
Vol. 22 - Num. 88
Original Papers
Alterations in carbohydrate metabolism in paediatric patients with obesity
José M.ª Basain Valdésa, M.ª Carmen Valdés Alonsoa, Margarita Pérez Martínezb, Miriam Álvarez Viltresc, Silvia M.ª Marín Juliád
aServicio de Endocrinología. Hospital Pediátrico Docente Juan Manuel Márquez. La Habana. Cuba.
bGinecóloga. Grupo Básico de Trabajo 2. Policlínico Universitario Carlos Manuel Portuondo Lambert. La Habana. Cuba .
cMédico General Integral. Grupo Básico de Trabajo 2. Policlínico Universitario Carlos Manuel Portuondo Lambert. La Habana. Cuba.
dPediatra. Servicio de Endocrinología Pediátrica. Instituto Nacional de Endocrinología. La Habana. Cuba.
Correspondence: JM Basain. E-mail: josemb@infomed.sld.cu
Reference of this article: Basain Valdés JM, Valdés Alonso MC, Pérez Martínez M, Álvarez Viltres M, Marín Juliá SM. Alterations in carbohydrate metabolism in paediatric patients with obesity. Rev Pediatr Aten Primaria. 2020;22:371-8.
Published in Internet: 02-12-2020 - Visits: 13878
Abstract
Introduction: high prevalence of obesity in the paediatric population carries a risk of development of comorbidities, including abnormal blood glucose levels. Objective: to determine whether abnormal blood glucose levels are present in paediatric patients with obesity.
Material and methods: we conducted a cross-sectional descriptive study in 76 paediatric patients with a diagnosis of obesity managed in the Department of Endocrinology of the Juan Manuel Márquez hospital (Havana, Cuba) between January 2015 and January 2019. The variables under study were: age, sex, type of prediabetes, duration and severity of obesity. We described qualitative variables as absolute and relative frequencies and analysed the association between categorical variables with the χ2 and Fisher exact tests. We defined statistical significance as an alpha probability of 0.05.
Results: we found that 71.05% of the patients in the sample had prediabetes, of who 40.59% were female and 72.22% aged more than 10 years. There was a predominance of patients with impaired glucose tolerance (70.37%), of who 50.0% were older than 10 years and 37.04% female. We did not find a significant association between the duration of obesity and prediabetes, but we found an increase in prediabetes with increasing severity of obesity (p = 0.0095).
Conclusions: we found abnormalities in carbohydrate metabolism manifesting as prediabetes. The prevalence was higher in female patients. We did not find a significant association between the duration of obesity and prediabetes, but we found an increase in prediabetes with increasing severity of obesity.
Keywords
● Malnutrition ● Obesity ● prediabetesINTRODUCTION
In recent years there have been changes in epidemiological patterns, the most marked of which include a decrease in the incidence of infectious diseases and a gradual increase in the incidence of untransmissible chronic and progressive diseases, such as obesity and its complications,1 which are developing at increasingly early ages and have a clinical impact on children and adolescents (psychological disorders, social adjustment disorders, orthopaedic problems, hyperlipidaemia, hypertensin, sleep apnoea, among others)2.
The inflammation induced by obesity plays an important role in the development of insulin resistance, yet it is still unknown whether inflammation of adipose tissue is a cause or a consequence of insulin resistance.3
According to estimates from 34 member countries of the Organisation for Economic Co-operation and Development, 21% of girls and 23% of boys have excess weight.4 Data from the National Health and Nutrition Examination Survey (NHANES) of the United states show a prevalence of obesity of 9.5% in children aged 0-2 years and a prevalence of 16.9% in children aged 2-19 years.5
Since diabetes can be mostly asymptomatic for many years, 46% of individuals with diabetes are unaware of having the disease, and there is also a group of patients that, while not meeting the criteria for diagnosis of diabetes, have blood sugar levels that are too high to be considered normal and who are at increased risk of developing diabetes mellitus.6 This dysglycaemic state is known as prediabetes.
