
Vol. 22 - Num. 87
Original Papers
Adolescent lifestyle and its influence on oral health
Antonia Alcaina Lorentea, Virginia Saura Lópezb, Ana Pérez Pardob, Sonia Guzmán Pinac, Olga Cortés Lillod
aUnidad de Odontopediatría. Facultad de Medicina y Odontología. Universidad de Murcia. Unidad de Odontopediatría. Hospital General Universitario Morales Meseguer. Murcia. España.
bOdontóloga. Murcia. España.
cUnidad de Odontopediatría. Facultad de Medicina y Odontología. Universidad de Murcia. Murcia. España.
dUnidad de Odontopediatría. Departamento de Dermatología, Estomatología, Radiología y Medicina Física. Facultad de Medicina y Odontología. Universidad de Murcia. Murcia. España.
Correspondence: O Cortés . E-mail: ocortes@um.es
Reference of this article: Alcaina Lorente A, Saura López V, Pérez Pardo A, Guzmán Pina S, Cortés Lillo O. Adolescent lifestyle and its influence on oral health. Rev Pediatr Aten Primaria. 2020;22:251-61.
Published in Internet: 17-07-2020 - Visits: 21848
Abstract
Introduction: the high prevalence of oral disease in adolescents, together with the direct or indirect association between disease and lifestyle habits, call for the implementation of oral health prevention and promotion strategies at the school, household and public health levels. Our main objective was to design a questionnaire on lifestyle habits in adolescents to determine their prevalence and assess their association with oral health.
Materials and methods: we conducted a cross-sectional observational study in 39 preadolescent and adolescent students aged 12 to 17 years. We developed a 42-item questionnaire and administered it to participating students. We analysed the obtained responses using contingency tables, defining statistical significance as a p-value of <0.05.
Results: we found that the frequency of brushing was correct in 54% of participating students, while only 48.7% visit the dentist every year. We found a significant association between nationality and visits to the dentist (p = 0.02) and between the frequency of brushing with: eating breakfast (p = 0.005), consumption of industrial baked goods or snacks (p = 0.02) and consumption of sugary drinks (p = 0.011), the use of computer, television and gaming consoles (p = 0.049), and a sedentary lifestyle (p = 0.00).
Conclusion: we found statistically significant associations between lifestyle habits and oral health. The development and implementation of oral health prevention and promotion strategies targeting the adolescent population is essential in order to establish adequate habits that will not have a detrimental effect on the general health of the adolescent.
Keywords
● Adolescent ● Healthy habits ● Lifestyles ● Oral health ● Unhealthy habitsINTRODUCTION
The World Health Organization (WHO) defines adolescence as the phase of life between childhood and adulthood, from ages 10 to 19.1
When we talk about lifestyle, we are referring to the way of life of an individual or subset of the population influenced by personal characteristics and behavioural patterns, such as living conditions and sociocultural aspects.
The collection of positive habits and behaviours that an adolescent engages in will play a role in ensuring a satisfactory level of wellbeing, as well as good health and quality of life in the future. On the other hand, unhealthy lifestyles will have deleterious effects on health.2
Among the lifestyle habits that have a positive or negative impact on oral health in adolescents are those related to physical activity, of which a higher level is required in childhood and adolescence.
It is recommended that the paediatric population engages in at least 1 hour of physical activity a day 4 or 4 days a week, while restricting the time devoted to sedentary activities, such as videogames, to less than 2 hours a day.3,4
Nutrition in adolescence is of great importance when it comes to future adult health. It is one of the main lifestyle factors that affect health and quality of life. Adequate nutrition ensures correct growth and reduces the risk of developing obesity and dental caries.5,6
Screen time corresponds to the sum of the time spent watching television, playing videogames, surfing the web and using cell phones. It is a new construct that can translate to a good or bad habit depending on time devoted to these activities each day, with more than 2 hours a day considered excessive.7
Another bad habit that usually starts in adolescence is smoking. Today, the number of adolescents that smoke is increasing globally, especially female adolescents.8
Furthermore, today’s adolescents either have or want piercings, a deleterious habit when it comes to oral health as the mouth is a habitual site for piercings, especially the lips, tongue, check, uvula or a combination thereof.9
Thus, taking into account all the habits mentioned above, adolescence is an important stage for health prevention and promotion during which beneficial habits can be established. There is evidence that certain behaviours (especially unhealthy ones) do not occur in isolation, but are combined to form a constellation of risk behaviours during adolescence.10
Oral health is an essential part of general health. In adolescence, there are two very common oral health problems: caries and gingivitis. This is due to hormone changes and a decline in dental care. Instilling good oral hygiene habits in adolescents is providing them with a correct pattern of behaviour that can be maintained through life, making them understand the importance it has in everyday life.11,12
Thus, efforts in oral health education are extremely important. In addition, adolescence is a phase characterised by change during which habits are established that will affect the present and future health of the adolescent.
The aims of our study were to establish the prevalence of certain lifestyle habits in preadolescents and adolescents and their association with oral health by means of a questionnaire, to then identify health promotion strategies that could be applied to this specific subset of the population.
MATERIAL AND METHODS
We conducted a cross-sectional observational study in a sample of 39 preadolescent and adolescent students of both sexes aged 12-13 years and 15-17 years, respectively. There were 2 groups, one including 22 students enrolled in year 1 of compulsory secondary education in Spain (ESO), and another including 17 students enrolled in year 4 of the ESO (Table 1). The study was carried out in the 2018-2019 academic year at the Francisco de Goya Secondary Education School in Molina de Segura, in the autonomous community of Region of Murcia, Spain.
| Table 1. Sample | ||
|---|---|---|
| Age group | n | % |
| 12-13 years | 22 | 56.41 |
| 15-17 years | 17 | 43.59 |

After informing the administration of the school about the survey we wished to conduct, we obtained the approval of the principal first, followed by the agreement of the entire teaching staff and then the broader school community.
