8%). Out of the total 591 included patients, 249 had symptoms compatible with COVID-19 and 342 were asymptomatic contacts of a positive case.
In the sample under study, 55.9% of patients were female, and 222 patients were aged less than 14 years (mean age 6.69 years; standard deviation [SD] 3.9).
Previously trained paediatricians and nurses obtained 2 nasopharyngeal swab samples for each patient. One of the samples was used on the spot to perform the Abbot Panbio COVID-19 antigen test following the directions of the manufacturer, obtaining the results within 15 minutes; the second swab was placed in universal transport medium for viruses (Deltalab, MDD, CE 0318, Spain) to undergo PCR testing (Cobas® SARS-CoV-2 test for use in Cobas® 6800/8800 Systems) within 24 hours in the Department of Microbiology of the corresponding referral hospital (Hospital Clínico de Valladolid, Hospital del Río Hortega, Hospital de Segovia).
The study was approved by the Scientific Research and Ethics Committee of the Regional Health Care Administration. All patients invited to participate accepted voluntarily, providing informed consent and, in the case of minors, with obtention of consent from a parent or legal guardian.
The reagents were provided by the Regional Health Care Administration of Castilla y León. There were no conflicts of interest involving the pharmaceutical industry.
Statistical analysis
We have expressed quantitative variables as mean and standard deviation (SD) and qualitative variables as frequency distributions.
Based on antigen and PCR test results, we calculated the Sen and specificity (Spe) of the test with the corresponding 95% confidence intervals (CIs). We assessed the independence of both results with the McNemar test.
The analysis was carried out with the statistical package IBM SPSS Statistics version 24.0 for Windows and Epidat version 3.1. We considered p-values of less than 0.05 statistically significant.
RESULTS
In the total sample (n = 591), there were 59 positive antigen tests (10%) and 89 positive PCR tests (15%) at a time that the prevalence of COVID-19 in the population of Castilla y León was 10%.
Analysis of symptomatic patients
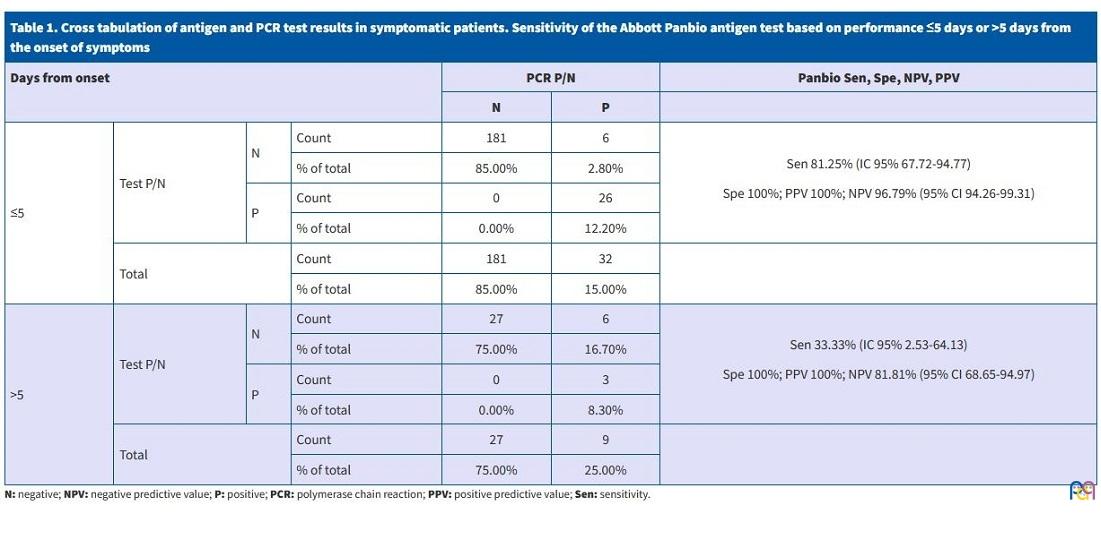
The analysis included 249 patients with symptoms compatible with COVID-19. In this group, we found an overall Sen of 68% (95% CI: 53.28-83.08) and an overall Spe of 100%. However, in a separate analysis, in the group tested within 5 days of onset (n = 213) the Sen was 81% (95% CI: 66.16-96.34) and the Spe 100%, while in the group tested more than 5 days after the onset (n = 36) the Sen decreased to 33% (95% CI: 0.00-69.69), while the Spe continued to be 100% (Table 1).
