
Vol. 21 - Num. 82
Original Papers
What do our elementary school children know about bullying?
M.ª Mar Alonso Montejoa, Eduardo Zamorano Gonzálezb, Juana M.ª Ledesma Albarránc
aMIR-Pediatría. Hospital Materno Infantil de Málaga. Málaga. España.
bMédico. Málaga. España.
cPediatra. CS Delicias. Málaga. España.
Correspondence: MM Alonso. E-mail: marialonsom9@gmail.com
Reference of this article: Alonso Montejo MM, Zamorano González E, Ledesma Albarrán JM. What do our elementary school children know about bullying? Rev Pediatr Aten Primaria. 2019;21:121-9.
Published in Internet: 11-04-2019 - Visits: 23128
Abstract
Background: bullying is an emergent problem that is growing in importance on account of its increasing prevalence and its impact on the children that experience it (health, academic or psychosocial problems).
Objectives: to analyse and determine the different characteristics of victims and bullies, explore their health problems, identify the characteristics of cyberbullying and assess the effectiveness of interventions targeting students for the prevention of bullying.
Materials and methods: the sample included 65 students (59.4% female, 21.9% victims and 17.2% bullies), that completed a validated questionnaire about school bullying. We used a pre-test, post-intervention study and established intervention and control groups.
Results: we found differences between victims and non-victims in academic problems, the location of the computer in the habitual residence of the child and in feelings of sadness. We found that 12.5% of surveyed students reported having witnessed cyberbullying in the past 2 months. We found differences between the pre-test and post-test periods in several variables (ignoring, badmouthing, hitting, hiding belongings). Lastly, we found significant differences between the intervention and the control groups in the stealing of belongings.
Conclusions: in conclusion, our findings corroborated the importance of the early detection of school bullying and the need to implement interventions to decrease its prevalence.
Keywords
● Anxiety ● Bullying ● Depression ● Somatic symptom disordersINTRODUCTION
School bullying and victimisation are widespread phenomena in childhood that are of great relevance and importance to various agents in education and public health as well as parents, teachers, counsellors and health professionals.
According to Olweus1, bullying is defined as recurrent negative actions performed over time within a relationship characterised by an imbalance of strength and power. That is, school bullying is a behaviour performed repeatedly and over time by one individual or group with the purpose of hurting, threatening, intimidating, blackmailing, excluding, frightening or harassing another person with the intention of causing some type of harm. The characteristic that differentiates bullying from other types of aggressive behaviour is the power imbalance between the victim and the perpetrator.2 Bullying may be physical or psychological, and in every instance is an attack on the dignity and rights of the other party.
There is a particular form of school bullying known as cyberbullying that takes place through mobile phone applications (text messages, pictures, calls, videos), the internet (email, social networks, instant messaging, webpages, chats) or other information and communication technologies.2 The most recent scientific studies on the subject have reported data on this form of bullying. In November 2011, a study on privacy and security in the use of mobile services by Spanish children conducted by INTECO and Orange found that 2.5% of Spanish minors had been subject to cyberbullying by other minors through their mobile phones.3
The involvement of children in school bullying, be it as bullies or victims, has a significant impact on their wellbeing.4,5 Victims are at higher risk of suffering health problems, low self-esteem and psychiatric disorders such as anxiety, depression and psychotic symptoms. Bullies exhibit more behavioural problems and a poorer social adjustment throughout the lifespan. In addition, both victims and bullies tend to have poorer academic outcomes compared to children that are not involved in bullying.4 These adverse outcomes are independent of the behavioural and emotional problems that may have existed prior to the start of bullying and victimization.4,5
Victims of school bullying are more likely to experience sleep disturbances, enuresis, abdominal pain, headache and sadness compared to peers not affected by bullying. They are also more likely to experience anxiety and depression and miss school,6 with an increased risk in those that experience cyberbullying compared to traditional school bullying.7,8
There is a clear association between parental educational attainment and the prevalence of bullying in children. Thus, children of parents who are unemployed, with a low educational attainment or a low socioeconomic status are at higher risk of being victims or bullies. Living in single-parent household and having young parents are also risk factors.4
The prevalence of this problem is increasing. In Spain, a systematic review by García et al. that included 120 000 children with a mean age of 14.6 years between 1999 and 2016 found an overall prevalence of traditional school bullying of 13.3% and of cyberbullying of 7.62%. The percentage of children that have experienced both school bullying and cyberbullying simultaneously was 6.90%.9
On account of this high prevalence and the impact that bullying may have on health and academic performance, interventions are being developed to prevent bullying and to respond to it once it occurs (primary and secondary prevention, respectively).
