
Vol. 22 - Num. 88
Original Papers
Impact of an educational intervention about asthma on early childhood and primary education teachers in one health district
Ana Fierro Urturia, Raquel Acebes Puertasb, Alicia Córdoba Romeroc, Sara del Amo Ramosd, Mónica Sanz Fernándeza
aPediatra. CS Pisuerga. Arroyo de la Encomienda. Valladolid. España.
bPediatra. Servicio de Pediatría. Hospital Universitario Río Hortega. Valladolid. España.
cMédico de Familia. CS Pisuerga. Arroyo de la Encomienda. Valladolid. España .
dMédico de Familia. CS Pisuerga. Arroyo de la Encomienda. Valladolid. España.
Correspondence: A Fierro. E-mail: anfier99@gmail.com
Reference of this article: Fierro Urturi A, Acebes Puertas R, Córdoba Romero A, del Amo Ramos S, Sanz Fernández M. Impact of an educational intervention about asthma on early childhood and primary education teachers in one health district. Rev Pediatr Aten Primaria. 2020;22:353-60.
Published in Internet: 23-11-2020 - Visits: 15797
Abstract
Introduction: an appropriate knowledge about asthma by teachers in schools is essential for its control. Objective: to determine the impact of an educational intervention on the knowledge of teachers about asthma and its management in the primary schools located in one health district.
Patients and methods: quasi-experimental pre-post intervention study assessing an educational intervention aimed at improving the knowledge on asthma of teachers. A questionnaire was administered before, immediately after and 6 months after the educational intervention.
Results: 100 teachers (69.93%) employed in 5 schools participated in the study. The mean age was 44.2 ± 8 years (range, 28-59 years), 82% were women. We found a low level of asthma knowledge in the teaching staff. Many participants could identify the main symptoms of asthma (65%) and the main triggers (59%). Thirty percent did not know whether these students could participate in competitive sports, and 26% believed it was not possible to prevent exercise-induced asthma attacks. Seventy-nine percent knew that inhaled therapy was the best approach. Seven percent stated that antibiotics are a component of asthma treatment. Five percent believed salbutamol could damage the heart. After the educational intervention, we noticed a significant increase on asthma knowledge (p <0.001). The level of knowledge was maintained 6 months after the intervention.
Conclusions: educational interventions aimed at teachers significantly increase the level of asthma knowledge. This improvement is maintained for at least 6 months. Educational activities and organizational measures on asthma are necessary in the school setting.
Keywords
● Asthma ● Educational advice ● School centresINTRODUCTION
Asthma is the most prevalent chronic disease in childhood in developed countries and has a significant impact on individuals, families, society and the economy.1 It is a leading cause of school absenteeism and of hospital admission in children.
In Spain, the prevalence of asthma is of 9-10%, similar to the prevalence in the rest of the European Union.2,3
Clinical guidelines for the management and treatment of asthma highlight education as a key determinant in the improvement of asthma control.
In the case of children, this education must be extended to family members and other adult caregivers.4
In the school years, children spend 30% of the time in the school setting, to which we need to add any extracurricular activities, during which teachers are responsible for their supervision.
Given the prevalence of asthma, most teachers will face situations related to this disease in their students at some point in their career.
Appropriate decision-making in the management of asthmatic children in the school setting may be hindered by a lack of knowledge about the disease on the part of the teaching staff, a lack of resources, a lack of management protocols and formal assignment of responsibilities in asthma care to specific individuals or inadequate communication between families and the school/teaching staff about the condition and specific needs of the child.5-7
Assessing the knowledge of teachers about asthma to determine whether educational interventions are needed is important, as the main current guidelines and consensus documents on the management of asthma recommend educational intervention as one of the pillars in treatment and followup.8,9
Schools rarely have specific protocols on the management of asthma. Such protocols must address the distribution of responsibilities in the care for students with asthma, the channels of communication between families and the school, and the need for an individualised asthma action plan detailing the specific needs of each student with asthma in terms of medication and triggers.10
In recent years, several studies have assessed the circumstances and knowledge of teachers as regards the management of asthma. They all agree that teachers have little knowledge and training on this disease but would like to be better informed on the subject.11-14
Other countries have ample experience in the delivery of asthma education programmes in schools. In Spain, we ought to highlight the programme promoted in Andalusia by the Group on Asthma Education and Health (GESA) and the Study on Asthma in Spanish Schools (EACCE).15-18
The most successful asthma education programmes are those that involve health care professionals, teachers and families.5,19,20
MATERIAL AND METHODS
The research team included 3 paediatricians, 2 family physicians, 3 nurses and 1 midwife.
