
Vol. 22 - Num. 86
Original Papers
Impact of the rapid diagnostic test of Streptococcus pyogenes on the consumption of antibiotics in Primary Care
M.ª Rosario Bachiller Luquea, M.ª Nazaret Sánchez Sierrab, Ana M.ª Ruiz San Pedroc, M.ª Ana Prado Prietoc, Tomás Maté Enríquezc, Laura Melero Guijarrod, José M.ª Eiros Bouzae
aPediatra. CS Pilarica Circular. Valladolid. España.
bCS Pilarica Circular . Valladolid. España.
cGerencia de Atención Primaria de Valladolid Este. Valladolid. España.
dMIR-Medicina Familiar y Comunitaria. CS Pintor Oliva. Palencia. España.
eGerencia de Atención Primaria Valladolid Oeste. Valladolid. España.
Correspondence: MN Sánchez. E-mail: nazaret91.ns@gmail.com
Reference of this article: Bachiller Luque MR, Sánchez Sierra MN, Ruiz San Pedro AM, Prado Prieto MA, Maté Enríquez T, Melero Guijarro L, et al. Impact of the rapid diagnostic test of Streptococcus pyogenes on the consumption of antibiotics in Primary Care. Rev Pediatr Aten Primaria. 2020;22:153-9.
Published in Internet: 25-05-2020 - Visits: 21555
Abstract
Objective: the aim of the study was to analyse the use of the rapid Streptococcus antigen detection test in primary care paediatrics, its impact on antibiotic prescription and the associated decrease in antibiotic treatment costs.
Material and methods: we conducted a cross-sectional descriptive study in children aged less than 15 years managed in 24 primary care centres between April 2017 and February 2018. We developed a protocol for the use of the rapid strep test (RST). We included patients with a Centor score equal to or greater than 2 points. We collected data on the number of daily defined doses (DDDs) and amount antibiotics prescribed in the study period from the prescription billing system and compared it with the costs corresponding to the previous 12-month period.
Results: 819 TDRS were performed. The results were positive in 250 (30.5%), negative in 557 (68%) and inconclusive in 12 (1.5%). Antibiotics were prescribed to 33% of the patients (all patients with a positive test, 18 with a negative test and 3 with an inconclusive test). Antibiotherapy was not prescribed to 539 of the patients with a negative result (97%). The total number of prescribed DDDs decreased by 21 960 (12%), of which 19 023 (86.6%) corresponded to the most frequently prescribed antibiotics (penicillins, amoxicillin, amoxicillin-clavulanic acid and azithromycin). We found a reduction of €11 320 in antibiotherapy costs (12.5%), while the total cost of rapid testing was € 991, corresponding to total savings of €10 329.
Conclusions: the introduction of the RST in primary care paediatrics has achieved a reduction in the frequency of antibiotherapy. Its use has proven effective in optimising antibiotic use, reducing antibiotic prescription and therefore preventing associated adverse events and reducing unnecessary pharmacotherapy costs.
Keywords
● Streptococcus pyogenes ● Cost analysis ● Diagnostic test kit ● Drug utilization evaluation ● Primary care ● TonsillitisINTRODUCTION
Acute pharyngotonsillitis (AP) is one of the most common diseases of childhood and generates up to 30% of paediatric primary care (PC) visits.1,2 It is more prevalent in countries with temperate climates, with incidence peaks in winter and spring in the northern hemisphere. It is an inflammatory disease of the mucosae of the pharynx or pharyngeal tonsils, manifesting with redness, swelling, exudate, ulcers or vesicles.
The aetiology is usually infectious, most frequently viral (40%-80% of cases), with a self-limiting course and favourable outcomes of disease.3
Group A beta-haemolytic streptococcus (GABHS), or Streptococcus pyogenes, is the most frequent bacterial causative agent, and is responsible for approximately 15% to 30% of total cases.4 It is usually detected in patients aged more than 3 years and is rare in younger children (6%-10% of cases of GABHS). However, some authors have reported a prevalence of approximately 20% in infants aged less than 1 year and 26% in children aged 2 to 3 years5,6 (possibly including asymptomatic carriers, which may account for up to 12% of the total). Thus, despite its low prevalence, some authors recommend performance of diagnostic tests and contemplating the need for treatment in children aged less than 3 years with close contact with cases of AP due to GABHS in the household or at school to decrease the spread of the bacterium and transmission of the disease.7
More than 50% of patients with a clinical diagnosis of AP receive empirical antibiotherapy.4-8 Antibiotic treatment of pharyngotonsillitis caused by GABHS has been generally recommended to reduce the duration of symptoms and to prevent transmission as well as suppurative and nonsuppurative complications of the disease.8
However, the clinical presentation of pharyngotonsillitis does not suffice to discriminate between a viral and a bacterial aetiology.9 Therefore, the purpose of performing diagnostic tests is to be able to make this differentiation. The introduction of rapid antigen detection tests (RADTs) for detection of streptococcus, known as the rapid strep test (RST) and easy to perform in the primary care setting, allows early diagnosis and initiation of treatment with a high specificity, and therefore could help reduce unnecessary antibiotic use.
