
Vol. 24 - Num. 94
Original Papers
Breastfeeding promoting factors: LATMAGAL study
Carmen González Méndeza, Raquel López Rodríguezb, Pablo Diéguez Reyc, Jorge Suanzes Hernándezd, Carmen Amparo Rodríguez Lombardíae, Rosaura Leis Trabazof, Grupo LACTMATGAL
aServicio de Pediatría. Hospital Universitario Germans Trias i Pujol. Universidad Autónoma de Barcelona. Barcelona. España.
bMIR-Alergología. Hospital Universitario de A Coruña. A Coruña. España.
cMIR-Traumatología. Hospital Universitario del Henares. Coslada. Madrid. España.
dCoordinador Unidade de Apoio á Investigación. Responsable UICEC A Coruña - INIBIC / SCReN (ISCIII). Complejo Hospitalario Universitario de A Coruña. A Coruña. España.
ePediatra. CS Do Castrillón. A Coruña. España.
fServicio de Pediatría. Hospital Clínico Universitario de Santiago. Santiago de Compostela. A Coruña. España.
Correspondence: C González . E-mail: karmenglez_7@hotmail.com
Reference of this article: González Méndez C, López Rodríguez R, Diéguez Rey P, Suanzes Hernández J, Rodríguez Lombardía CA, Leis Trabazo R, et al. Breastfeeding promoting factors: LATMAGAL study. Rev Pediatr Aten Primaria. 2022;24:127-36.
Published in Internet: 13-06-2022 - Visits: 13816
Abstract
Introduction: the WHO recommends exclusive breastfeeding (EBF) up to 6 months of life due to its proven benefits. The latest published studies show that this objective is currently not being accomplished. The aim of this study was to determine the prevalence of breastfeeding (BF) in a Galician population, and the factors that promoted and limited breastfeeding.
Methods: observational and cross-sectional descriptive study through anonymous surveys of mothers of babies aged from 12 to 18 months (n = 280) in primary care paediatrics clinics.
Results: we found a prevalence of 85.3% for BF initiation, of 47.2% for EBF at 6 months and of only 38.9% for BF maintenance at 1 year. We found a higher frequency of BF initiation in rural settings (87.1% vs. 83.5%), although BF duration was greater in urban settings (EBF6 53.1% vs. 35.5%). We identified the recommendation by professionals to start BF during the puerperium and BF guidance before discharge from hospital as the main factors that promoted BF (p <0.01). Supervision of the first feedings increased the probability of initiation of BF by up to 3 times. The main BF limiting factors were insufficient milk production (p = 0.01), maternal health problems (p = 0.01) and the end of maternal leave (p = 0.04).
Conclusion: we found a higher prevalence of BF initiation and EBF at 6 months compared to other Spanish studies. Increasing promotion of BF in both the hospital and primary care setting and supervision of the first feedings are important strategies to achieve figures that approximate the targets set in international breastfeeding recommendations.
Keywords
● BreastfeedingINTRODUCTION
Exclusive breastfeeding until 6 months post birth (EBF6) provides the ideal nutrition to infants. Among its multiple benefits, we ought to highlight the establishment of a healthier intestinal microbiota, healthier development of the immune system, improved neurodevelopmental outcomes and a reduced incidence of infection.1-3 It also benefits maternal health, as it is associated with a decreased risk of breast and ovarian cancer. It also promotes mother-child bonding,4-8 is less costly and is more environmentally sustainable.2,9 For all these reasons, the World Health Organization (WHO) recommends exclusive breastfeeding (EBF) through age 6 months and breastfeeding (BF) combined with complementary foods through age 2 years.2,10-12 However, there are factors that pose barriers to BF, such as low socioeconomic status, young maternal age or lack of support to the mother.5,10-14 Early discontinuation of BF is mainly associated with the separation of mother and child, either due to the mode of delivery or to work-related factors. Overall, the most frequent reason for quitting BF is inadequate management and technique.15-18
At present, BF rates are far below the recommended targets, both in developed and developing countries,14-19 with substantial variability in the reported data. In 2016, the United Nations Children's Fund (UNICEF) published that 43% of children worldwide receive EBF6, with the highest rates found in South Asia, with a prevalence of 60%.20-22 In 2013 in the United States, the rate of BF initiation was 76%, but the rate of EBF6 was only 16%.23,24 In Europe, in 2003, United Kingdom and France had the lowest prevalence of BF, while the highest prevalence corresponded to the Nordic countries. Thus, Baerung et al. (2004) found a prevalence of BF initiation in the delivery room of 99% and a prevalence of EBF6 of 80% in Oslo.3,25-29 On the other hand, in Spain, based on data from the 2017 National Health Survey (NHS), the BF rate at 6 weeks was 73.9%, and the rate of EBF6 39%. This reflected a considerable increase compared to the 2006 NHS, in which the rate at 6 weeks was 68.4% and the rate of EBF6 was 24.7%.30
The current global target for 2025 is to achieve an EBF6 rate of 50%,5,30,31 for which different organizations, such as the American Academy of Pediatrics, the Iniciativa para la Humanización de la Asistencia al Nacimiento y a la Lactancia (Baby-Friendly Hospital Initiative in Spain, IHAN) and the Asociación Española de Pediatría (Spanish Association of Pediatrics, AEP) recommend the implementation at both the hospital and primary care (PC) level of measures to support BF initiation and maintenance.
