

Analysis of tetanus vaccination coverage in adolescents: evolution and current state in Extremadura
aFarmacéutica de Equipo Atención Primaria. CS de Montijo. Badajoz. España.
Correspondence: L Serrano. E-mail: laura.serrano@salud-juntaex.es
Reference of this article: Serrano Peláez L. Analysis of tetanus vaccination coverage in adolescents: evolution and current state in Extremadura. Rev Pediatr Aten Primaria. 2019;21:e193-e200.
Published in Internet: 21-10-2019 - Visits: 17122
Abstract
Introduction: tetanus is a severe acute disease that is difficult to treat, and therefore its prevention is essential. The administration of 5 doses of tetanus vaccine suffices to confer long-term protection. In recent years, there has been evidence of a decrease in vaccination coverage, which entails that immunization in the population is insufficient. The aim of this study was to analyse the vaccination coverage rate for the booster dose of tetanus vaccine in adolescents residing in the town of Santa Amalia in the province of Badajoz (Spain) in the past 20 years (1996-2016).
Materials and methods: the study had a cross-sectional and observational design and involved the review of vaccination cards and records of the administered doses of vaccine, both manual and electronic (JARA Primary Care system). Between 1996 and 2001, vaccination was performed in the school setting and documented manually. Since 2002, vaccination was performed in the primary care centre, and documented manually between 2002 and 2007 and in the electronic health records system between 2008 and 2016.
Results: the analysis of vaccination coverage by groups found the poorest results in the period that vaccination was performed in the primary care centre and documented manually (35.6%), while the best results corresponded to the period when vaccination was made in the primary care centre and documented in the electronic health records (100%), followed by the period of vaccination in the school with manual documentation (83.0%).
Conclusions: the study found a high vaccination coverage for the booster dose of tetanus vaccine in adolescents aged 14 years residing in Santa Amalia, similar to the national average coverage, despite the low coverage rates documented in the rest of Extremadura.
Keywords
● Adolescent ● Tetanus ● Vaccination coverage ● VaccinesINTRODUCTION
Tetanus is a severe acute disease caused by the toxin of the bacillus Clostridium tetani, which proliferates under anaerobic conditions at wound sites. These wounds, which may or may not be noticed, provide the point of entry to the body, and puncture, scrape or burn wounds are particularly dangerous. Contaminated injections and some surgical techniques also may lead to tetanus. This disease is never transmitted through close contact between people, and it always occurs through a reservoir. The clinical picture of tetanus is characterised by painful muscle spasms and a very characteristic facial expression known as the “sardonic smile’. This disease is difficult to treat, and therefore its prevention is essential. The latter can only be achieved by active immunisation (tetanus vaccine) or passive immunisation (tetanus immune globulin). Vaccination is the most effective preventive measure.1,2
Tetanus is an infectious disease with a low morbidity but a high mortality, and the main means available to reduce its incidence and ultimately eradicate it is an effective, safe and inexpensive vaccine.3 Vaccines save millions of lives each year and are among the most safe and effective public health interventions, providing benefits in terms of disease prevention and control but also social and economic ones. The recent development of the Global Vaccine Action Plan (GVAP) for 2011-2020, endorsed by the 194 Member States of the World Health Assembly, is a framework that recognises the importance of vaccines and reaffirms that expanding vaccination would advance global wellness.4 One of the main objectives of the World Health Organization (WHO) in developed countries is fighting tetanus by maintaining a high vaccination coverage, with the administration of sufficient booster doses to prevent tetanus in all age groups.2
The administration of booster doses achieves the maintenance of a high titre of protective antibodies, and it is believed that 5 doses of tetanus vaccine suffice to confer long-term protection. The vaccine used in Spain is a suspension of inactivated diphtheria and tetanus toxoids adsorbed in aluminium salts. After vaccination, nearly 100% of vaccinated individuals produce antibodies against vaccine antigens, but the conferred immunity declines over time. The number of doses of diphtheria and tetanus vaccine administered during childhood has a significant impact on the duration of the immunity acquired after ach booster dose given in adulthood.1