| Table 1. Cross tabulation of antigen and PCR test results in symptomatic patients. Sensitivity of the Abbott Panbio antigen test based on performance ≤5 days or >5 days from the onset of symptoms | ||||||
|---|---|---|---|---|---|---|
| Days from onset | PCR P/N | Panbio Sen, Spe, NPV, PPV | ||||
| N | P | |||||
| ≤5 | Test P/N | N | Count | 181 | 6 |
Sen 81.25% (IC 95% 67.72-94.77) Spe 100%; PPV 100%; NPV 96.79% (95% CI 94.26-99.31) |
| % of total | 85.00% | 2.80% | ||||
| P | Count | 0 | 26 | |||
| % of total | 0.00% | 12.20% | ||||
| Total | Count | 181 | 32 | |||
| % of total | 85.00% | 15.00% | ||||
| >5 | Test P/N | N | Count | 27 | 6 |
Sen 33.33% (IC 95% 2.53-64.13) Spe 100%; PPV 100%; NPV 81.81% (95% CI 68.65-94.97) |
| % of total | 75.00% | 16.70% | ||||
| P | Count | 0 | 3 | |||
| % of total | 0.00% | 8.30% | ||||
| Total | Count | 27 | 9 | |||
| % of total | 75.00% | 25.00% | ||||
Analysis of contacts
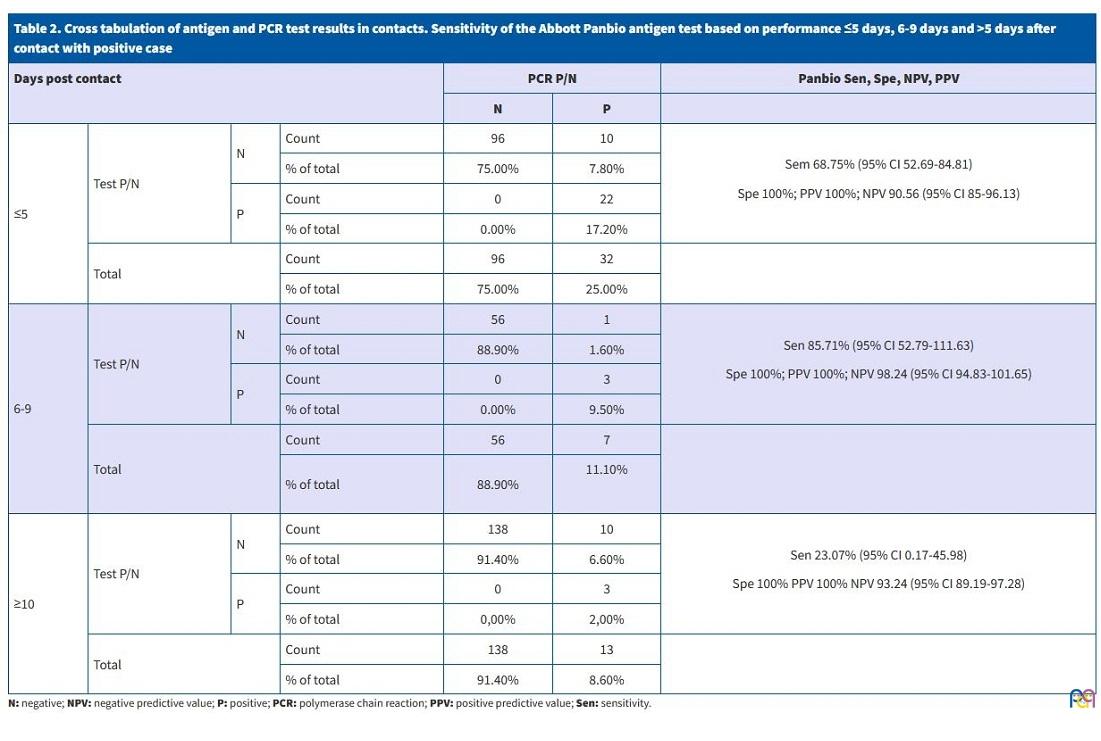
In the testing of contacts (n = 342), the overall Spe of the antigen test was 60% (95% CI: 46.40-75.16) and the overall Spe was 100%, while in the separate analysis we found that for tests performed between days 6 and 9 after the last exposure to the positive contact, the Sen increased to 85% (95% CI: 52.65-100.00) and the Spe was 100%, compared to a Sen of 68% (95% CI: 51.13-86.37) and a Spe of 100% in those tested within 5 days of exposure (Table 2).
