
Vol. 23 - Num. 89
Original Papers
Economic evaluation of e-mail consulting and its impact on COVID-19. A five-year experience
Nerea Gil Giméneza, Guillermo Peña Blascob, M.ª Lucía Bartolomé Lalanzac, Esther Atance Melendod, Susana Buil Langaritaa, M.ª Jesús Blasco Pérez-Aramendíae
aEnfermera pediátrica. CS Valdefierro. Zaragoza. España.
bDepartamento de Economía Pública. Universidad de Zaragoza. Zaragoza. España.
cPediatra. CS Valdefierro, Zaragoza, España. Departamento de Pediatría. Universidad de Zaragoza. Zaragoza. España .
dEnfermera pediátrica. CS Valdefierro. Zaragoza. España .
ePediatra. CS Valdefierro, Zaragoza, España. Departamento de Pediatría. Universidad de Zaragoza. Zaragoza. España.
Correspondence: G Peña. E-mail: gpenablasco@gmail.com
Reference of this article: Gil Giménez N, Peña Blasco G, Bartolomé Lalanza ML, Atance Melendo E, Buil Langarita S, Blasco Pérez-Aramendía MJ. Economic evaluation of e-mail consulting and its impact on COVID-19. A five-year experience. Rev Pediatr Aten Primaria. 2021;23:43-51.
Published in Internet: 22-03-2021 - Visits: 13025
Abstract
Introduction: in this study, we describe our experience with an email consultation service in a primary care centre in Aragon (Spain) over a 5-year period. We evaluated the economic impact of the service, user satisfaction and use of the service during the COVID-19 pandemic.
Method: in the first in-person appointment with the parents, we offered the use of email consultation with the paediatrician or nurse for non-urgent concerns. We provided directions. Two years after introducing the service, we performed a user satisfaction survey to evaluate the use of the service. At 3 years, we analysed the number of email consultations and the time and resources that they saved. Lastly, we assessed the use of the service during the lockdown imposed in the COVID-19 pandemic of 2020.
Results: the use of email consultations increased in the early months and remained stable thereafter. During the pandemic, the use of the service was massive. Parents reported high satisfaction with the service, and even requested that it be extended to other clinics in the primary care centre. As for the economic impact, we estimated annual savings of €37 271.5 based on the time the paediatrician needed to spend on responding by email compared to in person. But when we estimated the number of visits that would have been made if the email service was not available, we found it did not result in a decrease in in-person visits, perhaps due to the increased accessibility achieved with the service. Still, its use during the pandemic was essential to maintain confinement measures.
Conclusions: the email consultation service in paediatrics was perceived positively and achieved significant reductions in health care costs. The service has been very useful during the COVID-19 pandemic.
Keywords
● COVID-19 ● Health economics ● Telemedicine consultation ● User satisfactionINTRODUCTION
Communication provides the foundation and is a key element of the patient-physician relationship. Traditionally, face-to-face contact in the office and telephonic contact have been the main modalities of interaction of patients and health care providers, but at present, the electronic mail (email) is one of the most widely used forms of communication. Therefore, the use of this medium could also extend to health care delivery. The internet in general and the use of email in particular are changing the way in which individuals interact with each other and exchange information. These changes, albeit slowly, are also occurring in the health care field and provide a new means for patients to access health care providers and for providers to communicate with one another.1
The email is a useful tool as long as it is used as a supplementary form of communication and should never substitute direct face-to-face communication. However, complicated or negative messages, or messages that require followup, should be conveyed in person. Email consultations are a form of telemedicine.2
Email consultation (EC) has several advantages, as it allows rapid and inexpensive communication and sharing information in a variety of formats.3,4 It does not require travel of the user to a health care facility, which is useful in rural areas where the population is dispersed over a large geographical area. Compared to telephone calls, email gives the provider more time to think about how to respond. It can be tracked and saved, and it is a suitable vehicle for giving medical or nursing advice,5 or make changes to current treatments. Secure storage of email provides legal protection to both parties if documentation is ever needed.6
Notwithstanding, there can also be problems with email, including system outages, loss of data due to technical problems or computer viruses, concerns regarding confidentiality, insufficient identification of the involved parties or inadequate use due to the content or purpose of the communication.7
Another controversial aspect is the use of email with new patients with who the provider has not had previous face-to-face contact. Email consultation is a service that should be offered in the context of in-person care, developing the personal relationship and positive rapport between provider and patient through in-person visits at the health care facility. This positive rapport can be projected into ECs, and the latter may even strengthen the patient-physician relationship when used as a supplemental tool.6
To establish practice guidelines for the use of EC, its advantages and disadvantages need to be examined. It involves a shift in the patient-physician relationship.4 Health care providers and patients must discuss and agree on the appropriate use of this vehicle, and the patient needs to be informed about technical and security aspects of EC and of the established maximum turnaround time. Lastly, the patient must be given written information on the appropriate use of this vehicle, making it clear that it should never be used in an emergency.3
To establish an EC practice, health care providers must have time specifically allotted to it in their schedules.