The aim of our study was to analyse the use of the RST in PC paediatric clinics for diagnosis of streptococcal pharyngitis, the impact of this test in antibiotic prescription and the associated reduction in the costs associated with the use of antibiotherapy in these patients.
MATERIAL AND METHODS
We conducted a cross-sectional descriptive study in 34 PC clinics in 24 primary care centres in the Eastern Health District (Área de Salud Este) of Valladolid. The study period ranged from April 2017 to February 2018.
We included all cases of patients aged 14 years or younger that sought care in our clinic for AP of probable streptococcal aetiology. To determine this, we used the Centor score modified by McIsaac (Table 1),10,11 including all cases with a score of 2 or greater. The exclusion criteria were: Centor score of less than 2, that is, patients with a low probability of having streptococcal pharyngotonsillitis, and additional visits related to the same episode of disease.
| Table 1. Modified/McIsaac Centor Score | |
|---|---|
| Criteria | Score |
| 1. Fever >38° | 1 |
| 2. Tonsillar swelling or exudate | 1 |
| 3. Tender/swollen lateral anterior cervical nodes | 1 |
| 4. Absence of cough | 1 |
5. Age:
|
1 0 |
Risk of streptococcal infection (%)
|
|

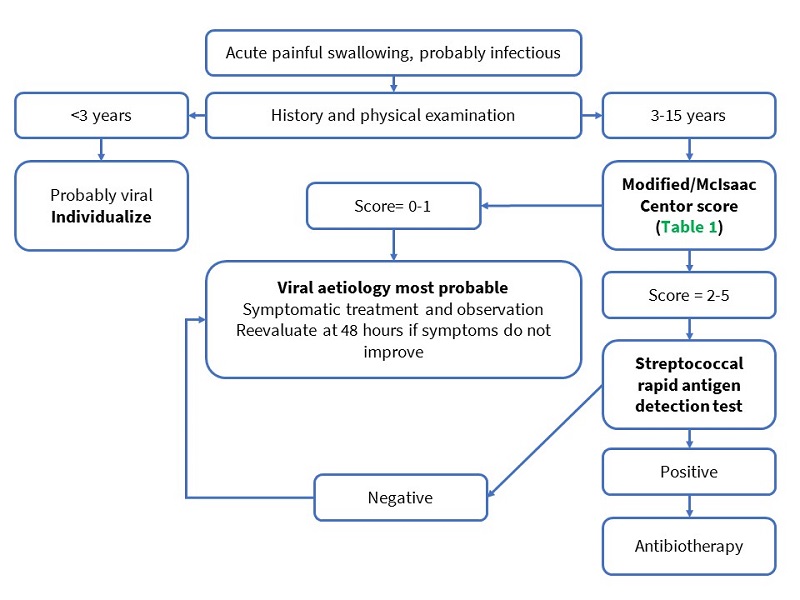
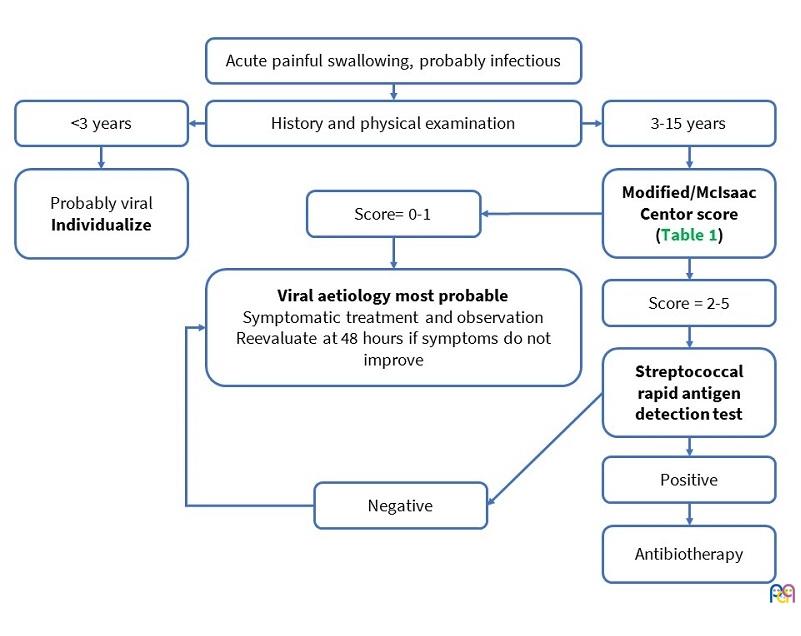
We developed a management protocol (Figure 1) based on the age of the patient and the Modified/McIsaac Centor score to select patients that would benefit from performance of a RST and to determine the approach to treatment based on its results.
