

Analysis of child temperament in relation to screen use
Josep Oriol Casanovas Marsala, Diana Merino Leivab, Andrea Paúl Nadalb, Marina Cruz Leivab, Esther Aladrén Hernandob, Delia González de la Cuestac
aEnfermero. Hospital Universitario Miguel Servet. Instituto de Investigación Sanitaria Aragón. Zaragoza. España.
bEspecialista en Enfermería Pediátrica. Hospital Universitario Miguel Servet. Zaragoza. España.
cEnfermera. Área de Innovación e Investigación. Hospital Universitario Miguel Servet. Instituto de Investigación Sanitaria Aragón. Zaragoza. España.
Correspondence: JO Casanovas. E-mail: jocasanovas@iisaragon.es
Reference of this article: Casanovas Marsal JO, Merino Leiva D, Paúl Nadal A, Cruz Leiva M, Aladrén Hernando E, González de la Cuesta D. Analysis of child temperament in relation to screen use. Rev Pediatr Aten Primaria. 2022;24:e45-e51.
Published in Internet: 12-04-2022 - Visits: 15665
Abstract
Introduction: the aim of this study was to describe the screen time in children and analyse its association with personality traits and behaviour.
Methods: observational and descriptive study through a structured, self-administered questionnaire completed by parents to assess screen time in their children and the Emotionality, Activity and Sociability (EAS) questionnaire to assess traits and behaviours in children aged 0 to 10 years in the caseloads of the Revolería and Torrero-La Paz primary care centres in Zaragoza (Spain) between June 2019 and February 2020. Research Ethics Committee of the Autonomous Community of Aragón (PI 19/00260).
Results: the sample included 212 children, 54.1% female. The mean age was 5.3 ± 2.7 years; the mean weight 21.2 ± 9.6 kg, the mean height 1.1 ± 0.2 m, and 62.9% had a normal weight. Of the total, 76.1% reported physical activity. The age at which exposure to screens started was greater than 24 months in 39%; and 42.4% used screens between 60 and 120 minutes on average. The assessment of traits with the EAS survey yielded the following mean scores: sociability, 18.1 ± 3.1; activity, 19.0 ± 4.2; emotionality, 13.9 ± 4.04; shyness, 12.3 ± 4.1.
Conclusion: in the sample under study, screen time and use were greater in older children. There were no statistically significant differences in screen time associated with differences in temperament.
Keywords
● Child behaviour ● Information technologies ● Psychological dependency ● TemperamentINTRODUCTION
The presence of information and communication technology (ICT) has become the norm1 in children’s lives and defines them as digital natives growing in a digitalized society that quickly learn how to handle computers, tablets and mobile phones.2,3 Teaching methods, games, entertainment and the ways to communicate have changed, raising controversy among experts as to the medium- to long-term benefits and possible impact of these changes.4-6
Based on data from the National Health Survey of Spain of 2017,7 57% of children aged 1-4 years spend more than 1 hour a day during the week using screens, and this percentage rises to 76.1% in the 5-9 years age group and to up to 83.7% in the 10-14 years group, thus exceeding the current screen time recommendations of the American Academy of Pediatrics (AAP).8
Anxiety and low self-esteem, the deterioration of social relationships and a low frustration tolerance are associated with excessive use of new technologies in adolescents. However, their use in younger age groups has not been studied in the same detail. It would be interesting to determine when screen time could be considered excessive and even become an addiction.9,10 Three levels of dependency have been described11: a) adequately controlled use: the daily activities and leisure of the individual re not affected by the use of ICTs; b) moderately controlled use: there is an excessive interest in ICTs to the detriment of other interests or personal relationships with individuals that do not partake in the same activities and there may be incipient behavioural changes, and c) excessive and addictive use: all other activities in life are relegated to the background, the individual only finds satisfaction in activities involving ICTs and the change in social behaviour is patent and pathological.
The AAP offers recommendations regarding the settings and timeframes in which screens should be absent and also reflects on the content: there is an emphasis on the importance of adult supervision and adherence to the recommended age limits of contents.12,13
When a habit turns into an addition there is a change in social behaviour, and this is more likely to happen in individuals with an introverted personality, impulsivity traits,13 depression, low self-esteem, social anxiety or shyness.12,14 On the other hand, friendliness and high self-esteem may have a protective effect.13
The transition from a hobby to an addiction manifests with shorter sleep duration, the neglect of family and social relationships, a fixation on ICTs as the sole source of entertainment, excessive irritation when the use of ICTs is withheld, poor academic performance and excessive euphoria in the presence of emerging technologies.12
The identification of changes in personality traits (sociability, shyness, emotionality and activity) in children could contribute to the prevention of addiction to technology through interventions delivered by parents and educators. The aim of our study was to describe screen use and its association with personality traits and behaviour in children.