It has been proposed that in the transition from normal to impaired and diabetic glucose tolerance, insulin sensitivity deteriorates by about 40%, whereas insulin secretion deteriorates by 3- to 4-fold.7 At present, new concepts such as the epigenetic programming of gene expression and body composition in the foetal period, infancy and early childhood offer a better explanation for the interrelation between obesity and type 2 diabetes (T2D), leading to the coining of the term “diabesity” to refer to this issue. The basis of this assumed interrelation is that adipose tissue is considered an actual endocrine organ that secretes adipokines, which have diverse endocrine functions, and enzymes such as the aromatases and 11β-hydroxysteroid dehydrogenase (11-β-HSD), which are actively involved in hormone regulation. There is evidence of overexpression of 11-β-HSD in obese individuals, which is associated with high blood pressure, insulin resistance and dyslipidaemia, among other health problems. These are mainly associated with increased abdominal fat, which promotes the development of so-called “dysglycaemic states,” disorders of glucose metabolism of varying severity.8
Type 2 diabetes is believed to result from the chronic low-grade inflammation present in the context of obesity. However, the mechanisms that link low-grade systemic inflammation to obesity and T2D are poorly understood, although several have been investigated, such as the function of the intestinal microbiota, which plays an important role in obesity due to the increased intestinal permeability, which results in higher levels of circulating lipopolysaccharides (LPS) from gram-positive bacteria in the gut. Lipopolysaccharides can trigger a proinflammatory cascade by activating pattern recognition receptors in adipocytes, such as toll-like receptor 4 (TLR4, a LPS receptor), leading to low-grade systemic inflammation, insulin resistance and eventually T2D.9
The obesity-insulin resistance relationship is most likely causal, as demonstrated by studies that show that weight gain/loss is unquestionably correlated to a decrease/increase in insulin sensitivity.10
Prediabetes is an old term first coined by the World Health Organization as a retrospective diagnosis that described the condition of an individual prior to diagnosis of diabetes mellitus.11 At present, the American Diabetes Association uses the term with prospective implications, so that a given blood glucose or post-load glucose level would be a predictor of future development of the corresponding individuals of a prediabetic state, diabetes or increased risk of cardiovascular complications.12
The term dysglycaemia encompasses different abnormalities, such as impaired fasting glucose (IFG), impaired glucose tolerance (IGT), combined or double prediabetes (presence of both IFG and IGT) and diabetes itself. Impaired fasting glucose is defined as a fasting glucose greater than 5.6 mmol/l and less than 7.1 mmol, IGT as is defined as 2-hour glucose levels of 7.8 to 11.0 mmol/l on the oral glucose tolerance test, and combined prediabetes as meeting the criteria for both IFG and IGT.8 The duration of dysglycaemia varies, as it is directly associated to its natural history, and is estimated to range from 7 to 10 years. Of the total individuals that develop prediabetes, 70% eventually progress to diabetes.11
The term IGT was introduced in 1979 and reflects peripheral resistance to insulin activity, while the term IFG emerged in 1997 and reflects increased gluconeogenesis in the liver and impaired early insulin secretion. Both are considered intermediate states between normal glucose tolerance and diabetes.11
Several epidemiological studies suggest that lowering the cut-off point used to define the normal fasting glucose range to 5.6 mmol/l would optimise the sensitivity and specificity of this test in predicting the likelihood of T2D, especially in individuals with obesity and hypertriglyceridemia, introducing the concept of “fasting dysglycaemia”. Fasting dysglycaemia, as an expression of insulin resistance at the level of the liver, has exhibited a correlation of approximately 0.7 with peripheral insulin resistance.13
Given this current global and domestic situation, we wondered about the patterns of carbohydrate intolerance in paediatric patients with obesity managed in the specialised obesity clinic of our hospital.
The aim of our study was to assess abnormalities in carbohydrate metabolism in paediatric patients with obesity managed in the specialised obesity clinic of the Department of Paediatric Endocrinology of the Hospital Pediátrico Docente Juan Manuel Márquez in the period ranging from January 2015 to January 2019.