Questionnaire design and development
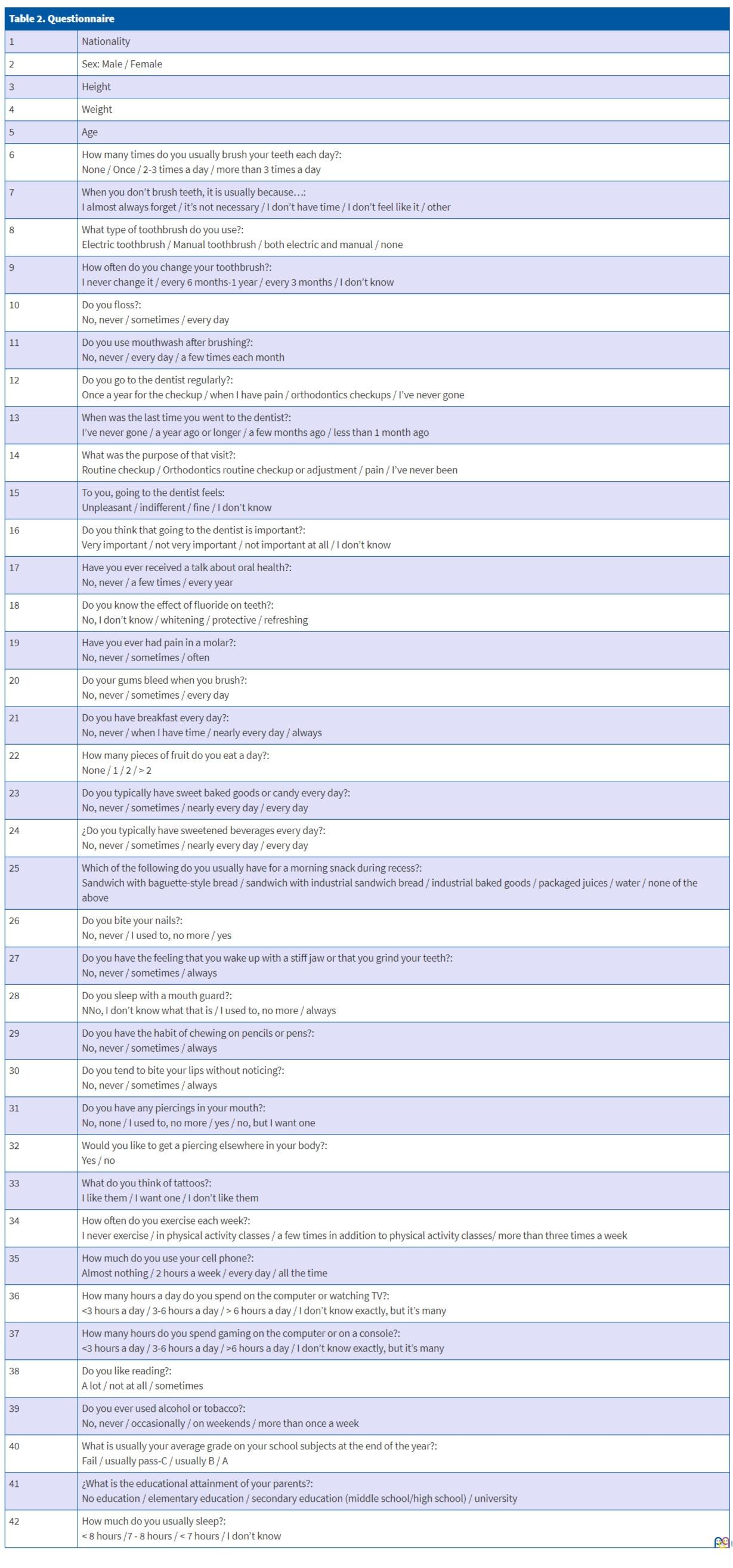
Table 2 presents the questionnaire, which comprised 42 items distributed into 4 sections on healthy and unhealthy habits. The variables measured in the questionnaire explored the personal characteristics of the student as well as specific lifestyle habits. The students filled out the questionnaire on the appointed date. In the days preceding the survey, we obtained the informed consent of the parents and collected data on the weight and height of the adolescents.