The first time that the immunization schedule in Spain included a booster dose of tetanus vaccine at age 14 years was 1975.2 At present, the Advisory Committee on Vaccines of the Asociación Española de Pediatría (Spanish Association of Paediatrics) (CAV-AEP) publishes the immunisation schedule that it considers optimal for children in Spain on a yearly basis, taking into account the available evidence on vaccines and the current official routine immunization schedules in the country. It continues to recommend the use of the tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine (Tdap) at age 12 to 14 years as a booster dose.5 At the same time, the Committee on the Vaccination Programme and Register, a scientific and technical organism of the Interterritorial Council of the Spanish National Health System, carries out evaluations and proposes changes that are later incorporated in the immunisation schedules of the different autonomous regions in Spain.6 After evaluating programmes for vaccination against tetanus in Spain and neighbouring countries and reviewing the scientific evidence on the protection conferred by different vaccination schemes, this organism has recommended administration of a booster dose of tetanus-diphtheria vaccine (Td) at age 14 years.7
Both Decree 14/2016, of 23 February, which amends Decree 161/2006, of September 6 and approves the full immunization schedule of the region of Extremadura, and Decree 149/2018, of September 4, which amends Decree 204/2016, of December 14, which approve the full vaccination schedule for Extremadura and was published in the Diario Oficial de Extremadura (Official Bulletin of Extremadura), recommend administration of a dose of Td at age 14 years. The Td vaccine has a reduced diphtheria antigen load and may be used starting at age 7 years, although it is meant for use in children aged 14 or more years and adults.8
The policy of routine universal vaccination and the high vaccination coverage rate achieved have succeeded in making tetanus an infrequent disease in Spain. There are no cases of neonatal tetanus and the few cases of tetanus occur in adults with incorrect or incomplete vaccination,6 with the same age distribution, number of cases and mortality found in other western countries.7 In Extremadura, the last notified case dated from 2005, until a case of tetanus was reported in June 2, 2017 in a man aged 68 years for who there is no documentation of any previous vaccination against tetanus.9
In Spain, childhood vaccination is not only accepted but widely demanded by the population, and therefore there is a high vaccination coverage rate.10 In adults, the frequency of complete vaccination is low, and it is important to remember that the titre of circulating antibodies decreases with time.3 In spite of this, in recent years there has been a decline in some vaccination coverage rates, which means that in some regions of Spain, there may be entire pockets of the population that are not immunised and therefore not protected. 10
A preliminary analysis of the vaccination coverage for the booster dose of tetanus-diphtheria in year 2016 showed a coverage of 82% for the population aged 14-16 years in Spain.11 By autonomous region, Catalonia had the highest coverage with a rate of 96.4%, while Extremadura only had a coverage rate of 52.7% in adolescents aged 14 years.12 In the Don Benito-Villanueva health district, the coverage is of 71.1% (data of the Public Health System of Extremadura, accessed August 18, 2017).
The rationale for this study was that we did not know of any previous studies of these characteristics in our region, as few studies provide global data allowing comparison with similar criteria. We also believed it would be useful for the purpose of knowing the actual vaccination rate, as we used data rather than estimates, as this can help improve the development of vaccination policies in the Public Health System of Extremadura.
The main objective of the study was to analyse the vaccination coverage for the booster dose of tetanus-diphtheria vaccine (Td) administered at age 14 years in the town of Santa Amalia (Don Benito-Villanueva Health District of Extremadura) to observe its evolution in the 1996-2016 period. A secondary objective was to determine whether coverage was lower in adolescents aged 14 years (from this point on referred to as “adolescents’) vaccinated in primary care centres compared to those vaccinated in the school.
MATERIALS AND METHODS
Study design: cross-sectional observational descriptive study of all doses of tetanus vaccine administered at age 14 years to residents of the town of Santa Amalia in the province of Badajoz (Spain) in the past 20 years (1996-2016).
Study universe: adolescents aged 14 years residing in the town of Santa Amalia.