| Figure 1. Pharyngotonsillitis management protocol |
|---|
 |
In the weeks before starting the study, we held training sessions open to all PC paediatricians and nurses and specific trainings in clinics in which we distributed printed documents featuring the indications for antibiotic prescription and directions for correct performance of RSTs.
The study was approved by the Ethics Committee of the Eastern Valladolid health district. After informing families about the study and obtaining informed consent, paediatricians performed the clinical evaluation and had a nurse collect a throat swab specimen. The specimen was collected by rubbing a cotton swab on the posterior wall of the pharynx and both pharyngeal tonsils with emphasis on the most reddened areas or areas with exudate, avoiding contact with the tongue, uvula or any other part of the mouth to avoid contamination of the sample with the saprophytic flora of the respiratory tract. The RST was subsequently performed by chromatographic immunoassay (Strep A MonlabTest). The result was available 15 minutes later, and subsequent treatment was administered in adherence with the protocol (Figure 1).
We collected data for the following variables: sex, age in years, care setting, signs and symptoms of AP, modified/McIsaac Centor score, use of RST and results, antibiotic prescription and prescribed antibiotic.
We collected data from the CONCYLIA prescription billing system of the Public Health System of Castilla y León (SACYL), documenting the daily defined dose (DDD) and the expenditure in antibiotic prescriptions in the paediatrics sector during the study period, comparing the expenditure with that of the 12 months prior (April 2016-March 2017).
We performed a descriptive analysis of the study variables, expressing quantitative data as mean and standard deviation and qualitative data as absolute frequency and percentage distributions.
RESULTS
We recruited a total of 819 patients with manifestations compatible with acute pharyngotonsillitis and a modified/McIsaac Centor score of 2 or higher. The mean age was 7.5 years (1-14). We found no difference in the presenting signs and symptoms based on age or sex.
The most frequent presenting complaints were fever, painful swallowing and pharyngeal redness or exudate. We found a scarlatiniform rash in 8% of patients. Less frequent manifestations included abdominal pain (1.5%), headache (1.2%) and vomiting (0.6%).
A RST was performed in all patients. The results were positive in 250 (30.5%), negative in 557 (68%) and inconclusive in 12 (1.5%). Four percent of the tests performed corresponded to patients younger than 3 years. In this subset of younger patients, 17.5% had a positive result. The most frequent indication for the RST in this group of patients was the presence of scarlatiniform rash, found in more than half (53%), followed by exudate in the pharynx or tonsils with fever in absence of cough (32%) and fever of unknown origin (15%).
