

Association between indicators of neighbourhood socioeconomic status in Seville and the incidence of pertussis and related hospital admissions in children
Sebastián Tornero Patricioa, Liliana Charris Castrob, Pedro Terol Barreroc, Manuel Praena Crespod, Antonio Daponte Codinae
aPediatra. Dirección Médica del Área de Gestión Sanitaria Osuna. Servicio Andaluz de Salud. Hospital La Merced. Osuna. Sevilla. España.
bMédico. Unidad de Cuidados Intensivos. Hospital General de Riotinto. Servicio Andaluz de Salud. Huelva. España.
cPediatra. Sección de Infectología Pediátrica. UGC de Pediatría. Hospital Universitario Virgen Macarena. Servicio Andaluz de Salud. Sevilla. España.
dPediatra. CS La Candelaria. Sevilla. España.
eCiber de Epidemiología y Salud Pública (CIBERESP). Observatorio de Salud y Medio Ambiente de Andalucía (OSMAN). Escuela Andaluza de Salud Pública. Campus Universitario de la Cartuja. Granada. España.
Correspondence: S Tornero. E-mail: sebastian.tornero.sspa@juntadeandalucia.es
Reference of this article: Tornero Patricio S, Charris Castro L, Terol Barrero P, Praena Crespo M, Daponte Codina A. Association between indicators of neighbourhood socioeconomic status in Seville and the incidence of pertussis and related hospital admissions in children. Rev Pediatr Aten Primaria. 2021;23:e81-e92.
Published in Internet: 28-04-2021 - Visits: 14168
Abstract
Introduction: the aim of our study was to analyse the association between the SES of the neighbourhood of residence and the incidence of pertussis and frequency of hospital visits associated with pertussis in the paediatric population.
Material and methods: we conducted a cross-sectional observational study, with 2 sets of observations in children under 15 years living in Seville: 1) admissions for any reason to the 2 public hospitals of Seville (2013-2015; n = 7315) and 2) reported cases of pertussis (2013-2017; n = 102). The independent variables were age, sex and residence in areas in need of social transformation (ANSTs), areas at risk of poverty (ARPs) and areas with low educational attainment (ALEAs). In the analysis of the reported cases data set, we calculated the incidence and incidence ratio for each subdistrict.
Results: of the total hospital admissions, 1.12% (n = 82) were due to pertussis. Between 2.0 and 2.4% of admissions in children that resided in disadvantaged subdistricts were due to pertussis, compared to 0.8 to 0.9% in children living in the rest of the city (p <0.001). The sex- and age-adjusted odds ratios (with their corresponding 95% confidence intervals) were: ANST 2.76 (1.74-4.32) for ANSTs, 2.48 (1.47-4.04) for ARPs and 2.17 (1.38-3.39) for ALEAs. The incidence ratios were also higher in these disadvantaged areas (2.50, 1.99 and 2.01, respectively).
Conclusions: low neighbourhood socioeconomic status in Seville was associated with a higher incidence of pertussis and a higher frequency of related hospital admissions in the paediatric population.
Keywords
● Areas of poverty ● Education status ● Social determinants of health ● Social inequity ● Socioeconomic factors ● Whooping coughINTRODUCTION
Pertussis is an endemic disease that exhibits incidence peaks every 2 to 5 years.1 Reinfection is frequent in adults and manifests with mild symptoms, becoming a source of transmission mainly to children, who develop more severe forms of disease.1-3 As has been observed in other countries, there has been an increase in the number of cases in Spain since 2010. 1,2,4,5 Still, it is believed that the incidence of pertussis is underestimated.1-3,6 The reported incidence in 2017 was of 9.4 cases per 105 inhabitants in Europe and 8.7cases per 105 inhabitants in Spain,7 which a higher incidence in infants aged less than 1 year.8 The last outbreak of pertussis in Andalusia took place in the 2011-2016 period, with the incidence peaking in 2016 at 11.4 cases per 105 inhabitants with a subsequent descent to 2.7 cases per 105 inhabitants in 20189. Following the introduction of the strategy of vaccinating pregnant women in 2015, the incidence in infants started showing a significant decline.9,10
Poor socioeconomic conditions, weaknesses in health care systems and difficulties accessing universal vaccination programmes may justify the increase in the incidence of pertussis in some countries.1,6 A multicentre systematic review conducted in several countries11 evinced an association between economic recessions and increases in infectious diseases in the most vulnerable groups of the population. The latest economic crisis has promoted risk factors associated with the increase in the incidence of pertussis, such as unemployment, poverty and social exclusion.12,13 Crowding is a proven risk factor for pertussis,14 as it facilitates transmission between household and/or family members, who are the main source of transmission in 36% to 67% of cases, depending on the study.15-17 Although a study of 1791 cases of pertussis in Barcelona did not find differences in incidence in the periods before and after the recent economic crisis, it did find an association between higher incidence and residence in the most disadvantaged neighbourhoods of the city.5
In epidemiological studies, the neighbourhood socioeconomic status (SES) is frequently used as an indicator of the SES of households located in that area. It is usually estimated based on census data for variables such as educational attainment, employment status, occupation, housing characteristics, etc.18-20 Some studies conducted in Spain have found an association between SES and the incidence or prevalence of infectious diseases such as tuberculosis,21 but few studies other than the one conducted in Barcelona mentioned above5 have assessed the association between the SES of the area of residence and the frequency of hospital visits due to pertussis in the paediatric population. The aim of our study was to analyse the association between the SES of the area of residence, established based on poverty, social exclusion and educational attainment, and the incidence of pertussis and frequency of hospital visits associated with pertussis in the paediatric population of Seville, Spain.
MATERIAL AND METHODS
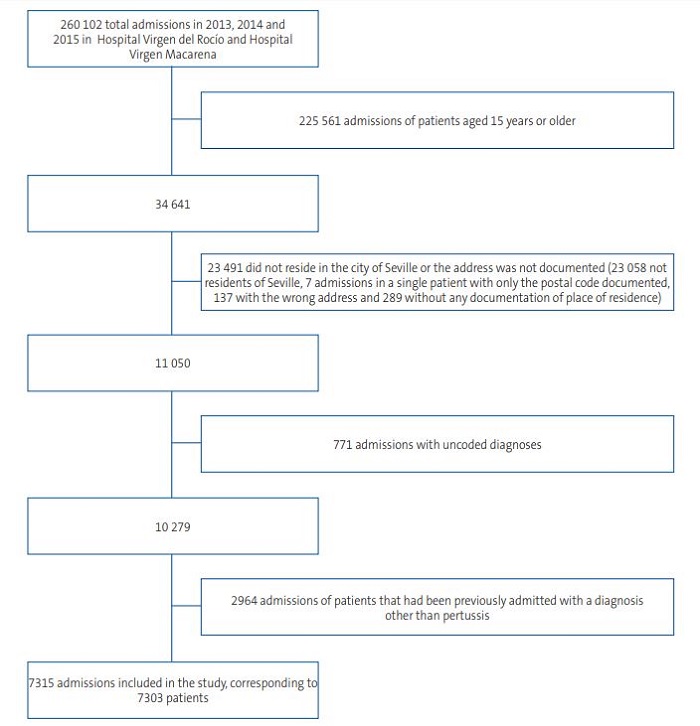
We conducted a cross-sectional observational study of the hospital admissions and reported cases of pertussis in children that resided in the city of Seville. There were 2 sets of observations: hospital admissions and reported cases. The main set corresponded to hospital admissions, which included admissions of children aged less than 15 years for any reason in either of the 2 public referral hospitals in the city of Seville (Hospital Virgen del Rocío and Hospital Virgen Macarena) between 01/01/2013 and 31/12/2015, with the hospitalization episode coded by 01/01/2016. The exclusion criteria were: residence outside the municipality of Seville or not documented, episodes without a primary diagnosis code and episodes corresponding to readmission, unless the reason for readmission was pertussis (Figure 1). Of the 433 episodes excluded due to absence of a documented address, 1 corresponded to a case of pertussis. After applying these criteria, the hospital admission data set included 7315 hospitalizations corresponding to 7303 patients, of which 82 admissions were due to pertussis.