| Table 2. Cross tabulation of antigen and PCR test results in contacts. Sensitivity of the Abbott Panbio antigen test based on performance ≤5 days, 6-9 days and >5 days after contact with positive case | ||||||
|---|---|---|---|---|---|---|
| Days post contact | PCR P/N | Panbio Sen, Spe, NPV, PPV | ||||
| N | P | |||||
| ≤5 | Test P/N | N | Count | 96 | 10 |
Sem 68.75% (95% CI 52.69-84.81) Spe 100%; PPV 100%; NPV 90.56 (95% CI 85-96.13) |
| % of total | 75.00% | 7.80% | ||||
| P | Count | 0 | 22 | |||
| % of total | 0.00% | 17.20% | ||||
| Total | Count | 96 | 32 | |||
| % of total | 75.00% | 25.00% | ||||
| 6-9 | Test P/N | N | Count | 56 | 1 |
Sen 85.71% (95% CI 52.79-111.63) Spe 100%; PPV 100%; NPV 98.24 (95% CI 94.83-101.65) |
| % of total | 88.90% | 1.60% | ||||
| P | Count | 0 | 3 | |||
| % of total | 0.00% | 9.50% | ||||
| Total | Count | 56 | 7 | |||
| % of total | 88.90% | 11.10%
|
||||
| ≥10 | Test P/N | N | Count | 138 | 10 |
Sen 23.07% (95% CI 0.17-45.98) Spe 100% PPV 100% NPV 93.24 (95% CI 89.19-97.28) |
| % of total | 91.40% | 6.60% | ||||
| P | Count | 0 | 3 | |||
| % of total | 0,00% | 2,00% | ||||
| Total | Count | 138 | 13 | |||
| % of total | 91.40% | 8.60% | ||||
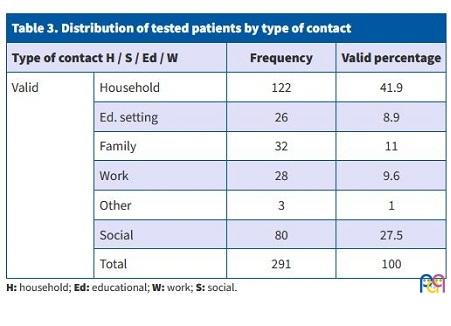
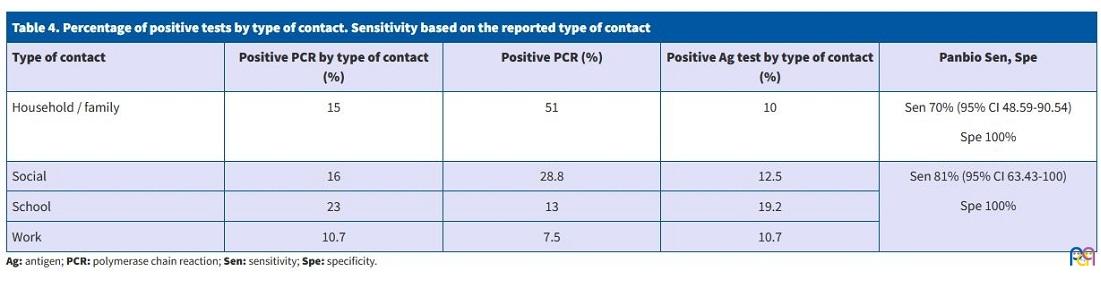
The highest percentage of studied contacts had been exposed in the home (n = 41.9%) followed by other forms of social contact (n = 27.5%) (Table 3). The Sen of the antigen test in cases of exposure to household and family members was 70% (95% CI: 48.59-90.54), with a Spe of 100% (Table 4).
