
Vol. 24 - Num. 94
Original Papers
Use of antibiotics in the population aged less than fourteen years
Juan Ríos Laordena, Carlos Marcilla Vázquezb, Ángeles Lloret Callejoc, Francisco Tejada Cifuentesc, M.ª José Tirado Peláezc
aPediatra. CS Zona VI. Gerencia de Atención Integrada de Albacete. Albacete. España.
bServicio de Pediatría. Complejo Hospitalario Universitario. Gerencia de Atención Integrada de Albacete. Albacete. España.
cFarmacéutico de Atención Primaria. Gerencia de Atención Integrada de Albacete. Albacete. España.
Reference of this article: Ríos Laorden J, Marcilla Vázquez C, Lloret Callejo A, Tejada Cifuentes F, Tirado Peláez MJ. Use of antibiotics in the population aged less than fourteen years. Rev Pediatr Aten Primaria. 2022;24:137-47.
Published in Internet: 15-06-2022 - Visits: 20773
Abstract
Objective: to map antibiotic prescription for management of infections by age group in children aged less than 14 years at the primary care level.
Patients and methods: observational descriptive study of medication use focused on antibiotic prescription. The study population corresponded to all children in our health care area that received antibiotic prescriptions during the study period (January 2017 to December 2019). We assessed the usefulness of the indicators described in the antibiotic use optimization programme.
Results: in 2017, the total number of prescribed antibiotics was 28 030, 12% and 14% more than in 2018 and 2019, respectively. In 2018, 31.4% of the population under study received a prescription for at least one antibiotic per year, while in 2019 the percentage was 35.8%. When it came to children who received 2 prescriptions per year, the percentage was 15.4% in 2018 and 14.4 % in 2019. The prescription of beta-lactamase sensitive penicillins increased from 1.7 % in 2017 to 7.7% in 2019, while prescription of macrolides exhibited the opposite trend, decreasing from 19.6% in 2017 to 14.9% in 2019.
Conclusion: this study is the first to obtain quantitative and qualitative indicators of antibiotic use in paediatric age for management of common infectious diseases. It confirmed the high consumption of antibiotics, especially in children under 4 years of age, in addition to the inappropriate use of certain groups of antibiotics, such as macrolides and cephalosporins, for diseases for which they are not the first-line treatment.
Keywords
● Antibiotics ● Indicators ● Paediatric population ● Rational useINTRODUCTION
Consumption of antibiotics for systemic use in the Spanish paediatric population at the autonomous community level is high.1 Indeed, in 2019 we were in fifth place in the list of European countries with the highest consumption of antibiotics, taking into account only the data on those dispensed with an official prescription funded by the National Health System and excluding three other important sources: self-medication, private prescription and hospital use.2 This excessive consumption is not confined to any particular age group, and in the paediatric population it is also high.3 The European Centre for Disease Prevention and Control (ECDC) has recently reported, based on to the data available from the Spanish Pharmacovigilance System, that the current situation of antimicrobial drug resistance in Spain poses a serious public health threat for the country, with very high levels of methicillin-resistant Staphylococcus aureus, extended-spectrum beta-lactamase-producing Enterobacteriaceae4,5 and Acinetobacter baumannii, above the European Union (EU) mean. Furthermore, the rapid increase in carbapenemase-producing Enterobacteriaceae in the past five years represents a new threat to patient safety in every area of healthcare. All these factors, combined with the high consumption of antibiotics, do not constitute optimum conditions for controlling these multidrug-resistant organisms.6
The increase in the prevalence of drug-resistant bacteria in recent years makes the implementation of strategies aimed at prevention and control of such resistances a matter of pressing urgency. These interventions must be directed primarily at preventing the transmission of infections and promoting rational use of antimicrobials.7
In December 2014, approval was given for the implementation of antibiotic stewardship programmes (ASPs) in the hospital and primary care (PC) settings, through the national plan for combating antibiotic resistance in Spain, known as PRAN, which was in force for 5 years (2014-2018). Subsequently, in 2019, the PRAN for 2019-2021 was approved, and it continues moving forward on the foundation constructed with the work undertaken between 2014 and 2018, with the general aim of reducing or at least slowing down the growth of antimicrobial resistance and its impact on the health of the whole population. To achieve this, two general strategies are proposed: reducing the consumption of antibiotics and reducing the need to use antibiotics in human and veterinary medicine.8 Optimization of antibiotic prescribing must be seen as a process of changing prescribing habits, with the ultimate objectives of obtaining better clinical results in patients with infections and minimizing the adverse effects of antibiotics, primarily the emergence, evolution and spread of antimicrobial resistance.