MATERIAL AND METHODS
We conducted an observational and descriptive study by means of a structured questionnaire for parents from June 2019 to February 2020. We assessed the traits of children through the Emotionality, Activity and Sociability (EAS) temperament questionnaire (adapted version in Spanish).15 The sample consisted of children of both ages aged 0 to 10 years in the catchment populations of the Rebolería and the Torrero-La Paz primary care centres in the city of Zaragoza (Spain). We excluded children with chronic diseases that affected psychomotor development, required frequent hospitalization or impaired their comprehension or communication skills, impeding participation.
Patients were recruited and participated in the study through the primary care paediatrics clinics of participating centres. The nurse in charge informed parents of the study and, if they consented to participate, they were given a questionnaire for self-administration consisting of 13 items to collect data on the child, including age, sex, height, weight and total number of siblings, type of family (two-parent, single parent, separated, blended and extended), usual caregiver (mother, father, both), extracurricular activities unrelated to the use of screens with the hours a week spent in these activities and physical activity with the hours a week spent in physical activity.
When it came to the use of screens, we asked parents the age at which the child started to be exposed to screens, the daily screen time, the contents consumed, the devices used (tablet, mobile phone, computer, television and/or console), the timing of screen exposure (during meals, trips, leisure time, before sleep, at school etc), the tolerance exhibited by the child when the device is taken away, which was categorised as very good (never gets upset, does not mind), good (does not usually get upset but may need to be distracted), fair (accepts the limit but tends to get upset), poor (always gets upset) and very poor (gets angry, resists the withholding of device, screams, cries or kicks) and whether the parent considered the screen use of the child problematic.
To assess the temperament of the child, parents were provided with a scale designed to assess traits in children (EAS) translated to Spanish and validated in the Spanish population.15 The scale is a self-administered questionnaire about behaviour in the child completed by a parent. It comprises 20 items rated on a Likert scale, with 1 corresponding to an observable behaviour that is very uncharacteristic in the child and 5 an observable behaviour that is very typical in the child. Each of the domains of the questionnaire is assessed by means of 5 items, and there are a total of 6 reverse items in the scale. The score for the reverse items is calculated with the following formula:
Sr = (Sm + 1) – S0
Where Sr is the transformed score for the reverse item that is ready to be used in the calculation of the total score for the questionnaire, Sm the maximum score that can be given for the item and S0 the original score for the item. The 20 items of the questionnaire measure 3 basic dimensions of temperament in the child: emotionality, activity and sociability, with the latter further subdivided into sociability and shyness.
The analysis of the data was performed with the software JAMOVI® version 1.2.7. In the descriptive analysis, we summarised quantitative variables as mean and standard deviation and qualitative variables as frequency and percentage distributions. We assessed the goodness of fit to the normal distribution of quantitative variables with the Shapiro-Wilk test. To assess the association between variables, we performed hypothesis tests comparing proportion in the case of 2 qualitative variables, means when one of the variables was quantitative (Kruskal-Wallis) and bivariate correlation tests when both were quantitative (Spearman correlation coefficient). We considered results significant if p <0.05.
As concerns ethical considerations, data collection adhered to current legislation on the subject of confidentiality (Organic Law 3/2018, of 5 December, on the Protection of Personal Data and Guaranteeing Digital Rights). The consent process consisted of providing a description, verbally and in writing, of all the information related to the study and its objectives (informative sheet for participants and parents/legal guardians), obtaining consent to participation on a voluntary basis through the signing of an informed consent form. The study adhered to national and international ethical principles (medical ethics code, Declaration of Helsinki). The study was approved by the Research Ethics Committee of the Autonomous Community of Aragón under file code PI 19/00260.