| Table 3. Distribution of tested patients by type of contact | |||
|---|---|---|---|
| Type of contact H / S / Ed / W | Frequency | Valid percentage | |
| Valid | Household | 122 | 41.9 |
| Ed. setting | 26 | 8.9 | |
| Family | 32 | 11 | |
| Work | 28 | 9.6 | |
| Other | 3 | 1 | |
| Social | 80 | 27.5 | |
| Total | 291 | 100 | |
| Table 4. Percentage of positive tests by type of contact. Sensitivity based on the reported type of contact | ||||
|---|---|---|---|---|
| Type of contact | Positive PCR by type of contact (%) | Positive PCR (%) | Positive Ag test by type of contact (%) | Panbio Sen, Spe |
| Household / family | 15 | 51 | 10 |
Sen 70% (95% CI 48.59-90.54) Spe 100% |
| Social | 16 | 28.8 | 12.5 |
Sen 81% (95% CI 63.43-100) Spe 100% |
| School | 23 | 13 | 19.2 | |
| Work | 10.7 | 7.5 | 10.7 | |
Analysis in children under 14 years
In the total sample (n = 591), 222 patients were aged less than 14 years; the mean age was 6.69 years (DE 3.9), 54.5 % of the patients were female, 122 symptomatic and 100 contacts of positive cases.
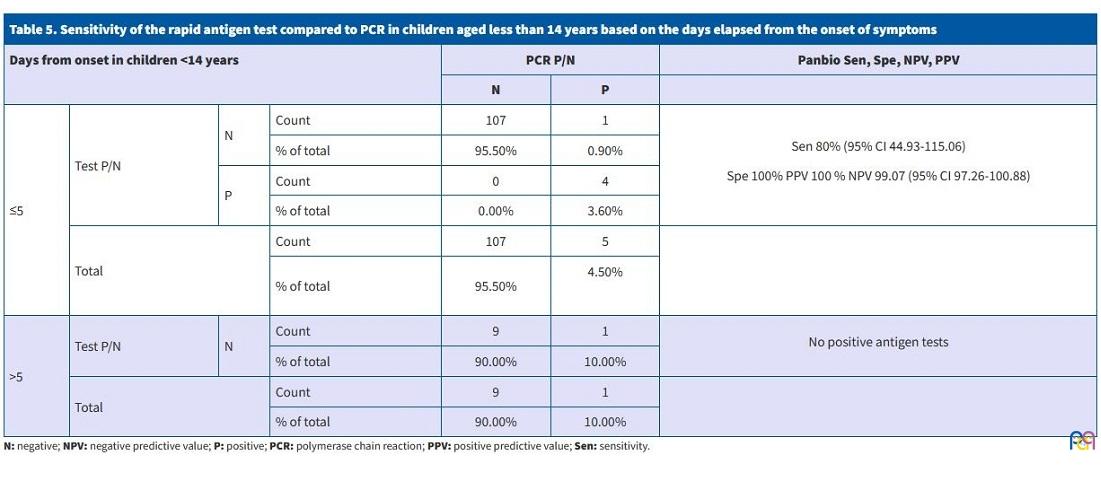
The Sen of the Panbio antigen tests in children under 14 years within 5 days of the onset of symptoms was 80% (95% CI: 34.94-100) and the Spe was 100%. Of those tested more than 5 days after the onset, only 1 child had a positive PCR test of the 10 that had a negative result in the antigen test (Table 5).
| Table 5. Sensitivity of the rapid antigen test compared to PCR in children aged less than 14 years based on the days elapsed from the onset of symptoms | ||||||
|---|---|---|---|---|---|---|
| Days from onset in children <14 years | PCR P/N | Panbio Sen, Spe, NPV, PPV | ||||
| N | P | |||||
| ≤5 | Test P/N | N | Count | 107 | 1 |
Sen 80% (95% CI 44.93-115.06) Spe 100% PPV 100 % NPV 99.07 (95% CI 97.26-100.88) |
| % of total | 95.50% | 0.90% | ||||
| P | Count | 0 | 4 | |||
| % of total | 0.00% | 3.60% | ||||
| Total | Count | 107 | 5 | |||
| % of total | 95.50% | 4.50%
|
||||
| >5 | Test P/N | N | Count | 9 | 1 |
No positive antigen tests |
| % of total | 90.00% | 10.00% | ||||
| Total | Count | 9 | 1 | |||
| % of total | 90.00% | 10.00% | ||||
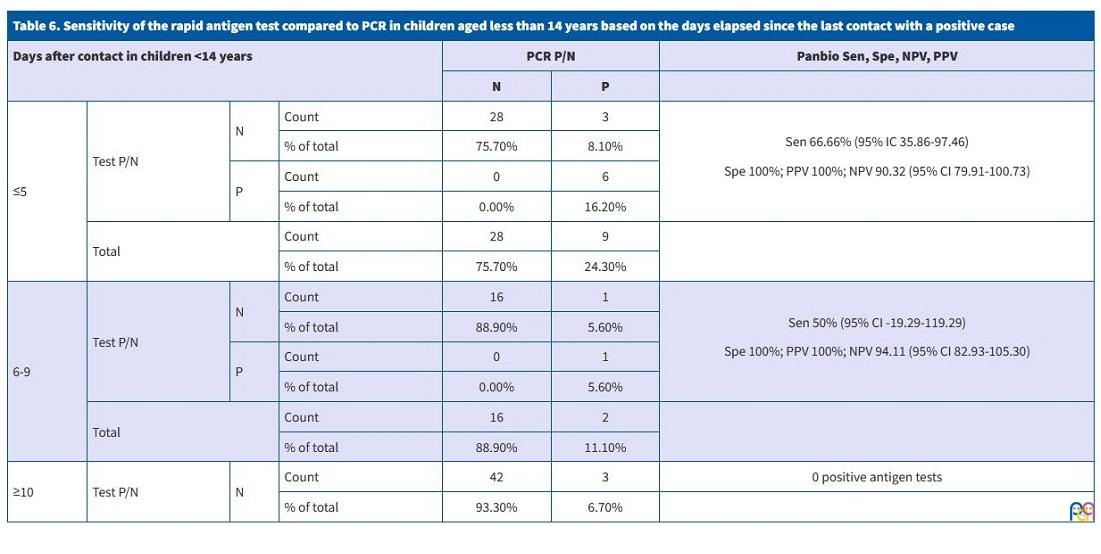