Few studies have analysed the impact of intervention with different strategies. However, in order to determine which are the most suitable and achieve the established target, it would be interesting to analyse the current situation in different communities in Spain. The main objectives of our study were to establish the current prevalence of BF in different health care areas in the region of Galicia and to identify factors associated with the establishment of BF and its maintenance through time.
MATERIAL AND METHODS
We conducted a retrospective cross-sectional observational and descriptive study. Based on the analysis of previous results, we estimated a proportion of EBF6 in the population of 40%, based on which we calculated that for a level of confidence of 95% to detect changes of 6 percentage points, assuming a nonresponse rate of 10%, the minimum sample size required would be of 256 patients. The sample was stratified by health care area and type of setting (rural/urban), including 8 primary care centres that were representative of each of the provinces of the autonomous community of Galicia. The sample included 280 children, 35 per primary care centre.
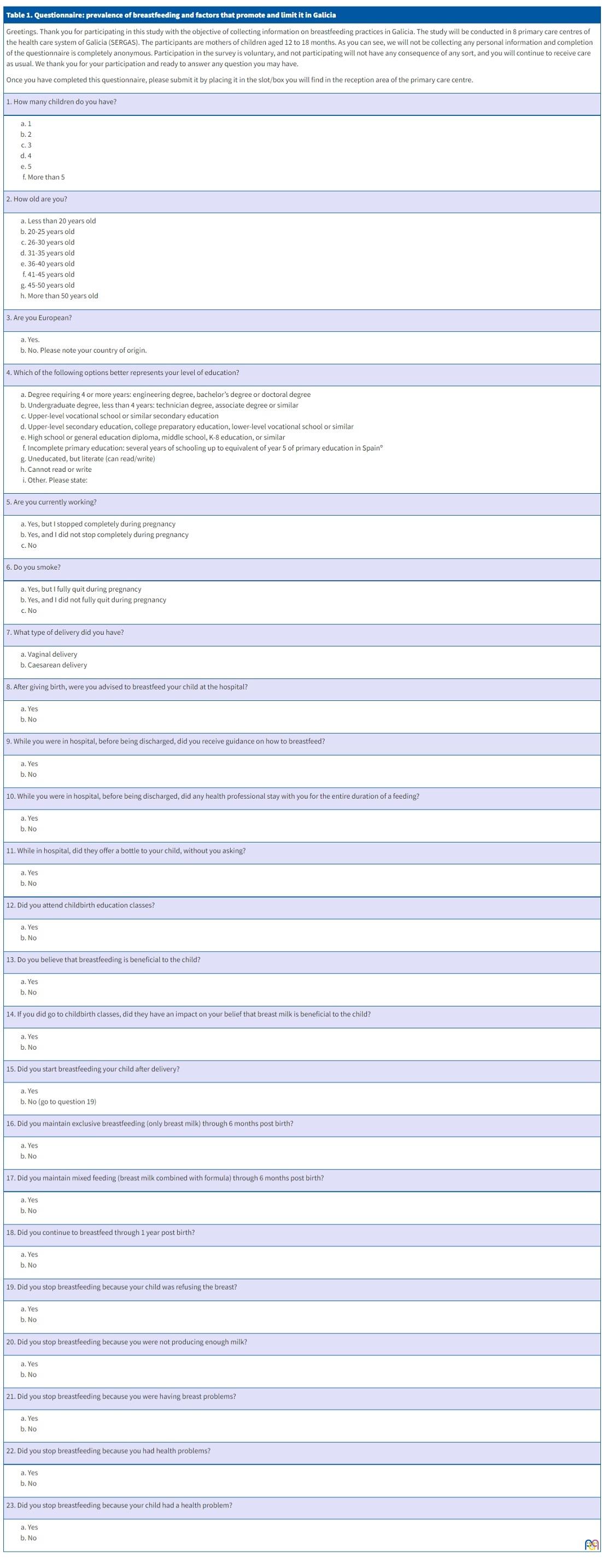
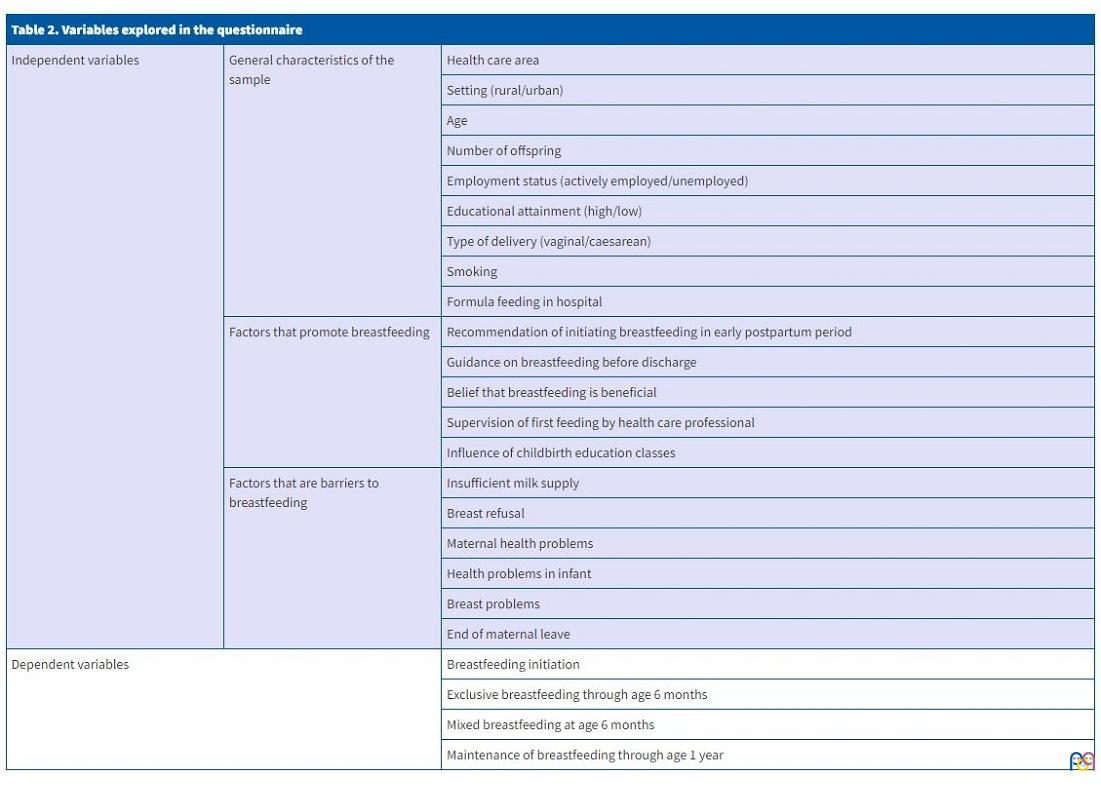
We collected data by administering a questionnaire to mothers of children aged 12 to 18 months that visited participating primary care paediatrics clinics between January and March 2019. Questionnaires were given to the mothers and completed in the primary care centre under the supervision of health care staff. The instrument was an in-house questionnaire and consisted of 25 items with dichotomous or multiple-choice answers (Table 1). It explored variables concerning the practice of BF and EBF6 and factors that could promote or pose barriers to BF, such as maternal age, number of children and BF support (Table 2).