| Figure 1. Flowchart of the hospital admission observation set |
|---|
 |
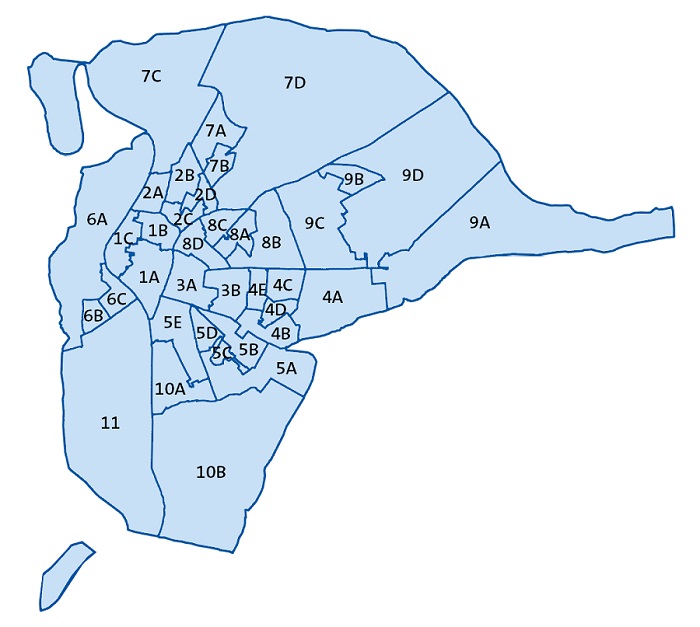
The main source of information regarding hospital admissions was the minimum basic dataset (MBDS) database that records basic mandatory information at discharge.22 Since the MBDS form does not include complete addresses, we obtained patient addresses from the health care user information database of the Department of Health of Andalusia. We assigned addresses to specific residential areas according to the boundaries of the administrative divisions of the city of Seville (subdistricts).23 We assigned addresses to subdistricts applying the criteria used by the Urban Audit project24 (Figure 2). This was also the source of the data for the mean annual household net income (MAHNI) and the age distribution of each subdistrict in year 2015, which we used as reference. Primary diagnoses were coded according to the International Classification of Diseases, ninth revision, clinical modification (ICD-9-CM).25
| Figure 2. Subdistricts of the city of Seville |
|---|
 |

The purpose of the reported cases data set was to supplement the analysis of the hospital admissions set, as the latter does not include pertussis cases that did not require hospital admission. It includes the cases of pertussis reported by every health care facility in Seville to the Department of Epidemiology of the Seville Primary Care Health District in children under 15 years residing in the city of Seville in the 2013-2017 period, whether they were hospitalised or not (n = 127). It includes years 2016 and 2017, which were not included in the hospital admission set, to assess trends in the years that followed the introduction of vaccination of pregnant women. We excluded cases that had not been confirmed (n = 25). This set included 102 observations. We applied the case definition used by the Epidemiological Surveillance System of Andalusia,26 which only includes infection by Bordetella pertussis in the laboratory criteria for diagnosis of pertussis. We assigned addresses to subdistricts of Seville in the same manner as we did for the hospital admission data set, as well as the same three indicators of SES.
The independent variables in the analysis of both data sets were age, sex and SES of the area of residence. The variable area at risk of poverty (ARP) classified the 37 subdistricts of the city of Seville based on the MAHNI in 201524,27: subdistricts where the mean net income was below the threshold for risk of poverty were classified as ARPs28 (Fig. 2). This threshold was set at 16 823 euros, which corresponds to 60% of the median net income of households composed of 2 adults and 2 dependents aged less than 14 years based on data from the survey of living standards conducted by the Instituto Nacional de Estadística (INE) of Spain in the same year.29 The variable area with low educational attainment (ALEA) classified subdistricts based on the percentage of the population over 16 years that was illiterate or had not completed primary education, with subdistricts considered a ALEA if this percentage exceeded 16.38%30,31 (Figure 2). We obtained information on the educational attainment of the population in each subdistrict from the national census conducted in 2011.32 Lastly, area in need of social transformation (ANST) is a multidimensional variable that encompasses information based on economic, educational, employment and social exclusion data to define areas with structural poverty. Based on this information, the Government of Andalusia identifies the ANSTs in different municipalities in the region: in the city of Seville, there are 11 ANSTs. The ANST variable in our study classified subdistricts based on whether they contained any or no ANSTs33-35 (Figure 2).
The dependent variable in the hospital admission data set was the frequency of hospital admissions with a primary diagnosis of pertussis documented with any of the 033 codes of the ICD-9-CM, which includes infections by Bordetella pertussis, parapertussis and bronchiseptica and other unspecified organisms. In the reported cases data set, the dependent variable was the frequency of cases of pertussis with laboratory confirmation of infection by Bordetella pertussis.
In the statistical analysis, we made a univariate analysis of the hospital admission data set summarising variables as absolute and relative frequencies, and a bivariate analysis with comparisons performed with the χ2 test. The multivariate analysis consisted of fitting logistic regression models for each independent variable indicative of the SES of the area of residence, adjusted for age and sex. We calculated adjusted odds ratios (aORs) with the corresponding 95% confidence intervals (CIs). We defined statistical significance as p <0.05. The analysis was performed with the software R (version 3.5.1). In the analysis of the reported cases set, we calculated the annual and cumulative incidence of confirmed cases of pertussis in the five-year period under study in each of the 37 subdistricts, as well as in subdistricts grouped based on the ARP, ANST and ALEA variables. To compare the incidence in relation to the SES of the area of residence, we calculated the incidence ratio (IR). We analysed the spatial distribution of cases using the gvSIG software system (version 2.2.0.2312)36.