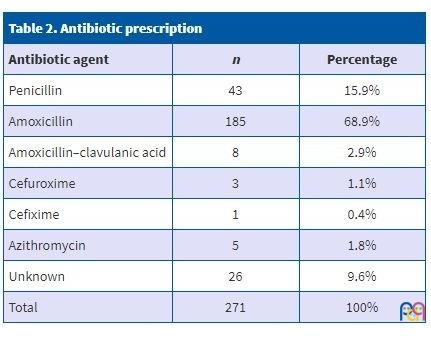
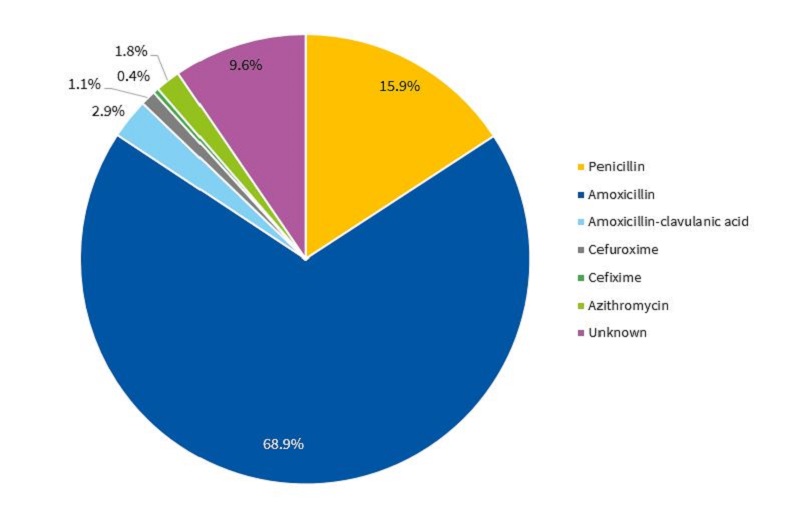
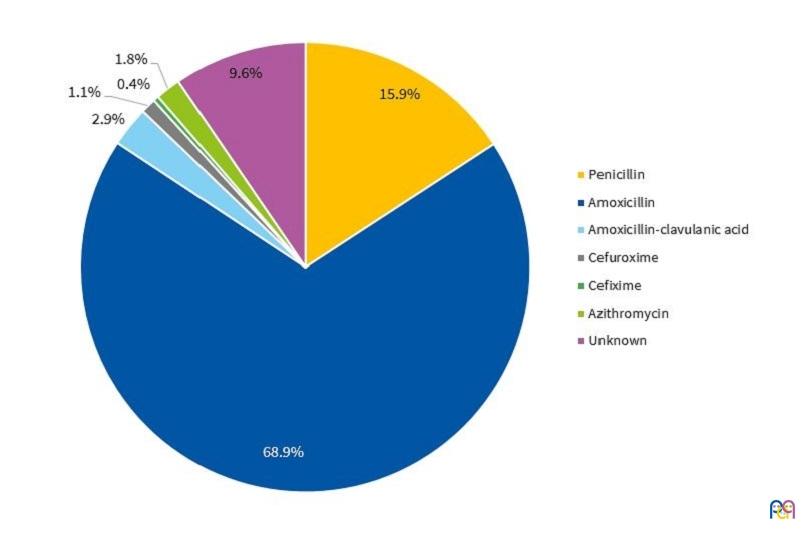
Antibiotherapy was prescribed to 271 patients (33.1%), including all with a positive result of the RST, 18 with a negative result (3.2%) and 3 with inconclusive results (25%). Antibiotherapy was not initiated in 539 patients with negative results (96.8%). Table 2 and Figure 2 present the antibiotic agents used in the sample.
| Table 2. Antibiotic prescription | ||
|---|---|---|
| Antibiotic agent | n | Percentage |
| Penicillin | 43 | 15.9% |
| Amoxicillin | 185 | 68.9% |
| Amoxicillin–clavulanic acid | 8 | 2.9% |
| Cefuroxime | 3 | 1.1% |
| Cefixime | 1 | 0.4% |
| Azithromycin | 5 | 1.8% |
| Unknown | 26 | 9.6% |
| Total | 271 | 100% |
| Figure 2. Chart of prescribed antibiotic agents |
|---|
 |
All patients had achieved full resolution of symptoms after completing the course of antibiotherapy, and we did not observe any complications of this treatment.
After analysing the prescription database, we found that the number of DDDs in the study period decreased by 21 960 (12%) compared to the same period a year before, of which 19 023 (86.6%) corresponded to the antibiotic agents used most frequently in PC (penicillins, amoxicillin, amoxicillin-clavulanic acid and azithromycin).
The reduction in antibiotherapy costs was €11 320 (12.5%) while the cost of performing RSTs was €991, which resulted in savings of €10 329 in health care costs (11.4%) in our health district.