| Table 1. Questionnaire: prevalence of breastfeeding and factors that promote and limit it in Galicia |
|---|
|
Greetings. Thank you for participating in this study with the objective of collecting information on breastfeeding practices in Galicia. The study will be conducted in 8 primary care centres of the health care system of Galicia (SERGAS). The participants are mothers of children aged 12 to 18 months. As you can see, we will not be collecting any personal information and completion of the questionnaire is completely anonymous. Participation in the survey is voluntary, and not participating will not have any consequence of any sort, and you will continue to receive care as usual. We thank you for your participation and ready to answer any question you may have. Once you have completed this questionnaire, please submit it by placing it in the slot/box you will find in the reception area of the primary care centre. |
|
1. How many children do you have? |
|
|
2. How old are you? |
|
|
3. Are you European? |
|
|
4. Which of the following options better represents your level of education? |
|
|
5. Are you currently working? |
|
|
6. Do you smoke? |
|
|
7. What type of delivery did you have? |
|
|
8. After giving birth, were you advised to breastfeed your child at the hospital? |
|
|
9. While you were in hospital, before being discharged, did you receive guidance on how to breastfeed? |
|
|
10. While you were in hospital, before being discharged, did any health professional stay with you for the entire duration of a feeding? |
|
|
11. While in hospital, did they offer a bottle to your child, without you asking? |
|
|
12. Did you attend childbirth education classes? |
|
|
13. Do you believe that breastfeeding is beneficial to the child? |
|
|
14. If you did go to childbirth classes, did they have an impact on your belief that breast milk is beneficial to the child? |
|
|
15. Did you start breastfeeding your child after delivery? |
|
|
16. Did you maintain exclusive breastfeeding (only breast milk) through 6 months post birth? |
|
|
17. Did you maintain mixed feeding (breast milk combined with formula) through 6 months post birth? |
|
|
18. Did you continue to breastfeed through 1 year post birth? |
|
|
19. Did you stop breastfeeding because your child was refusing the breast? |
|
|
20. Did you stop breastfeeding because you were not producing enough milk? |
|
|
21. Did you stop breastfeeding because you were having breast problems? |
|
|
22. Did you stop breastfeeding because you had health problems? |
|
|
23. Did you stop breastfeeding because your child had a health problem? |
|
| Table 2. Variables explored in the questionnaire | ||
|---|---|---|
| Independent variables | General characteristics of the sample | Health care area |
| Setting (rural/urban) | ||
| Age | ||
| Number of offspring | ||
| Employment status (actively employed/unemployed) | ||
| Educational attainment (high/low) | ||
| Type of delivery (vaginal/caesarean) | ||
| Smoking | ||
| Formula feeding in hospital | ||
| Factors that promote breastfeeding | Recommendation of initiating breastfeeding in early postpartum period | |
| Guidance on breastfeeding before discharge | ||
| Belief that breastfeeding is beneficial | ||
| Supervision of first feeding by health care professional | ||
| Influence of childbirth education classes | ||
| Factors that are barriers to breastfeeding | Insufficient milk supply | |
| Breast refusal | ||
| Maternal health problems | ||
| Health problems in infant | ||
| Breast problems | ||
| End of maternal leave | ||
| Dependent variables | Breastfeeding initiation | |
| Exclusive breastfeeding through age 6 months | ||
| Mixed breastfeeding at age 6 months | ||
| Maintenance of breastfeeding through age 1 year | ||
The study was approved by the Clinical Research Ethics Committee of La Coruña-Ferrol.
The statistical analysis of the data was carried out with the software IBM SPSS Statistics 24. We used the chi square (χ2) test or Fisher exact test for the bivariate analysis, and considered that variables were associated if the p-value was less than 0.05. We also performed a multivariate logistic regression analysis.
RESULTS
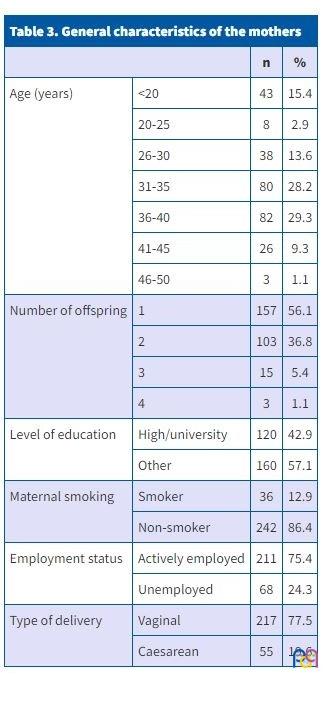
Maternal age was between 31-40 years in 57.9% of the 280 surveyed mothers, with a peak of 15.4% at 20 years. The mean number of offspring was 1.51 children (standard deviation, ± 0.65), which was maintained when we stratified the analysis by setting and health care area. As regards the mode of delivery, 19.6% of children were born by caesarean section. In terms of educational attainment and socioeconomic status, 42.9% of mothers had university degrees and 75.4% were actively employed (Table 3).