The study was approved by the Biomedical Research Ethics Committee of Andalusia.37
RESULTS
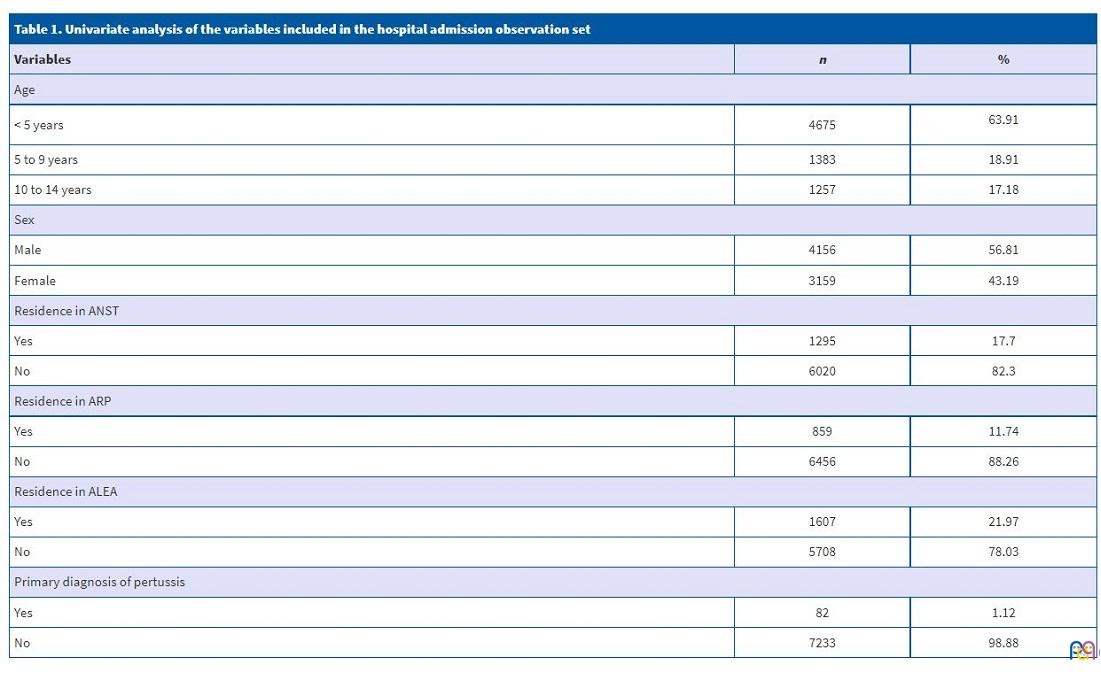
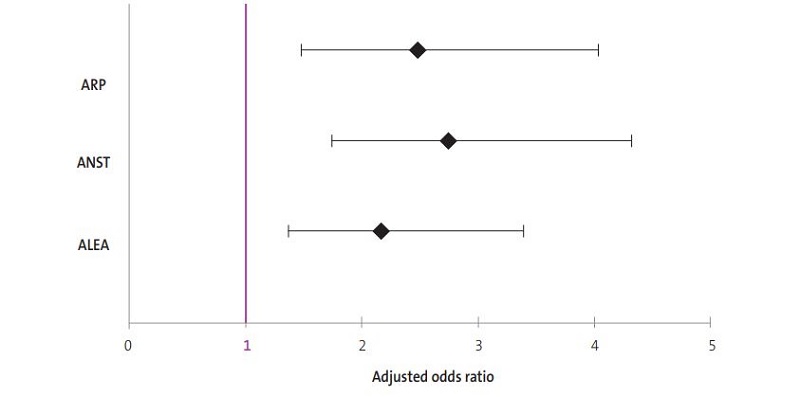
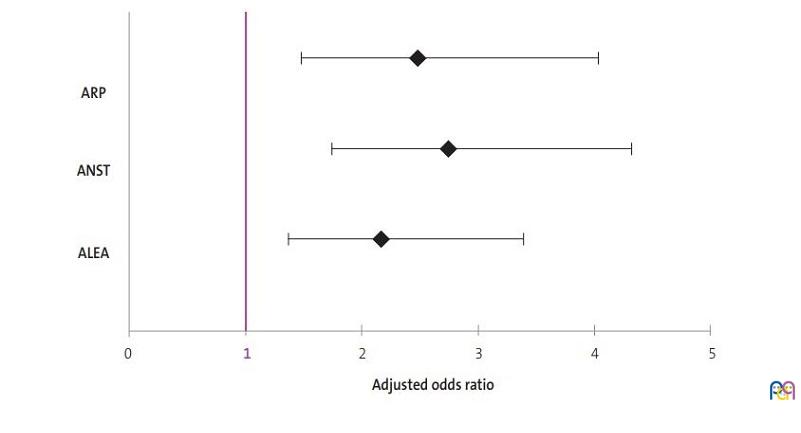
Table 1 presents the results of the univariate analysis of the 7315 hospital admission events included in the hospital admissions data set. Of the total admissions, 63.91% occurred in children under 5 years and 43.19% in girls. The reason for admission was pertussis in 82 admissions (1.12% of the total). The admissions of children residing in areas corresponding to the low SES category of the ANST, ARP or ALEA variables amounted to 17.70%, 11.74% and 21.97% of the total, respectively. The proportion of admissions due to pertussis in children under 15 years that resided in subdistricts of low SES (based on the categories of the variables used to assess SES) was higher compared to children that resided in areas of higher SES, with percentages ranging from 2.0 to 2.4% compared to 0.8 to 0.9%, respectively. These differences were statistically significant, with a p-value of less than 0.001 (Table 2). The differences were also statistically significant in the multivariate analysis, with an aOR for age and sex of 2.76 (95 CI: 174 to 4.32) for ANSTs, 2.48 (95 CI: 1.47 to 4.04) for ARPs and 2.17 (95 CI: 1.38 to 3.39) for ALEAs (Table 2 and Figure 3).