The decision-making process for antibiotic prescribing is influenced by internal and external factors, to such an extent that it is known that 35% to 50% of antibiotic treatments could be optimised in different care settings.9
Strategic line I of the PRAN of the Agencia Española del Medicamento y Productos Sanitarios (AEMPS: Spanish Agency for Medicines and Medical Devices) establishes surveillance of antibiotic consumption and resistance. Specifically, it indicates the need to monitor consumption of antibiotics as an indispensable measure to ascertain the pressure that their use exerts on the emergence of resistances, by implementing two actions: improving the collection of data on antibiotic consumption in the community and in hospitals and ensuring that the data are used and analysed locally, regionally and nationally, and that this information is fed back to those systems, in addition to facilitating access to it through a public platform (consumption maps) where national data can be consulted, resources in which, to date, data stratified by age or population groups has yet to be made available.10
Similarly, strategic line II of the PRAN set reducing the amount of prescribing, overall and in non-bacterial infections, and improving appropriate use in specific diseases as priority objectives in PC paediatrics.11
At the European level, southern countries consume higher amounts of antibiotics than northern ones, as much as three times the quantity of the countries with the lowest consumption (the Netherlands and Nordic Countries). This north–south pattern is clear both in the consumption of antibiotics and in antimicrobial resistance, and it is most obvious in PC, with a more homogeneous level of consumption across countries in hospital settings.12 A comparison of antibiotic consumption in paediatric age groups between different European countries reveals substantial variation in antibiotic prescribing patterns, suggesting that a large proportion of antimicrobials are being used inappropriately, mainly for treatment of respiratory infections.13-15
For years, health systems have been monitoring antibiotic prescribing by medical professionals, especially in PC. In our health system, monitoring has been based mainly on calculating the defined daily dose per 1000 people per day (DDD/1000/day) of anti-infectives for systemic use, cephalosporins and macrolides, and of second-line anti-infectives for systemic use (fluoroquinolones and third- and fourth-generation cephalosporins). In the National Plan, total and paediatric population indicators have been established, although the published data on these are general and not stratified by age.16
The objective of this study was to perform an analysis of antibiotic consumption and appropriateness of antibiotic prescribing in the paediatric population in the Albacete Integrated Healthcare Management District (Gerencia de Atención Integrada) for management of the most prevalent infectious processes, and to propose a set of general and specific indicators of antibiotic use for paediatrics. Furthermore, we will present the results stratified by population groups (stratification by age).
In addition, following the recommendations of the PRAN, we are providing feedback to inform and educate healthcare staff, with the aim of reducing the consumption and improving the use of antibiotics in the paediatric population, in the context of an antimicrobial stewardship programme.
MATERIAL AND METHODS
We conducted a descriptive, observational study of medication use in relation to antibiotic prescribing in the paediatric population in the Albacete Integrated Healthcare Management District (Spain), followed by a training intervention for healthcare professionals in the area.
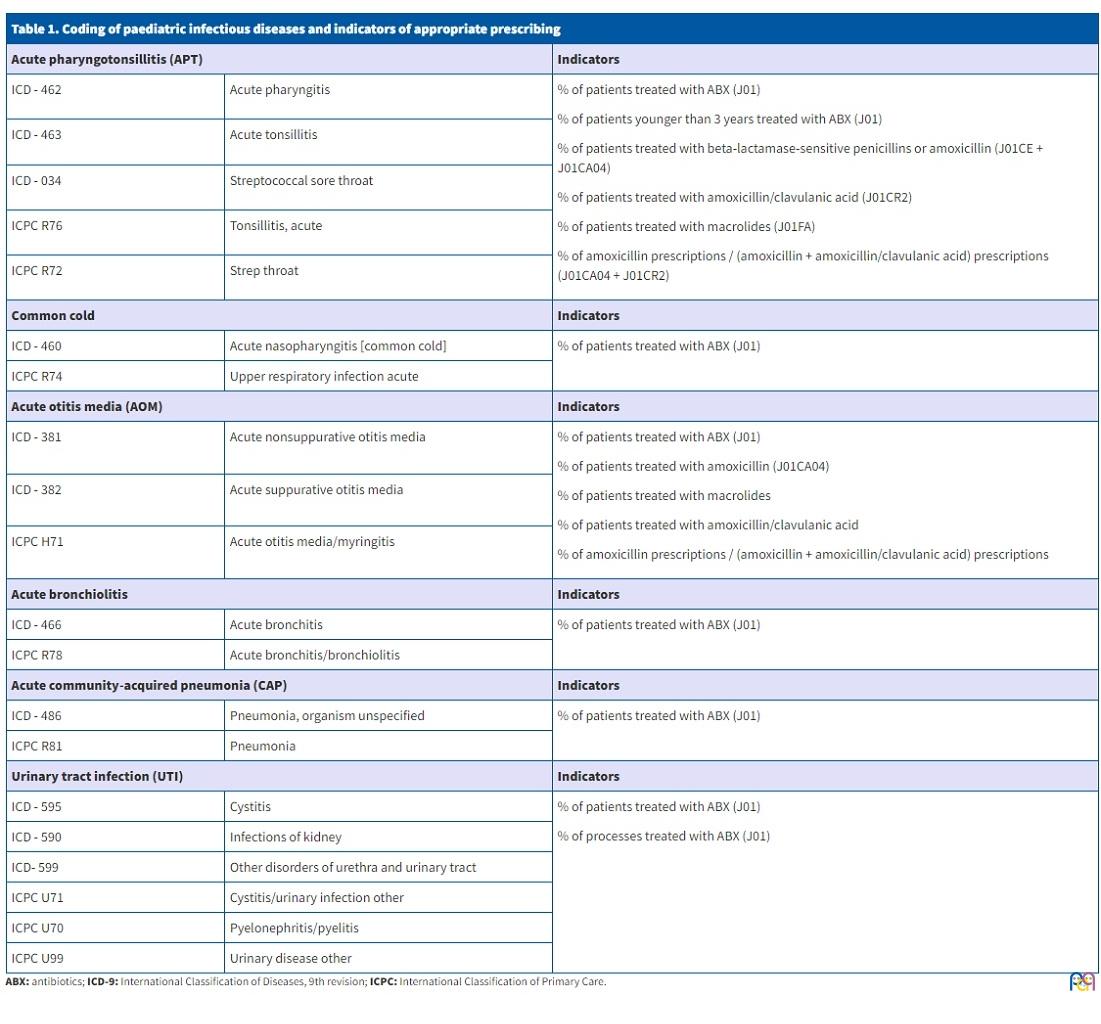
The study sample consisted of all the children in the area, of both sexes (aged 0-14 years), who received a prescription for at least one antibiotic during the study period (January 2017 to December 2019). The variables collected for conducting the study, obtained from the PC information system (Turriano) of the Castilla-La Mancha Health Service (SESCAM), are described below. All the data were coded in an anonymized form: day of the week of prescription; month of prescription; sex; diagnosis: we used the coding of the International Classification of Diseases, 9th revision (ICD-9-CM) and of the International Classification of Primary Care (ICPC) (Table 1); antibiotic: we used the Anatomical Therapeutic Chemical (ATC) classification system, pharmacological subgroup J01; date of birth of patient; primary care centre.