The study was conducted in 2 phases:
- Phase 1. Cross-sectional observational and descriptive study by means of a survey of the knowledge of childhood asthma of teachers in early childhood and primary education schools located within one health district in the city of Valladolid.
- Phase 2. Quasi-experimental pre-post intervention study with implementation of an educational intervention (EI) aimed at improving the knowledge, attitudes and beliefs regarding childhood asthma and its management in the teaching staff of the participating schools. The same questionnaire used in the initial assessment was administered immediately after the intervention and 6 months later.
Study setting: 5 early childhood and primary education schools in our health district. All participating schools were public, as there are no private schools within our health district.
Study period: phase 1, January-June 2018; phase 2, September 2018-February 2019.
Inclusion criteria: teaching and non-teaching staff of the schools in the health district under study that agreed to participate in the study.
We obtained the approval of the administrators of the selected schools before starting the study.
Measurements: the instrument used in the survey was a self-administered questionnaire filled out on a voluntary and anonymous basis that had been developed by the researchers based on a literature review and their own experience.17,18,21,22 Variables under study: school-related: type of school, ownership (public/private); participant-related: age, sex, teacher/staff, year taught, general knowledge about asthma and its management.
The questionnaire consisted of 10 items: 5 single-answer multiple choice questions and 5 true-false questions.
It was administered initially before the intervention, immediately after its completion and 6 months after to assess whether the intervention had fostered greater understanding, a change in behaviour and assimilation of the taught contents in the short and medium terms.
The educational intervention was developed taking as reference the most salient projects for asthma education in schools in Spain.15,24-26
The intervention included a descriptive theoretical component and a practical component, both of which were delivered with an interactive approach to the teaching staff during school hours, and lasted 90 minutes.
The contents of the theoretical component were: basic anatomy and physiology of the respiratory system, definition of asthma, aetiology, triggers, symptoms, assessment of severity of exacerbations, diagnosis, approaches to treatment and control, description of inhalers and directions for their optimal use, prevention and treatment of exercise-induced asthma, fieldtrips and extracurricular activities in children with asthma.
We explained the requirements and organizational system that need to be established in schools (asthma ID card for the child, individualised asthma action plan, stocking of emergency care supplies in the first aid kit, healthy school environment, reduction of allergens in classrooms and grounds, lunchroom and allergies).
In the practical component, we taught the correct use of inhalers and how to respond to an asthma exacerbation.
The training was delivered with PowerPoint presentations and videos. In the practical component, we used placebo inhalers and spacers.
Statistical analysis: the analysis was performed with the software SPSS v. 15.0 (SPSS Inc. 1989-2006). We analysed the missing data in the survey and the distribution of missing responses for every variable under study. We considered a proportion of 15% for missing values in any given variable a potential source of information bias in the study.
Descriptive statistics: quantitative variables were described as mean ± standard deviation (SD) or median and interquartile range (IQR) depending on whether the data followed a normal distribution. On the other hand, we described qualitative variables as the absolute and relative (percentage) frequency distributions of their categories.
Bivariate analysis: we analysed the association between qualitative variables by means of the χ2 test along with the Fisher exact test or likelihood ratios, and the differences between paired proportions using the McNemar test or the Cochran Q as applicable. We defined statistical significance as p <0,05 in any of the tests.
Ethical and legal considerations: the study adhered to international ethical principles, mainly the Declaration of Helsinki (Fortaleza, Brazil, 2013). The study protocol was evaluated and approved by the Ethics Committee on Research Involving Medicines of the Valladolid Oeste health district.
We requested the informed consent of teachers for participation in the study. We safeguarded the confidentiality of the obtained information in adherence with current law (Organic Law 15/1999 on the Protection of Personal Data).