| Table 1. Univariate analysis of the variables included in the hospital admission observation set | ||
|---|---|---|
| Variables | n | % |
| Age | ||
| < 5 years | 4675 | 63.91 |
| 5 to 9 years | 1383 | 18.91 |
| 10 to 14 years | 1257 | 17.18 |
| Sex | ||
| Male | 4156 | 56.81 |
| Female | 3159 | 43.19 |
| Residence in ANST | ||
| Yes | 1295 | 17.7 |
| No | 6020 | 82.3 |
| Residence in ARP | ||
| Yes | 859 | 11.74 |
| No | 6456 | 88.26 |
| Residence in ALEA | ||
| Yes | 1607 | 21.97 |
| No | 5708 | 78.03 |
| Primary diagnosis of pertussis | ||
| Yes | 82 | 1.12 |
| No | 7233 | 98.88 |
| Table 2. Bivariate and multivariate analysis of hospital admissions due to pertussis and area of residence | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Area of residence | Pertussis | Odds ratio crude | Odds ratio (adjusted for age and sex) | |||||||||||
| No | Yes | Total | p-value | cOR | 95 CI | p-value | aOR | 95 CI | p-value | |||||
| n | % | n | % | n | % | |||||||||
| ANST | No | 5969 | 99.2 | 51 | 0.8 | 6020 | 100 | <0.001 | 1 | - | <0.001 | 1 | - | <0.001 |
| Yes | 1264 | 97.6 | 31 | 2.4 | 1295 | 100 | 2.87 | 1.81-4.48 | 2.76 | 1.74-4.32 | ||||
| ARP | No | 6395 | 99.1 | 61 | 0.9 | 6456 | 100 | <0.001 | 1 | - | <0.001 | 1 | - | <0.001 |
| Yes | 838 | 97.6 | 21 | 2.4 | 859 | 100 | 2.63 | 1.56-4.26 | 2.48 | 1.47-4.04 | ||||
| ALEA | No | 5658 | 99.1 | 50 | 0.9 | 5708 | 100 | <0.001 | 1 | - | <0.001 | 1 | - | <0.001 |
| Yes | 1575 | 98.0 | 32 | 2.0 | 1607 | 100 | 2.30 | 1.46-3.58 | 2.17 | 1.38-3.39 | ||||
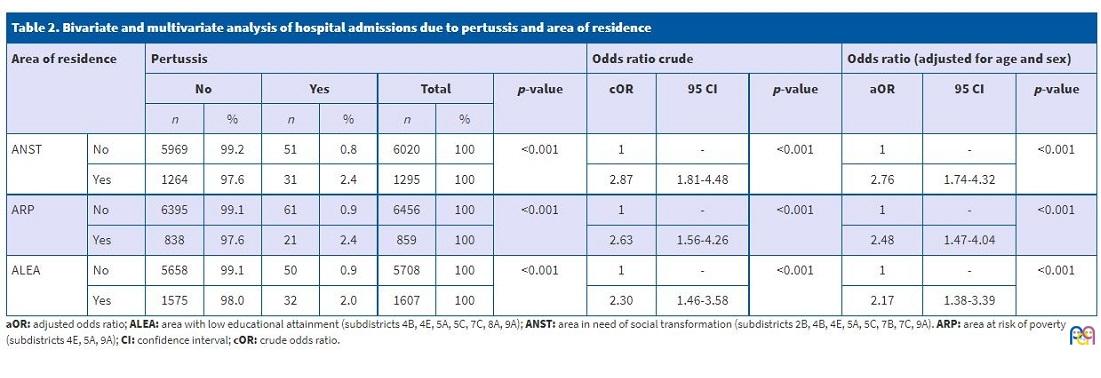
| Figure 3. Adjusted odds ratios in the multivariate analysis of hospital admission and area of residence |
|---|
 |
There were 82 paediatric hospital admissions due to pertussis in the 2 public referral hospitals in the city of Seville in the 2013-2015 period (including infection by different Bordetella species and unspecified organisms). In the same period, there were a total of 81 reported cases of pertussis with laboratory confirmation in the same population. In addition, in 2016 and 2017 there were 21 confirmed cases, adding to a total of 102 for the 2013-2017 period (Table 3).
| Table 3 Annual incidence and cumulative 5-year incidence of pertussis in children under 15 years by subdistrict in the city of Seville, 2013-2017 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Subdistricts | Reference population <15 years (2015) | Pertussis, 2013-2017 period | Pertussis, 2013 | Pertussis, 2014 | Pertussis, 2015 | Pertussis, 2016 | Pertussis, 2017 | ||||||
| n | n | Incidenciea | n | Incidenciea | n | Incidenciea | n | Incidenciea | n | Incidenciea | n | Incidenciea | |
| 1-A | 2569 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| 1-B | 2966 | 1 | 33.72 | 1 | 33.72 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| 1-C | 1988 | 2 | 100.60 | 1 | 50.30 | 0 | 0.00 | 1 | 50.30 | 0 | 0.00 | 0 | 0.00 |
| 2-A | 1494 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| 2-Bb | 4070 | 7 | 171.99 | 2 | 49.14 | 2 | 49.14 | 3 | 73.71 | 0 | 0.00 | 0 | 0.00 |
| 2-C | 1868 | 1 | 53.53 | 1 | 53.53 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| 2-D | 2043 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| 3-A | 4167 | 1 | 24.00 | 1 | 24.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| 3-B | 2839 | 3 | 105.67 | 0 | 0.00 | 1 | 35.22 | 0 | 0.00 | 1 | 35.22 | 1 | 35.22 |