MATERIAL AND METHODS
We conducted a cross-sectional descriptive study in 76 patients with obesity diagnosed according to the World Health Organization standards (N = n = 76) of both sexes aged 1 to 18 years and managed in the specialised obesity clinic of the Department of Endocrinology of the Hospital Pediátrico Docente Juan Manuel Márquez between January 2015 and January 2019. We stratified the sample, which resulted in the following distribution: 38 male patients (19 aged less than 10 years and 19 aged 10 or more years) and 38 female patients (19 aged less than 10 years and 19 aged 10 or more years). We excluded patients with genetic or endocrine-metabolic disorders, drug-induced obesity or whose health records did not include all the necessary information for the analysis.
The variables under study were age, sex, presence of prediabetes, type of prediabetes, duration of obesity and degree of obesity. We retrieved the following information from patient health records: age, sex and duration of obesity. We measured the weight and height of every patient, after which we measured the fasting blood glucose level and the glucose level at 2 hours.
Based on the weight and height measurements, we calculated the body mass index (BMI) applying the Quetelet formula: BMI = weight (kg)/height (m2). Once we had calculated the BMI, we found the percentile for each patient in the growth charts for age and sex for the Cuban population. We defined obesity as a BMI above the 97th percentile for sex in the Cuban charts.
Blood samples were obtained by venepuncture following a 12-hour fast at the clinical laboratory of the Hospital Pediátrico Docente Juan Manuel Márquez. Blood glucose measurements were made at the same laboratory with the glucose oxidase method.
We entered the data in an Excel 2003 spreadsheet to create an automated database. We summarised the data as absolute frequency and percentage distributions. We analysed the association between categorical variables with the Fisher exact test and the χ2 test of independence, and considered it statistically significant if p <0,05. As for ethical considerations, we requested the informed consent from the parents or legal guardians of all patients, and the study was approved by the scientific committee and the research ethics board of the hospital.
RESULTS
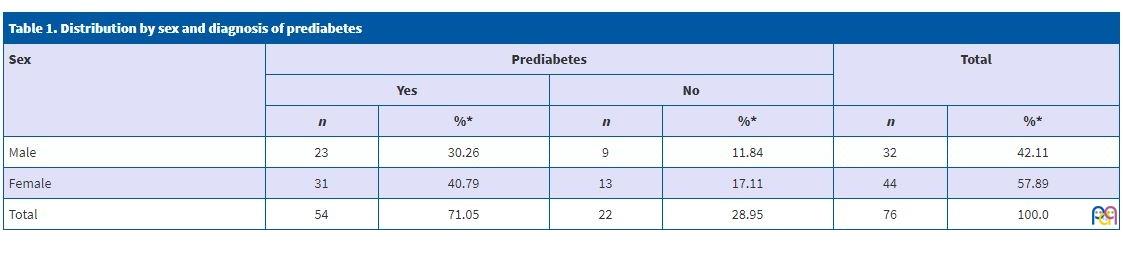
Table 1 shows the distribution of the sample by sex and diagnosis of prediabetes. We found prediabetes in 71.05% of patients, with a higher prevalence in female patients (40.79%).
| Table 1. Distribution by sex and diagnosis of prediabetes | ||||||
|---|---|---|---|---|---|---|
| Sex | Prediabetes | Total | ||||
| Yes | No | |||||
| n | %* | n | %* | n | %* | |
| Male | 23 | 30.26 | 9 | 11.84 | 32 | 42.11 |
| Female | 31 | 40.79 | 13 | 17.11 | 44 | 57.89 |
| Total | 54 | 71.05 | 22 | 28.95 | 76 | 100.0 |
The age distribution by type of prediabetes is shown in Table 2. We did not find a statistically significant association between age and type of prediabetes (p = 0.9572), although 70.37% of patients had IGT, 22.22% IFG and a very small minority (7.41%) combined prediabetes.