RESULTS
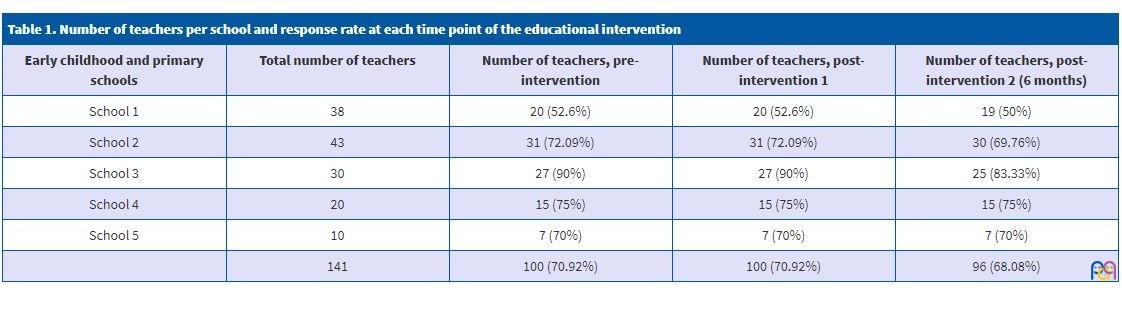
All the early childhood and primary education schools located in our health district (n = 5), which employed 141 teachers, participated in the study. We received responses to the questionnaire from 105 teachers. Incomplete questionnaires were excluded from the analysis. Table 1 presents information on the number of participating schools, number of teachers included in the survey and the response rate.
| Table 1. Number of teachers per school and response rate at each time point of the educational intervention | ||||
|---|---|---|---|---|
| Early childhood and primary schools | Total number of teachers | Number of teachers, pre-intervention | Number of teachers, post-intervention 1 | Number of teachers, post-intervention 2 (6 months) |
| School 1 | 38 | 20 (52.6%) | 20 (52.6%) | 19 (50%) |
| School 2 | 43 | 31 (72.09%) | 31 (72.09%) | 30 (69.76%) |
| School 3 | 30 | 27 (90%) | 27 (90%) | 25 (83.33%) |
| School 4 | 20 | 15 (75%) | 15 (75%) | 15 (75%) |
| School 5 | 10 | 7 (70%) | 7 (70%) | 7 (70%) |
| 141 | 100 (70.92%) | 100 (70.92%) | 96 (68.08%) | |
The mean age of respondents was 44.2 ± 8 years (range: 28-59), and there was a predominance of female teachers (82%).
The distribution of respondents based on the cycle of education they taught was: 35% early childhood education, 57% primary education, and 8% both.
Knowledge of teachers about asthma
Table 2 presents the results. Eighty-seven percent of respondents considered their knowledge inadequate. All knew that asthma is not an infectious disease and believed that with adequate treatment most patients can have a normal life (92%). However, 30% did not know whether children with asthma could engage in competitive sports and 7% believed they could not.
| Table 2. Questionnaire on the knowledge of asthma, answers, and statistical significance | ||||||
|---|---|---|---|---|---|---|
| Item | Answer | Pre-intervention answers n (%) |
Post-intervention 1 answers n (%) |
p | Post-intervention 2 answers n(%) |
p |
| 1. Do you think your knowledge of asthma is adequate? | Yes | 13 (13%) | 85 (85%) | <0.001 | 84 (87.5%) | <0.001 |
| No | 87% | 15% | 12 (12.5%) | |||
| 2. Asthma is infectious, can be transmitted from one person to another | True | 0 | 0 | 0 | ||
| False | 100 (100%) | 100 (100%) | 96 (100%) | |||
| I don’t know | 0 | 0 | 0 | |||
| 3. With adequate treatment, individuals with asthma can have normal lives | True | 92 (92%) | 100 (100%) | 0.0115 | 96 (100%) | 0.0136 |
| False | 4% | 0 | 0 | |||
| I don’t know | 4% | 0 | 0 | |||
| 4. Mark the possible symptoms in an asthma attack | Cough | 1 (1%) | 0 | <0.001 | 0 | <0.001 |