DISCUSSION
Rapid strep tests are easy to do, yield results in a few minutes in the patient care setting, and allow early and individualised initiation of treatment. This reduces disease transmission and the days of missed school and, above all, optimises antibiotic use. These tests offer a specificity of 95% or higher and a sensitivity that ranges from 70% to 90%12-18 for diagnosis of AP caused by GABHS. The main drawbacks of this test is that it cannot detect other serotypes and that a negative result does not fully rule out infection by GABHS. In cases in which the RST is negative but there is a high suspicion of streptococcal AP, a throat swab culture could be useful,19,20 as it has a specificity of nearly 99% and, if the sample has been collected correctly, the sensitivity can be as high as 90% to 95%.12,21 Although the turnaround time for culture is longer (24-48 hours), this method has the advantage that it can identify different bacteria and serotypes and allows assessment of antimicrobial susceptibility and resistance. Neither test can discriminate between AP caused by GABHS or GABHS carrier status. Nevertheless, given the low prevalence of asymptomatic carriage (ranging from 6% to 12%), antibiotherapy is not recommended routinely in patients with negative results,3 but only in select cases.11
Several scales have been proposed to facilitate diagnosis of AP caused by GABHS and identify patients in who some form of testing is indicated. The one used most frequently is the modified/McIsaac Centor score. This score is based on the presence or absence of certain clinical features, while taking age into account: a body temperature greater than 38°C, tonsillar swelling or exudate, tender swollen anterolateral cervical nodes and absence of cough. It has a high negative predictive value,22 so that the probability of a positive result in microbiological diagnostic tests is of 3% or less in patients that meet none of the clinical criteria and of 38% to 63% in patients that meet 4 to 5 criteria.19 Some form of diagnostic testing (RST or culture) is indicated in cases with a score of 2 or greater, unless the clinical presentation were compatible with viral infection, which would invalidate the indication.23
The introduction of the RST in the primary care paediatrics setting has allowed to greatly reduce the prescription of unnecessary antibiotic treatments. As we specified above, the number of total DDDs decreased by 21 960 (12%), of which 19 023 (86.6%) corresponded to the antibiotic agents prescribed most frequently in PC (penicillins, amoxicillin, amoxicillin-clavulanic acid and azithromycin). Our findings were consistent with the previous literature. In 2008, Maltezou et al.24 reported that the use of RSTs achieved a reduction in antibiotic prescription of 61% compared to empirical management of patients based on clinical features. In 2016, Kose et al.25 found that the exclusive use of clinical criteria for diagnosis of streptococcal pharyngotonsillitis led to antibiotic prescription in a high proportion of patients (79.8%), which dropped to 42.6% after performance of rapid testing.
Thus, the use of RSTs in this care setting has proven useful in terms of rational antibiotic use, reducing antibiotic prescription and contributing to preventing the development of drug resistance as well as adverse events.
Another aspect we ought to highlight is that the use of the RST in PC reduces unnecessary drug costs.
Phof et al.26 calculated that the average medical care costs per GABHS case was of $118 (58% of the total cost). Antibiotic treatment amounted to 20% of these costs ($23.60 per case). Kose et al.25 determined that the average cost of empirical antibiotherapy was $7.20 per patient, which decreased by 76.4% ($5.50) with individualisation of treatment following performance of rapid testing. Considering the cost of the RST (of $1.14 per patient), the cost of treatment per patient decreased by 60.6%.
In our study, the reduction in drug prescription costs was of 11 320 € (12.5%), while the costs of rapid testing amounted to €991, with overall savings of €10 329.
In light of all of the above, the use of rapid streptococcal antigen detection tests seems to be an efficient and advisable intervention in primary care paediatrics clinics.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
FUNDING
Department of Pharmacy of the Primary Care Administration of Eastern Valladolid.
ABBREVIATIONS
AP: acute pharyngotonsillitis · DDD: daily defined dose · GABHS: group A beta-haemolytic streptococcus · PC: Primary Care · RST: rapid antigen detection test for streptococcus.
REFERENCES
- García Vera C. Faringoamigdalitis estreptocócica en la infancia. APPap Monogr. 2016;2:26-33.
- Kronman MP, Zhou C, Mangione-Smith R. Bacterial prevalence and antimicrobial prescribing trends for acute respiratory tract infections. Pediatrics. 2014;134:e956.
- Oliver J, Malliya Wadu E, Pierse N, Moreland NJ, Williamson DA, Baker MG. Group A Streptococcus pharyngitis and pharyngeal carriage: a meta-analysis. PLoS Negl Trop Dis. 2018;19;12:e0006335.
- Regueras G, Santos PM, Villa L, Pérez A, Arbesú E, Barreiro L, et al. Utilidad de una técnica antigénica rápida en el diagnóstico de faringoamigdalitis por Streptococcus pyogenes. An Pediatr (Barc). 2012;77:193-9.
- Tellechea AL, Salvo MG, Méndez JH, Cavagnaria B. Frecuencia del estreptococo betahemolítico del grupo A en las fauces de niños sintomáticos menores de 15 años según el grupo etario. Arch Argent Pediatr. 2012;110:516-9.