| Table 2. Questionnaire | |
|---|---|
| 1 | Nationality |
| 2 | Sex: Male / Female |
| 3 | Height |
| 4 | Weight |
| 5 | Age |
| 6 | How many times do you usually brush your teeth each day?: None / Once / 2-3 times a day / more than 3 times a day |
| 7 | When you don’t brush teeth, it is usually because…: I almost always forget / it’s not necessary / I don’t have time / I don’t feel like it / other |
| 8 | What type of toothbrush do you use?: Electric toothbrush / Manual toothbrush / both electric and manual / none |
| 9 | How often do you change your toothbrush?: I never change it / every 6 months-1 year / every 3 months / I don’t know |
| 10 | Do you floss?: No, never / sometimes / every day |
| 11 | Do you use mouthwash after brushing?: No, never / every day / a few times each month |
| 12 | Do you go to the dentist regularly?: Once a year for the checkup / when I have pain / orthodontics checkups / I’ve never gone |
| 13 | When was the last time you went to the dentist?: I’ve never gone / a year ago or longer / a few months ago / less than 1 month ago |
| 14 | What was the purpose of that visit?: Routine checkup / Orthodontics routine checkup or adjustment / pain / I’ve never been |
| 15 | To you, going to the dentist feels: Unpleasant / indifferent / fine / I don’t know |
| 16 | Do you think that going to the dentist is important?: Very important / not very important / not important at all / I don’t know |
| 17 | Have you ever received a talk about oral health?: No, never / a few times / every year |
| 18 | Do you know the effect of fluoride on teeth?: No, I don’t know / whitening / protective / refreshing |
| 19 | Have you ever had pain in a molar?: No, never / sometimes / often |
| 20 | Do your gums bleed when you brush?: No, never / sometimes / every day |
| 21 | Do you have breakfast every day?: No, never / when I have time / nearly every day / always |
| 22 | How many pieces of fruit do you eat a day?: None / 1 / 2 / > 2 |
| 23 | Do you typically have sweet baked goods or candy every day?: No, never / sometimes / nearly every day / every day |
| 24 | ¿Do you typically have sweetened beverages every day?: No, never / sometimes / nearly every day / every day |
| 25 | Which of the following do you usually have for a morning snack during recess?: Sandwich with baguette-style bread / sandwich with industrial sandwich bread / industrial baked goods / packaged juices / water / none of the above |
| 26 | Do you bite your nails?: No, never / I used to, no more / yes |