RESULTS
The total sample included 212 children (54.1% were female and 45.9% male) with a mean age of 5.3 ± 2.7 years, a mean weight of 21.2 ± 9.6 kg and a mean height of 1.11 ± 0.20 m. The distribution by weight status was 10.6% underweight, 62.9% normal weight, 13.6% overweight and 12.9% obese. The distribution by family category was: 86.4% two-parent, 6.1% blended, 3.3% separated, 2.3% single-parent and 1.9% extended. Single children accounted for 24.9% of the sample, while 75.1% had at least 1 sibling, and most had both parents as primary caregivers (43.2%). When it came to extracurricular activities unrelated to screen use, we found that 63.4% engaged in such activities and 76.1% in physical activity.
The age at initiation of exposure to screens was greater than 24 months in 39% of the cases, between 12 and 24 months in 35.1%, between 6 and 12 months in 22.4% and before 6 months in 3.4%.
As for screen time, we found that 42.4% used screens between 60 and 120 minutes during the week, 40.5% less than 30 minutes, 11% between 120 and 180 minutes, 3.3% were not exposed to screens and 2.9% used them more than 180 minutes. We found that school-aged children were the largest group that used screens between 60 and 120 minutes (Table 1).
| Table 1. Screen time by age group | |||||||
|---|---|---|---|---|---|---|---|
| Age | Screen time | Total | |||||
| None | <30 min | 60-120 min | 120-180 min | >180 min | |||
| Infancy | Observed value | 5.0 | 12.0 | 2.0 | 1.0 | 0.0 | 20.0 |
| Expected value | 0.7 | 8.1 | 8.5 | 2.2 | 0.6 | 20.0 | |
| % row | 25.0 | 60.0 | 10.0 | 5.0 | 0.0 | 100.0 | |
| % column | 71.4 | 14.1 | 2.2 | 4.3 | 0.0 | 9.5 | |
| % total | 2.4 | 5.7 | 1.0 | 0.5 | 0.0 | 9.5 | |
| Early childhood | Observed value | 2.0 | 40.0 | 41.0 | 8.0 | 2.0 | 93.0 |
| Expected value | 3.1 | 37.6 | 39.4 | 10.2 | 2.7 | 93.0 | |