When it came to exposed contacts, the Sen of the antigen test in children tested within 5 days after the last exposure (37%) was 66% (95% CI: 30.3-100), with a Spe of 100%. Among contacts tested 6 to 9 days post-exposure (17%) the Sen decreased to 50%, with a Spe of 100%, and after 10 days (45%) the antigen test did not detect any of the 3 positive cases detected by the PCR test (Table 6).
| Table 6. Sensitivity of the rapid antigen test compared to PCR in children aged less than 14 years based on the days elapsed since the last contact with a positive case | ||||||
|---|---|---|---|---|---|---|
| Days after contact in children <14 years | PCR P/N | Panbio Sen, Spe, NPV, PPV | ||||
| N | P | |||||
| ≤5 | Test P/N | N | Count | 28 | 3 |
Sen 66.66% (95% IC 35.86-97.46) Spe 100%; PPV 100%; NPV 90.32 (95% CI 79.91-100.73) |
| % of total | 75.70% | 8.10% | ||||
| P | Count | 0 | 6 | |||
| % of total | 0.00% | 16.20% | ||||
| Total | Count | 28 | 9 | |||
| % of total | 75.70% | 24.30% | ||||
| 6-9 | Test P/N | N | Count | 16 | 1 |
Sen 50% (95% CI -19.29-119.29) Spe 100%; PPV 100%; NPV 94.11 (95% CI 82.93-105.30) |
| % of total | 88.90% | 5.60% | ||||
| P | Count | 0 | 1 | |||
| % of total | 0.00% | 5.60% | ||||
| Total | Count | 16 | 2 | |||
| % of total | 88.90% | 11.10% | ||||
| ≥10 | Test P/N | N | Count | 42 | 3 | 0 positive antigen tests |
| % of total | 93.30% | 6.70% | ||||
We found that 44.2% of infections in children were transmitted in the household and 30% in social gatherings.
DISCUSSION
The now generally available RDTs in our region offer an opportunity to contain the transmission of the virus. The Sen of the Panbio COVID-19 rapid antigen test in symptomatic patients of approximately 81% in our study in Castilla y León was consistent with the findings of other studies conducted elsewhere in Spain, and it is recommended that the test be used within 5 days of the onset of symptoms.2,5,6
At the time we conducted this study, most previous works had focused on patients admitted to the hospital or managed in the emergency department,7-9 where the positivity rate was higher. However, as paediatricians working in primary care, we designed the study considering that it is in this care setting where RDTs could be more useful if they are effective and efficient.