| Table 3. General characteristics of the mothers | |||
|---|---|---|---|
| n | % | ||
| Age (years) | <20 | 43 | 15.4 |
| 20-25 | 8 | 2.9 | |
| 26-30 | 38 | 13.6 | |
| 31-35 | 80 | 28.2 | |
| 36-40 | 82 | 29.3 | |
| 41-45 | 26 | 9.3 | |
| 46-50 | 3 | 1.1 | |
| Number of offspring | 1 | 157 | 56.1 |
| 2 | 103 | 36.8 | |
| 3 | 15 | 5.4 | |
| 4 | 3 | 1.1 | |
| Level of education | High/university | 120 | 42.9 |
| Other | 160 | 57.1 | |
| Maternal smoking | Smoker | 36 | 12.9 |
| Non-smoker | 242 | 86.4 | |
| Employment status | Actively employed | 211 | 75.4 |
| Unemployed | 68 | 24.3 | |
| Type of delivery | Vaginal | 217 | 77.5 |
| Caesarean | 55 | 19,6 | |
We found a rate of BF initiation after delivery of 85.3%, a rate of EBF6 of 47.2% and a rate of BF maintenance at 1 year of 38.9%. At the same time, 39.1% engaged in mixed feeding in the first 6 months of life. We found a higher prevalence of BF in urban settings (81.3%) compared to rural settings (70%).
When it came to BF maintenance at 1 year, we found that 38.9% of Galician mothers continued to breastfeed 1 year after BF initiation.
The rate of BF initiation was higher in mothers that received guidance during in the postpartum hospital stay (72.5% vs. 27.5%; p = 0.005) or at discharge (77.2% vs. 22.8%; p = 0.004), and in mothers whose first feeding was supervised by a health care professional (81.6% vs. 16.4%; p = 0.009).
We analysed the association of EBF6 with the aforementioned factors and with potential barriers, and found a statistically significant association of BF discontinuation with insufficient milk supply (p <0.01), the type of delivery (caesarean section) (p = 0.03) and maternal employment (p = 0.01) (Table 4).
| Table 4. Factors that promoted and hindered exclusive breastfeeding through age 6 months | ||||
|---|---|---|---|---|
| Breastfeeding (%) | No breastfeeding (%) | p | ||
| Factors that promoted exclusive breastfeeding through age 6 months | Guidance in hospital | 45.3 | 51.3 | 0.005 |
| Recommendation during hospital stay | 46.6 | 51.2 | 0.004 | |
| Supervision of first feeding | 47.1 | 46.9 | 0.009 | |
| Barriers to exclusive breastfeeding through age 6 months | Employment (actively employed) | 47.9 | 62.9 | 0.04 |
| Breast problems | 16.7 | 37.7 | 0.01 | |
| Type of delivery (caesarean) | 28.4 | 71.4 | 0.03 | |
| Breast/food refusal | 27.5 | 37.8 | 0.26 | |
| Insufficient milk supply | 12.3 | 46.3 | 0.00 | |

The factors identified as barriers to mixed breastfeeding and BF at 1 year post birth were a decreased milk supply, breast refusal and the end of maternal leave (p <0.01). Additional factors that limited BF at 1 year were active maternal employment (p <0.01) and maternal smoking during the pregnancy (p <0.05), factors that were also associated with EBF6. We ought to highlight the association between mixed feeding at 6 months (MF6) and having fed the infant formula during the hospital stay (p <0.05).
As regards geographical differences, the highest rate of BF corresponded to the province of Lugo (94.2%), and the lowest rates were found in the province of Orense.
As for setting, BF initiation was more frequent in rural settings (87.1%), after which the BF decreased in subsequent months (EBF6, 42%; BF at 1 year, 34.9%), contrary to urban settings, where BF initiation was less frequent at 83.5%, but the rates of EBF6 and BF at 1 year were higher (53% and 43.4%, respectively). We found higher frequencies of BF in urban settings in La Coruña and Vigo in both BF initiation and maintenance. However, in Lugo and Orense BF rates were higher in rural settings, except for EBF6 in Lugo, which was more frequent in the urban setting.
The logistic regression analysis showed that mothers who received guidance at the hospital or whose first feeding was supervised by a professional were 3.18 and 2.8 times more likely to initiate BF, respectively. Vaginal delivery was associated with a 2.44-fold increase in the probability of EBF6, and mothers with university degrees were 2.1 times more likely to maintain BF through age 1 year. However, bottle feeding in the first hours post birth was negatively associated with BF initiation (odds ratio [OR] 0.4). In addition, active maternal employment (OR 0.40; 0.19-0.84) or residence in a rural setting (OR 0.55; 0.27-0.93) were also factors negatively associated with EBF6.