| % row | 2.2 | 43.0 | 44.1 | 8.6 | 2.2 | 100.0 | |
| % column | 28.6 | 47.1 | 46.1 | 34.8 | 33.3 | 44.3 | |
| % total | 1.0 | 19.0 | 19.5 | 3.8 | 1.0 | 44.3 | |
| School age | Observed value | 0.0 | 33.0 | 46.0 | 14.0 | 4.0 | 97.0 |
| Expected value | 3.2 | 39.3 | 41.1 | 10.6 | 2.8 | 97.0 | |
| % row | 0.0 | 34.0 | 47.4 | 14.4 | 4.1 | 100.0 | |
| % column | 0.0 | 38.8 | 51.7 | 60.9 | 66.7 | 46.2 | |
| % total | 0.0 | 15.7 | 21.9 | 6.7 | 1.9 | 46.2 | |
| Total | Observed value | 7.0 | 85.0 | 89.0 | 23.0 | 6.0 | 210.0 |
| Expected value | 7.0 | 85.0 | 89.0 | 23.0 | 6.0 | 210.0 | |
| % row | 3.3 | 40.5 | 42.4 | 11.0 | 2.9 | 100.0 | |
| % column | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | |
| % total | 3.3 | 40.5 | 42.4 | 11.0 | 2.9 | 100.0 | |
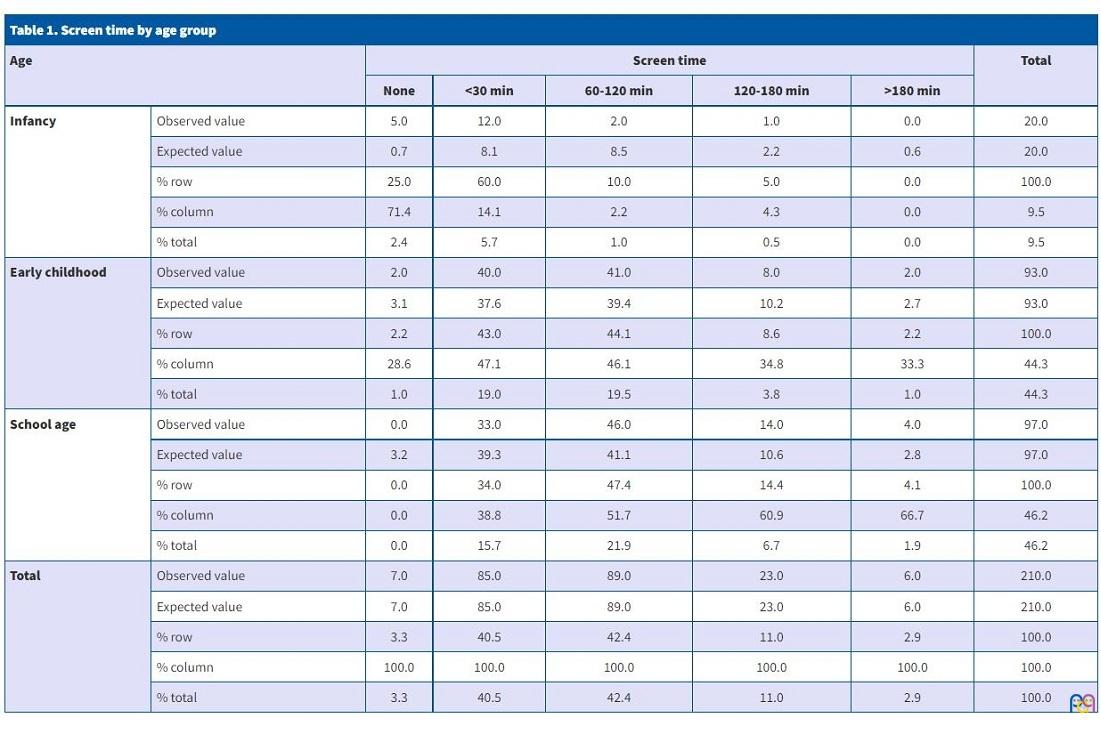
Movies were the type of content consumed most frequently (66%) and televisions the most widely used device (43.4%). Screens were never used to induce sleep in 83.6% of cases and 58.9% of parents did not think the reaction of the child to having the device removed was problematic, with 58.9% reporting the child never getting upset or sometimes needing a distraction to not becoming upset.
In the assessment of temperament using the EAS questionnaire, the mean scores in the different dimensions were 18.10 ± 3.17 for sociability (range 7-25), 19.0 ±4.2 for activity (range 5-25), 13.9 ± 4.0 for emotionality (range 6-24) and 12.3 ± 4.1 for shyness (range 5-22).
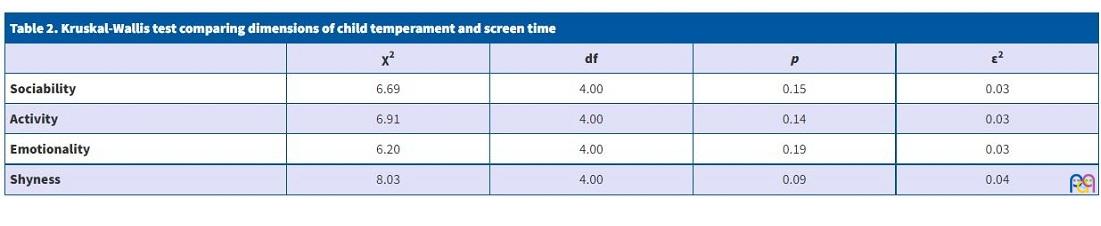
The analysis did not reveal statistically significant differences in screen time in relation to sex (χ² = 3.98; p = 0.41), the sociability score (χ² = 6.69; p = 0.15), the activity score (χ² = 6.9; p = 0.1), the emotionality score (χ² = 6.2; p = 0.2) or the shyness score (χ² = 8.03; p = 0.1) (Table 2).