All email correspondence is part of the health record of the patient, and the latter must document the exchanged questions and answers, processing the information in adherence with current law on health records and making backup copies.4 Emails can be considered official documents from a legal standpoint.
Emerging technologies are important for economic efficiency, including health care administration, as health care providers should not be unaware of the economic component of health care delivery. 8-10 The impact of the internet on efficiency is one of the areas being researched in the field of information economy.11 Complete information helps achieve economic efficiency and reduce costs.
During the coronavirus disease 2019 (COVID-19) pandemic, in the region of Aragon, as was the case elsewhere in Spain, the population was put under lockdown to prevent widespread transmission. Remote working was encouraged to pursue this objective. Telemedicine services have been used to replace in-person visits. Children in particular were not allowed to leave their homes, unless absolutely necessary, between March 15 and April 26, 2020.
The aim of our study was to determine whether EC succeeded in streamlining care delivery and alleviate the considerable demand for health care services, to assess its economic performance in terms of improvements in time management and use of health care resources by providers and therefore of the economic efficiency of health care centres. Another goal of EC is to make it easier for parents to gain access to health care professionals, minimise the number of hours of missed work and improve user satisfaction. We assessed the use of EC during the lockdown imposed in the context of the COVID-19 pandemic.
MATERIAL AND METHODS
We conducted the study in the autonomous community of Aragon, Spain, in an urban primary care centre serving a population without geographical dispersion. The paediatric catchment population of the centre, aged 0 to 14 years, has ranged from 2384 children in 2013 to 2424 children in 2020, served by a staff consisting of 2 paediatricians and 2 paediatric nurses.12
The EC service was launched in 2016 and a specific email account with a confidential password was established for patient consultation. This service was introduced to patients during the initial in-person visit by providing an information sheet detailing the subjects considered appropriate for this type of consultation. The provider had to respond within 48 hours.
Two years after the launch of the EC service, we conducted a user satisfaction survey. Users participated in the survey anonymously through a Google® Forms questionnaire. We sent the link to the survey to the 524 emails of the users of this service.
Three years after the launch, we analysed the use of the EC service and the associated increases or decreases in costs. To do so, we made a descriptive analysis of the total number of remote consultations (Fig. 1). We analysed the correlation between remote consultations and in-person visits, including only the 2014-2015 and 2017-2018 periods and excluding 2016, the year the EC service was launched, as we deemed the latter an atypical year (Fig. 2).