We found that BF maintenance despite breast problems or after the end of maternity leave increased the likelihood of BF maintenance at 1 year post birth, with ORs of 16.2 and 16.5, respectively, and of EBF6 despite maternal health problems, with an OR of 9.42 (2.32-38.22).
DISCUSSION
In our study, we found a high prevalence of BF initiation in Galicia (85.3%), greater compared to the rates reported in neighbouring countries such as France (63%), Ireland (44%) or the United Kingdom (77%)27,28 and also the United States (76%)24 and different regions in Africa.22 However, it was lower compared to the rates reported in Italy (91.6%),29 the Nordic countries (100%)26 and Australia (90%).23 The prevalence we found could be due to adequate education of pregnant women regarding the significant benefits of BF and guidance on how to breastfeed.10
Comparing the prevalence found in our study to rates in other areas of Spain, we found that it was lower than the prevalence found in Catalonia (90.7%)30 or Madrid (88%),5 with higher percentages found in areas like Lugo (94.2%) and Vigo (91.3%). The prevalence in the province of Orense (73.9%) was similar to the prevalence found in the United States24 or the United Kingdom.27,28 Therefore, it is reasonable to state that the rate of BF initiation in Galicia is generally good, although there is still opportunity for improvement until reaching the 100% BF rate recommended by the WHO.
The prevalence of EBF6 in Galicia found in the study was 47.2%, 4 percentage points higher than the global prevalence found by the worldwide study conducted by UNICEF and lower compared to the prevalence observed in countries in South Asia (60%).22 It was very close to the 50% of EBF6 proposed as a global nutrition target for 2025.31 Compared to the rates reported in Australia (2%)23 and the United States (16%)24, the prevalence of EBF6 found in Galicia was much higher. In addition, it was higher than all the rates documented in other European countries: less than 20% in Nordic countries,27 less than 1% in the United Kingdom, 8 5.5% in Italy (in 2016).9 Although the rates of EBF6 found in most of the catchment areas under study were higher compared to the rest of the European Union, the prevalence in Orense (37.5%) was much lower than in the rest of Galicia, which suggest the need to implement more intensive interventions in this region. The data currently available for Spain show EBF6 rates lower than those found in Galicia: the 2017 NHS found a nationwide rate of 39%,10 the 2017 ELOIN study in the Community of Madrid a rate of 25.4%5 and a 2015 study conducted in Gipuzkoa a rate of 15.4%.11,14 In the Vigo area, we found a prevalence of EBF6 of 44.4%, below the prevalence found in a study conducted in the same area in 2017 (50.3%)19.
The prevalence of EBF6 in rural settings is lower, although in Galicia it is close to the global target.
There is a dearth of data from previous studies regarding the prevalence of BF at 1 year, but a study in Vigo (2017) found that 34.62% of mothers of babies aged 12 to 18 months continued to breastfeed,19 a prevalence that was similar to the prevalence found in our study in the same area (37.7%). A study conducted in Italy published in 2016 found a similar prevalence of BF at 1 year, 32.5%, slightly lower compared to the prevalence found in Galicia.29
Based on our findings, BF initiation in Galicia seems to be associated with the health care area and factors that may promote BF: encouragement to initiate BF in the hospital, guidance on BF or supervision by a health professional of the first feeding. In opposition, bottle feeding the baby at hospital was associated with a decrease in BF initiation. On the other hand, residence in La Coruña, Lugo and Vigo were associated with an increased probability of initiating BF compared to residence in Orense.
As regards BF maintenance, we found different associations: of EBF6 with the health care area, maternal employment, type of delivery and maternal smoking during pregnancy, among which we ought to highlight that active maternal employment decreases the probability of maintaining BF through age 6 months by nearly half (OR = 0.40), and therefore behaves as a barrier to BF. These findings were consistent with those of other studies conducted in Spain, such as the INMA study in Gipuzkoa.14 In contrast, vaginal delivery would promote BF, as it was associated with a more than 2-fold increase in the probability of EBF6. Supporting BF initiation in the hospital setting women that undergo a caesarean delivery would be beneficial, in addition to urging governmental institutions to promote a maternal leave system that would allow maintenance of EBF through 6 months post birth.