Study sample: adolescents aged 14 years residing in the town of Santa Amalia vaccinated against tetanus in the local school or primary care centre.
Inclusion criteria: having been vaccinated in the school or primary care centre at age 14 years while being included in the population census of Santa Amalia.
Exclusion criteria: age other than 14 years at the time of vaccination (different birth year), age of vaccinated individual unknown (birth year unknown), residence in a town other than Santa Amalia (Valdehornillos, Torrefresneda, Conquista del Guadiana, Hernán Cortés, Yelbes or Medellín).
Sample size and sampling method: there were a total of 1142 adolescents aged 14 years residing in the town of Santa Amalia, of who 869 had been vaccinated, 551 at the primary care centre and 318 in school. The initial sample was larger, but the application of the exclusion criteria led to the elimination of 142 children vaccinated between 1996 and 2007. The adolescents included in the final analysis were those that had been vaccinated, as shown in Table 1, which presents the vaccination coverage rates.
| Table 1. Vaccination coverage rate for the Td vaccine at the CS Santa Amalia, 1996-2016 | ||||||||
|---|---|---|---|---|---|---|---|---|
| School | ||||||||
| 1996 | 1997 | 1998 | 1999 | 2000 | 2001 | |||
| 85.7 | 56.3 | 108.0 | 100.0 | 78.7 | 78.1 | |||
| Primary Care Centre, manual records | ||||||||
| 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | |||
| 52.8 | 55.1 | 12.7 | 10.0 | 4.0 | 88.0 | |||
| Primary Care Centre, electronic records | ||||||||
| 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 |
| 94.2 | 95.7 | 81.5 | 102.9 | 117.0 | 114.0 | 89.8 | 92.5 | 116.0 |
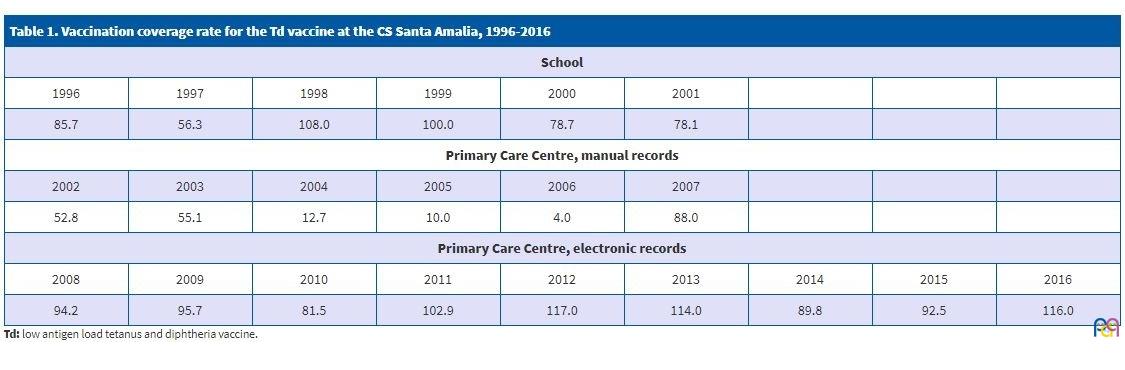
Data collection and calculation of coverage: a spreadsheet was created to group and count vaccinated adolescents from the population under study by year of administration of the vaccine as well as the size of the reference population. There were 3 distinct groups or periods: school setting (1996-2001), primary care centre and manual records (2002-2007) and primary care centre and electronic records (2008-2016). The vaccination coverage rate was calculated as a percentage with a single decimal value.
The data on the vaccinated adolescents included in the analysis was obtained from different sources. Data for years 1996-2007 was obtained from the review of individual vaccination cards and handwritten records of administrated doses of vaccines that were compiled on a monthly basis. For years 2008 through 2016, the data was obtained from the records of administered doses entered through applications for the JARA Primary Care system, which is the database used by the public health system of Extremadura.
The vaccination coverage rate was calculated with the following formula:
Vaccination coverage rate (%) = vaccinated individuals × 100 / reference population.