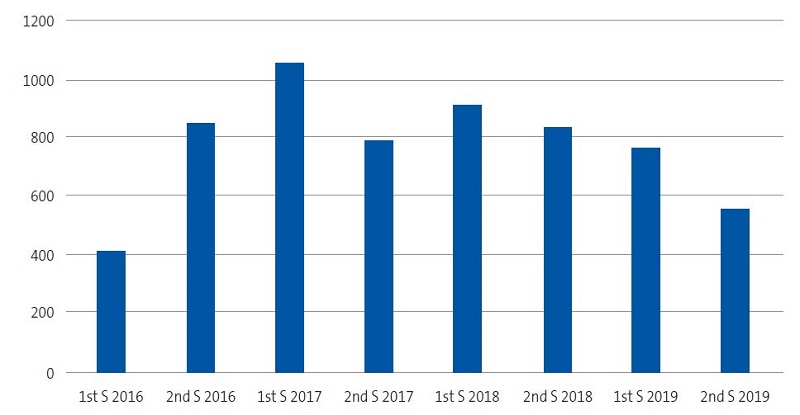
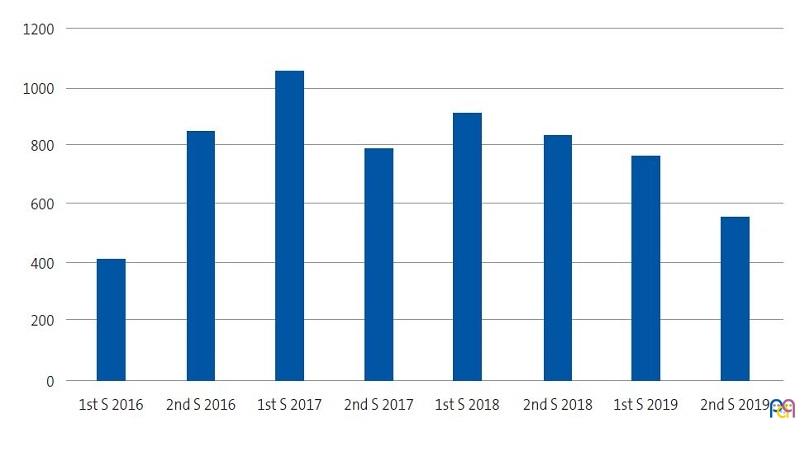
| Figure 1. Number of email consultations per semester (S) since the introduction of the service (years 2016-2019) |
|---|
 |
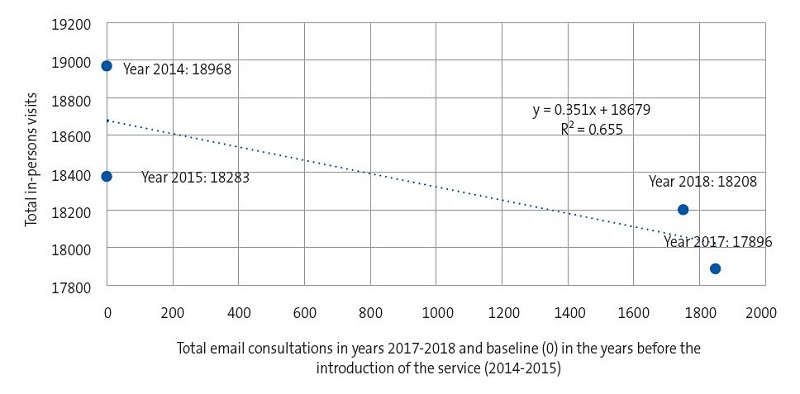
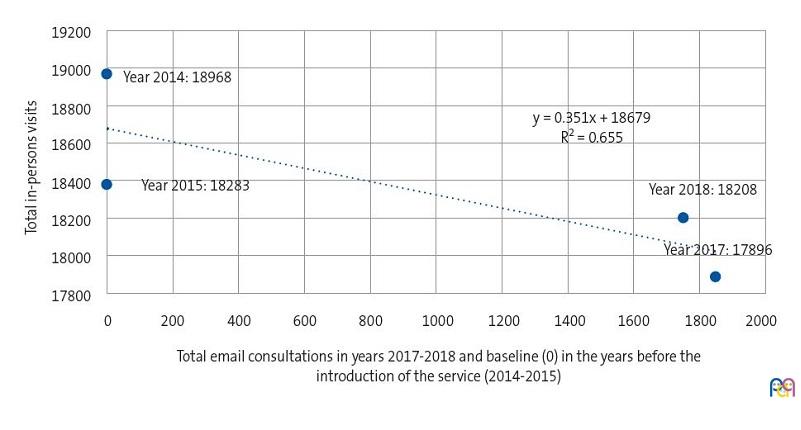
| Figure 2. Impact of the email consultation service on the total in-person visits in years 2014-2015 and 2017-2018 |
|---|
 |
Having done this, we analysed the number of avoided in-person visits, obtaining 2 estimates by mean of simple regression (ordinary least squares [OLS] method).
The first estimate calculated the number of in-person visits that would have been made in 2014 and 2015 if the EC service had already been operative. The second estimate calculated the number of in-person visits that would have been made in the 2016-2018 period if the EC service had not been established.