The Sen of the Panbio COVID-19 test in our analysis of asymptomatic contacts was 68% in the first 5 days following the last exposure, lower compared to other studies.10 However, we were surprised to find an increase to 85% between days 6 and 9, which could be due to an increase in viral replication in that timeframe. In fact, Gremmels11 and Van der Moeren12 found a negative correlation between viral load and the number of PCR cycles required for detection of the virus, which would explain why antigen tests are rarely positive from day 10 while the PCR test is positive. Albert and Torres 13 and Pekosz14 found that when a rapid test was negative, SARS-CoV-2 also did not grow in specific culture medium. This suggests that despite the low sensitivity of the test from day 10 (Sen 65%) and at the time of a second PCR test in asymptomatic contacts, false negative results could be due to patients not having a high enough viral load and that it is possible to prevent transmission results with the detection of the virus only in infectious patients.
In patients with a previous diagnosis of COVID-19, it seems that no study has detected virus capable of growing in culture after 9 days of illness, despite persistently high viral loads.15 In fact, it seems that viral clearance is quicker in positive but asymptomatic individuals, so that the infectious period would be shorter. In this regard, we should consider whether it is necessary to perform an antigen test in positive cases after 10 days of isolation to ensure that they do not transmit the infection after discharge. Thus, the rapid antigen test could replace the PCR test that is ordered routinely for nursing home staff, health care workers or teachers before returning to work.
As for the type of contact, in our study half of the asymptomatic patients who tested positive had been exposed to the virus in the family, followed by other social interactions, and less frequently in educational settings (13%), as reported by other authors.16,17 The mean age of patients exposed in school was less than 16 months, which suggest that transmission was associated with childcare centres rather than schools.
In children, based on our results, it seems useful to make the test if they are symptomatic within 5 days from onset (Sen = 80%). As regards contacts, further consideration is required to determine whether the sensitivity of 66% in the first 5 days following last exposure to a positive case warrants use of the test given that the viral load is lower in these patients,18 which is not to say that they could not transmit the infection. However, this could explain the lower rate of transmission among children independently of the safety measures implemented in schools.
It would be interesting to conduct a study differentiating between contacts who are asymptomatic and those who have started to experience symptoms that could initially have gone unnoticed, in addition to analysing results based on the prevalence of the disease in the corresponding health care area or district, as the number of tests ordered, the indication of testing based on a greater or lesser presence of symptoms or delays in testing due to increases in the health care burden may play a role.
Through the different waves of the pandemic, we have learned to use more sensitive testing methods when the incidence is lower, such as PCR, to try not to miss any cases.
One of the objectives to pursue in the short-term would be for clinical guidelines to define more accurately the symptoms present most frequently in positive cases based on tracing data. Also, needless to say, the analysis of inflammatory markers in the immune response of symptomatic individuals, asymptomatic contacts and immunosuppressed individuals based on the days from onset or exposure could explain the reduced expression of COVID-19 in children or the susceptibility of those who go on to develop multisystem inflammatory syndrome temporally associated with SARS-CoV-2.
CONCLUSION
The SARS-CoV-2 rapid antigen test may be useful to detect positive cases among symptomatic patients in the first 5 days from the onset, in both children and adults. The rapid antigen test may also be useful between 5 and 10 days post-exposure in asymptomatic adult contacts.
The test can be used to detect positive cases in household contacts, as the home is the most frequent setting of exposure.
The decline in sensitivity from day 10 compared to the PCR test should be interpreted taking into account published data on the correlation between viral loads and infectivity.
ABBREVIATIONS
CI: confidence interval · PCR: polymerase chain reaction · RDT: rapid diagnostic test/testing · SD: standard deviation · Sen: sensitivity · Spe: specificity.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to disclose in relation to the preparation and publication of this article.
REFERENCES
- Harrington A, Cox B, Snowdon J, Bakst J, Ley E, Grajales P, et al. Comparison of Abbott ID Now and Abbott m2000 methods for the detection of SARS-CoV-2 from nasopharyngeal and nasal swabs from symptomatic patients. J Clin Microbiol. 2020;58:e00798.
- Porte l, Legarraga P, Vollrath V, Aguilera X, Munita JM, Araos R, et al. Evaluation of a novel antigen-based rapid detection test for the diagnosis of SARS-CoV-2 in respiratory samples. Int J Infect Dis. 2020;99:328-33.
- Calderaro A, De Conto F, Buttrini M, Piccolo G, Montecchini S, Maccari C, et al. Human respiratory viruses, including SARS-CoV-2, circulating in the winter season 2019-2020 in Parma, Northern Italy. Int J Infect Dis. 2021;102:79-84.