| 4-A | 4044 | 7 | 173.10 | 0 | 0.00 | 2 | 49.46 | 3 | 74.18 | 2 | 49.46 | 0 | 0.00 |
| 4-Bb | 3579 | 4 | 111.76 | 0 | 0.00 | 1 | 27.94 | 3 | 83 | 0 | 0.00 | 0 | 0.00 |
| 4-C | 1672 | 1 | 59.81 | 0 | 0.00 | 0 | 0.00 | 1 | 59.81 | 0 | 0.00 | 0 | 0.00 |
| 4-D | 1890 | 5 | 264.55 | 1 | 52.91 | 1 | 52.91 | 1 | 52.91 | 1 | 52.91 | 1 | 52.91 |
| 4-Eb | 2714 | 2 | 73.69 | 0 | 0.00 | 1 | 36.85 | 0 | 0.00 | 1 | 36.85 | 0 | 0.00 |
| 5-Ab | 3703 | 10 | 270.05 | 3 | 81.02 | 1 | 27.01 | 3 | 81.02 | 3 | 81.02 | 0 | 0.00 |
| 5-B | 1459 | 5 | 342.70 | 1 | 68.54 | 0 | 0.00 | 2 | 137.08 | 2 | 137.08 | 0 | 0.00 |
| 5-Cb | 1319 | 1 | 75.82 | 1 | 75.82 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| 5-D | 1860 | 1 | 53.76 | 0 | 0.00 | 1 | 53.76 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| 5-E | 3089 | 1 | 32.37 | 0 | 0.00 | 0 | 0.00 | 1 | 32.37 | 0 | 0.00 | 0 | 0.00 |
| 6-A | 2194 | 2 | 91.16 | 0 | 0.00 | 0 | 0.00 | 2 | 91.16 | 0 | 0.00 | 0 | 0.00 |
| 6-B | 1358 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| 6-C | 2650 | 2 | 75.47 | 0 | 0.00 | 0 | 0.00 | 2 | 75.47 | 0 | 0.00 | 0 | 0.00 |
| 7-A | 5184 | 5 | 96.45 | 0 | 0.00 | 2 | 38.58 | 1 | 19.29 | 2 | 38.58 | 0 | 0.00 |
| 7-Bb | 2348 | 6 | 255.54 | 3 | 127.77 | 1 | 42.59 | 2 | 85.18 | 0 | 0.00 | 0 | 0.00 |
| 7-Cb | 2099 | 7 | 333.49 | 1 | 47.64 | 3 | 142.93 | 1 | 47.64 | 0 | 0.00 | 2 | 95.28 |
| 7-D | 1743 | 2 | 114.74 | 0 | 0.00 | 2 | 114.74 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| 8-Ab | 2230 | 2 | 89.69 | 0 | 0.00 | 1 | 44.84 | 0 | 0.00 | 1 | 44.84 | 0 | 0.00 |
| 8-B | 1217 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| 8-C | 1740 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| 8-D | 2661 | 2 | 75.16 | 0 | 0.00 | 0 | 0.00 | 1 | 37.58 | 1 | 37.58 | 0 | 0.00 |
| 9-Ab | 3190 | 5 | 156.74 | 0 | 0.00 | 2 | 62.70 | 3 | 94.04 | 0 | 0.00 | 0 | 0.00 |
| 9-B | 3235 | 2 | 61.82 | 0 | 0.00 | 0 | 0.00 | 2 | 61.82 | 0 | 0.00 | 0 | 0.00 |
| 9-C | 3439 | 2 | 58.16 | 0 | 0.00 | 1 | 29.08 | 1 | 29.08 | 0 | 0.00 | 0 | 0.00 |
| 9-D | 9471 | 7 | 73.91 | 2 | 21.12 | 2 | 21.12 | 3 | 31.68 | 0 | 0.00 | 0 | 0.00 |
| 10-A | 1563 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| 10-B | 6194 | 6 | 96.87 | 0 | 0.00 | 1 | 16.14 | 2 | 32.29 | 3 | 48.43 | 0 | 0.00 |
| 11 | 3538 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| Total | 105400 | 102 | 96.77 | 18 | 17.08 | 25 | 23.72 | 38 | 36.05 | 17 | 16.13 | 4 | 3.80 |
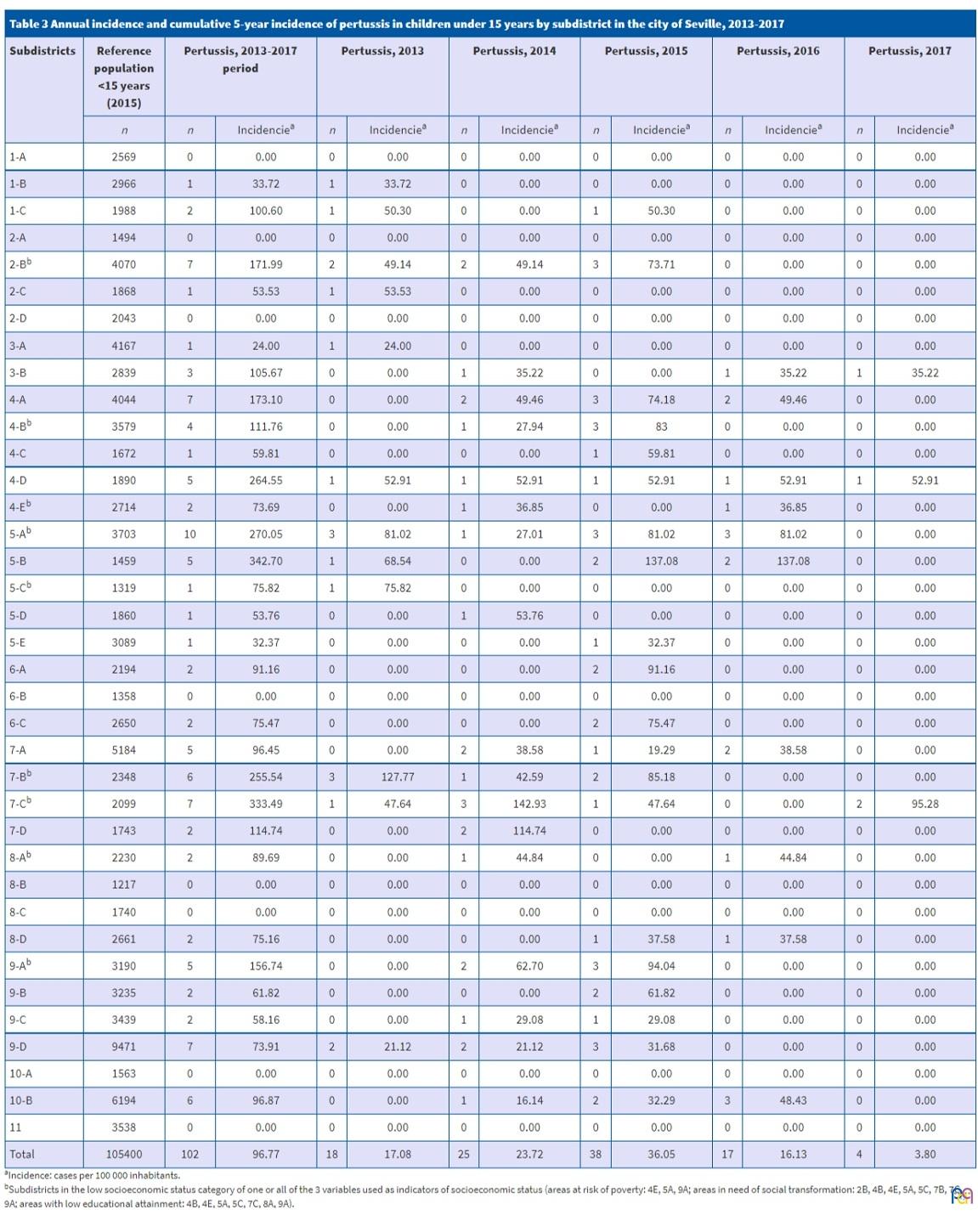
The cumulative incidence of confirmed cases in the 2013-2017 period varied between subdistricts, ranging from 0 to 342 cases/105 inhabitants under 15 years (Table 3). In 8 subdistricts, there were no reported confirmed cases of pertussis in that five-year period, and none of them were considered an ANST, ARP or ALEA. The incidence in 6 of the 9 subdistricts of lower SES was higher compared to the overall incidence for Seville, with cases adding up to 39 cases of the total 102 confirmed cases reported in the period (38.2%). Table 3 shows how to the overall incidence increased yearly between 2013 (17.08/105) and 2015 (36.05/105), followed by a decline in 2016 (16.13/105) and 2017 (3.80/105).