| Table 2. Age distribution of the different types of prediabetes | ||||||||
|---|---|---|---|---|---|---|---|---|
| Age (years) | IGT | IFG | IGT/IFG | Total | ||||
| n | %* | n | %* | n | %* | n | %* | |
| <10 | 11 | 20.37 | 3 | 5.56 | 1 | 1.85 | 15 | 27.78 |
| ≥10 | 27 | 50.0 | 9 | 16.67 | 3 | 5.56 | 39 | 72.22 |
| Total | 38 | 70.37 | 12 | 22.22 | 4 | 7.41 | 54 | 100.0 |
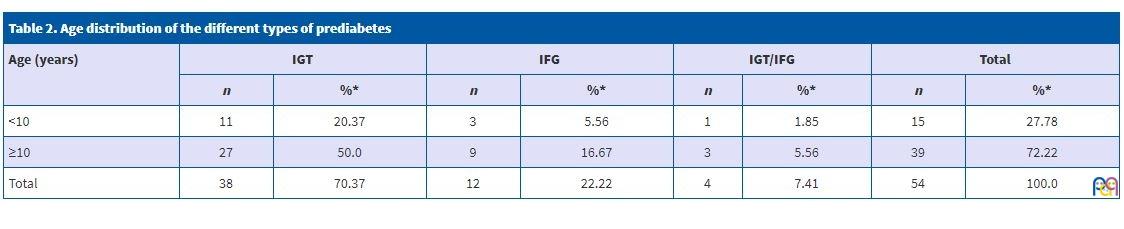
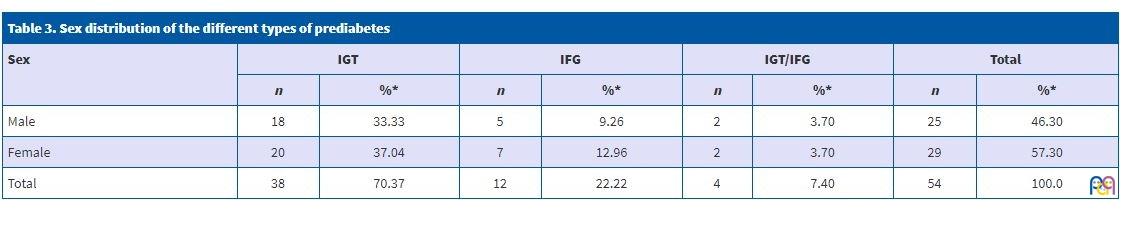
Table 3 presents the sex distribution of the different types of prediabetes. As can be seen, there was no significant association between these two variables.
| Table 3. Sex distribution of the different types of prediabetes | ||||||||
|---|---|---|---|---|---|---|---|---|
| Sex | IGT | IFG | IGT/IFG | Total | ||||
| n | %* | n | %* | n | %* | n | %* | |
| Male | 18 | 33.33 | 5 | 9.26 | 2 | 3.70 | 25 | 46.30 |
| Female | 20 | 37.04 | 7 | 12.96 | 2 | 3.70 | 29 | 57.30 |
| Total | 38 | 70.37 | 12 | 22.22 | 4 | 7.40 | 54 | 100.0 |
The distribution of patients with prediabetes based on the duration of obesity and sex can be found in Table 4. We found that changes in glucose levels were not significantly associated with the duration of obesity (p = 0.7640).
| Table 4. Distribution of patients with prediabetes by duration of obesity and sex | ||||||
|---|---|---|---|---|---|---|
| Duration of obesity (years) | Sex | Total | ||||
| Male | Female | |||||
| n | %* | n | %* | n | %* | |
| <5 | 6 | 11.11 | 8 | 14.81 | 14 | 25.93 |
| ≥5 | 19 | 35.19 | 21 | 38.89 | 40 | 74.07 |
| Total | 25 | 46.30 | 29 | 53.70 | 54 | 100.0 |
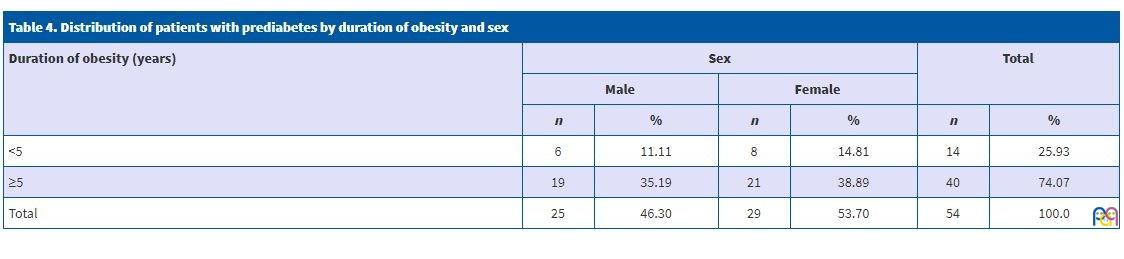
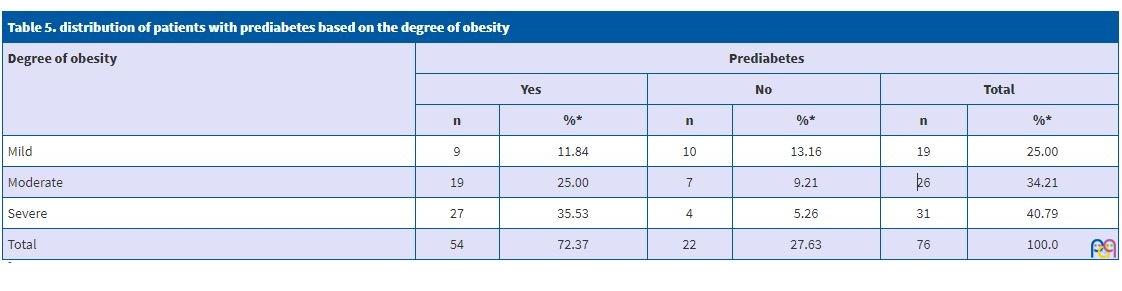
Table 5 shows the distribution of patients with prediabetes based on the degree of obesity. We found a statistically significant association between these two variables (p = 0.0095).
| Table 5. distribution of patients with prediabetes based on the degree of obesity | ||||||
|---|---|---|---|---|---|---|
| Degree of obesity | Prediabetes | |||||
| Yes | No | Total | ||||
| n | %* | n | %* | n | %* | |
| Mild | 9 | 11.84 | 10 | 13.16 | 19 | 25.00 |
| Moderate | 19 | 25.00 | 7 | 9.21 | 26 | 34.21 |
| Severe | 27 | 35.53 | 4 | 5.26 | 31 | 40.79 |
| Total | 54 | 72.37 | 22 | 27.63 | 76 | 100.0 |
DISCUSSION