- CDC COVID-19 Response Team, CDC COVID-19 Response Team, Bialek S, Gierke R, Hughes M, McNamara LA, et al. Coronavirus Disease 2019 in Children — United States, February 12–April 2, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:422-6.
- Candel FJ, Barreiro P, San Román J, Abanades JC, Barba R, Barberán J, et al. Recommendations for use of antigenic tests in the diagnosis of acute SARS-CoV-2 infection in the second pandemic wave: attitude in different clinical settings. Rev Esp Quimioter. 2020;33:466-84.
- Linares M, Pérez Tanoira R, Romanyk J, Pérez García F, Gómez-Herruz P, Arroyo T, et al. Panbio antigen rapid test is reliable to diagnose SARS-CoV-2 infection in the first 7 days after the onset of symptoms. J Clin Virol. 2020;133:104659.
- Young S, Taylor SN, Cammarata CL, Varnado KG, Roger-Dalbert C, Montano A, et al. Clinical Evaluation of BD Veritor SARS-CoV-2 Point-of-Care Test Performance Compared to PCR-Based Testing and versus the Sofia 2 SARS Antigen Point-of-Care Test. J Clin Microbiol. 2020;59:e02338-20.
- Scohy A, Anantharajah A, Bodéus M, Kabamba-Mukadi B, Verroken A, Rodriguez-Villalobos H. Low performance of rapid antigen detection test as frontline testing for COVID-19 diagnosis. J Clin Virol. 2020;129:104455.
- Lambert-Niclot S, Cuffel A, Le Pape S, Vauloup-Fellous C, Morand-Joubert l, Roque-Afonso A-M, et al. Evaluation of a Rapid Diagnostic Assay for Detection of SARS-CoV-2 Antigen in Nasopharyngeal Swabs. J Clin Microbiol. 2020;58:e00977.
- Alemany A, Baro B, Ouchi D, Ubals M, Corbacho-Monné M, Vergara-Alert J, et al. Analytical and Clinical Performance of the Panbio COVID-19 Antigen-Detecting Rapid Diagnostic Test. J Infect. 2021;82:186-230.
- Gremmels H, Winkel BMF, Schuurman R, Rosingh A, Rigter NAM, Rodriguez O, et al. Real-life validation of the Panbio COVID-19 Antigen Rapid Test (Abbott) in community-dwelling subjects with symptoms of potential SARS-CoV-2 infection. Eclinical Med. 2021;31:100677.
- Van der Moeren N, Zwart VF, Lodder EB, Van den Bijllaardt W, Van Esch HRJM, Stohr JJJM, et al. Evaluation of the test accuracy of a SARS-CoV-2 rapid antigen test in symptomatic community dwelling individuals in the Netherlands. PLos One. 2021;16:e0250886.
- Albert E, Torres I, Bueno F, Huntley D, Molla E, Fernández-Fuentes MÁ, et al. Field evaluation of a rapid antigen test (Panbio COVID-19 Ag Rapid Test Device) for the diagnosis of COVID-19 in primary healthcare centers. Clin Microbiol Infect. 2021;27:472.e7-472.e10.
- Pekosz A, Cooper CK, Parvu V, Li M, Andrews JC, Manabe YC, et al. Antigen-based testing but not real-time PCR correlates with SARS-CoV-2 virus culture. Clin Infect Dis. 2021;73(9):e2861-e2866.
- Cevik M, Tate M, Lloyd O, Maraolo AE, Schafers J, Ho A. SARS-CoV-2, SARS-CoV, and MERS-CoV viral load dynamics, duration of viral shedding, and infectiousness: a systematic review and meta-analysis. The Lancet Microbe. 2021;2:e13-e22.
- Melé M, Henares D, Pino R, Asenjo S, Matamoros R, Fumadó V, et al. Low impact of SARS-CoV-2 infection among paediatric acute respiratory disease hospitalizations. J Infect. 2021;82:414-51.
- Ríos-Barnés M, Lanaspa M, Noguera-Julian A, Baleta l, De Sevilla MF, Ferri D, et al. The Spectrum of COVID-19 Disease in Adolescents. Arch Bronconeumol. 2021;57:84-5.
- Kociolek LK, Muller WJ, Yee R, Dien Bard J, Brown CA, Revell P, et al. Comparison of upper respiratory viral load distributions in asymptomatic and symptomatic children diagnosed with SARS-CoV-2 infection in pediatric hospital testing programs. J Clin Microbiol. 2020;59:e02593-20.