The pattern of BF maintenance through age 1 year is similar to the one of EBF6, as it is associated with current maternal employment and smoking. A higher educational attainment nearly doubles the probability of BF maintenance at 1 year, and greater support should be provided to first-time mothers and mothers of lower socioeconomic status, who are at increased risk of early BF discontinuation.14,32,33
The discontinuation of BF due to the mother returning to work evinces that the governmental intervention through work-life balance policies are necessary to reach the target established by the WHO. Other strategies could focus on providing more information and support through PC paediatricians to prevent potential reasons for BF discontinuation, such as food refusal or a low milk supply, that could be resolved by supporting mothers in achieving adequate BF technique.32,33
Lastly, we found that BF initiation was more frequent in rural compared to urban settings. However, the prevalence of EBF6 was higher in urban settings, and residence in a rural setting, interestingly, decreased the probability of maintaining EBF through age 6 months by half. Further studies are required to corroborate these findings and to identify potential limiting factors that could account for these differences.
In conclusion, the prevalence of BF found in our study was higher compared to other studies conducted in Spain and abroad and neared the global target for 2025 proposed by the WHO. Early interventions implemented at hospital and supervision of the first feeding could promote not only BF initiation but also its maintenance, and the support of primary care paediatricians is essential to address potential causes of BF discontinuation that could be avoided, such as food refusal or an insufficient milk supply, both of which, in some cases, can be resolved by achieving adequate BF technique.
Limitations: the study design, with the use of an anonymous questionnaire in a non-random sample, entails a risk of selection bias that would likely result in overestimation of BF rates, as it is reasonable to assume that women that continued to breastfeed for at least 6 months would be more willing to complete the questionnaire. In addition, the anonymous completion of the questionnaire precluded proactive interviewing of women that chose not to respond to assess whether they differed or not from those who did. In any case, given the agreement of our findings with those of other studies and the fact that the study was conducted in multiple centres distributed throughout Galicia, we expect that its external validity has not been affected.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to disclose in relation to the preparation and publication of this article.
ABBREVIATIONS
BF: breastfeeding · EBF6: exclusive breastfeeding until age 6 months · MF6: mixed feeding at age 6 months · NHS: National Health Survey · OR: odds ratio · PC: Primary Care.
REFERENCES
- Leung AKC, Sauve RS. Breast is best for babies. J Natl Med Assoc. 2005;97:1010-9.
- González JL, Valls T, Mosquera E, Herranz M, López Y, Sanromán MJ, et al. Estudio sobre la prevalencia de la lactancia materna en los centros de salud de Val Miñor. Rev Pediatr Aten Primaria. 2008;10:603-16.
- Turck D. Breast feeding: health benefits for child and mother. Arch Pediatrie. 2005;12:14565.
- Lawrence RM, Pane CA. Human breast milk: current concepts of immunology and infectious diseases. Curr Probl Pediatr Adolesc Health Care. 2007;37:7-36.
- Ramiro MD, Ortiz H, Arana C, Esparza MJ, Cortés O, Terol M, et al. Prevalencia de la lactancia materna y factores asociados con el inicio y la duración de la lactancia materna exclusiva en la Comunidad de Madrid entre los participantes en el estudio ELOIN. An Pediatr (Barc). 2018;89:32-43.
- Ip S, Chung M, Raman G, Chew P, Magula N, DeVine D, et al. Breastfeeding and maternal and infant health outcomes in developed countries. Evid Rep Technol Assess (Full Rep). 2007;153:1-186.
- Horta BL, Loret de Mola C, Victoria CG. Breastfeeding and intelligence: A systematic review and meta-analysis. Acta Paediatr. 2015;104:14-9.
- Victora CG, Bahl R, Barros AJD, França GVA, Horton S, Krasevec J, et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387:475-90.
- Bellantuono C, Migliarese G, Maggioni F, Imperadore G. Antidepressant drugs and breastfeeding. Recenti Prod Med. 2007;98:2942.
- Recomendaciones para la Lactancia Materna. In: Asociación Española de Pediatría (2005). Comité de Lactancia Materna [online] [accessed 06/06/2022]. Available at www.aeped.es
- Pallás CR. Lactancia materna. Rev Pediatr Aten Primaria. 2003;5:69-88.
- Rodicio MM, Abadi A, Silveira M, Rodríguez MJ, Andrés A, Vázquez M. Trends and course of breastfeeding in the north of Lugo, Spain. Acta Pediatr Esp. 2007;65:6-11.
- Esteves TRB, Daumas RP, Oliveira MI, Andrade CA, Leite IC. Factors associated to breastfeeding in the first hour of life: Systematic review. Rev Saude Publica. 2014;48:697-708.