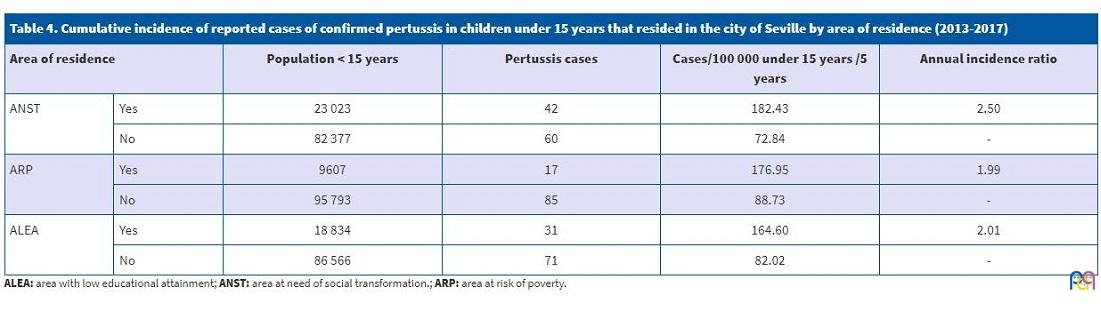
The incidence of pertussis was higher in subdistricts classified in the lower SES categories of the 3 variables used to assess the SES of the area of residence. We found an incidence ratio of 2.50 for ANSTs, 1.99 for ARPs and 2.01 for ALEAs (Table 4 and Figure 4).
| Table 4. Cumulative incidence of reported cases of confirmed pertussis in children under 15 years that resided in the city of Seville by area of residence (2013-2017) | |||||
|---|---|---|---|---|---|
| Area of residence | Population < 15 years | Pertussis cases | Cases/100 000 under 15 years /5 years | Annual incidence ratio | |
| ANST | Yes | 23 023 | 42 | 182.43 | 2.50 |
| No | 82 377 | 60 | 72.84 | - | |
| ARP | Yes | 9607 | 17 | 176.95 | 1.99 |
| No | 95 793 | 85 | 88.73 | - | |
| ALEA | Yes | 18 834 | 31 | 164.60 | 2.01 |
| No | 86 566 | 71 | 82.02 | - | |
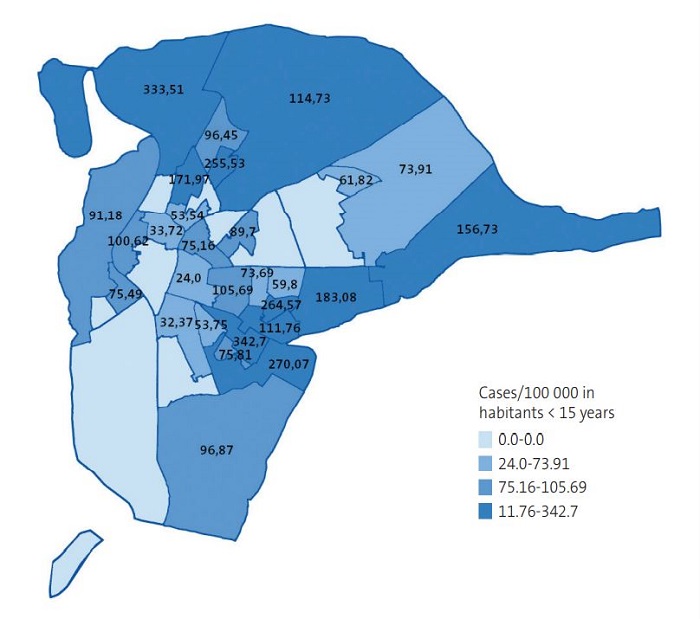
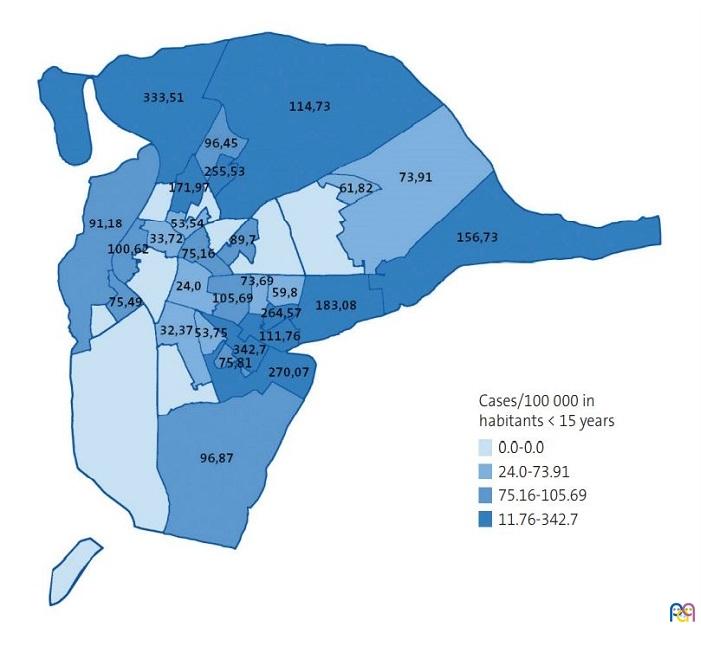
| Figure 4. Quartile distribution of the cumulative incidence of reported cases of pertussis with laboratory confirmation in children aged less than 15 years residing in the different subdistricts of the city of Seville (2013-2017) |
|---|
 |
DISCUSSION
The results of the study show that the rate of hospital admission due to pertussis and the incidence of pertussis in children under 15 years living in Seville were higher in children residing in low SES areas. The different variables used as indicators of SES based on exclusively economic, exclusively educational or multidimensional data all yielded similar results that corroborated this finding.
The number of paediatric hospital admissions due to pertussis in the 2 public referral hospitals of Seville in the 2013-2015 period and the number of reported confirmed cases of pertussis in the city in the same period were similar (n = 82 vs. n = 81). The MBDS may be a valid source of information for research on pertussis in children on account of the high frequency of hospital admission associated with pertussis and the underreporting of cases to passive surveillance systems.3 The decrease in cases reported since 2015 may be explained by the characteristic temporal pattern of this disease1,9 and, above all, to the introduction of vaccination against pertussis in pregnant women,4,10 as can be seen in the decline in annual incidence observed in years 2016 and 2017, which was most marked in subdistricts of low SES.
The frequency of hospital admission due to pertussis was 2.17 to 2.76 times greater in children that resided in neighbourhoods of low SES in Seville. We found the greatest differences in both data sets applying the independent variable that included multidimensional information on SES (ANST), so this variable may be useful in future research on SES and pertussis. Our findings agree with those of previous studies conducted in Spain5 and abroad.12-14 The aOR values obtained in the multivariate analysis were similar to those reported by Brugueras et al. in Barcelona5 for the lowest SES category (aOR = 2.83), despite their study also including the adult population.
Two of the 5 subdistricts with the highest cumulative incidence (5-B and 4-D) did not fit the ANST, ARP or ALEA categories. This may be explained because both subdistrict 5-B (cumulative incidence, 342.70/105) and subdistrict 4-D (cumulative incidence, 264.55/105) are surrounded by other subdistricts that are included in one or more disadvantaged areas, which makes it more likely for children to be in shared spaces where they can contract the infection (Figures 2 and 4).