| Difficulty breathing | 10 (10%) | 0 | 0 | |||
| Cough and difficulty breathing | 8 (8%) | 0 | ||||
| Wheezing and difficulty breathing | 15 (15%) | 0 | 0 | |||
| All of the above | 66 (66%) | 100 (100%) | 96 (100%) | |||
| 5. Mark which triggers can cause asthma | Infections | 1 (1%) | 0 | <0.001 | 0 | <0.001 |
| Allergies | 19 (19%) | 0 | 0 | |||
| Exercise | 3 (3%) | 1 (1%) | 2 (2.1%) | |||
| Infections and allergies | 4 (4%) | 0 | 0 | |||
| Infections and exercise | 1 (1%) | 0 | 0 | |||
| Allergies and exercise | 13 (13%) | 1 (1%) | 1 (1%) | |||
| All of the above | 59 (59%) | 98 (98%) | 93 (96.9%) | |||
| 6. In the event of an asthma attack, the best response is … | Oral medication | 0 | 0 | <0.001 | 0 | <0.001 |
| Inhaled medication | 79 (79%) | 100 (100%) | 96 (96%) | |||
| Have student lie down and drink water | 1 (1%) | 0 | 0 | |||
| I don’t know | 20 (20%) | 0 | 0 | |||
| 7. Antibiotics are an important component of treatment | True | 7 (7%) | 2 (2%) | 0.117 | 0 | 0.024 |
| False | 67 (67%) | 95 (95%) | <0.001 | 95 (99%) | <0.001 | |
| I don’t know | 26 (26%) | 3 (3%) | <0.001 | 1 (1%) | <0.001 | |
| 8. Some asthma drugs (Ventolin) damage the heart | True | 5 (5%) | 0 | 0.070 | 0 | 0.077 |
| False | 41 (41%) | 100 (100%) | <0.001 | 95 (99%) | <0.001 | |
| I don’t know | 54 (54%) | 0 | <0.001 | 1 (1%) | <0.001 | |
| 9. Children with asthma cannot do competitive sports | True | 7 (7%) | 2 (2%) | 0.172 | 0 | 0.024 |
| False | 63 (63%) | 96 (96%) | <0.001 | 96 (100%) | <0.001 | |
| I don’t know | 30 (30%) | 2 (2%) | 0.001 | 0 | <0.001 | |
| 10. Ways to prevent an exercise-induced asthma attack. Mark the false answer | Previous warmup | 23 (23%) | 3 (3%) | <0.001 | 2 (2.1%) | <0.001 |
| Avoid cold air | 17 (17%) | 8 (8%) | 0.087 | 2 (2.1%) | 0.001 | |
| Administration of bronchodilator beforehand | 34 (34%) | 12 (12%) | <0.001 | 5 (5.2%) | <0.001 | |
| Cannot be prevented | 26 (26%) | 77 (77%) | <0.001 | 87 (90.6%) | <0.001 | |
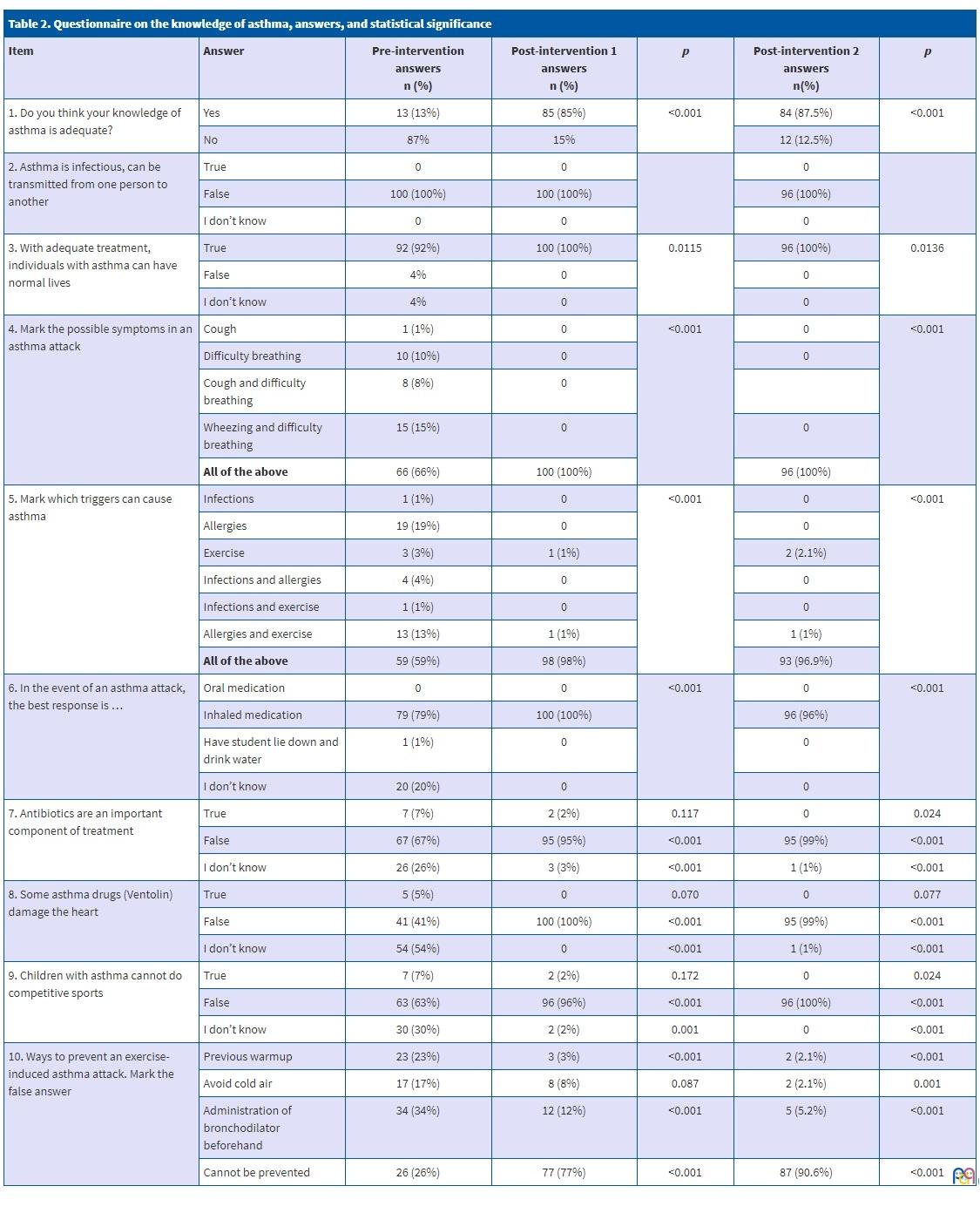
In the assessment of the knowledge on the symptoms of asthma, 65% identified the main symptoms (cough, difficulty breathing, wheezing) and the rest only identified some of them.
Fifty-nine percent considered that infections, allergies and exercise were the main triggers of asthma attacks, while 19% only selected allergies.
When it came to the management of asthma exacerbations, 79% stated that the most effective approach was to administer inhaled medication.
Seven percent believed that antibiotics were included in the treatment of asthma, and 26% did not know whether they should be used.