| 27 | Do you have the feeling that you wake up with a stiff jaw or that you grind your teeth?: No, never / sometimes / always |
| 28 | Do you sleep with a mouth guard?: NNo, I don’t know what that is / I used to, no more / always |
| 29 | Do you have the habit of chewing on pencils or pens?: No, never / sometimes / always |
| 30 | Do you tend to bite your lips without noticing?: No, never / sometimes / always |
| 31 | Do you have any piercings in your mouth?: No, none / I used to, no more / yes / no, but I want one |
| 32 | Would you like to get a piercing elsewhere in your body?: Yes / no |
| 33 | What do you think of tattoos?: I like them / I want one / I don’t like them |
| 34 | How often do you exercise each week?: I never exercise / in physical activity classes / a few times in addition to physical activity classes/ more than three times a week |
| 35 | How much do you use your cell phone?: Almost nothing / 2 hours a week / every day / all the time |
| 36 | How many hours a day do you spend on the computer or watching TV?: <3 hours a day / 3-6 hours a day / > 6 hours a day / I don’t know exactly, but it’s many |
| 37 | How many hours do you spend gaming on the computer or on a console?: <3 hours a day / 3-6 hours a day / >6 hours a day / I don’t know exactly, but it’s many |
| 38 | Do you like reading?: A lot / not at all / sometimes |
| 39 | Do you ever used alcohol or tobacco?: No, never / occasionally / on weekends / more than once a week |
| 40 | What is usually your average grade on your school subjects at the end of the year?: Fail / usually pass-C / usually B / A |
| 41 | ¿What is the educational attainment of your parents?: No education / elementary education / secondary education (middle school/high school) / university |
| 42 | How much do you usually sleep?: < 8 hours /7 - 8 hours / < 7 hours / I don’t know |
Statistical analysis
In an initial phase, we carried out a descriptive analysis of the collected responses. We analysed the association between quantitative variables and between qualitative variables by means of the χ2 test to identify significant differences, comparing tables of descriptive statistics and contingency tables. We defined statistical significance as p <0.05. The statistical analysis was performed with the software package SPSS 19.0 in the Department of Biostatistics of the School of Medicine of the Universidad de Murcia.
RESULTS
Descriptive analysis
The sample included 39 adolescents aged 12-17 years. Table 3 presents the distribution of the variables under analysis in the overall sample.
| Table 3. Variable distribution | |||||
|---|---|---|---|---|---|