| Table 1. Coding of paediatric infectious diseases and indicators of appropriate prescribing | ||
|---|---|---|
| Acute pharyngotonsillitis (APT) | Indicators | |
| ICD - 462 | Acute pharyngitis |
% of patients treated with ABX (J01) % of patients younger than 3 years treated with ABX (J01) % of patients treated with beta-lactamase-sensitive penicillins or amoxicillin (J01CE + J01CA04) % of patients treated with amoxicillin/clavulanic acid (J01CR2) % of patients treated with macrolides (J01FA) % of amoxicillin prescriptions / (amoxicillin + amoxicillin/clavulanic acid) prescriptions (J01CA04 + J01CR2) |
| ICD - 463 | Acute tonsillitis | |
| ICD - 034 | Streptococcal sore throat | |
| ICPC R76 | Tonsillitis, acute | |
| ICPC R72 | Strep throat | |
| Common cold | Indicators | |
| ICD - 460 | Acute nasopharyngitis [common cold] | % of patients treated with ABX (J01) |
| ICPC R74 | Upper respiratory infection acute | |
| Acute otitis media (AOM) | Indicators | |
| ICD - 381 | Acute nonsuppurative otitis media |
% of patients treated with ABX (J01) % of patients treated with amoxicillin (J01CA04) % of patients treated with macrolides % of patients treated with amoxicillin/clavulanic acid % of amoxicillin prescriptions / (amoxicillin + amoxicillin/clavulanic acid) prescriptions |
| ICD - 382 | Acute suppurative otitis media | |
| ICPC H71 | Acute otitis media/myringitis | |
| Acute bronchiolitis | Indicators | |
| ICD - 466 | Acute bronchitis | % of patients treated with ABX (J01) |
| ICPC R78 | Acute bronchitis/bronchiolitis | |
| Acute community-acquired pneumonia (CAP) | Indicators | |
| ICD - 486 | Pneumonia, organism unspecified | % of patients treated with ABX (J01) |
| ICPC R81 | Pneumonia | |
| Urinary tract infection (UTI) | Indicators | |
| ICD - 595 | Cystitis |
% of patients treated with ABX (J01) % of processes treated with ABX (J01) |
| ICD - 590 | Infections of kidney | |
| ICD- 599 | Other disorders of urethra and urinary tract | |
| ICPC U71 | Cystitis/urinary infection other | |
| ICPC U70 | Pyelonephritis/pyelitis | |
| ICPC U99 | Urinary disease other | |
Bearing in mind that in paediatric patients the dosage is not standardized but calculated according to the patient’s weight, we used the number of days of treatment (DOT) as the unit of measurement in this study. Calculating this unit involved considerable difficulty and variability due to irregularities in the completion of the prescription form, which did not reliably include the section on duration of treatment. Therefore, we calculated the DOT based on the theoretical use of each antibiotic for each of the common diseases analysed in our study, taking into account the indicated duration of treatment for each disease according to Spanish consensus guidelines and how age affects it in some of them, for example, in acute otitis media (AOM).17,18
We performed a descriptive analysis of the variables, analysing both the consumption and the indication of the antibiotic. We included as outcomes all the indicators described in the PC paediatrics ASP. We calculated the consumption indicators for each of the 3 years of the study period and by age group (0-4, 5-9 and 10-14 years): consumption rate of antibiotics for systemic use; prevalence of antibiotic use or percentage of the paediatric population that consumed antibiotics in a year; percentage of beta-lactamase-sensitive penicillin consumption in the paediatric population; percentage of amoxicillin consumption relative to the total; percentage of amoxicillin/clavulanic acid consumption relative to the total; percentage of consumption of amoxicillin without clavulanic acid; percentage of macrolide consumption relative to the total and percentage of third-generation cephalosporin consumption relative to the total (Table 1). We assessed the appropriateness of antibiotic prescribing by calculating all the qualitative indicators, plus others that we developed ourselves for diagnoses for which the PRAN has not established indicators.
The study was conducted in accordance with the principles of the Declaration of Helsinki and of the Organic Data Protection Law of 25 May 2018. This study was approved by the regional Ethics Committee of Research with Medicines.
RESULTS
The study population did not vary much over the 3-year period, ranging from 38 857 children aged 0 to 14 years in 2017 to 38 299 in 2019. During the first year (2017), the total number of group J01 antibiotics prescribed in children aged 0 to 14 years was 28 030, 12% more than in 2018 (25 016) and 14% more than in 2019 (24 557). In the overall 3-year period, prescribing was more frequent in boys and in the 0 to 4-year age group, decreasing as age increased.