We obtained information for the reference population for years 1997 to 2016, both included, from census data of the Instituto Nacional de Estadística (National Institute of Statistics, INE). For year 1996, the population reference was obtained from CIVITAS, the population and health care resource management electronic system of Extremadura. The census of the INE started in 1997, and therefore census data were not available for year 1996.
RESULTS
Table 1 presents the vaccination coverage rate for the booster dose of Td in adolescents residing in Santa Amalia, divided in three periods that correspond to the different combinations of the setting where the vaccine was administered and the form of documentation: 1996-2001, 2002-2007 and 2008-2016.
A comparison of the overall data for each of these periods in Santa Amalia showed that the highest coverage was achieved in the group vaccinated at the primary care centre with electronic records (2008-2016) followed by the group vaccinated in the school, which also had high coverage rates (1996-2001). The lowest coverage, with a substantial difference compared to the other 2 periods, corresponded to the group vaccinated in the primary care centre with manual documentation of the administered vaccines in 2002-2007. The lowest coverage rates in the town of Santa Amalia (Don Benito-Villanueva health district) occurred in years 2004, 2005 and 2006. However, these 3 years are the years for which the highest percentages of adolescents were eliminated from the sample due to the application of exclusion criteria (40%, 44.4% and 75%, respectively).
DISCUSSION
This study analyses the tetanus vaccination coverage in the town of Santa Amalia in the province of Badajoz, Spain, in the past 20 years (1996-2016), during which adolescents have received the tetanus vaccine in different settings and vaccinations have been recorded using different formats. Between 1996 and 2001, the vaccine was given in the school and vaccination was documented manually. From 2002, the vaccine was given in the primary care centre, and vaccination was initially recorded by hand (2002-2007) and later electronically (2008-2016).
The strategy of vaccination against tetanus in the school (1996-2001) achieved high coverage rates, and it would be fair to say that this was a good approach, in which practically the entire target population was vaccinated en masse in a single day. In fact, the vaccination coverage in that period was nearly as good as it is now, using the electronic system JARA-Primary Care introduced in 2008. The transition period when vaccination moved from the school to the primary care centre, from 2002 to 2007, corresponded to the worst results. During this period, adolescents visited the primary care centre for the Well Child programme routine checkup, which included administration of the tetanus vaccine. The possible causes of this dramatic drop in vaccination may be due to patients forgetting the routine visit at this age and the manual documentation of vaccines with its inadequate archiving system, as we found months and years mixed up in the records, incomplete documentation (missing date of birth, address or town) and duplicate records, among other problems.
One of the limitations of the study was that in the school setting, vaccines were administered by school year, that is, vaccination was not performed taking into account the year the adolescent was born or the town where the adolescent resided. Thus, exclusion criteria were needed to make the different groups under study homogeneous. In 1997 there were 2 vaccination campaign periods: vaccination in February for the 1996/1997 academic year, and vaccination in October and November for the 1997/1998 academic year.
Other limitations to be taken into account for the appropriate interpretation of the results is that vaccination was delivered in 2 settings (school versus primary care centre) and issues related to documentation, which was performed either manually or electronically. In fact, the vaccination coverage rates of more than 100% found in some years may be due to the inclusion in the numerator of vaccinated children that were not part of the reference population or not registered as residents of Santa Amalia. Cases that did not meet the established inclusion criteria were categorised as unvaccinated individuals, when in fact most of these adolescents were probably correctly vaccinated.