We also estimated the reductions in costs achieved in the 2016-2018 period by the introduction of the EC service (based on actual data on ECs) and the savings that would have been achieved in 2014-2015 (based on the first estimate of the number of in-person visits). The total reduction in costs was calculated as the cumulative savings achieved through the entire study period.
We also took into account the time that health care staff reported devoting to each EC, which was approximately half the time devoted to an in-person visit.
The cost-effectiveness analysis was performed monetizing the data with a discount rate of 3% relative to 2019.13
To conclude the economic evaluation, we performed a sensitivity analysis14,15 to assess the cost or benefit of public policy changing the applied discount rate (2%; 2.5%; 3%; 3.5%; 4%) or the estimated benefit per EC (changing from 1/3 to ½ to 2/3), the results of which can be seen in Table 2.
The cost of in-care visits can be found in the official gazette of the autonomous community of Aragon16 and has been updated with the data published by the Instituto Nacional de Estadística (National Institute of Statistics, INE).17
During the COVID-19 pandemic, we analysed the use of the EC service before and during the strict lockdown in 2020, comparing it to telephone consultations and in-person services.
RESULTS
Of the 2418 patients in the paediatrics caseload, 524 (21.67%) used the EC service. We obtained 236 responses to the survey (45%). Of all respondents, 97.4% considered that the EC service improved the accessibility of paediatric care. Also, 93.8% considered this new service helped them resolve concerns regarding the health of their children. Attached documents sent through email were considered useful by 84.1%. The service received a rating of more than 9/10 from 81.6% of users. All the added comments about the service were positive, and some users even asked that the service be expanded to include other clinics in the primary care centre.
A total of 4849 ECs were made in these 3 years, with a mean of 134 consultations per month and 6.7 per working day.
Figure 1 shows the number of ECs made in the 2016-2019 period. In the first semester of 2016, there were 411 ECs, and from the introduction of the service the number of consultations remained pretty consistent, ranging between 1057 and 788 per semester until the second semester of 2019, when there was a slight drop.
Figure 2 shows that there was an inverse correlation between the number of in-person visits and the number of ECs in 2014-2015 (18 968 and 18 383 in-person visits) and in 2017-2018 (17 896 and 18 208 in-person visits). The analysis did not include year 2016 (when the EC service was launched, during which there were 12 011 in-person visits) because it was an atypical period compared to the rest of the data included in the analysis.
We estimated the number of avoided visits. The dependent variable was the number of ECs in the first estimate and the number of in-person visits in the second. In both estimates, time, measured in years, was included as an independent variable. First, using simple regression analysis by the OLS method, , we estimated the number of visits that could have been avoided if EC had been available in 2014 and 2015, which was 1615.7 and 825.7, respectively, for a total of 2441.4 in-person visits that could have been avoided in those 2 years.
We also calculated the additional number of in-person visits that would have taken place in the 2016-2018 period if the EC service had not been operational. We found that without this service, there would have been an additional 5505.6 in-person visits in 2016 (an atypical year) and that 1180.8 and 2294.2 visits were avoided in 2017 and 2018, respectively.
Table 1 shows the estimated annual savings associated with the use of EC in the years that this service was available and that would have been associated with its use if the service had been available in previous years using the OLS method. We estimated the discounted present value of the cumulative savings achieved by this service between 2014 and 2018 at €127 483.84.