To calculate the antibiotic consumption rate, we used the theoretical DOT obtained for each antibiotic and each disease. More appropriate prescribing is reflected in the decrease in the DOT observed over the course of the study period, from 8.2 in 2017 to 7.7 in 2018 and 7.2 in 2019 (Table 2).
| Table 2. Population data, antibiotic consumption and days of treatment, overall and by age group | |||
|---|---|---|---|
| 2017 | 2018 | 2019 | |
| Population by age group | |||
| Age 0-4 years | 11 529 | 11 074 | 11 103 |
| Age 5-9 years | 13 493 | 13 142 | 13 150 |
| Age 10-14 years | 13 835 | 14 087 | 14 046 |
| Age 0-14 years | 38 857 | 38 303 | 38 299 |
| Prevalence of ABX use (%) by age group per year | |||
| ABX, 0-4 years | 13 387 (116.1%) | 12 271 (110.8%) | 11 777 (106.1%) |
| ABX, 5-9 years | 9266 (68.7%) | 7940 (60.4%) | 7835 (59.6%) |
| ABX, 10-14 years | 5377 (38.9%) | 4805 (34.1%) | 4945 (35.2%) |
| ABX, 0-14 years | 28 030 | 25 016 | 24 557 |
| DOT (days) by age group | |||
| DOT, 0-4 years | 8.1 | 7.5 | 7 |
| DOT, 5-9 years | 8.2 | 7.9 | 7.4 |
| DOT, 10-14 years | 8.4 | 8 | 7.5 |
| Mean DOT | 8.2 | 7.7 | 7.2 |
| Total no. of episodes | 61 534 | 61 334 | 58 818 |

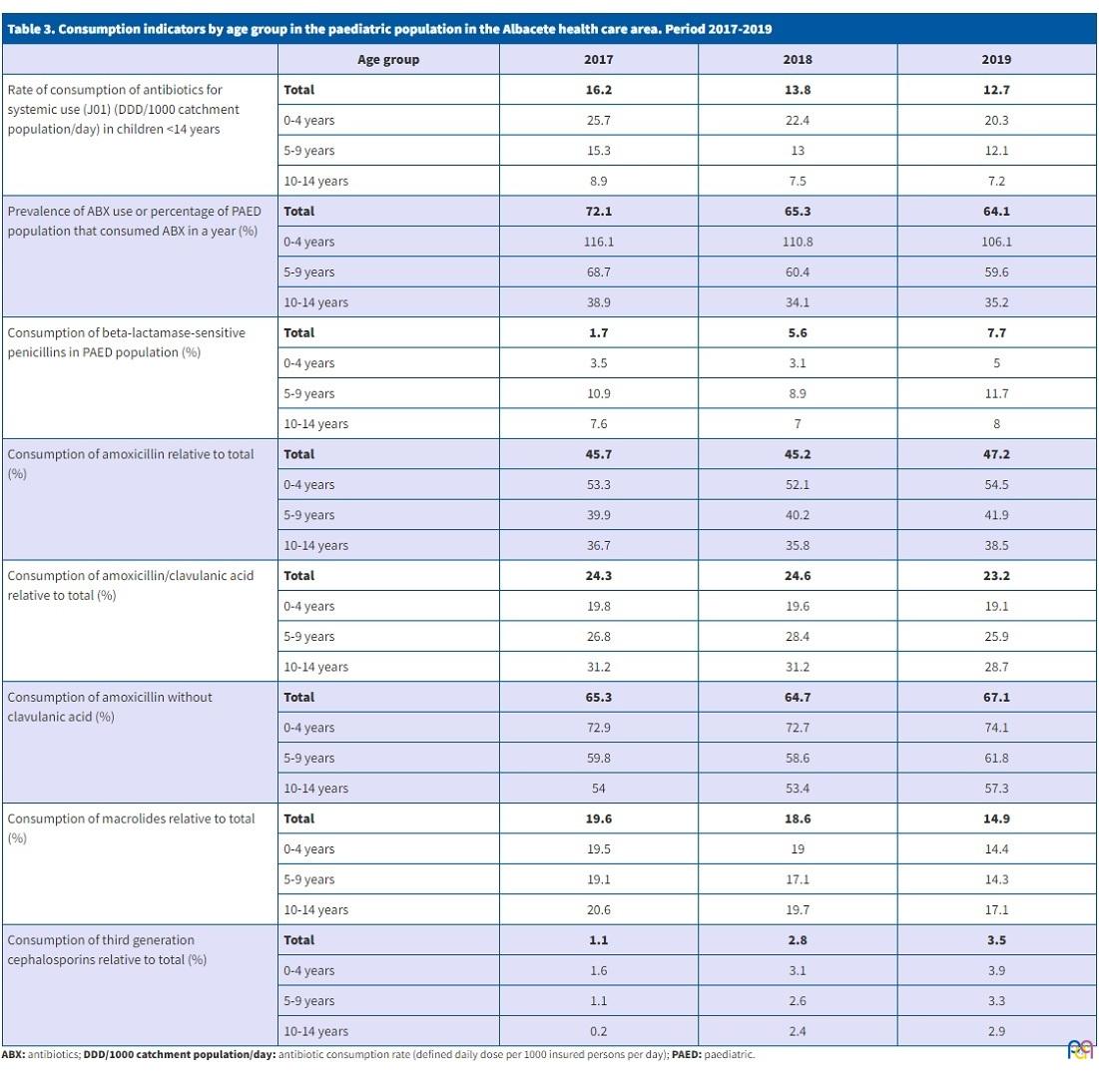
The antibiotic consumption rate found in the group aged 0 to 4 years was almost double the rate found in the group aged 10 to 14 years throughout the study period (Table 3). Antibiotic use was also higher in the first four years of life, decreasing over the course of the study period, from 116.1% in 2017 to 106.1% in 2019. The consumption rate was higher in rural areas than urban areas (19.1% in 2018 and 18.6% in 2019 versus 10.8% and 10.7%).