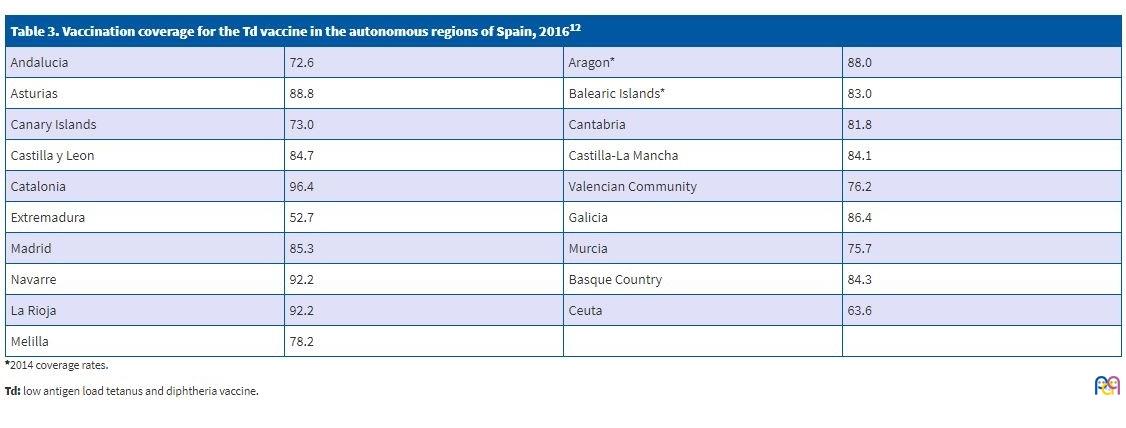
Comparing the vaccination data for Santa Amalia to the overall coverage in the Don Benito-Villanueva health district, we found that this town had a high coverage rate, which was much higher than the overall coverage rate for the entire district every year under study (Table 2). In this study, the definition of correct vaccination corresponded to administration of the vaccine in the year that the adolescent turned 14 years of age. In the last 9 years, the vaccination coverage in adolescents for the tetanus vaccine was similar or slightly higher in Santa Amalia compared to the average in Spain (Table 2). A comparison of data for 2016 (Table 2) shows that while the overall coverage in Spain was 82.0%, the coverage for the region of Extremadura was of 52.7%. This was far below the national average and the coverage rates in all other autonomous regions in Spain, which were similar to the national average (Table 3). Still, it is important to remember that an accurate comparison at different levels (nationwide, autonomous region and health district) requires that the databases used for the calculation of coverage rates correspond to the actual population and that these databases are comparable to each other.
| Table 2. Vaccination coverage rate for the Td vaccine in Extremadura and Spain, 2008-201611 | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Health district | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 |
| Badajoz | 105.7 | 100.0 | 26.0 | 20.8 | 59.1 | 36.8 | 39.5 | 34.3 | 41.9 |
| Merida | 78.7 | 100.0 | 31.6 | 25.9 | 74.8 | 44.7 | 48.8 | 43.0 | 53.7 |
| Don Benito-Villanueva | 65.3 | 60.3 | 20.6 | 16.9 | 65.8 | 39.4 | 44.7 | 65.4 | 71.1 |
| Zafra-Llerena | 121.4 | 100.4 | 28.2 | 12.9 | 91.5 | 24.2 | 30.9 | 46.4 | 61.1 |
| Caceres | 93.5 | 95.6 | 70.2 | 25.5 | 66.1 | 40.5 | 37.4 | 41.1 | 57.0 |
| Coria | 91.9 | 95.4 | 36.2 | 16.4 | 53.5 | 42.0 | 55.4 | 54.8 | 50.3 |
| Plasencia | 61.4 | 72.4 | 72.9 | 42.1 | 75.4 | 59.2 | 68.7 | 62.6 | 44.2 |
| Navalmoral | 77.0 | 48.3 | 57.7 | 40.3 | 60.9 | 51.2 | 45.2 | 37.7 | 65.3 |
| Extremadura | 88.7 | 88.3 | 40.5 | 24.1 | 68.1 | 40.9 | 44.4 | 45.7 | 52.7 |
| Spain | 82.7 | 74.1 | 80.0 | 72.5 | 74.6 | 77.1 | 80.6 | 83.2 | 82.0 |

| Table 3. Vaccination coverage for the Td vaccine in the autonomous regions of Spain, 201612 | |||
|---|---|---|---|
| Andalucia | 72.6 | Aragon* | 88.0 |
| Asturias | 88.8 | Balearic Islands* | 83.0 |
| Canary Islands | 73.0 | Cantabria | 81.8 |
| Castilla y Leon | 84.7 | Castilla-La Mancha | 84.1 |
| Catalonia | 96.4 | Valencian Community | 76.2 |
| Extremadura | 52.7 | Galicia | 86.4 |
| Madrid | 85.3 | Murcia | 75.7 |
| Navarre | 92.2 | Basque Country | 84.3 |
| La Rioja | 92.2 | Ceuta | 63.6 |
| Melilla | 78.2 | ||
Broader studies of vaccination coverage data would be useful, starting with the rest of the towns included in the Don Benito-Villanueva health district with potential expansion in later projects to other health districts, all with the aim of identifying the causes of these low coverage rates and guiding improvements in vaccination strategies so that the vaccination coverage rates will increase toward the national average. Although the electronic records system was introduced in the entire territory of Extremadura in 2008, there are substantial differences in vaccination coverage in all health districts and different years that cannot be explained (Table 2). In the 9 years that the electronic system has been in use (2008-2016), correct vaccination was achieved in half of the population of adolescents aged 14 years. These data were very similar across health districts. In all health districts, there were years with high vaccination coverage rates compared to others with very low rates, and there was no clear secular trend in any of them.