| Sample characteristics (n = 39) | |||||
| n | % | n | % | ||
| Nationality | Oral piercings | ||||
| Spanish | 34 | 87.2 | None | 32 | 82.1 |
| Not Spanish | 5 | 12.8 | Used to have, none now | 1 | 2.6 |
| Frequency of brushing | Yes | 0 | 0 | ||
| None | 1 | 2.6 | None, but I want some | 6 | 15.4 |
| Once a day | 11 | 28.2 | Perception of tattoos | ||
| 2-3 times a day | 21 | 53.8 | I like them | 17 | 43.6 |
| >3 times a day | 6 | 15.4 | I want to get one | 10 | 25.6 |
| Dental visits | I don’t like them | 11 | 28.2 | ||
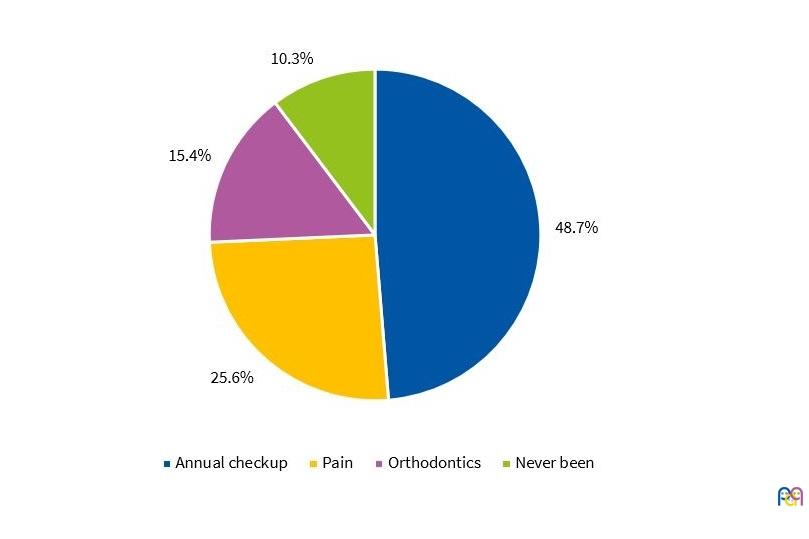
| Once a year for checkup | 19 | 48.7 | Frequency of physical activity | ||
| For pain | 10 | 25.6 | Never | 1 | 2.6 |
| For orthodontics | 6 | 15.4 | In PE class | 9 | 23.1 |
| Never been | 4 | 10.3 | A few times in addition to PE class | 13 | 33.3 |
| Breakfast | >3 times/ week | 16 | 41.0 | ||
| Never | 3 | 7.7 | Frequency of cell phone use | ||
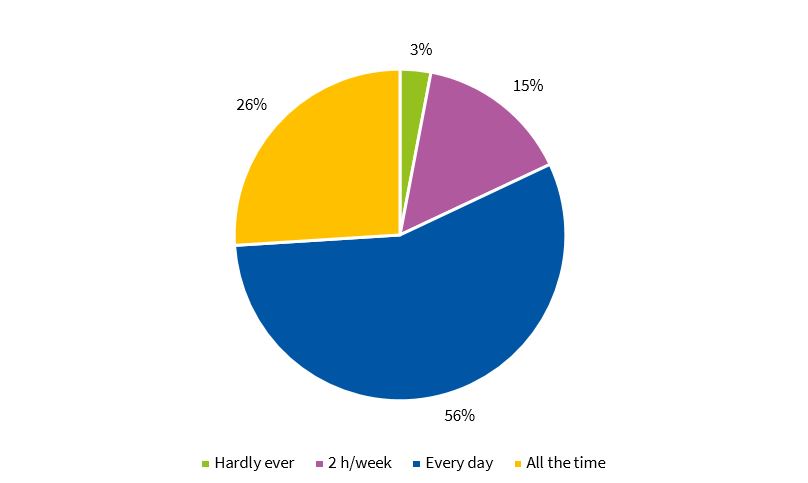
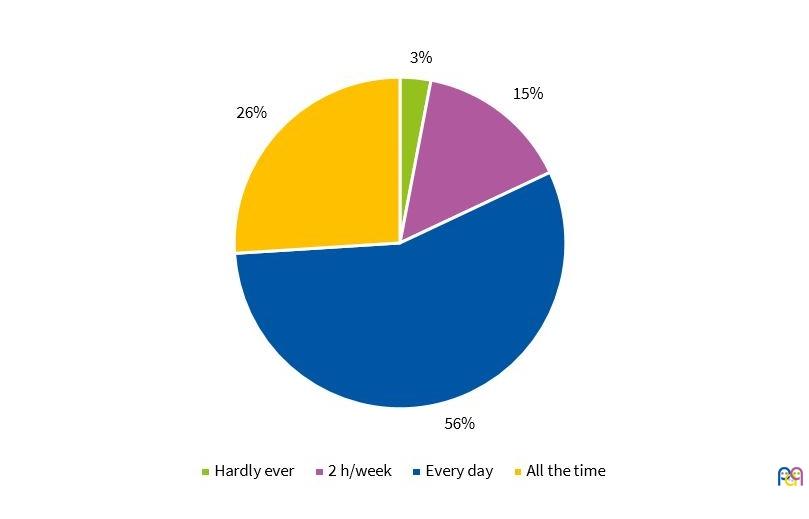
| When I have time | 5 | 12.8 | Almost never | 1 | 2.6 |
| Nearly every day | 6 | 15.4 | 2 hours/week | 6 | 15.4 |
| Every day | 25 | 64.1 | Every day | 22 | 56.4 |
| Consumption of sweet baked goods | All the time | 10 | 25.6 | ||
| Never | 7 | 17.9 | Screen time at computer/watching television (hours) | ||
| Sometimes | 24 | 61.5 | <3 h/day | 25 | 64.1 |
| Nearly every day | 8 | 20.5 | 3-6 h/day | 10 | 25.6 |
| Every day | 0 | 0 | >6 h/day | 1 | 2.6 |
| Time spent gaming on computer/console (hours) | I don’t know, but many | 3 | 7.7 | ||
| <3 h/day | 29 | 74.4 | Mean grade in school | ||
| 3-6 h/day | 6 | 15.4 | Fail | 6 | 15.4 |
| > 6 h/day | 1 | 2.6 | Pass/C | 15 | 38.5 |
| I don’t know, but many | 3 | 7.7 | B | 13 | 33.3 |
| A | 5 | 12.8 | |||
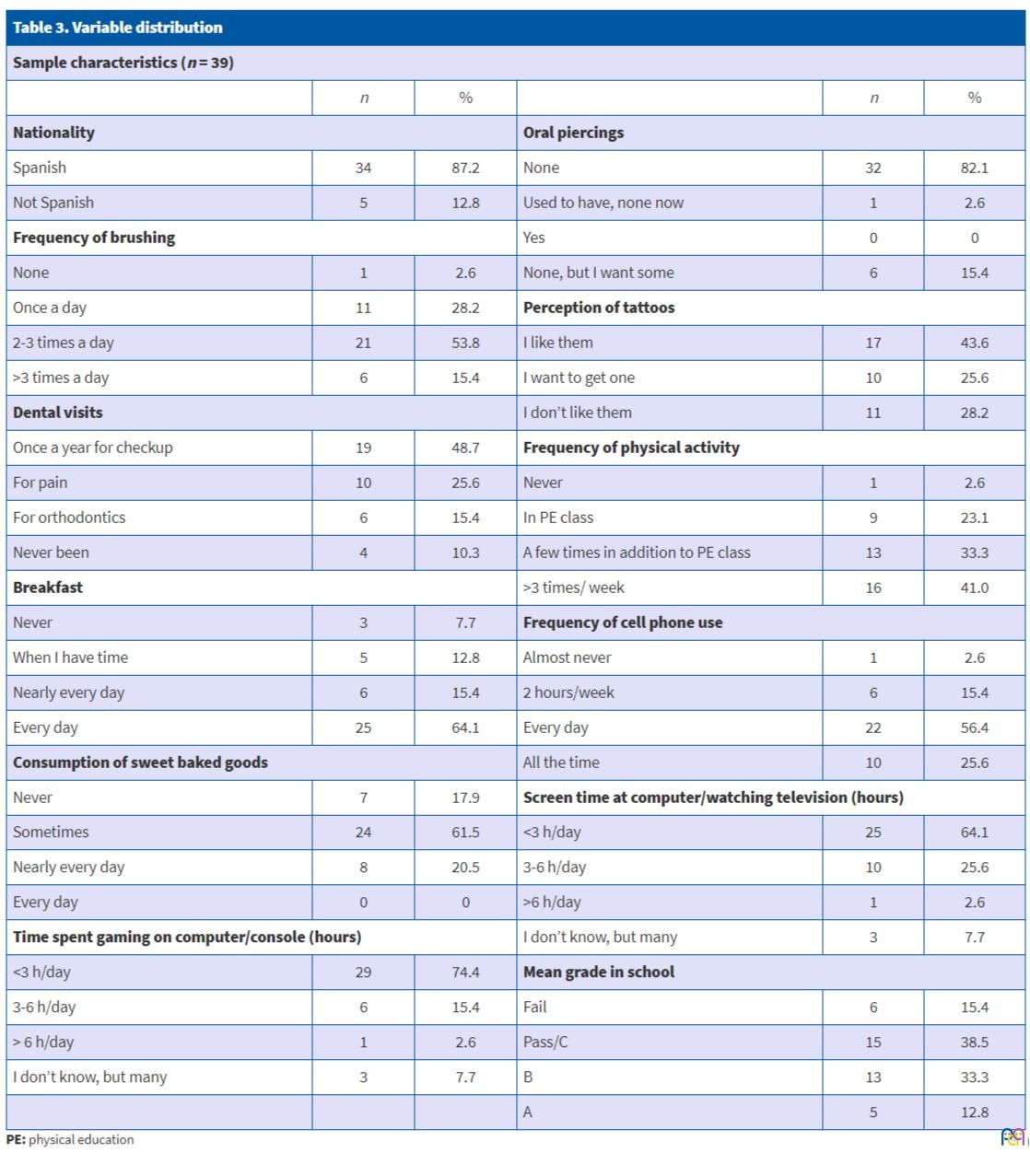
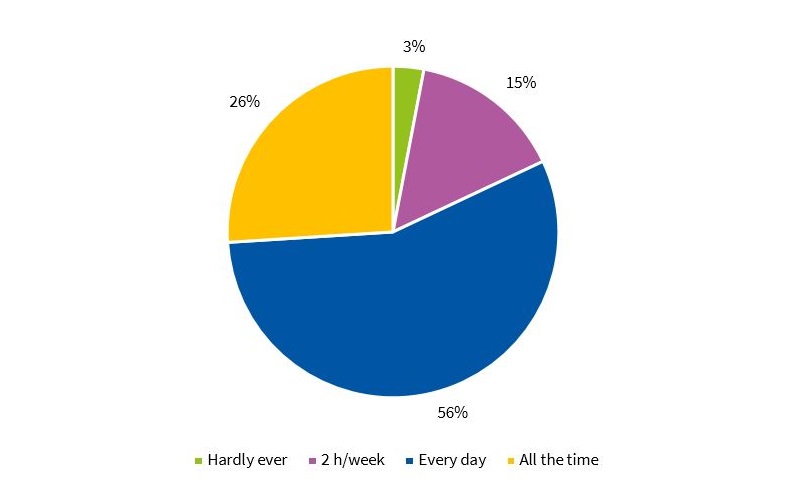
The most relevant findings were that most participants were Spanish (87.2%), and that 58.8% brushed their teeth 2 to 3 times a day (Fig. 1), although 10.3% had never had an appointment with a dentist (Fig. 2). Three percent reported that they never had breakfast, and 15.4% reported consuming sweet baked goods nearly every day. Nearly half (41%) engaged in physical activity more than 3 times a week, while 56.4% reported daily cell phone use (Fig. 3).
| Figure 1. Frequency of brushing |
|---|
 |
| Figure 2. Frequency of visits to dentist |
|---|
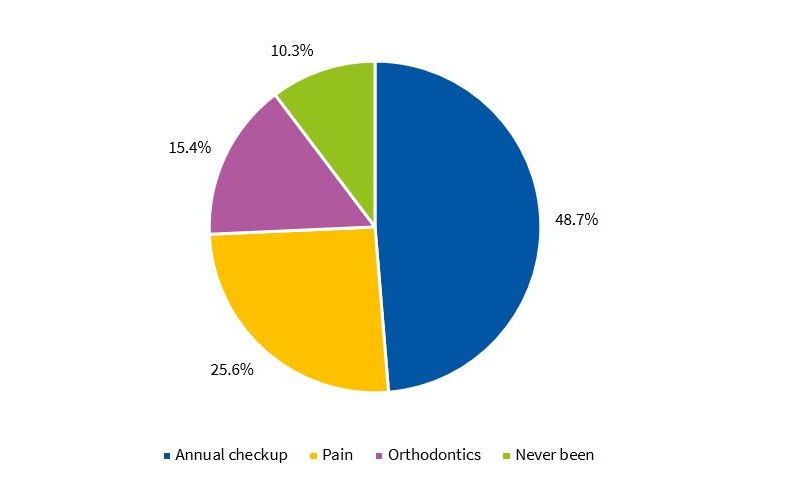 |
| Figure 3. Frequency of cell phone use |
|---|
 |
Inferential analysis
We used contingency tables to analyse the association between variables.