| Table 3. Consumption indicators by age group in the paediatric population in the Albacete health care area. Period 2017-2019 | ||||
|---|---|---|---|---|
| Age group | 2017 | 2018 | 2019 | |
| Rate of consumption of antibiotics for systemic use (J01) (DDD/1000 catchment population/day) in children <14 years | Total | 16.2 | 13.8 | 12.7 |
| 0-4 years | 25.7 | 22.4 | 20.3 | |
| 5-9 years | 15.3 | 13 | 12.1 | |
| 10-14 years | 8.9 | 7.5 | 7.2 | |
| Prevalence of ABX use or percentage of PAED population that consumed ABX in a year (%) | Total | 72.1 | 65.3 | 64.1 |
| 0-4 years | 116.1 | 110.8 | 106.1 | |
| 5-9 years | 68.7 | 60.4 | 59.6 | |
| 10-14 years | 38.9 | 34.1 | 35.2 | |
| Consumption of beta-lactamase-sensitive penicillins in PAED population (%) | Total | 1.7 | 5.6 | 7.7 |
| 0-4 years | 3.5 | 3.1 | 5 | |
| 5-9 years | 10.9 | 8.9 | 11.7 | |
| 10-14 years | 7.6 | 7 | 8 | |
| Consumption of amoxicillin relative to total (%) | Total | 45.7 | 45.2 | 47.2 |
| 0-4 years | 53.3 | 52.1 | 54.5 | |
| 5-9 years | 39.9 | 40.2 | 41.9 | |
| 10-14 years | 36.7 | 35.8 | 38.5 | |
| Consumption of amoxicillin/clavulanic acid relative to total (%) | Total | 24.3 | 24.6 | 23.2 |
| 0-4 years | 19.8 | 19.6 | 19.1 | |
| 5-9 years | 26.8 | 28.4 | 25.9 | |
| 10-14 years | 31.2 | 31.2 | 28.7 | |
| Consumption of amoxicillin without clavulanic acid (%) | Total | 65.3 | 64.7 | 67.1 |
| 0-4 years | 72.9 | 72.7 | 74.1 | |
| 5-9 years | 59.8 | 58.6 | 61.8 | |
| 10-14 years | 54 | 53.4 | 57.3 | |
| Consumption of macrolides relative to total (%) | Total | 19.6 | 18.6 | 14.9 |
| 0-4 years | 19.5 | 19 | 14.4 | |
| 5-9 years | 19.1 | 17.1 | 14.3 | |
| 10-14 years | 20.6 | 19.7 | 17.1 | |
| Consumption of third generation cephalosporins relative to total (%) | Total | 1.1 | 2.8 | 3.5 |
| 0-4 years | 1.6 | 3.1 | 3.9 | |
| 5-9 years | 1.1 | 2.6 | 3.3 | |
| 10-14 years | 0.2 | 2.4 | 2.9 | |
In 2017, 39.4% of the total population received a prescription for 1 antibiotic per year and 16.6% prescriptions for 2 antibiotics per year, with a maximum of 18 antibiotic prescriptions in 1 patient. In 2018, 31.4% of the total population received a single prescription and 15.4% two prescriptions. Finally, in 2019, 35.8% of the total population received one prescription for an antibiotic and 14.4% prescriptions for 2 antibiotics. In both 2017 and 2018, the maximum number of prescriptions made was 20, in both cases in a single patient.
The largest increase in antibiotic consumption during the study period corresponded to the group of beta-lactamase-sensitive penicillins (from 1.7% in 2017 to 5.6% in 2018 and 7.7% in 2019), followed by third generation cephalosporins (1.1% in 2017, 2.8% in 2018 and 3.5% in 2019). In contrast, the largest reduction was found in the macrolide consumption indicator, which went from 19.6% in 2017 to 18.6% in 2018 and decreased more markedly in 2019 to 14.9%. The decrease was proportional in each age group.
In children aged 0-4 years, a total of 61 534 episodes of infectious disease were documented during 2017, and 61 334 episodes in 2018, both greater than the total number of episodes recorded in 2019, which was 58 818. Of these, more than 85% corresponded to respiratory diseases, such as common colds or acute pharyngotonsillitis (APT).
In 2017, 37.7% of the paediatric population received treatment for an episode of APT. This proportion fell to 27.3% in 2018 and 27.3% in 2019 (Table 4). Out of all the care episodes coded as APT, the proportion treated with antibiotics was 68.6% in 2017, 58.6% in 2018 and 57.4% in 2019. In children aged less than 3 years, the proportion decreased over the course of the study (41.3% in 2017, 33% in 2018 and 23.8% in 2019). With regard to the choice of antibiotic to treat APT, there was an increase in the prescription of beta-lactamase-sensitive penicillins (from 60.3% in 2017 and 60.9 % in 2018 to 66.8% in 2019). In contrast, APT episodes treated with macrolides exhibited a significant decrease (from 20.7% in 2017 and 19.6% in 2018 to 14.3% in 2019). There was a lesser reduction in episodes treated with amoxicillin/clavulanic acid, which went from 12.5% in 2017 to 10.4% in 2018 and 9.5% in 2019.