- Oribe M, Lertxundi A, Basterrechea M, Begiristain H, Santa Marina l, Villa M, et al. Prevalencia y factores asociados con la duración de la lactancia materna exclusiva durante los 6 primeros meses en la cohorte INMA de Guipúzcoa. Gac Sanit. 2015;29:4-9.
- Sacristán AM, Lozano JE, Gil M, Vega AT. Situación actual y factores que condicionan la lactancia materna en Castilla y León. Rev Pediatr Aten Primaria. 2011;13:33-46.
- Narramore N. Supporting breastfeeding mothers on children’s wards: an overview. Paediatr Nurs. 2007;19:18-21.
- Pallás C, Soriano J, Grupo PrevInfad. Apoyo a la Lactancia Materna en atención Primaria. In: Previnfad [online] [accessed 06/06/2022]. Available at http://previnfad.aepap.org/monografia/lactancia-materna#introduccion
- Management of breast conditions and other breastfeeding difficulties. World Health Organization. 2009.
- Rodríguez-Pérez MJ. Prevalencia de lactancia materna en el área sanitaria de Vigo, Galicia. Rev Esp Salud Pública. 2017;91:e1-e9.
- Lactancia Materna en cifras: Tasas de inicio y duración de la lactancia en España y en otros países. In: Comité de Lactancia Materna de la Asociación Española de Pediatría [online] [accessed 08/08/2022]. Available at www.aeped.es
- Victora CG, Horta BL, de Mola CL, Quevedo l, Pinheiro RT, Gigante DP, et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387(10017):475-90.
- From the first hour of life: Making the case for improved infant and young child feeding everywhere. In: United Nations Children’s Fund UNICEF. October 2016 ISBN: 978-92-806-48522 [online] [accessed 06/06/2022]. Available at http://data.unicef.org/resources/first-hour-life-new-report-breastfeedingpractices/
- National Infant Feeding Survey: 2010. Australian National Infant Feeding Survey: Indicator Results. In: Canberra: Australian Institute of Health and Welfare, 2011 [online] [accessed 06/06/2022]. Available at www.aihw.gov.au/publication-detail/?id=10737420927
- Breastfeeding report card-United States 2013. In: Centers for Disease Control and Prevention [online] [accessed 06/06/2022]. Available at www.cdc.gov/breastfeeding/data/reportcard.htm
- Hunt F. Breast feeding and society. Paediatr Nurse. 2006;18:24-6.
- Baerug A, Bjoerneboe G, Tufte E, Forum KR. Implementation of the WHO multicentre growth reference study in Norway. Food Nutr Bull. 2004;25:S72-S77.
- CO1.5: Breastfeeding rates OECD Family database. In: OECD - Social Policy Division - Directorate of Employment, Labour and Social Affairs [online] [accessed 06/06/2022]. Available at www.oecd.org/els/family/43136964.pdf
- Black l-A. Research and Information Service briefing paper: Breastfeeding rates. In: North Ireland Assembly, NIAR Publication number 392-11. 2011 [online] [accessed 06/06/2022]. Available at www.niassembly.gov.uk/Documents/RaISe/Publications/2011/Health/14811.pdf
- Lauria l, Spinelli A, Grandolfo M. Prevalence of breastfeeding in Italy: a population based follow-up study. Ann Ist Super Sanita. 2016, 52(3):457-61.
- Encuesta Nacional de Salud. In: Instituto Nacional de Estadística, 2006 [online] [accessed 08/06/2022]. Available at www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176783&menu=resultados&idp=1254735573175
- Ortiz-Marrón H, Cuadrado-Gamarra JJ, Vasallo ME, Cortés-Rico O, Sánchez-Díaz J, Galán-Labaca I, et al. Estudio Longitudinal de Obesidad Infantil (ELOIN): Diseño, participación y características de la muestra. Rev Esp Cardiol. 2016;69:521-3.
- Comprehensive Implementation Plan on Maternal Infant and Young Child Nutritional. In: World Health Organization 2014 [online] [accessed 06/06/2022]. Available at http://apps.who.int/iris/bitstream/10665/113048/1/WHO_NMH_NHD_14.1_eng.pdf?ua=1
- Ruowei l, Fein SB, Chen J, Grummer-Strawn LM. Why Mothers Stop Breastfeeding: Mothers’ Self-reported Reasons for Stopping During the First Year. Pediatrics. 2008;122:S69-76