| Table 2. Kruskal-Wallis test comparing dimensions of child temperament and screen time | ||||
|---|---|---|---|---|
| χ2 | df | p | ε2 | |
| Sociability | 6.69 | 4.00 | 0.15 | 0.03 |
| Activity | 6.91 | 4.00 | 0.14 | 0.03 |
| Emotionality | 6.20 | 4.00 | 0.19 | 0.03 |
| Shyness | 8.03 | 4.00 | 0.09 | 0.04 |
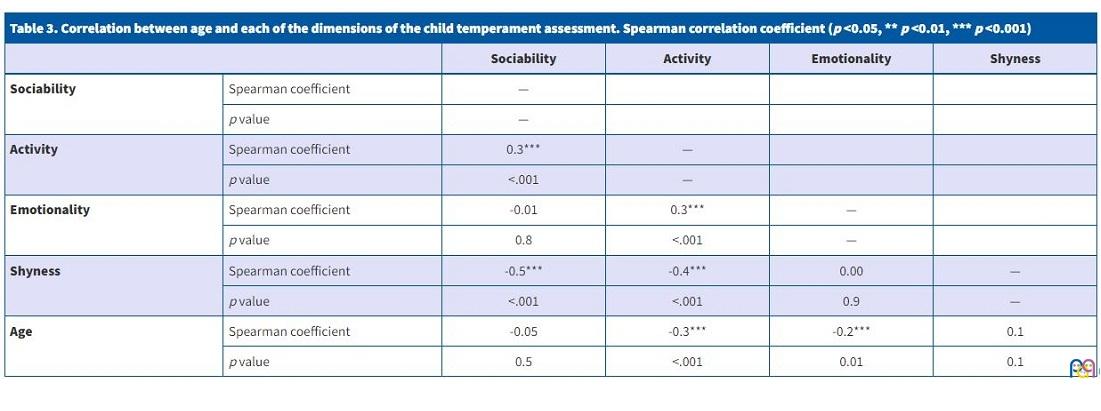
However, we found that age was mildly and directly correlated to the activity score and mildly and inversely correlated to the emotionality score (Table 3).
| Table 3. Correlation between age and each of the dimensions of the child temperament assessment. Spearman correlation coefficient (p <0.05, ** p <0.01, *** p <0.001) | |||||
|---|---|---|---|---|---|
| Sociability | Activity | Emotionality | Shyness | ||
| Sociability | Spearman coefficient | — | |||
| p value | — | ||||
| Activity | Spearman coefficient | 0.3*** | — | ||
| p value | <.001 | — | |||
| Emotionality | Spearman coefficient | -0.01 | 0.3*** | — | |
| p value | 0.8 | <.001 | — | ||
| Shyness | Spearman coefficient | -0.5*** | -0.4*** | 0.00 | — |
| p value | <.001 | <.001 | 0.9 | — | |
| Age | Spearman coefficient | -0.05 | -0.3*** | -0.2*** | 0.1 |
| p value | 0.5 | <.001 | 0.01 | 0.1 | |
We found statistically significant differences in the dimensions of activity (χ² = 5.83; p = 0.02) and emotionality (χ² = 4.3; p = 0.04), with girls obtaining higher scores in both compared to boys (activity, 19.6 ± 4.5 vs. 18.1 ± 4.0; emotionality, 14.5 ± 3.9 vs. 13.1 ± 3.9).
DISCUSSION
The results of our study show that most of the sample used screens for more than 1 hour a day. The AAP8 recommends limiting the use of screens to less than 1 hour a day and establishes different maximum screen time intervals based on age, recommending no exposure at all for children 0-2 years, between half and one hour a day for children 2-5 years, an hour under adult supervision and never during meals in children 7-12 years, an hour and a half in children 12 to 15 years being particularly mindful of social media and 2 hours for adolescents 16 years and older.
As regards age, we found that screen time increased with increasing age in our sample. As screen time increases, so does the probability of developing addition16 and experiencing symptoms of attention-deficit hyperactivity disorder, conduct disorder, depression, anxiety and changes in sleep patterns.12,14,16,17
As regards physical activity, in our sample we found an inverse correlation between screen and physical activity.19
Although the sample was obtained in an urban population, previous studies have described a higher screen time in the rural versus the urban population.20
When it came to screen time, we considered that the use of screens was adequately controlled if it did not have an impact on daily life activities or leisure activities outside the use of screens, that it was moderately controlled if the child exhibited an excessive interest in screens to the detriment of other activities and relationships with individuals that did not partake in the same screen-based activities with incipient changes in behaviour, and that use was excessive or addictive if all other life activities were relegated to the background, the child only experienced satisfaction with screen-related activities and changes in social behaviour were patent and problematic.11
Scales to detect addiction to screen use21 are useful tools for the purpose of establishing criteria for identification and, if applicable, resolution of the problem.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to disclose.
ABBREVIATIONS
AAP: American Academy of Pediatrics · EAS: Emotionality Activity Sociability questionnaire · ICT: information and communication technology.
REFERENCES
- Instituto Nacional de Estadística. Encuesta sobre equipamiento y uso de tecnologías de información y comunicación en los hogares. In: Instituto Nacional de Estadística. 2019;1-12 [online] [accessed 18/03/2022] Available at: www.ine.es/prensa/tich_2019.pdf
- İnal EE, Demİrcİ K, Çetİntürk A, Akgönül M, Savaş S. Effects of smartphone overuse on hand function, pinch strength, and the median nerve. Muscle Nerve. 2015;52:183-8.