| Table 4. Indicators of appropriate prescribing in the most prevalent infectious diseases in the paediatric population in the Albacete health care area, 2017-2019 period | ||||
|---|---|---|---|---|
| Infectious disease | Indicator | 2017 | 2018 | 2019 |
| Acute pharyngotonsillitis (APT) | % of patients treated with ABX (J01) | 37.6% | 27.3% | 27.3% |
| % of patients younger than 3 years treated with ABX (J01) | 41.3% | 33% | 23.8% | |
| % of patients treated with beta-lactamase-sensitive penicillins or amoxicillin (J01CE + J01CA04) | 60.3% | 60.9% | 66.8% | |
| % of patients treated with amoxicillin/clavulanic acid (J01CR2) | 18.2% | 17.7% | 16.6% | |
| % of patients treated with macrolides (J01FA) | 14.2% | 11.5% | 8.2% | |
| % of amoxicillin prescriptions / (amoxicillin + amoxicillin/clavulanic acid) prescriptions (J01CA04 + J01CR2) | 73.1% | 73.1% | 74.9% | |
| Common cold | % of patients treated with ABX (J01) | 8.6% | 5.5% | 4.1% |
| Acute otitis media (AOM) | % of patients treated with ABX (J01) | 15.7% | 15.3% | 15.1% |
| % of patients treated with amoxicillin (J01CA04) | 42.2% | 44.9% | 45.7% | |
| % of patients treated with macrolides | 8.1% | 5.5% | 4.9% | |
| % of patients treated with amoxicillin/clavulanic acid | 19.7% | 22.9% | 21.7% | |
| % of amoxicillin prescriptions / (amoxicillin + amoxicillin/clavulanic acid) prescriptions | 68.2% | 66.3% | 67.8% | |
| Acute bronchiolitis | % of patients treated with ABX (J01) | 3.1% | 2.6% | 2.2% |
| Acute community-acquired pneumonia (CAP) | % of patients treated with ABX (J01) | 0.3% | 0.8% | 0.8% |
| Urinary tract infection (UTI) | % of patients treated with ABX (J01) | 0.7% | 1.7% | 1.7% |
| % of processes treated with ABX (J01) | 31% | 80.2% | 69.8% | |
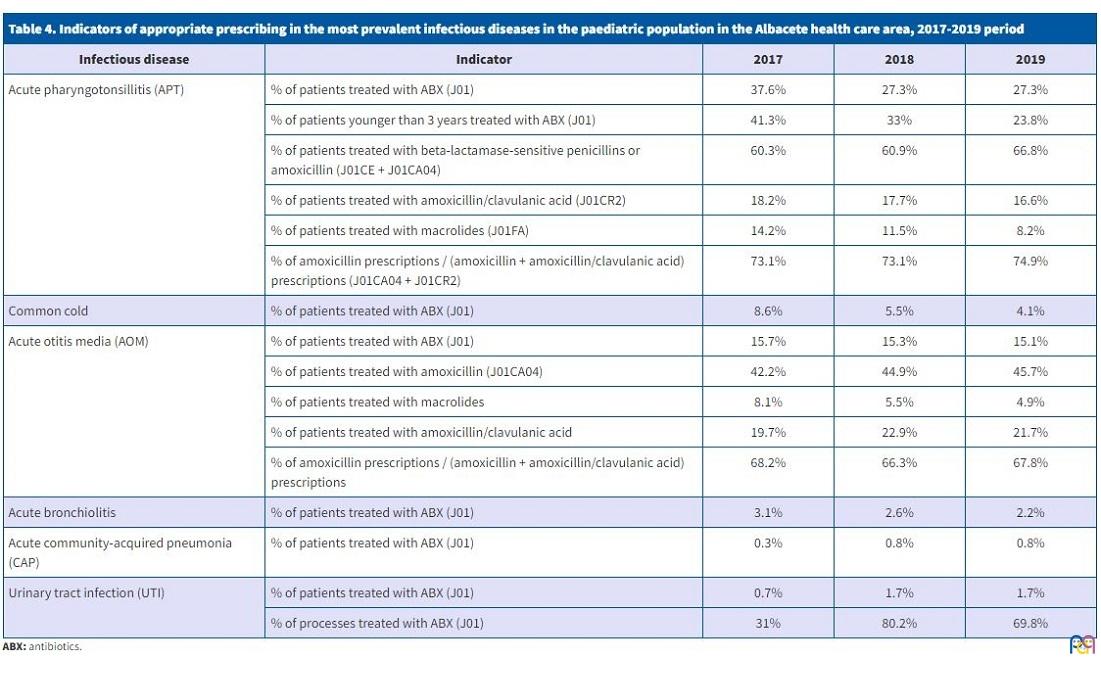
In the common cold diagnosis category, there was a decrease in patients treated with antibiotics: 8.6% in 2017, 5.5% in 2018 and 4.1% in 2019. The reduction was much steeper in the group aged less than 3 years, going from 16.6% in 2017 to 13.8% in 2018 and 9% in 2019.
As for acute otitis media (AOM), the proportion treated with antibiotics was very similar throughout the study period: 15.7% in 2017, 15.2% in 2018 and 15.1% in 2019. Approximately three-quarters of all the episodes coded as AOM were treated with antibiotics: 73.1% in 2017, 76.8% in 2018 and 76.6% in 2019. Nearly half the episodes of AOM were treated with amoxicillin (42.2% in 2017, 44.9% in 2018 and 45.7% in 2019). A not inconsiderable percentage (19.7% in 2017, 22.9% in 2018 and 21.7% in 2019) were treated with amoxicillin/clavulanic acid, and there was also a significant number of cases treated with macrolides (8.1% in 2017, with a significant decrease in the subsequent years to 5.5% in 2018 and 4.9% in 2019).
DISCUSSION
The paediatric population under study remained stable over the 3-year period, as did the trend of an annual reduction in antibiotic consumption. This is the first time that quantitative data have been obtained in the catchment population of our health care area stratified by age groups (0-4, 5-9 and 10-14 years), contrary to what is usually reported in most studies, which is usually data for the overall population,19-21, as is the case of the PRAN.8
Using the DOT to calculate overall consumption rates allowed us to get results that better reflect the selection of the different groups of antibiotics. The consumption rates in our study gradually decreased (2017-2019), although they were higher in the first years of life, contrary to what should happen, given that the number of viral infections is greater in this age group and therefore antibiotic treatment would be indicated less frequently.