| Table 1. Estimated discounted present values of the savings associated with the use of email consultations in a primary care centre, applying a unit contribution margin of 0.50 | |||||
|---|---|---|---|---|---|
| Year | Cost in euro | Factor | Number of avoided visits | Yearly savings | Present value |
| 2014 | 32.04 | 0.03 | 1615.70 | 25 880.29 | 30 902.42 |
| 2015 | 31.46 | 0.03 | 825.70 | 12 987.99 | 15 056.65 |
| 2016 | 31.24 | 0.03 | 1259 | 19 665.58 | 22 133.78 |
| 2017 | 30.58 | 0.03 | 1845 | 28 210.05 | 30 825.88 |
| 2018 | 30.86 | 0.03 | 1745 | 26 925.35 | 28 565.10 |
| Suma: 12 7483.84 euros | |||||
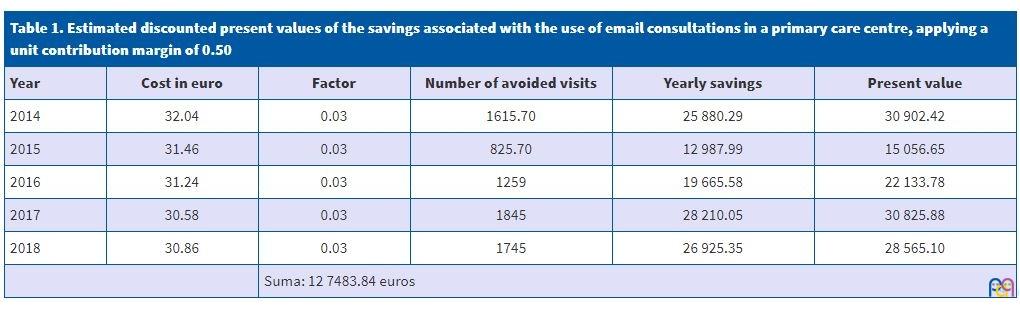
Table 2 presents the results of the sensitivity analysis, according to which yearly savings of €22 979.53 could have been achieved if this service had been available in 2014 and 2015. During the 2016-2018 period, with the EC service running, the estimated savings amounted to €27 174.92. The sensitivity analysis showed that the annual savings based on different values for the variables would range between €14 495.07 and €37 271.50 assuming each EC would have been an in-person visit.
| Table 2. Sensitivity analysis applying different unit contribution margins and real interest rates | |||||
|---|---|---|---|---|---|
| Yearly savings in euro | r = 2% | r = 2.5% | r = 3% | r = 3.5% | r = 4% |
| Unit contribution margin of 1/3 | |||||
| 2014-2015 | 14 495.07 | 14 902.64 | 15 319.69 | 15 746.38 | 16 182.90 |
| 2016-2018 | 17 608.12 | 17 861.05 | 18 116.62 | 18 374.84 | 18 635.75 |
| Unit contribution margin of 1/2 | |||||
| 2014-2015 | 21 742.6 | 22 353.96 | 22 979.53 | 23 619.58 | 24 274.35 |
| 2016-2018 | 26 412.17 | 26 791.57 | 27 174.92 | 27 562.27 | 27 953.63 |
| Unit contribution margin of 2/3 | |||||
| 2014-2015 | 28 990.14 | 29 805.29 | 30 639.38 | 31 492.77 | 32 365.81 |
| 2016-2018 | 35 216.23 | 35 722.09 | 36 233.23 | 36 749.69 | 37 271.50 |
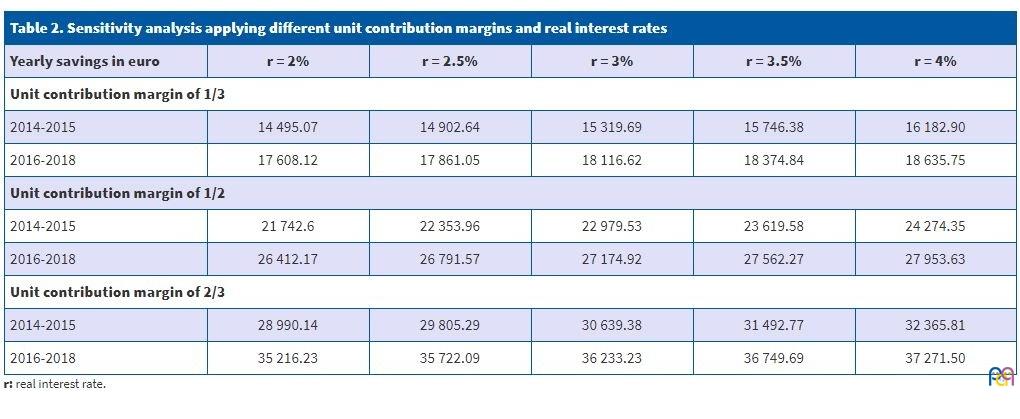
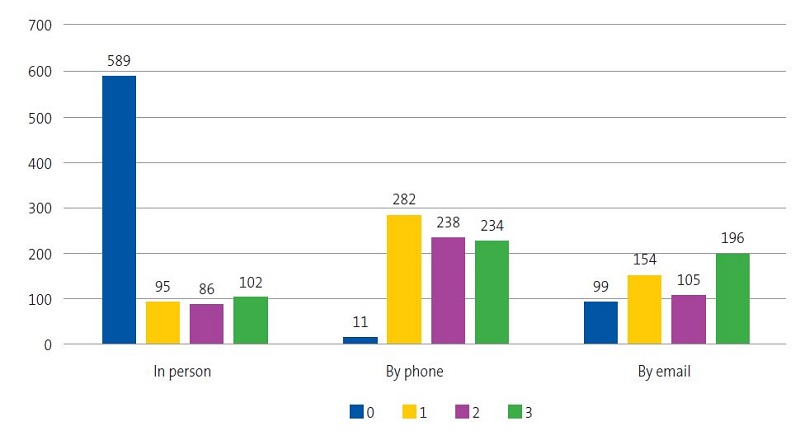
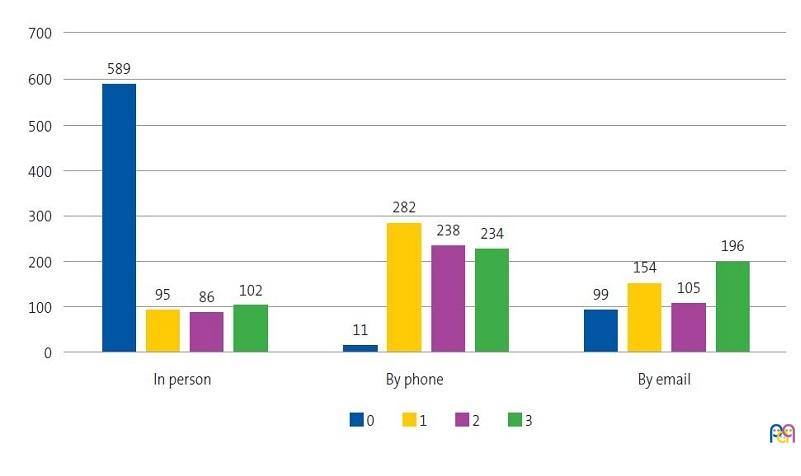