Few domestic articles have been published in Cuba allowing to draw firm conclusions on the prevalence of diabetes. González Tabares et al.6 consider that this is due to the diagnosis of glycaemia not being something that can be completed at once, but a process involving several measures: fasting glucose, oral glucose tolerance test and more recently the concentration of glycated haemoglobin (HbA1c). Most published studies are based on patient self-reporting rather than experiments or tests. Using this approach, a time series conducted in the Ciego de Ávila province found a very low prevalence of diabetes, of only 2.89%, and did not contribute any data on prediabetes.14
A study by Girón Bombull et al.in 50 prediabetic patients residing in the village of Boniato in the province of Santiago de Cuba11 found a predominance of the female sex (92.0% of cases), which was consistent with the findings of González et al.,15 who found that out of the 40 cases included in their study, 29 corresponded to female patients, which is also in agreement with our own findings.
In 2009, a study conducted by Valdés et al.16 found a greater prevalence of IGT compared to IFG. In addition, the American Diabetes Association17 considers that IFG is a better predictor of the risk of diabetes
A study by Girón Bombull et al.11 in 2012 in the village of Boniato in Santiago de Cuba found a prevalence of fasting glucose intolerance of 64.0%.
The frequency of abnormal fasting glucose levels found in the study by Bustillo Solano et al.18 on the prevalence of diabetes and IFG in a neighbourhood of the city of Sancti Spíritus was 25.22%.
Our online search of the biomedical literature did not yield any other studies on the prevalence of IFG in other cities or provinces in Cuba.
A recent study conducted in four cities in India found frequencies of IFG or IGT ranging from 8.1 to 14.6%.19
It has not been established with certainty whether IGT and IFG are two stages in a continuum of disease that ranges from normal glucose tolerance to T2D or two distinct forms of glucose tolerance impairment.20 There is variability between studies in the diagnosis of these two states, and the greater frequency of IFG detected in our study was consistent with the findings of studies in several other regions such as the United States, China, Denmark, India21 and, within Cuba, the study conducted in the municipality of Centro Habana, in which 16.1% of the sample had abnormal fasting glucose levels,22 while the study conducted in Sancti Spíritus found a high prevalence of IFG of 25.22%.18 These results were consistent with the results of our study.