As for the adverse effects of anti-asthmatic drugs, 5% of respondents believed that salbutamol (Ventolin) caused heart damage.
Lastly, concerning what could be done to prevent an asthma attack during physical activity, 26% responded that it could not be prevented.
Educational intervention
Table 2 shows the differences in the percentage of answers to each question compared to the previous timepoints at which the questionnaire was administered.
We observed a significant increase in the knowledge on asthma after the educational intervention, (p <0.001) which was maintained at 6 most post intervention.
DISCUSSION
Clinical guidelines for the management of asthma recommend patient education as a key intervention to improve wellbeing through self-care. In the case of children, this recommendation extends to the adults in charge of their care.
During the school year, children spend more than half of their time in school, where teachers are in charge of their supervision and care. For this reason, it is important to determine how much teachers know about asthma and identify training needs.
Our study describes the knowledge, attitudes and beliefs of teachers regarding asthma and assessed the impact of an educational intervention. The results provide an essential basis to understand the real-world situation in our area, provide adequate information to this professional collective and assess the efficacy of the intervention.
One of the limitations of our study was its non-randomised experimental design, and that participation of teachers was voluntary. Another of the limitations was the use of a questionnaire that was not validated, developed by the research team based on the findings of a literature review10,17,18,21,22 and their professional experience, selecting the most representative items used in the past.
The overall response rate was good (70.92%), similar to the response rate reported in many of the previous studies in the literature.12,16 we ought to highlight the greater proportion of female respondents (82%), a predominance that was also found in the EACEE study conducted in different Spanish cities.16
Most teachers considered their knowledge of asthma inadequate, which was consistent with the findings of previous studies.10,16
Although most respondents believed that children with asthma could lead a normal life with adequate treatment, a significant proportion did not know whether these children could engage in competitive sports, and 26% believed that exercise-induced asthma exacerbations could not be prevented, which could limit what they may perceive these students can do.