Figure 3 shows the considerable use of ECs during the COVID-19 pandemic in 2020 (19.6 emails received each weekday during the 3rd fortnight, and a mean of 15.16 ECs during the strict lockdown period). We also observed an increase in telephone consultations. Fortnight 0 corresponds to the two weeks before the lockdown, and during the pandemic there was a decrease in the number of in-person visits of nearly one sixth. The use of ECs doubled during the lockdown, as can be seen in the data for the third fortnight. The marginal use of telephone consultations before the lockdown also increased noticeably during the period that children were not allowed to leave their homes.
| Figura 3. Use of in-person and remote consultation services (by telephone and email) in the fortnights that preceded the lockdown (0) and during the lockdown (1, 2 and 3) due to the COVID-19 pandemic |
|---|
 |
DISCUSSION
Once the EC service had been operating for 2 years, we did a user satisfaction survey, and after 3 years’ operation, we performed an economic evaluation. We re-evaluated the use of the service during the COVID-19 pandemic.
In paediatrics clinical practice, this type of consultation contributes to health education through the dissemination of health information. It facilitates access to the paediatrician for emerging specific concerns, which is very useful in the rural setting. Based on the results of our survey, users were very satisfied. Miranda6 argues that this increase in user satisfaction strengthens the patient-physician relationship.
Participants in our study were young adults, parents used to new technologies that had difficulty travelling to the primary care centre on account of work, as described in other studies about family medicine and nursing.5,18
From the organizational standpoint, health care staff and tasks can be scheduled leaving aside time to answer email. This is very useful to streamline health care bureaucracy by using the most convenient time to answer email and be able to craft the response more carefully compared to a phone call or WhatsApp messaging. The use of email can decrease in the number of consultations related to administrative matters, consultations by telephone and interruptions of visits with other patients. According to González,18 it is a very useful tool in clinics with a high volume of visits.