There are limitations to our study. When it came to the hospital admissions data set, the end date for inclusion of coded hospital admissions (01/01/2016) may have resulted in the exclusion of up to 2.1% of hospital admissions of the total 260 initially recorded events.39 This would mostly affect admissions in late 2015, when the incidence started to decline. We did not include admissions due to pertussis in private hospitals or cases managed at the primary care level. To estimate the potential effect of this selection bias, we included the second set of observations, corresponding to reported cases, which included every case reported by public or private hospitals or primary care facilities. The results of the analysis of both data sets are concordant and evince a greater incidence of pertussis in low SES areas, with differences of similar magnitude. However, it is important to interpret other comparisons between both sets of observations with caution, as their definitions of pertussis as an outcome differed.
It is possible that some of the hospital admissions of children residing in low SES areas correspond to households of higher SES and vice versa. While this is a potential source of classification bias, it is unlikely that it affected families greatly, as the data used to determine whether a subdistrict did or did not correspond to a low SES area were mean values for the households in the area and the individuals residing in them. In addition, previous studies have demonstrated that the SES of the area of residence is independent from the SES of the household.40
The inclusion of the variables “vaccine coverage” and “parental vaccine refusal” could have enhanced the findings of this study, and we propose their investigation in future research. In a study conducted by Brugueras et al.5 in which most of the families that refused vaccination were clustered in higher SES areas, only 3.9% of cases of pertussis reported in children under 6 years corresponded to children with parents that refused vaccination. Our findings are consistent with theirs, as they suggest the greater importance of SES as a factor explaining the substantial differences observed in the incidence of pertussis children and related hospital admissions. Nevertheless, it is important to address the concerns of caregivers regarding vaccination to prevent potential cases in children.5,38
The main strength of the study was the large number of observations included in the hospital admission set, data obtained from the 2 public referral hospitals in the city of Seville. The exclusion of readmissions for reasons other than pertussis prevented duplication of the observations, and the inclusion of the second set of observations, which did not have the biases intrinsic in the first set, allowed us to compare the respective results. The use of official sources of data and the application of standardised criteria established or used by government agencies for the definition of SES indicators, subdistricts and diagnoses ensures the objectivity and comparability of our findings. The inclusion of different variables as indicators of SES offers added value, as we were able to differentiate the effect of each variable. Lastly, the graphic representation of the geographical case distribution obtained with the gvSIG software facilitated the interpretation of results.
Few studies have analysed the incidence of pertussis from the perspective of social determinants of health and inequity, particularly during recession periods. In conclusion, the results of our study showed an association between residence in areas of low SES in Seville and increases in the frequency of inpatient care and the incidence of pertussis in the population under 15 years. The availability and accessibility of health care services and vaccination programmes must be enhanced with integrated social policy and public health measures to reduce the incidence of pertussis in the paediatric population and the associated need of hospital-based care.
CONFLICT OF INTERESTS
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS
ALEA: area with low educational attainment · ANST: area in need of social transformation · aOR: adjusted odds ratio · ARP: area at risk of poverty · CI: confidence interval · ICD-9-CM: International Classification of Diseases, ninth revision, clinical modification · MAHNI: mean annual household net income · MBDS: Minimum Basic Data Set · SES: socioeconomic status.
ACKNOWLEDGMENTS
We thank Dr. Eduardo Briones Pérez de la Blanca (Department of Epidemiology, Public Health Unit of the Primary Health District of Seville), Dr. José Salas Turrens (Medical Documentation, Hospital Universitario Virgen Macarena) And Ms. María José Vázquez Ferri (Department of Analysis and Evaluation of the Hospital Universitario Virgen del Rocío) for the collaboration in data collection for the study.
REFERENCES
- Weekly epidemiological record: position paper on pertussis vaccines. In: World Health Organization [online] [accessed 20/04/2021]. Available at www.who.int/wer
- Campins M, Moreno Pérez D, Gil de Miguel A, González Romo F, Moraga Llop FA, Arístegui Fernández J, et al. Tosferina en España. Situación epidemiológica y estrategias de prevención y control. Recomendaciones del Grupo de Trabajo de Tosferina. Enferm Infecc Microbiol Clin. 2013;31:240-53.
- Fernández-Cano MI, Armadans-Gil L, Álvarez-Bartolomé M, Rodrigo-Pendás JÁ, Campins-Martí M. Hospitalización por tosferina en España (1997-2011). Enferm Infecc Microbiol Clin. 2014;32:638-42.
- Viarce Torres M, López Perea N, Masa Calles J. Situación de la tosferina en España 2005-2016. In: Instituto de Salud Carlos III [online] [accessed 20/04/2021]. Available at www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Paginas/Enfermedades-A-Z.aspx
- Brugueras S, Rius C, Millet J-P, Casals M, Caylà JA. Does the economic recession influence the incidence of pertussis in a cosmopolitan European city? BMC Public Health. 2019;19:1-9.
- Yeung KHT, Duclos P, Nelson EAS, Hutubessy RCW. An update of the global burden of pertussis in children younger than 5 years: a modelling study. Lancet Infect Dis. 2017;17:974-80.
- Pertussis Annual Epidemiological Report for 2017. In: European Centre for Disease Prevention and Control [online] [accessed 20/024/2021]. Available at www.ecdc.europa.eu/sites/default/files/documents/AER_for_2017-pertussis.pdf
- Pertussis annual epidemiological report for 2015 In: European Centre for Disease Prevention and Control [online] [accessed 20/024/2021]. Available at www.ecdc.europa.eu/sites/default/files/documents/AER_for_2015-pertussis.pdf
- Gallardo García V. Tosferina Andalucia 2018. In: Boletín Epidemiológico Semanal del Sistema de Vigilancia Epidemiológica de Andalucía [online] [accessed 20/04/2021]. Available at www.repositoriosalud.es/handle/10668/3048
- Viarce Torres M, López Perea N, Masa Calles J. Situación de la tosferina en España 1998-2016: Análisis preliminar del impacto de la vacunación de tosferina en embarazadas. In: Instituto de Salud Carlos III [online] [accessed 20/04/2021]. Available at www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Paginas/Enfermedades-A-Z.aspx
- Suhrcke M, Stuckler D, Suk JE, Desai M, Senek M, McKee M, et al. The impact of economic crises on communicable disease transmission and control: a systematic review of the evidence. PLoS One. 2011;6:1-12.
- Maclure A, Stewart GT. Admission of children to hospitals in Glasgow: relation to unemployment and other deprivation variables. Lancet. 1984;2:682-5.
- Zamir CS, Dahan DB, Shoob H. Pertussis in infants under one year old: Risk markers and vaccination status-A case-control study. Vaccine. 2015;33:2073-8.
- Levri KM, Reynolds L, Liko J, Dott M, Robinson BF, Cieslak PR. Risk factors for pertussis among hispanic infants. Pediatr Infect Dis J. 2016;35:488-93.
- Kowalzik F, Barbosa AP, Fernandes VR, Carvalho PR, Avila-Aguero ML, Goh DYT, et al. Prospective multinational study of pertussis infection in hospitalized infants and their household contacts. Pediatr Infect Dis J. 2007;26:238-42.