When it came to the knowledge about asthma, we ought to highlight the high percentage (66%) that correctly identified 3 symptoms of asthma, which was higher compared to the reports of other authors.12,15,16,23
As for the erroneous beliefs regarding the deleterious effects of anti-asthmatic agents, half of the respondents were unsure whether the use of salbutamol could damage the heart, a concern that could restrict the response of teachers to an asthma exacerbation.
On the subject of asthma triggers, slightly more than half of the respondents (59%) identified all the possible triggers, a proportion that was similar to those found in other studies12,16 and greater compared to the proportion found by Korta Murua et al. in schools in Guipúzcoa.23
Our findings and those of other studies reveal significant gaps in knowledge that may impact the care and management of students with asthma.
After the educational intervention, the knowledge on asthma of participating teachers improved significantly.
Recommended by the main current guidelines and consensus documents on asthma, educational intervention is one of the pillars in the management of asthma. The results of our study agreed with those of previous authors, demonstrating that the educational intervention was effective in improving knowledge and that the effects persisted in the short and medium terms. 12,23,27
Based on our findings, and in agreement with previous studies, it would be beneficial to establish an adequate programme for education on asthma and its management in the school setting, addressing the basics on the subject and with booster sessions to maintain the acquired level of knowledge over time.5,8,15,16,19,20,23,27,28
CONCLUSIONS
The information that teachers receive about asthma is scarce and not standardised. Educational interventions delivered by health care professionals in the school setting are effective in increasing and improving the knowledge of teachers about asthma.
Health education intervention strategies must be developed based on the identified needs and implemented at regular intervals.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS
EACCE: Estudio sobre el asma en los Centros Escolares Españoles (Study on asthma in Spanish Schools) · EI: educational intervention · GESA: Grupo de educación y salud en asma (Group on Asthma Education and Health) · IQR: interquartile range · SD: standard deviation
REFERENCES
- Chronic respiratory diseases: Asthma. In: World Health Organization [online] [accessed 18/11/2020]. Available at http://www.who.int/respiratory/asthma/en/
- Ellwood P, Asher MI, Beasley R, Clayton TO, Stewart AW, ISAAC Steering Committee. The International Study of Asthma and Allergies in Childhood (ISAAC): Phase Three Rationale and Methods. Int J Tuberc Lung Dis. 2005;9:10-6.
- Carvajal-Ureña I, García Marcos L, Busquets-Monge R, Morales M, García N, Batles Garrido J, et al. Geographic variation in the prevalence of asthma symptoms in spanish children and adolescents. International Study of Asthma and Allergies in Childhood (ISAAC) Phase 3, Spain. Arch Bronconeumol. 2005;41:659-66.
- GEMA 4.3. Guía Española para el manejo del Asma 2018 [online] [accessed 18/11/2020]. Available at www.gemasma.com/
- Bruzesse JM, Evans D, Kattan M. School-based asthma programs. J Allergy Clin Immunol 2009;124:195-200.
- Figuerola Mulet J. Escenarios de la educación. Praena Crespo M (ed.). VII Curso de Educadores en Asma. CD-ROM. 1st Seville: Wanceulen; 2010.
- Coffman JM, Cabana MD, Yelin EH. Do School-Based Asthma Education Programs Improve Self-Management and Health Outcomes? Pediatrics. 2009;124:729-42.
- Korta Murúa J, López-Silvarrey Varela A. Asma, educadores y escuela. An Pediatr (Barc). 2011;74:141-4.
- Global Strategy for Astha management and prevention, global initiative for asthma. In: GINA. Global Initiative for Asthma [online] [accessed 18/11/2020]. Available at www.ginasthma.org
- Cobos N, Picado C. Estudio piloto de los conocimientos sobre asma y su tratamiento entre los educadores españoles. Med Clin (Barc). 2001;117:452-3.
- Wheeler L, Buckley R, Gerald LB, Merkle S, Morrison TA. Working with schools to improve pediatric asthma management. Pediatr Asthma Allergy Immunology. 2009;22:197-207.