Our study contributes new insights from an economic perspective. Email is a quick and inexpensive vehicle for communication. It saves time to the paediatrician and also the parents. We analysed the economic advantages of ECs. We found a strong economic effect upon introducing the EC service. We estimated annual savings of €14 495.07 to €37 271.50 in our primary care centre. We believe that the actual decrease in the number of in-person visits in 2016 was not due exclusively to the introduction of the email service but above all to health care reasons. But while our estimates show a sharp decrease in the number of in-person visits in 2017 and 2018, we assume that the impact of the EC service on the total number of in-person visits was probably not as large on account of the presence of additional factors. Thus, thanks to the accessibility of email, patients probably made consultations they would otherwise not had made, so that the decrease in the demand of in-person visits was not as large as expected.
The sensibility analysis showed that the economic value attributed to each consultation (made in person or by email) affects the performance of the service. Therefore, questions remain about the actual reduction in economic costs achieved by it.
From a legal standpoint, the important aspects to consider include privacy concerns, the need to establish a direct patient-physician relationship and the supplemental nature of EC.19,20 Therefore, this type of consultation should be used as a complement to in-person care. This would make ECs acceptable from an ethical standpoint.7 In our study, the service was introduced in a face-to-face contact and its use explained. A regulatory framework should be established at the international level along with reference price schedules.
Electronic consultation during the COVID-19 pandemic
The fact that the EC service had been running between 2016 and 2020, helped substituting ECs for in-person care during the lockdown imposed in the COVID-19 pandemic, contributing to maintaining isolation and preventing transmission. As we noted in the introduction, in the first three fortnights the confinement of children was strict. During the COVID-19 pandemic, in adherence with the protocols established by the Ministry of Health,21 patients with suspected COVID-19 or that had contact with a case had to be quarantined and followed up remotely with daily contact for a minimum of 15 days. The EC service was very useful for monitoring symptoms and for sending protocols for isolation, hygiene, waste management etc.
Our results (Fig. 3) show a considerable decrease in the number of in-person visits, prioritising routine healthy-child check-up visits with vaccinations and urgent acute diseases.22
The service received approximately 19.6 emails each day with pictures, and submitted reports or safe conducts (for example, to allow certain children to go on walks). The practice of teledermatology was promoted. Before the pandemic, the EC service did not contemplate submission of photographs to avoid technical issues. But the problems associated with transporting children under lockdown to the primary care centre led parents to submit images instead. Paediatricians (after obtaining parental consent) submitted these images to the dermatologist, so that a diagnosis could be made and treatment prescribed without delay. This evinces the usefulness of ECs at the primary care level.23-25 Maintaining this service and expanding it to clinics in other specialities is recommended as part of the strategic plan for reopening and for the prevention of resurgences.26
CONCLUSIONS
It is reasonable to conclude that EC is a rational application of technology to address problems or concerns that do not require in-person care. It can improve scheduling and turnaround times. Our survey revealed that users were very satisfied on account of the increased access of patients to the paediatrician. This is a supplemental tool that should never be considered a replacement for the face-to-face interaction with the patient.
Email consultation achieves an evident reduction in costs, although the estimated number of avoided in-person visits may not be as high as expected. During the COVID-19 pandemic, the EC service was indispensable to adhere to confinement measures. This service ought to be maintained to be ready to face potential resurgences.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS
COVID-19: coronavirus disease 2019; EC: email consultation.
REFERENCES
- Cobos M, Rifa A. Consulta no presencial. AMF. 2011;7:96-9.
- Bovi A, Council on Ethical and Judicial affairs of the American Medical Association. Ethical guidelines for use of electronic mail between patients and physicians. Am J Bioeth. 2003;3:W-IF2.
- Garvi P, Villanueva C, Andres E. Puesta en marcha de una consulta por correo electrónico, para dar soluciones y no para crear problemas. Rev Pediatr Aten Primaria. 2014;16:311-6.
- Mayer MA, Leis A. El correo electrónico en la relación médico-paciente: uso y recomendaciones generales. Aten Primaria. 2006;37:413-17.
- Tolosa JA, López MA, Díaz MV, Leándrez E, Marín-Barnuevo MP, García F. Uso del correo electrónico en la consulta de enfermería pediátrica en Atención Primaria. Metas enferm. 2015;18:20-5.
- Miranda M, Jadresic E, Chomali M, Miranda E, Cáceres C. El uso del correo electrónico en la comunicación médico-paciente. Rev Med Chile. 2013;141:1-3.