- Iglesias L, Casabella Pernas A, Hernández Febles M, Colino Gil E, Eisman Maraver A, Pena López MJ. Estudio clínico-epidemiológico de la infección por Bordetella pertussis en la isla de Gran Canaria en el periodo 2008-2016. An Pediat (Barc). 2018;89:170-5.
- Uriona Tuma SM, Martínez Gómez X, Campins Martí M, Codina Grau G, Ferrer Marcelles A, Rodrigo Pendás JÁ, et al. Estudio de contactos de casos pediátricos de tosferina en un hospital de tercer nivel de Barcelona. Med Clin (Barc). 2013;141:376-81.
- Geronimus AT, Bound J. Use of census-based aggregate variables to proxy for socioeconomic group: Evidence from national samples. Am J Epidemiol. 1998;148:475-86.
- Soobader M, LeClere F, Hadden W, Maury B. Using aggregate geographic data to proxy individual socioeconomic status: Does size matter? Am J Public Health. 2001;91:632-6.
- Borrell C, Serral G, Martínez-Beneito MÁ, Marí-Dell’Olmo, Marc Rodríguez-Sanz M. Atlas de mortalidad en ciudades de España (1996-2003). In: Proyecto MEDEA [online] [accessed 20/04/2021]. Available at www.proyectomedea.org
- Ordobás Gavín M, Fernández Rodríguez S, Cañellas Llabrés S, Rodríguez Artalejo F. Prevalencia de infección tuberculosa y su relación con la clase social en niños de la Comunidad de Madrid. An Pediatr (Barc). 2006;64:34-9.
- Conjunto Mínimo Básico de Datos al alta hospitalaria. In: Ministerio de Sanidad Servicios Sociales e Igualdad del Gobierno de España [online] [accessed 20/04/2021]. Available at www.msc.es/estadEstudios/estadisticas/cmbd.htm
- División administrativa de la ciudad de Sevilla. In: Ayuntamiento de Sevilla [online] [accessed 20/04/2021]. Available at www.sevilla.org
- Proyecto Urban Audit. División territorial del Área Submunicipal de Sevilla. In: Instituto Nacional de Estadística [online] [accessed 20/04/2021]. Available at www.ine.es/ss/Satellite?L=es_ES&c=INESeccion_C&p=1254735110672&pagename=ProductosYServicios%2FPYSLayout¶m1=PYSDetalleFichaSeccionUA¶m3=1259944561392&_charset_=UTF-8&cid=1259948749713
- Ministerio de Sanidad Servicios Sociales e Igualdad, Gobierno de España. Clasificación Internacional de Enfermedades. 9.ª Revisión Modificación Clínica. Madrid: 2014.
- Sistema de Vigilancia Epidemiológica de Andalucía. Protocolo de vigilancia y alerta de tosferina. In: Junta de Andalucía [online] [accessed 20/04/2021]. Available at www.juntadeandalucia.es/export/drupaljda/salud_5af95879cd397_p_tosferina.pdf
- Indicadores urbanos: método de estimación de la renta neta media anual de los hogares. 2018. In: Instituto Nacional de Estadística [online] [accessed 20/04/2021]. Available at www.ine.es/ss/Satellite?L=es_ES&c=INESeccion_C&cid=1259925949467&p=1254735110672&pagename=ProductosYServicios%2FPYSLayout¶m1=PYSDetalle¶m3=1259924822888
- Glossary: At risk of poverty rate. In: Eurostat Statistic Explained [online] [accessed 20/04/2021]. Available at http://ec.europa.eu/eurostat/statistics-explained/index.php?title=Glossary:At-risk-of-poverty_rate
- Encuesta de Condiciones de Vida 2015. In: Instituto Nacional de Estadística [online] [accessed 20/04/2021]. Available at www.ine.es/prensa/np969.pdf
- Instituto Juan de Herrera DUyOT. Análisis urbanístico de barrios vulnerables en España: sobre la vulnerabilidad urbana. In: Ministerio de Fomento [online] [accessed 20/04/2021]. Available at www.fomento.gob.es/NR/rdonlyres/C88DB66D-8669-497C-BEE4-442AE027E2FB/111287/SOBRE_vulnerabilidad.pdf
- Instituto Juan de Herrera DUyOT. Síntesis metodológica general del Catálogo de Barrios Vulnerables e Indicadores Básicos de Vulnerabilidad Urbana. In: Ministerio de Fomento [online] [accessed 20/04/2021]. Available at https://apps.fomento.gob.es/BarriosVulnerables/static/adjunto/Sintesis_metodologica_general_catalogo_bbvv.pdf
- Censos de población y vivienda, 2011. In: Instituto Nacional de Estadísticas [online] [accessed 20/04/2021]. Available at www.ine.es/censos2011_datos/cen11_datos_inicio.htm
- Zonas de necesidad de transformación social de Sevilla. In: Consejería de Sanidad de la Junta de Andalucía [online] [accessed 20/04/2021]. Available at www.znts.es/course/index.php?categoryid=8
- Decreto-ley 7/2013, de 30 de abril, de medidas extraordinarias y urgentes para la lucha contra la exclusión social en Andalucía. BOJA núm. 85 de 03/05/2013. Spain: Consejería de Salud y Bienestar Social de la Junta de Andalucía; 2013. p. 27-88.
- Mora Ruiz V, Jiménez Martín JA, Gamboa Gallego MDC. Diagnóstico de territorios desfavorecidos en la ciudad de Sevilla. In: Ministerio de Trabajo y Economía Social [online] [accessed 20/04/2021]. Available at www.empleo.gob.es/redretos/es/contenidos/actualidad/2011/06/Diagnostico_de_territorios_desfavorecidos_opt.pdf
- gvSIG: Sistema de Información Geográfica. In: gvSIG Association [online] [accessed 20/04/2021]. Available at www.gvsig.com/es
- Comité Coordinador de Ética de la Investigación Biomédica de Andalucía. 2018. In: Servicio de Salud Público Andaluz [online] [accessed 20/04/2021]. Available at http://si.easp.es/eticaysalud/content/comite-coordinador-etica-investigacion-biomedica-andalucia/contacto
- Salmon DA, Dudley MZ, Glanz JM, Omer SB. Vaccine Hesitancy: Causes, consequences and a call to action. Am J Prev Med. 2015;49:S391-8.
- Servicio de Análisis y Evaluación, Unidad de Comunicación. Memoria 2015. Hospitales Universitarios Virgen Macarena - Virgen del Rocío. In: Hospital Universitario Virgen del Rocío [online] [accessed 20/04/2021]. Available at www.hospitaluvrocio.es/memorias/2015.pdf
- Sellström E, Bremberg S. The significance of neighbourhood context to child and adolescent health and well-being: a systematic review of multilevel studies. Scand J Public Health. 2006;34:544-54.