Primary objectives: to determine the different personal and household characteristics of students who are or are not potential victims and non-victims; determine the personal and household characteristics of students who are or are not potential bullies and assess the frequency and characteristics of cyberbullying in the students included in the study.
Secondary objectives: to determine the frequency of health problems in students that are potential victims and potential bullies and those who are not, and analyse the effectiveness of various types of interventions to prevent bullying and raise awareness of it in different types of students (bullies, victims and witnesses).
MATERIALS AND METHODS
We conducted a pre-test, post-test quasi-experimental study with an intervention phase and 2 student groups (intervention group and control group without intervention). We compared a group of children enrolled in the 5th year of compulsory elementary education (CEE) in the pre-test period with the same group in the post-test period when the children were enrolled in the 6th year of CEE. We also compared the intervention and control groups in the post-test period. In both groups of students, we assessed the subgroups of victims, non-victims, bullies, non-bullies and witnesses.
We enrolled students by means by simple random sampling, including children enrolled in the 6th year of the CEE in a public school located in a middle-class residential neighbourhood in Malaga city. After obtaining the signed informed consent of the parents or legal guardians, we administered the questionnaire to the students of the selected school. The questionnaires were completed anonymously.
The exclusion criteria were absence of signed informed consent from a parent or legal guardian, refusal of the student to participate and incorrect completion of the questionnaire. The study was approved by the Research Ethics Committee of the Province of Malaga.
We used a questionnaire that has been validated and used in the past for developing the report Violencia escolar: el maltrato entre iguales en la Educación Secundaria Obligatoria 1999 (Violence in Schools—abuse between peers in Compulsory Education 1999),10 expanded by our research team with the addition of items to assess cyberbullying and somatization (Appendix 1 in the supplemental materials).
We analysed the following variables:
- Primary variables: epidemiological (age, sex, academic achievement, country of origin of participant and the parents, household composition, parental employment); cyberbullying (means of bullying: mobile phone, computer, bullying individual, feelings and duration of bullying); and school bullying (social exclusion: ignoring, not allowing joining in; verbal abuse: insults, insulting nicknames, gossiping; indirect physical abuse: hiding or breaking belongings; direct physical abuse: hitting; threatening or blackmailing).
- Secondary variables: epidemiological (falling behind one year in school, number of siblings and sibling order, ownership of a mobile phone, internet access and location of computer in the home); and health problems (sleep problems, enuresis, sad mood, headache, abdominal pain and school absenteeism).
We classified responses for qualitative data with the categories never, sometimes, often and always.
In 2015, we collected the data for what we considered the pre-test survey. The following academic year, we classified participants into 3 groups according to their classrooms. Each classroom was randomly assigned to either an intervention (2 different interventions) or the lack of intervention (control group). Once the interventions were completed, we collected the post-test data by consecutive sampling in the school setting during school hours. A resident in paediatrics and a medical student supervised the completion of questionnaires, answering any questions or concerns posed by the students. Teachers could also address these questions at any time, consulting with the resident or the medical student if needed.
The interventions performed in each group were the following:
Intervention I
- 90-minute talk delivered by a health care professional with the aim of educating and raising awareness on school bullying. The talk had a traditional one-way teaching format in which a resident in paediatrics and a medical student explained introduced and explained the basic concepts of bullying to the students.
- The key concepts covered in the talk were: definition and types of school bullying; especial emphasis on a type of bullying that has been growing in recent years (cyberbullying); how to identify bullying; how to prevent bullying; and how to act in response to bullying as either a victim or a witness.
Intervention II
- Interactive educational activity in the classroom in which all participants worked together to define bullying, discussed how to prevent it and how to face these situations (two-way learning approach). During this session, it was the students that defined and analysed the concepts related to school bullying with the help of the paediatrics resident physician and medical student. The latter guided the students so they could reach their own conclusions and have a debate. At the end of the session, one or more students summarised what had been discussed.
- The key concepts covered in the session were: definition and types of school bullying; especial emphasis on a type of bullying that has been growing in recent years (cyberbullying); how to identify bullying; how to prevent bullying; and how to act in response to bullying as either a victim or a witness.
For objectives 1, 2, 4 and 5 we performed comparisons between groups and measurements using the χ2 test. For objective 3 we performed descriptive analyses. We used the software SPSS 20.0. In the statistical analysis, we summarised variables as absolute frequencies and percentages, calculating point values and 95% confidence intervals.
RESULTS
The initial sample included 65 children enrolled in the 6th year of CEE in a public school. We excluded 1 questionnaire because it was incomplete. Of the 64 final respondents, 96.9% had a Spanish nationality (59.4% were female, 21.9% victims, 17.2% bullies and 7.8% had been held back a year), 17.2% lived in a single-parent home, 3.1% with the grandparents and 4.7% in a different situation (excluding a two-parent household). The mean number of siblings was 2.19, with a standard deviation (SD) of 0.77; 76.9% had a mobile phone, which had access to the internet in 70.3% of cases.