- Cia Gómez P. Las nuevas TIC y las consultas no presenciales. Aragón Médico. 2018;64:20-1.
- Blasco MJ, Peña G. Estudio coste-beneficio de la vacunación de varicela en Aragón. Arch Argent Pediatr. 2017;115:432-8.
- Larena I, Vara M, Peña G, Atance E, Gay B, Blasco MJ. Interrupción de la cadena del frío vacunal en un centro de Atención Primaria y su valoración económica. Enferm Clín. 2016;18:e107-e110.
- Mauskopf J, Standaert B, Connolly, MP, Culyer AJ, Garrison LP, et al. Economic Analysis of Vaccination Programs: An ISPOR Good Practices for Outcomes Research Task Force Report. Value Health. 2018;21:1133-49.
- Arnott R, Greenwald B, Stiglitz JE. Information and economic efficiency. Inform Econ Policy. 1994;6:77-82.
- Atención Primaria Zaragoza III. Zona básica de salud Valdefierro. In: Gobierno de Aragón [online] [accessed 10/03/2021]. Available at www.zaragoza3.es/Gerencia/eaps/mapas/mapa_valdefierro.htm
- The White House. OMB (Office of Management and Budget). 2003. Circular A-4: Regulatory Analysis. In: Executive Office of the President [online] [accessed 10/03/2021]. Available at www.whitehouse.gov/omb/circulars/
- Drupp MA, Freeman MC, Groom B, Nesje F. Discounting disentangled. Am Econ J Econ Policy. 2018;10:109-34.
- Goodfriend M. Interest rate policy and the inflation scare problem: 1979-1992. FRB Richmond Econ Quarterly. 1993;79:1-23.
- Boletín Oficial de Aragón (BOA) n.º 156 de 10/08/2012. In: Boletín Oficial de Aragón [online] [accessed 10/03/2021]. Available at www.boa.aragon.es/cgi-bin/EBOA/BRSCGI?CMD=VEROBJ&MLKOB=686810581515
- Resultados nacionales. In: Instituto Nacional de Estadística [online] [accessed 10/03/2021]. Available at www.ine.es/jaxiT3/Tabla.htm?t=22347
- González E, Hidalgo A, García E, Hernández M, García I. Implantación de una consulta de correo electrónico en Atención Primaria: uso del servicio y perfil de pacientes tras los tres primerio años. Med Gen Fam. 2017;6:1-14.
- Código de deontología médica. Guía de la ética médica. In: Organización Médica Colegial [online] [accessed 10/03/2021]. Available at www.cgcom.es/sites/default/files/codigo_deontologia_medica.pdf
- Electronic Communication With Patients. In: American Medical Association [online] [accessed 10/03/2021]. Available at www.ama-assn.org/delivering-care/ethics/electronic-communication-patients
- Documento técnico Manejo pediátrico en Atención Primaria del COVID-19, Versión del 18 de junio de 2020. In: Ministerio de Sanidad [online] [accessed 10/03/2021]. Available at www.mscbs.gob.es/en/profesionales/saludPublica/ccayes/alertasActual/nCov-China/documentos/Manejo_Pediatría_ap.pdf
- Albañil Ballesteros MR. Pediatría y COVID-19. Rev Pediatr Aten Primaria. 2020;22:125-8.
- Bravo J, Merino M. Uso de nuevas tecnologías en la comunicación con los pacientes, su utilidad y sus riesgos. An Pediatr (Barc). 2020;92:251-2.
- Amado AB, Villar N, Pereiro S, García L. Predisposición y validación del uso de WhatsApp como método de comunicación con familias. An Pediatr (Barc). 2019;92:300-2.
- Greenhalgh T, Choon G, Car J. COVID-19: a remote assessment in primary care. BMJ 2020;368:m1182.
- Ministerio de Sanidad, Centro de Coordinación de Alertas y Emergencias Sanitarias (CCAES), Dirección General de Salud Pública Calidad e Innovación. COVID-19: recomendaciones sanitarias para la estrategia de transición. In: Ministerio de Sanidad [online] [accessed 10/03/2021]. Available at www.mscbs.gob.es/gabinetePrensa/notaPrensa/pdf/25.04260420153138925.pdf