This low coverage should be a red flag for health care authorities and professionals about possible future trends. One of the possible reasons for this low coverage is the decline in the number of routine visits to the paediatrician performed in the context of the Well Child programme at age 14 years.
Some of the measures that could be implemented to prevent a low vaccine coverage rate for the booster dose are improved patient engagement strategies, such as administration on the vaccine during the routine visits scheduled in public health programmes, and urging medical and nursing staff to review the vaccination status and bring the patient up to date with vaccination in every visit, or to include alerts in the electronic health records, among other possible strategies to improve vaccination coverage. Coverage could also improve if campaigns for vaccination against tetanus were once more implemented in the school setting, as is currently being done to immunise girls against human papillomavirus. On the other hand, it is important that primary care team members are aware of the importance of correct vaccination and that they perform it rigorously, documenting each administered dose of vaccine, each dose added or taken from the stock and the storage conditions in health care facilities. The subtraction of a dose of vaccine from the total stock count can be due to administration of the dose or to loss of doses due to failure of the cold chain or mishandling during vaccination, among other reasons, all of which need to be taken into account at the time of calculating vaccination coverage. It is important that both paediatric nurses and health care staff responsible for vaccines, pharmacists in the case of Extremadura, are aware and motivated enough to perform related duties rigorously. Specific training on vaccines is also essential in this regard.
Lastly, given the low vaccination coverage found in recent years in Extremadura (although not so in Santa Amalia) for the booster dose of tetanus vaccine scheduled for age 14 years, broader studies should be conducted to assess the situation and identify the actual reasons why coverage is this low compared to the national average. There is an obvious need for intervention and for change in vaccination strategies, efforts that are already underway.
Year 2017 was not included in the analysis because the Ministry of Health, Consumption and Social Welfare of Spain introduced a new system for calculating the vaccination coverage as agreed by the Committee of Public Health in October 2017.
CONFLICTS OF INTEREST
The author has no conflicts of interest to declare in relation to the preparation and publication of this study.
TheThe contents of this article are based on the final practical project presented for the completion of the Certificate of Higher Education in Public Health (2017) of the School of Health Sciences and Social and Health Care of Extremadura, 2017, accredited by the Escuela Nacional de Sanidad (National School of Health), and the author is the sole individual responsible for the accuracy of the published data.
ABBREVIATIONS
CAV-AEP: Advisory Committee on Vaccines of the Asociación Española de Pediatría · GVAP: Global Vaccine Action Plan · INE: Instituto Nacional de Estadística · Td: low antigen load tetanus and diphtheria vaccine · Tdap: tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine · WHO: World Health Organization.