We found a significant association between nationality and the frequency of visits to the dentist. Adolescents of non-Spanish nationality did not visit the dentist yearly, whereas Spanish adolescents visited the dentist every year or every month (p = 0.02).
We also found that non-Spanish adolescent were more likely to report episodes of tooth pain compared to Spanish adolescents (p = 0.035).
When it came to dietary habits, we found the following significant patterns: adolescents that did not have breakfast every day brushed their teeth fewer times a day (p = 0.005). In addition, oral hygiene habits were worse in adolescents that had industrial baked goods for a morning snack (p = 0.02) compared to those that brought a sandwich made at home. Adolescents that habitually consumed sugary drinks did not consider that visiting the dentist was important to their general health (p = 0.011).
We found a significant association between the number of brushings per day and screen time. Respondents that brushed only once a day watched media for 3 to 6 hours a day in the computer or television (p = 0.49), respondents that did not brush their teeth spent many hours a day gaming with the computer (p = 0.023), while respondents that did not have breakfast every day spent many hours gaming with a console (p = 0.025). We also found a significant association with not engaging in any form of physical activity (p = 0.00).
We also found statistically significant differences based on cell phone use in association with the consumption of fruit and the consumption of sweet baked goods. Adolescents that spent considerable time using their cell phones were not likely to consume fruit (p = 0.027) but a high proportion did consume industrial baked goods (p = 0.01). We found significant differences in the consumption of home-made sandwiches for morning snack and physical activity. Respondents that exercised more than 3 times a week usually had a sandwich for their morning snack (p = 0.002).
When it came to the association of oral hygiene habits and tattoos, we also found significant differences. Students that brushed their teeth 2 to 3 times daily liked tattoos (p = 0.00).
Lastly, as concerns academic performance, we found that adolescents that performed most poorly were significantly less interested and invested significantly less in their oral and dental care (p = 0.072).
DISCUSSION
Oral health is an integral part of general health and has a significant impact on quality of life. During adolescence, behaviours that are beneficial or deleterious to health are shaped, so this is the most appropriate phase of life in which to promote the responsibility to take care of oneself and maintain good habits. The WHO considers that oral health education interventions must be implemented in 2 broad fields of action: the community and schools. Schools of secondary education are a main setting where the lives of adolescents unfold. Instilling certain educational values in academic institutions facilitates rapport between teaching staff and students, giving rise to direct health education with long-lasting results and achieving a decrease in the overall prevalence of disease.13,14
This process is approached generally in secondary schools but also more specifically through school-based health education interventions, although it is also understood that this endeavour starts from the first days of life in the household and that the school further these efforts with additional guidance.15
To start, we found a statistically significant association between nationality and the frequency of visits to the dentist. Spanish teenagers had yearly or monthly dental appointments, while students of other nationalities did not visit the dentist each year, despite the higher proportion of participants in this subset that reported episodes of tooth pain. Students from some countries outside of Europe did not seem to have an established cultural health education tradition that prioritised oral health. Economic or social factors may lead many families of non-Spanish origin to delay visits to the dentist and may hinder their access to preventive and conservative dental care.16
As for the section of the questionnaire devoted to dietary habits, we found direct associations with nutritional factors. In the items devoted to a balanced diet, we focused on the presence of correct habits, such as the frequency of breakfast, given its importance in nutrition, the daily consumption of fruit or the moderate intake of cariogenic foods such as pastries and sugary drinks. Adolescence is a phase characterised by nutritional risk. In our survey, we found a statistically significant association between not brushing teeth and skipping breakfast, excessive consumption of baked goods for a morning snack or frequent consumption of sugary drinks. Studies worldwide have reported varied findings on the association between the energy intake and nutritional imbalance, demonstrating an increased risk of developing caries, overweight and obesity.12,17,18
Processed foods and current lifestyles favour an intake of fats and carbohydrates much higher than recommended. Sedentary habits and substantial screen times are associated with the habit of inadequate brushing, which, when combined with an imbalanced diet, will have an impact on oral health in the form of dental and periodontal disease in the life of the adolescent.19
We ought to highlight that periodontal health is associated with dietary habits and that obesity is a risk factor for increased severity of periodontal disease in adulthood. Although this subject has been broached and investigated in the literature, few studies have explored it in specific age groups, and the current evidence still lacks rigorous scientific data to explain the increased incidence of periodontal disease in overweight and obese children.9,12,20
In this context, parents exert considerable influence on the dietary habits of children and adolescents, as they are responsible for deciding the quantity and quality of the foods given in these stages. Besides the parents, teachers in secondary schools play a significant role in the promotion and development of healthy habits through health promotion and education measures.21
When it came to physical activity, our study found a statistically significant association between a lower level of activity per week and poorer oral care habits. A more sedentary lifestyle is associated with a higher sugar intake, and a lack of motivation on the part of the adolescent in establishing a healthy routine and lack of engagement in physical activity usually lead to the main activity being watching television or playing videogames, which in turn are usually associated with an increased consumption of foods that are bad for teeth. The ultimate result is, for example, the development of caries.3,4
Our findings were consistent with those of studies in the literature: adolescents with healthier lifestyles habits brushed and flossed their teeth more frequently compared to peers with more sedentary lifestyles.22
As for the excessive use of technology, adolescents are exposed to large amounts of information through electronic devices, which children are starting to use at increasingly young ages and for an increasing number of hours, when excessive use is defined as more than 2 hours a day of screen time.8
In our study, we found that the association of poor oral hygiene habits with an excessive screen time was also associated with a higher probability of sedentary lifestyle habits, increased consumption of sugary drinks and industrial baked goods and the development of dental caries.