In our study we found a greater number of patients of both sexes with prediabetes and none with diabetes mellitus, as well as an increase directly associated with age with a predominance of IFG, which was consistent with the findings of Arteaga et al.23 but diverged from the findings of Alayón et al.24 in Cartagena de Indias, where the prevalence of diabetes was greater.
A study conducted by Díaz Díaz et al.8 in 1982 patients that visited the clinics of the Instituto Nacional de Endocrinología (National Institute of Endocrinology) due to suspected T2D, found that the most frequent type of dysglycaemia in male patients was IFG, detected in 95 patients in the sample (20.9%), followed by diabetes mellitus in 60 patients (13.2%), combined prediabetes in 38 patients (8.4%) and IGT in 25 patients (5.55%), while the most frequent type of dysglycaemia in female patients was IFG, found in 36 patients in the sample (6.9%), followed by IGT in 31 patients (5.9%), combined prediabetes in 24 patients (4.6%) and diabetes mellitus in 19 (3.6%).
A study conducted in a Chinese population studied the impact of different blood glucose levels through performance of oral glucose tolerance tests in normoglycaemic subjects and comparing the quartiles. The study found a clear positive relationship between increasing blood glucose levels and obesity.25
In a population-based study on adults conducted in Trujillo in 2011, Castillo et al.26 found a gradual increase in the BMI associated with the increase in abnormal fasting glucose levels.
The findings of our study highlight the need to actively screen for prediabetes, which is the starting point to initiate the investigation of this disorder of carbohydrate metabolism and to start interventions to prevent it at the primary care level.
CONCLUSIONS
We found abnormalities in carbohydrate metabolism manifesting as prediabetes. We found a higher prevalence in female patients and patients aged 10 or more years. We did not find an association between prediabetes and the duration of obesity, but we did find an association between prediabetes and the severity of obesity.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS
11-β-HSD: 11-β- hydroxysteroid dehydrogenase · T2D: type 2 diabetes · IFG: impaired fasting glucose · BMI: body mass index · LPS: lipopolysaccharides · NHANES: National Health and Nutrition Examination Survey · IGT: impaired glucose tolerance.
REFERENCES
- Muzzo BS, Monckeberg BF. Reflexiones sobre el aumento de la obesidad en Chile. Rev Chil Nutr. 2012;39:113-5.
- Rodríguez Domínguez L, Fernández-Britto Rodríguez JE, Díaz Sánchez ME, Ruiz Álvarez V, Hernández Hernández H, Herrera Gómez V, et al. Sobrepeso y dislipidemias en adolescentes. Rev Cubana Pediatr. 2014;86:433-44.
- Bluher M. Adipose tissue inflammation: a cause or consequence of obesity-related insulin resistance? Clin Sci (Lond). 2016;130:1603-14.
- Saavedra JM, Dattilo AM. Factores alimentarios y dietéticos asociados a la obesidad infantil: recomendaciones para su prevención antes de los dos años de vida. Rev Peruana Med Exp Salud Pública. 2012;29:379-85.
- Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999-2008. JAMA. 2010;303:235-41.
- González Tabares R, O’Relly Noda D, Guirola Fuentes J, Pérez Barly L, Acosta González FA, Navarro de Armas OL. Disglucemia y aterosclerosis en población laboralmente activa. Rev Cubana Med Militar. 2016;45:277-90.
- Gross Melo FJ, Huamán Saavedra JJ, Gonzáles Saldaña J, Gutiérrez Arana J, Álvarez Vargas M, Osada Liy JE. Características de los componentes del síndrome metabólico en pacientes con glucosa normal y disglicemia en ayunas. Rev Med Hered. 2018;29:137-46.
- Díaz Díaz O, Hernández Rodríguez J, Domínguez Alonso E, Martínez Montenegro I, Bosch Pérez Y, del Busto Mesa A, et al. Valor de corte de la circunferencia de la cintura como predictor de disglucemia. Rev Cubana Endocrinol. 2017;28:1-15.