- Henry RL, Gibson PG, Vimpani GV, francis JL, Hazell J. Randomized controlled trial of a teacher-led asthma education program. Pediatr Pulmonol. 2004;38:434-42.
- Sapien RE, Fullerton-Gleason L, Allen N. Teaching school teachers to recognize respiratory distress in asthmatic chidren. J Asthma. 2004;41:739-43.
- Rodríguez Fernández-Oliva CR,Torres Álvarez de Arcaya ML, Aguirre Jaime A. Conocimientos y actitudes del profesor ante el asma del alumno. An Pediatr (Barc). 2010;72:413-9.
- Praena Crespo M (coord.). Asma, deporte y salud. Proyecto de educación en asma en centros de enseñanza. Seville: Junta de Andalucía, Consejería de Salud; 2008.
- López-Silvarrey Varela A (coord.). Estudio sobre el asma en los centros escolares españoles (EACEE) 2009-2010. In: Fundación María José Jove [online] [accessed 18/11/2020]. Available at www.fundacionmariajosejove.org/inicio/areas-de-actividad/salud/investigacion/estudio-sobre-el-asma-en-los-centros-escolares-espanoles-eacee-20092010/
- Praena Crespo M, Lora Espinosa L, Aquino Linares N Sánchez Sánchez A, Jiménez Cortés A. Versión española del NAKQ. Adaptación transcultural y análisis de fiabilidad y validez. An Pediatr (Barc). 2009;70:209-17.
- López-Silvarrey Varela A, Pértega Díaz S, Iglesias López B, Rueda Esteban S. Validación de un cuestionario en español sobre conocimientos de asma en profesores. XXXII Reunión de la Sociedad Española de Neumología Pediátrica. An Pediatr (Barc). 2010;72:57.
- Praena Crespo M, Fernández Truhán JC, Morales Lozano JA, Navarro Montano MJ, Jiménez Cotes A, Gálvez González J, et al. Diseño de un programa de educación en asma para profesores de educación física de centros de enseñanza secundaria. Rev Pediatr Aten Primaria. 2008;10 Suppl2:71-2.
- Patterson E, Brennan MP, Linskey KM, Webb DC, Shields MD, Patterson CC. A cluster randomised intervention trial of asthma clubs to improve quality of live in primary school children: The School Care and Asthma Management Project (SCAMP). Arch Dis Child. 2005;90:786-91.
- Snow R, Larkin M, Kimball S, Iheagwara K, Ozuah P. Evaluation of asthma management policies in New York City public schools. J Asthma. 2005;1:51-3.
- Getch Y, Neuhart-Pritchett S. Teacher asthma management an information seeking scale. J Asthma. 2007;44:497-500.
- Korta Murua J, Pérez-Yarza EG, Pértega Díaz S. Impacto de una intervención educativa sobre asma en profesores. An Pediatr (Barc). 2012;77:236-46.
- Centro de Estudios de la Enfermedad Asmática (CESEA). Asma en los centros escolares. In: Sociedad Española de Neumología Pediátrica [online] [accessed 18/11/2020]. Available at https://neumoped.org/wp-content/uploads/2019/05/Guia-Asma-Centros-Escolares-1.pdf
- Guía de ayuda para centros docentes. Manejo práctico de los problemas de salud pediátricos más frecuentes. In: Asociación Española de Pediatría de Atención Primaria [online] [accessed 18/11/2020]. Available at https://www.aepap.org/grupos/grupo-de-educacion-para-la-salud/biblioteca/guia-aepap-para-centros-docentes
- Plan de actuación ante una crisis de asma en los centros educativos. In: Sociedad Española de Inmunología Clínica, Alergología y Asma Pediátrica [online] [accessed 18/11/2020]. Available at http://www.seicap.es/es/plan-de-actuaci%C3%B3n-ante-crisis-asm%C3%A1tica-en-centros-educativos_37440
- Domínguez Aurrecoechea B, González Guerra L, Mola Caballero de Rodas P, Alonso Lorenzo J. Ayúdanos a vivir con asma: intervención educativa escolar. ¿Qué conocen los profesores del asma? Rev Pediatr Aten Primaria. 2008;10:e73.
- Gawward ES, El-Herishi S. Asthma education for school staff in Riyadh city: effectiveness of pamplhlets as an educational tool. J Egypt Public Health Assoc. 2007;82:147-71.