We also found a significant association between screen time and diet. Adolescents that did not have breakfast every day spent many hours gaming with a console (p = 0.025). There were also significant differences in cell phone use in association with the consumption of fruit and of sweet baked goods. Adolescents that used their cell phones frequently were less likely to consume fruit (p = 0.027) and were more likely to consume industrial baked goods frequently (p = 0.01).
When it comes to technology addiction, an article published in BMC Pediatrics in 2012 reported a proportion of gaming addicts of 10.6%, of mobile phone addicts of 9.04%, moderate internet addicts of 21.88% and severe internet addicts of 0.76%. The incidence of addiction grows with time. The age at which technological devices are introduced is increasingly young, with 78.5% to 100% of new users aged less than 12 years, which calls for interventions for prevention of addition and promotion of responsible use of technology. The authors also corroborated that screen time is associated with other risk behaviours, such as physical inactivity, a high consumption of cariogenic foods and soft drinks or smoking, which, as we hypothesised in our study, have a negative impact in the health of adolescents.8
In our survey, 71% of respondents asserted that they used their cell phones every day all day long, and 4.6% reported spending more than 6 hours gaming, using the computer or watching television. We found a significant association between screen time and the frequency of daily brushing in our study, as adolescents that brushed only once a day watched video contents for 3 to 6 hours a day in the computer or the television (p = 0.49), and adolescents that did not brush teeth spent many hours playing computer games (p = 0.023).
One possible explanation of the association between excessive screen time and the low frequency of brushing would be that less time is available for brushing due to the many hours spent gaming or watching video contents.
The association between oral health and academic performance was strongly positive in terms of the level of oral care and the performance of the student. The direct association may be explained by a greater sense of academic responsibility being linked to greater awareness of health in general and of oral health in particular.
Certain aesthetic trends, such as oral piercings and tattoos, are increasingly common among adolescents that perceive them as a means of self-expression and to stand out from the crowd. However, many are not aware of their potential complications and the maintenance they require. Although our working hypothesis was that adolescents with tattoos would exhibit poorer oral hygiene, the statistical analysis showed that those that wished to get a tattoo in the future brushed more often, which may be an indication that they care more about their appearance and therefore about their teeth.
Similarly, although the results were not statistically significant, we asked about oral piercings. Since these are frequent at present, they should be added to the contents of health education programmes and dental checkups, as they carry a high risk of complications and require special care that adolescents should be made aware of to be able to prevent and control complications, such as the need to avoid constant contact of the piercing with the teeth or to clean the piercing site and surrounding area correctly.10,23
Contrary to other studies that found a proportion of adolescents with piercings of 21.85% to 50%, none of the participants in our study had piercings, although 15.4% planned to get one. It is possible that the fact that they were minors played a role on the absence of piercings.18,24
To conclude, unfortunately, we were unable to find an association between any oral parafunctional habit or temporomandibular disease and any dental variables of interest. Ignorance on the part of the adolescents about such subjects or their early age may pose a challenge in establishing an association between these variables.
Oral parafunctional habits in adolescents may affect the temporomandibular joint, as this is the most dynamic growth phase in humans. Our questionnaire addressed the habits of biting objects, lips or nails, which 13% to 23% of respondents reported doing, proportions that were lower than those found in a study conducted in Brazil (46%-60%).25
One of the main limitations of this study was that it was based on a self-report survey, which carries a risk of bias due to untruthful or inaccurate responses. However, since the questionnaire was completed anonymously, this risk was minimised, facilitating provision of honest answers. Another limitation is that due to its cross-sectional design, we were not able to establish causality in the observed associations, or to determine which habits were reinforced as years went by. Yet another limitation is the sample, which may not have been sufficiently large and representative, so that further studies of larger scale are required.
Due to the high prevalence of oral problems in association with lifestyle habits, we believe it important to continue studying this association. Furthermore, other aspects in the questionnaire should be explored, such as weight and height, in order to calculate the body mass index for each student and assess the potential association of obesity with the different variables under consideration.
All these correlations between unhealthy lifestyle habits and oral health could change by making adolescents aware of the strong association that exists and the significant impact that oral health has on quality of life. One possible way to do this would be to deliver talks in schools, as 36% of respondents reported never having received one.
CONCLUSION
The high prevalence of oral and dental disease in the population of schoolchildren suggests that school-based health education interventions are important. There is evidence of a significant association between the health of adolescents and specific oral and dental hygiene habits. Health education during the transition to adult life is essential for adolescents to solidly establish adequate dietary and oral health habits.
We must raise awareness of the need to promote healthy habits contributing to the good maintenance of the oral cavity in our youth. We must focus on developing preventive strategies so that adolescents, who are a subset of the population that is susceptible to information, establish and maintain good habits through this stage of development while reducing the impact of unhealthy habits on health.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS
ESO: Compulsory Secondary Education · WHO: World Health Organization.