- Cruz Sánchez JJ. Niveles plasmáticos de adiponectina e interleucina-1beta y su asociación con marcadores antropométricos, bioquímicos y clínicos en mujeres adultas mexicanas con obesidad y diabetes mellitus tipo 2. [Master of Science in Nutrition thesis]. Monterrey: Universidad Autónoma de Nuevo León; 2018.
- Godínez-Gutiérrez SA, Valerdi-Contreras L. Obesidad: resistencia endocrina múltiple. Rev Endocrinol Nutr. 2012;20(4):152-68.
- Girón Bombull JA, Fernández González A, Trujillo Feliciano Y, Ramos Labrada N, Silva Durán O. Caracterización clinicoepidemiológica de la prediabetes. MEDISAN. 2013;17:2096-3000.
- Díaz Díaz O. Primer consenso cubano de prediabetes. Rev Cubana Endocrinol. 2011;22:1.
- Buchaca Faxas EF. La pesquisa de los trastornos asintomáticos de la glucemia es una necesidad. Rev Cubana Endocrinol. 2013;24:103-6.
- Ramírez Leyva E, Álvarez Aldana D, García Moreiro R, Álvarez Fernández M, Rodríguez Bebet Y, Matos Valdivia Y. Diabetes mellitus en Ciego de Ávila: serie secular 1997-2008. Rev Cub Endocrinol. 2009;20.
- González Suárez RM, Perich Amador P, Arranz Calzado C. Heterogeneidad de los trastornos metabólicos de las etapas iniciales de la diabetes mellitus 2. Rev Cubana Endocrinol. 2009;20.
- Valdés S, Delgado E. Epidemiología de la prediabetes en España. Av Diabetol. 2009;25:99-104.
- American Diabetes Asociation. Standards of medical care in diabetes. Diabetes Care. Actualización Médica Periódica. 2009;32:S13-S61.
- Bustillo Solano EE, Bustillo Madrigal EE, Pérez Francisco Y, Pérez Sosa R, Brito García A, González Iglesia A, et al. Prevalencia de la diabetes mellitus y de la glucemia alterada en ayunas en un área de la ciudad de Sancti Spíritus. Rev Cubana Endocrinol. 2013;24:107-24.
- Di Flaviani A, Picconi F, Di Stefano P, Giordani I, Malandrucco I, Maggio P, et al. Impact of glycemic and blood pressure variability on surrogate measures of cardiovascular outcomes in type 2 diabetic patients. Diabetes Care. 2011;34:1605-9.
- Valdés Gómez W, Leyva Álvarez de la Campa G, Espinosa Reyes TM. Prediabetes y riesgo cardiovascular en población de alto riesgo en Atención Primaria de salud. Revista ALAD. 2014;4:22-9.
- Díaz Díaz O, Cabrera Rode E, Orlandi González N, Araña Rosaínz MJ, Díaz Horta O. Aspectos epidemiológicos de la prediabetes, diagnóstico y clasificación. Rev Cubana Endocrinol. 2011;22:3-10.
- Bermúdez S, Buchaca E,SuárezY, RodríguezL, Alonso CA, Mansur M, et al. Trastornos de la glucemia y de la acción de la insulina en una población de riesgo de diabetes. Rev Cubana Endocrinol. 2009;20:120-30.
- Arteaga A, Pollak F, Robres L, Velasco N. Características clínicas y metabólicas de los estados de intolerancia a la glucosa y glicemia de ayuno alteradas. Rev Méd Chile. 2009;137:193-9.
- Alayón AN, Alvear C. Prevalencia de desórdenes del metabolismo de los glúcidos y perfil del diabético en Cartagena de Indias (Colombia), 2005. Salud Uninorte Barranquilla (Col.). 2006;22:20-8.
- Thomas GN, McGhee SM, Schooling CM. Determinants of normoglycemia and contribution to cardiovascular risk factors in a Chinese population: the Hong Kong Cardiovascular Risk Factor Study. J Endocrinol Invest. 2006;29:528-35.
- Castillo K, Ríos M, Huaman J. Frecuencia y características de la glicemia basal alterada en adultos de Trujillo según criterios diagnósticos. Acta Médica Peru. 2011;28:132-45.