ACKNOWLEDGMENTS
I thank the following health care professionals for their valuable contributions both in conducting research and in reviewing the manuscript for publication: Adolfo Arias Senso, family physician at the CS de Santa Amalia; Teresa Gallego-Martín, pharmacist, biochemist, doctor in biomedical research and postdoctoral research fellow at the University of Pittsburgh (USA); Eulalio Ruiz Muñoz, physician with a certificate of higher education in public health at the General Directorate of Public Health of the Public Health System of Extremadura.
REFERENCES
- Grupo de trabajo recomendaciones Td 2017. Ponencia de Programa y Registro de Vacunaciones. Recomendaciones de utilización de vacunas Td. In: Ministerio de Sanidad, Servicios Sociales e Igualdad [online] [accessed 14/10/2019]. Available at www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/docs/TetanosDifteria_2017.pdf
- Ponencia de Programa y Registro de Vacunaciones. Vacunación en adultos. Recomendaciones. Vacuna de difteria y tétanos. Actualización 2009. In: Ministerio de Sanidad y Consumo [online] [accessed 14/01/2019]. Available at www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/docs/TetanosDifteria_2009.pdf
- Torres MM, Ramos E, Bonillo A, Sánchez F. Estrategia de seguimiento de la vacunación antitetánica en adultos. Vacunas. 2004;5:61-4.
- Tuells J. Controversias sobre vacunas en España, una oportunidad para la vacunología social. Gac Sanit. 2016;30:1-3.
- Moreno-Pérez D, Álvarez FJ, Arístegui J, Cilleruelo MJ, Corretger JM, García N, et al. Calendario de vacunaciones de la Asociación Española de Pediatría (CAV-AEP): recomendaciones 2017. An Pediatr (Barc). 2017;86:98.e1-98.e9.
- Limia-Sánchez A, Andreu MM, de Viarce Torres de Mier M, Navarro-Alonso JA. Nuevo calendario de vacunación para España, 2016 (Parte 1). Rev Esp Salud Pública. 2016;90:e20001.
- Navarro-Alonso JA, Taboada-Rodríguez JA, Limia-Sánchez A. Nuevo calendario de vacunación para España, 2016 (Parte 2). Rev Esp Salud Pública. 2016;90:e20002.
- Dirección General de Salud Pública. Programa de vacunaciones en Extremadura; año 2017. In: Servicio Extremeño de Salud, Consejería de Sanidad y Políticas Sociales, Junta de Extremadura [online] [accessed 14/10/2019]. Available at https://saludextremadura.ses.es/filescms/ventanafamilia/uploaded_files/CustomContentResources/Programas%20de%20vacunaciones%20en%20Extremadura.%20DG%20de%20Salud%20P%C3%BAblica.%202017.pdf
- Mauro Ramos J. Declarado un caso de tétanos en adulto sin vacunar en Extremadura [News section of the website of the Public Health System of Extremadura]. July 4, 2017 [accessed 31/07/2017]. [Restricted online access; available only to employees of the Public Health System of Extremadura]
- Grupo de Patología Infecciosa de la AEPap. Posicionamiento de la Asociación Española de Pediatría de Atención Primaria sobre vacunación infantil: análisis crítico y propuestas de mejora. 2016. In: Acta Sanitaria [online] [accessed 14/10/2019]. Available at www.actasanitaria.com/wp-content/uploads/2016/01/documento-de-posicionamiento.pdf
- Tabla 2A Coberturas de vacunación de recuerdo. España 2008-2016. In: Ministerio de Sanidad, Consumo y Bienestar Social [online] [accessed 14/10/2019]. Available at www.mscbs.gob.es/en/profesionales/saludPublica/prevPromocion/vacunaciones/docs/CoberturasVacunacion/Tabla2.pdf
- Tabla 6: Coberturas de vacunación de refuerzo en niños de 4 a 14 años. Comunidades autónomas, 2016. In: Ministerio de Sanidad, Servicios Sociales e Igualdad [online] [accessed 14/10/2019]. Available at www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/docs/CoberturasVacunacion/Todas_las_tablas2016.pdf