As the study period progressed, we observed greater use of beta-lactamase-sensitive penicillins and a decrease in the use of macrolides, although these results are still inadequate, since beta-lactamase-sensitive penicillins are the treatment of choice for APT and we should be getting closer to a use of amoxicillin/clavulanic acid limited exclusively to consensus criteria.22
One of the main areas of inappropriate antibiotic prescribing is the overuse of macrolides, which is too high relative to the national and international recommendations for this group of antibiotics, motivated, perhaps, by the false sense of security elicited by their broad spectrum and ease of administration (low number of doses, volumes and duration). In our study we obtained consumption levels close to 15% for this subgroup, with a similar distribution in the 3 analysed age groups. If we consider the case of APT, for example, the episodes treated with macrolides amounted to 20.7% in 2017, 19.6% in 2018 and 14.3% in 2019, percentages that were much higher than they should have, given that macrolides are only indicated for management of APT in patients with anaphylactic penicillin allergy, whose prevalence in children is 1.7% to 5.2%.23
Obtaining specific consumption indicators linked to diagnoses in any population group is complex, and perhaps more so in paediatrics, where deficient recording or complex coding may affect the results. However, automation is having a decisive and favourable impact on electronic health records.24 Our study succeeded, for the first time in the paediatric population, in obtaining data for all the specific indicators in very stable populations of both patients and prescribers for this purpose.
The analysis of these indicators in the treatment of the second most prevalent infectious disease in the paediatric population, APT, revealed a decrease in the total number of patients treated with antibiotics (especially those aged less than 3 years) and an increase in the prescription of beta-lactamase-sensitive penicillins, which reflects more appropriate antibiotic selection.17 We also found a decrease in the prescribing of macrolides for management of APT (which is mainly indicated in patients allergic to penicillins), and also of amoxicillin/clavulanic acid, which is indicated in children with APT caused by group A beta-haemolytic streptococcus (GABHS) in whom previous treatment has failed or who are known carriers of this pathogen.17
Our findings show a consolidation of the trend towards not prescribing antibiotics in uncomplicated viral processes, such as the common cold. Four percent of children still receive unnecessary, and the percentage is even higher in those aged less than 3 years.
When it came to AOM, a large percentage of patients were treated with antibiotics (73.1% in 2017, 76.8% in 2018 and 76.6% in 2019), very high figures given that in 90% of cases AOM can be considered a self-limiting disease that has favourable outcomes with prescription of analgesia.18 Although it is true that the use of antibiotics prevents complications such as acute mastoiditis, this is not a common complication and more than 4000 patients with AOM need to be treated to prevent a single case of mastoiditis.18,25 Perhaps the choice of antibiotic cannot be considered inappropriate, since practically half were treated with amoxicillin and one fifth with amoxicillin/clavulanic acid, and this distribution can be explained if we take into account the cases of failure of first-line treatment with amoxicillin, in infants aged less than of six months or in children aged less than 2 years with severe symptoms.18 In the case of macrolides, their use for management of AOM was more appropriate compared to APT, as in the last year only 4.9% of patients with AOM received treatment with this therapeutic group.23 Although 30% to 50% of pneumococcal isolates are resistant to macrolides, this group is the treatment of choice in patients with severe penicillin allergy with anaphylactic reaction.18,26 In the case of AOM, we need to continue promoting strategies aimed at delaying prescription and establishing clinical criteria to guide appropriate empirical antibiotherapy with short 5-day courses of treatment.27
In our predominantly urban health care area, we found that antibiotic consumption was greater in the rural population, which could be explained by the lower number of paediatricians in rural areas.
Our study shows that ongoing training and evaluation with collection of antibiotic consumption data and delivery of feedback to prescribing professionals remain important. It confirms the need to establish an ASP in the PC system of our health care area, with the involvement and multidisciplinary work of all health care professionals.
CONFLICTS OF INTEREST
This study has received no funding of any kind. The authors have no conflicts of interest to declare.
ABBREVIATIONS
AEMPS: Agencia Española del Medicamento y Productos Sanitarios (Spanish Agency for Medicines and Medical Devices) · AOM: acute otitis media · APT: acute pharyngotonsillitis · ASP: antimicrobial stewardship programme · ATC: Anatomical Therapeutic Chemical (classification system) · CEIM: Comité Ético de Investigación con Medicamentos (Medication Research Ethics Committee) · ICPC: International Classification of Primary Care · DDD/1000/day: defined daily dose per 1000 people per day · DOT: number of days of treatment · ECDC: European Centre for Disease Prevention and Control · EU: European Union · GABHS: Group A beta-haemolytic streptococcus · ICD-9: International Classification of Diseases, 9th revision · PRAN: National Plan for Combating Antibiotic Resistance · PC: primary care · SESCAM: Castilla La Mancha Health Service.
REFERENCES
- Albañil Ballesteros MR. Plan Nacional de Resistencia a Antibióticos. Form Act Pediatr Aten Prim. 2016;9;56-9.
- Antimicrobial consumption in the EU/EEA, annual epidemiological report for 2019. In: European Centre for Disease Prevention and Control. Stockholm: ECDC; 2020: 4-9 [online] [accessed 16/02/2021]. Available at http://ecdc.europa.eu/en
- Malo S, Bjerrum l, Feja C, Lallana MJ, Poncel A, Rabanaque MJ. Prescripción antibiótica en infecciones respiratorias agudas en Atención primaria. An Pediatr. 2014; 82: 412-16.
- Canton R, Loza E, Aznar J, Barrón-Adúriz R, Calvo J, Castillo FJ, et al. Antimicrobial susceptibility trends and evolution of isolates with extended spectrum beta-lactamases among Gram-negative organisms recovered during the SMART study in Spain (2011-2015). Rev Esp Quimioter 2018; 31:136-45.
- Díaz MA, Hernández JR, Martínez-Martínez l, Rodríguez Baño J, Pascual A, Grupo de Estudio de Infección Hospitalaria (GEIH). Escherichia coli y Klebsiella pneumoniae productoras de betalactamasas de espectro extendido en hospitales españoles: segundo estudio multicéntrico (proyecto GEIH-BLEE 2006). Enferm Infecc Microbiol Clin 2009; 27:503-10.
- European Centre for Disease Prevention and Control. ECDC country visit to Spain to discuss antimicrobial resistance issues. Stockholm: ECDC; 2018.