- Woods WA, Carter CT, Schlager TA. Detection of group A streptococci in children under 3 years of age with pharyngitis. Pediatr Emerg Care. 1999;15:338-40.
- Martí Fernández J, Gascón Casaredi I, Sandiumenge Durán M. Faringitis estreptocócica en niños menores de tres años. Algunas consideraciones. Rev Pediatr Aten Primaria. 2015;17:e125-8.
- Frost HM, Fritsche TR, Hall MC. Beta-hemolytic nongroup A streptococcal pharyngitis in children. J Pediatr. 2019;206:268-73.
- American Academy of Pediatrics. Group A streptococcal infections. In: Kimberlin DW, Brady MT, Jackson MA, Long SS (eds.). Red Book: 2018 Report of the Committee on Infectious Diseases. 31st edition. Itasca: American Academy of Pediatrics; 2018. p. 748.
- Roggen I, van Berlaer G, Gordts F, Pierard D, Hubloue I. Centor criteria in children in a paediatric emergency department: for what it is worth. BMJ Open. 2013;3:e002712.
- Piñeiro R, Hijano F, Álvez F, Fernández A, Silva JC, Pérez C, et al. Documento de consenso sobre el diagnóstico y tratamiento de la faringoamigdalitis aguda. An Pediatr (Barc). 2011;75:342.e1-13.
- Shulman ST, Bisno AL, Clegg HW, Gerber MA, Kaplan El, Lee G, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55:1279-82.
- Gieseker KE, Mackenzie T, Roe MH, Todd JK. Comparison of two rapid Streptococcus pyogenes diagnostic tests with a rigorous culture standard. Pediatr Infect Dis J. 2002;21:922-7.
- Gerber MA, Shulman ST. Rapid diagnosis of pharyngitis caused by group A streptococci. Clin Microbiol Rev. 2004;17:571-80.
- Tanz RR, Gerber MA, Kabat W, Rippe J, Seshadri R, Shulman ST. Performance of a rapid antigen-detection test and throat culture in community pediatric offices: implications for management of pharyngitis. Pediatrics. 2009;123:437-44.
- Lean WL, Arnup S, Danchin M, Steer AC. Rapid diagnostic tests for group A streptococcal pharyngitis: a meta-analysis. Pediatrics. 2014;134:771-81.
- Stewart EH, Davis B, Clemans-Taylor BL, Littenberg B, Estrada CA, Centor RM. Rapid antigen group A streptococcus test to diagnose pharyngitis: a systematic review and meta-analysis. PLoS One. 2014;9:e111727.
- Cohen JF, Bertille N, Cohen R, Chalumeau M. Rapid antigen detection test for group A streptococcus in children with pharyngitis. Cochrane Database Syst Rev. 2016;7:CD010502.
- McIsaac WJ, Kellner JD, Aufricht P, Vanjaka A, Low DE. Empirical validation of guidelines for the management of pharyngitis in children and adults. JAMA. 2004;291:1587-95.
- Dingle TC, Abbott AN, Fang FC. Reflexive culture in adolescents and adults with group A streptococcal pharyngitis. Clin Infect Dis. 2014;59:643-50.
- Gerber MA. Comparison of throat cultures and rapid strep tests for diagnosis of streptococcal pharyngitis. Pediatr Infect Dis J. 1989;8:820-4.
- Freer J, Ally T, Brugha R. Impact of Centor scores on determining antibiotic prescribing in children. Int J Health Care Qual Assur. 2017;30:319-26.
- Shapiro DJ, Lindgren CE, Neuman MI, Fine AM. Viral features and testing for streptococcal pharyngitis. Pediatrics. 2017;139:e20163403.
- Maltezou HC, Tsagris V, Antoniadou A, Galani L, Douros C, Katsarolis I, et al. Evaluation of a rapid antigen detection test in the diagnosis of streptococcal pharyngitis in children and its impact on antibiotic prescription. J Antimicrob Chemother. 2008;62:1407-12.
- Kose E, Sirin Kose S, Akca D, Yildiz K, Elmas C, Baris M, et al. The effect of rapid antigen detection test on antibiotic prescription decision of clinicians and reducing antibiotic costs in children with acute pharyngitis. J Trop Pediatr. 2016;62:308-15.
- Pfoh E, Wessels MR, Goldmann D, Lee GM. Burden and economic cost of group A streptococcal pharyngitis. Pediatrics. 2008;121:229-34.