REFERENCES
- World Health Organization. The Global Strategy for Women’s, Children’s and Adolescents’ Health, 2016-2030. Survive, thrive, transform. Geneva: WHO, 2015.
- Campo-Ternera L, Herazo-Beltrán Y, García-Puello F, Suárez-Villa M, Méndez O, Vásquez-De la Hoz F. Estilos de vida saludables de niños, niñas y adolescentes de Barranquilla. Salud Uninorte. 2017;33:419-28.
- Moreno LA, Gracia-Marco L. Prevención de la obesidad desde la actividad física: del discurso teórico a la práctica. An Pediatr (Barc). 2012;77:136.e1-136.e6.
- Martin A, Saunders DH, Shenkin SD, Sproule J. Lifestyle intervention for improving school achievement in overweight or obese children and adolescents. Cochrane Database Syst Rev. 2014;(3):CD009728.
- Palenzuela SM, Pérez A, Pérula de Torres LA, Fernández JA, Maldonado J. La alimentación en el adolescente. An Sis San Navarra. 2013;37:47-58.
- Gatou T, Mamai-Homata E, Koletsi-Kounari H, Polychronopoulou A. The shortterm effects of television advertisements of cariogenic foods on children’s dietary choices. Int Dent J. 2016;66:287-94.
- Busch V, Manders LA, de Leeuw J. Screen time associated with health behaviors and outcomes in adolescents. Am J Health Behav. 2013;37:819-30.
- Ramírez E, Sanz E, García E, Romero V, Codina A, Valls N, et al. ¿Adolescentes conect@dos o atrap@dos? Estudio sobre adicción a las TICs en población adolescente y su repercusión en salud mental. In: Congreso Nacional de la Sociedad Española de Pediatría Extrahospitalaria y Atención Primaria. Salamanca; 2016. p. 217-24.
- Ferrante D, Linetzky B, Ponce M, Goldberg L, Konfino J, Laspiur S. Prevalencia de sobrepeso, obesidad, actividad física y tabaquismo en adolescentes argentinos: Encuestas Mundiales de Salud Escolar y de Tabaco en Jóvenes, 2007-2012. Arch Argent Pediatr. 2014;112:496-503.
- Nieto E, Cerezo M, Cifuentes O. Frecuencia de uso de adornos corporales y motivaciones de los estudiantes para usar piercing oral. Rev Univ Salud. 2012;14:147-60.
- Silk H, Kwok A. Addressing adolescent oral health: a review. Pediatr Rev. 2017;38:61-8.
- Jordan LMR, Malta DC, Freire MCM. Clustering patterns of oral and general health-risk behaviours in Brazilian adolescents: findings from a national survey. Community Dent Oral Epidemiol. 2017;00:19.
- World Health Organization. The etiology and prevention of dental caries. Technical report series, no. 494. Geneva: WHO; 1972.
- Calle Purón ME, Gil Miguel A, Lasheras Lozano ML, Rey Calero J, Domínguez Rojas V. Estudio epidemiológico y evolución de la caries dental en colegios de Madrid. Av Odontoestomatol. 1990;6 611-4.
- World Health Organization. Global strategy for health for all by the year 2000. Geneva: WHO; 1981.
- Paredes Gallardo V, Paredes Cencillo C, Mir Plana B. Prevalencia de la caries dental en el niño inmigrante: estudio comparativo con el niño autóctono. An Pediatr (Barc). 2006;65:337-41.
- Roales-Nieto J, Ríos F, Moreno E. Concepto, creencias y comportamientos de salud en preadolescentes. Análisis y Modificación de Conducta. 2001;27:875-904.
- Tsuchiya M, Momma H, Sekiguchi T, Kuroki K, Kanazawa K, Watanabe M, et al. Excessive game playing is associated with poor toothbrushing behavior among athletic children: a cross-sectional study in Miyagi, Japan. Tohoku J Exp Med. 2017;241:131-8.
- García-Continente X, Allué N, Pérez-Giménez A, Ariza C, Sánchez-Martínez F, López MJ, et al. Hábitos alimentarios, conductas sedentarias y sobrepeso y obesidad en adolescentes de Barcelona. An Pediatr (Barc). 2015;83:3-10.
- Luca Sfasciotti G, Marini R, Pacifici A, Ierardo G, Pacifici L, Polimeni A. Childhood overweight-obesity and periodontal diseases: is there a real correlation? Ann Stomatol (Roma). 2016;7:65-72.
- Macías A, Gordillo S, Camacho R. Hábitos alimentarios de niños en edad escolar y el papel de la educación para la salud. Rev Chil Nutr. 2012;39:40-3.
- Alfaro M, Vázquez ME, Fierro A, Rodríguez L, Muñoz MF, Herrero B. Hábitos de alimentación y ejercicio físico en los adolescentes. Rev Pediatr Aten Primaria. 2016;18:221-9.
- Vozza I, Fusco F, Corridore D, Ottolenghi L. Awareness of complications and maintenance mode of oral piercing in a group of adolescents and young Italian adults with intraoral piercing. Med Oral Patol Oral Cir Bucal. 2015;20:e413-e418.
- Hooley M, Skouteris H, Boganin C, Satur J, Kilpatrick N. Body mass index and dental caries in children and adolescents: a systematic review of literature published 2004 to 2011. Syst Rev. 2012;1:57.
- Fonseca E, Teixeira C, Oliveira A. Malocclusion and deleterious oral habits among adolescents in a developing area in northeastern Brazil. Braz Res Oral. 2013;27:63-9.