- Fernández-Urrusuno R, Flores-Dorado M, Moreno-Campoy E, Montero-Balosa MC. Selección de indicadores para la monitorización continua del impacto de programas de optimización de uso de antimicrobianos en Atención Primaria. Enferm Infecc Microbiol Clin. 2015 May;33:311-9.
- Plan Nacional frente a la Resistencia de Antibióticos 2019-2021. In: Ministerio de Sanidad, Agencia Española de Medicamentos y Productos Sanitarios. 2019 [online] [accessed 01/12/2020]. Available at www.resistenciaantibioticos.es
- Hulscher MEJL, Grol RPTM, van der Meer JWM. Antibiotic prescribing in hospitals: a social and behavioural scientific approach. Lancet Infect Dis. 2010; 10:167-75.
- Plan estratégico y de riesgo para reducir el riesgo de selección y diseminación de la resistencia a los antibióticos. AEMPS. In: Ministerio de Sanidad, Servicios Sociales e Igualdad. 2015 [online] [accessed 09/06/2022] Available at www.aemps.gob.es/publicaciones/publica/plan-estrategico-antibioticos/v2/docs/plan-estrategico-antimicrobianos-AEMPS.pdf
- Objetivos de mejora prioritarios en Atención Primaria (Pediatría). AEMPS. In: Ministerio de Sanidad, Servicios Sociales e Igualdad. 2017 [online] [accessed 09/06/2022] Available at www.resistenciaantibioticos.es/es/publicaciones/objetivos-de-mejora-prioritarios-en-atencion-primaria-pediatria
- Ashiru-Oredope D, Hopkins S J. Antimicrobial stewardship: English Surveillance Programme for Antimicrobial Utilization and Resistance (ESPAUR). Antimicrob Chemother 2013; 68:2421-23.
- Holstiege J, Schink T, Molokhia M, Mazzaglia G, Innocenti F, Oteri A, et al. Systemic antibiotic prescribing to paediatric outpatients in 5 European countries: a population-based cohort study. BMC Pediatr. 2014; 14:11-14.
- Holstiege J, Garbe E. Systemic antibiotic use among children and adolescents in Germany: a population-based study. European Journal of pediatrics. 2013;172:787-95.
- Youngster I, Avorn J, Belleudi V, Cantarutti A, Díez-Domingo J, Kirchmayer U, et al. Antibiotic Use in Children. A Cross-National Analysis of six Countries. J Pediatr. 2017; 182:239-44.
- Informe anual PRAN. Junio 2019-Junio 2020. In: Ministerio de Sanidad, Agencia Española de Medicamentos y Productos Sanitarios. 2021 [online] [accessed 01/03/2021]. Available at www.resistenciaantibioticos.es
- Piñeiro Pérez R, Álvez González F, Baquero-Artigao F, Cruz Cañete M, de la Flor i Bru J, Fernández Landaluce A y Grupo Colaborador de Faringoamigdalitis Aguda en Pediatría. Actualización del documento de consenso sobre el diagnóstico y tratamiento de la faringoamigdalitis aguda. An Pediatr. 2020; 3:206.e1-206.e8
- Del Castillo Martín F, Baquero Artigao F, de la Calle Cabrera T, López Robles M, Ruiz Canela J, Alfayate Miguelez S, et al. Documento de consenso sobre etiología, diagnóstico y tratamiento de la otitis media aguda. An Pediatr (Barc): 2012; 77: 345.e1-345.e8
- Tyrstrup M, Beckman A, Mölstad S, Engström S, Lannering C, Melander E, et al. Reduction in antibiotic prescribing for respiratory tract infections in swedish primary care, a retrospective study of electronic patient records. BMC Infectious Diseases. 2016; 16:709.
- Lampi E, Carlsson F, Sundvall PD, Torres MJ, Ulleryd P, Åhrén C, et al. Interventions for prudent antibiotic use in primary healthcare: an econometric analysis. BMC Health Serv Res. 2020; 20: 895.
- García Vera C, Albañil Ballesteros R. Prescripción de antibióticos en pediatría de atención primaria: una responsabilidad compartida. An Pediatr. 2018; 89:195-6.
- Holten KB, Onusko EM. Appropriate prescribing of oral beta-lactam antibiotics. Am Fam Physician. 2000; 62:611-20.
- Baquero Artigao F, Michavila A, Suárez-Rodríguez A, Hernández A, Martínez-Campos l, Calvo C, et al. Documento de consenso de la Sociedad Española de Infectología Pediátrica, Sociedad Española de Inmunología Clínica y Alergia Pediátricas, Asociación Española de Pediatría de Atención Primaria y Sociedad Española de Pediatría Extrahospitalaria y Atención Primaria sobre antibioterapia en alergia a penicilina o Amoxicilina. An Pediatr (Barc) 2017; 86:99.e1-99.e9
- Ewald D, Huss G, Auras S, Cáceres JR, Hadjipanayis A, Geraedts M. Development of a core set of quality indicators for paediatric primary care practices in Europe, COSI-PPC-EU. Eur J Pediatr. 2018; 177:921-33.
- Thompson PL, Gilbert RE, Long PF, Saxena S, Sharland M, Wong IC. Effect of antibiotics for otitis media on mastoiditis in children: a retrospective cohort study. Pediatrics. 2009; 123:424-30
- Pérez E, Martín J, Mazón A, García C, Robles P, Iriarte V, et al. Antimicrobial resistance among respiratory pathogens in Spain: latest data and changes over 11 years (1996-1997 to 2006-2007). Antimicrobial Agents Chemother. 2010; 54:2953-59.
- Spurling G, del Mar C, Dooley l, Foxlee R, Farley R. Delayed antibiotic prescriptions for respiratory infections. Cochrane Database Syst Rev. 2017; 9.