- Muñoz-Miralles R, Ortega-González R, López-Morón MR, Batalla-Martínez C, Manresa JM, Montellà-Jordana N, et al. The problematic use of Information and Communication Technologies (ICT) in adolescents by the cross sectional JOIICTs study. BMC Pediatr. 2016;16:140.
- Víquez Barrantes I. Las ICTs en la educación inclusiva e influencia en el aprendizaje de preescolares. In: Congreso Iberoamericano de Ciencia, Tecnología, Innovación y Educación. Buenos Aires; 2014 [online] [accessed 18/03/2022] Available at: https://studylib.es/doc/5491141/las-tic-en-la-educaci%C3%B3n-inclusiva-e-influencia-en-el
- Casanova Correa J, González Pérez A. Educación Inclusiva y otros afines para el desarrollo de una escuela para todos en la sociedad de la información. Rev Educ Artes e Inclusão. 2010;3(1):1-18.
- Vara Robles E, Pons Grau R, Lajara Latorre F, Molina S, Villarejo Romera V, Planas Sanz E. Impacto del abuso de pantallas sobre el desarrollo mental. Rev Pediatría Aten Primaria. 2009;11:413-23.
- Ministerio de Sanidad, Consumo y Bienestar Social. Encuesta nacional de Salud. España 2017. In: Ministerio de Sanidad, Consumo y Bienestar Social [online] [accessed 18/03/2022] Available at: www.sanidad.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2017/ENSE17_pres_web.pdf
- Council on Comumunications and Media. Media and Young Minda. Pediatrics. 2016;138:e20162591.
- Sevelko K, Bischof G, Bischof A, Besser B, John U, Meyer C, et al. The role of self-esteem in Internet addiction within the context of comorbid mental disorders: Findings from a general population-based sample. J Behav Addict. 2018;7:976-84.
- Tresáncoras A, García-Oliva C, Piqueras JA. Relación del uso problemático de Whatsapp con la ansiedad y personalidad en adolescentes. Heal Addict Salud y Drog. 2017;17:27-36.
- Hernan Ruiz M. Adolescente y nuevas adicciones. Rev Asoc Esp Neuropsiq. 2015;35:309-22.
- Cía AH. Las adicciones no relacionadas a sustancias (DSM-5, APA, 2013): un primer paso hacia la inclusión de las Adicciones Conductuales en las clasificaciones categoriales vigentes. Rev Neuropsiquiatr. 2013;76:210-7.
- Puerta-Cortés DX, Carbonell X. El modelo de los cinco grandes factores de personalidad y el uso problemático de Internet en jóvenes colombianos. Addicciones. 2014;26:56-61.
- Echeburúa E, de Corral P. Adicción a las nuevas tecnologías y a las redes sociales en jóvenes: un nuevo reto. Adicciones. 2010;22:91-5.
- Bobes Bascarán MT, Jover M, Llácer B, Carot JM, Sanjuan J. Adaptación española del EAS Temperament Survey para la evaluación del temperamento infantil. Psicothema. 2011;23:160-6.
- Wichstrøm L, Stenseng F, Belsky J, von Soest T, Hygen BW. Symptoms of Internet Gaming Disorder in Youth: Predictors and Comorbidity. J Abnorm Child Psychol. 2019;47:71-83.
- Hu Y, Long X, Lyu H, Zhou Y, Chen J. Alterations in white matter integrity in young adults with smartphone dependence. Front Hum Neurosci. 2017;11:532.
- Tatum WO, DiCiaccio B, Yelvington KH. Cortical processing during smartphone text messaging. Epilepsy Behav. 2016;59:117-21.
- Zagalaz-Sánchez ML, Cachón-Zagalaz J, Sánchez-Zafra M, Lara-Sánchez A. Mini review of the use of the mobile phone and its repercussion in the deficit of physical activity. Front Psychol. 2019;10:1307.
- Jamir L, Duggal M, Nehra R, Singh P, Grover S. Epidemiology of technology addiction among school students in rural India. Asian J Psychiatr. 2019;40:30-8.
- Harris B, Regan T, Schueler J, Fields SA. Problematic mobile phone and smartphone use scales: a systematic review. Front Psychol. 2020;11:672.