We considered victims of bullying those students who reported one of the following in the academic year when we conducted the survey: always experiencing some type of bullying always; experiencing 3 different types of bullying sometimes; experiencing one type of bullying often and another type of bullying sometimes.
We considered bullies those students who reported one of the following in the academic year when we conducted the survey: having performed some type of bullying always; having performed 3 different types of bullying sometimes; having performed some type of bullying often and another type sometimes from the beginning of the academic year.
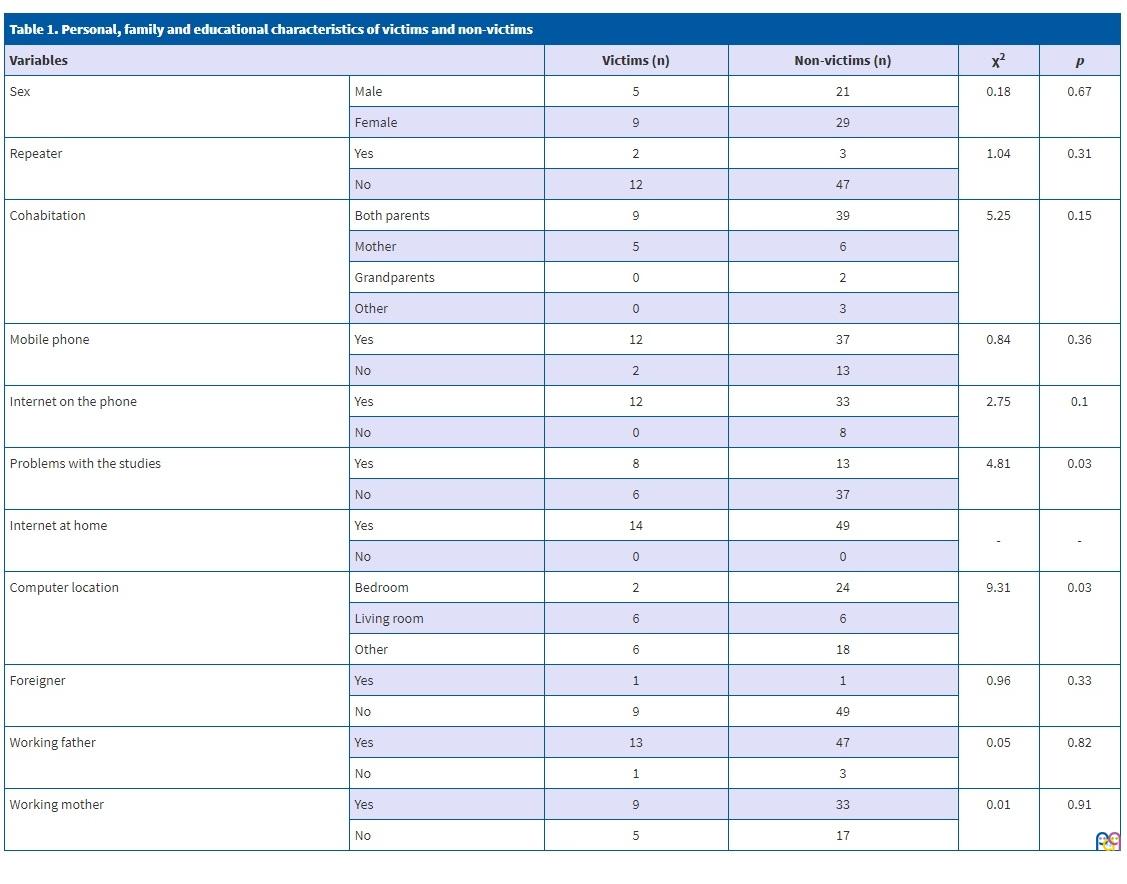
Table 1 presents the personal, household and educational characteristics of victims and non-victims. The comparison of bullies and non-bullies did not find significant differences in any of the variables under study.
| Table 1. Personal, family and educational characteristics of victims and non-victims | |||||
|---|---|---|---|---|---|
| Variables | Victims (n) | Non-victims (n) | χ2 | p | |
| Sex | Male | 5 | 21 | 0.18 | 0.67 |
| Female | 9 | 29 | |||
| Repeater | Yes | 2 | 3 | 1.04 | 0.31 |
| No | 12 | 47 | |||
| Cohabitation | Both parents | 9 | 39 | 5.25 | 0.15 |
| Mother | 5 | 6 | |||
| Grandparents | 0 | 2 | |||
| Other | 0 | 3 | |||
| Mobile phone | Yes | 12 | 37 | 0.84 | 0.36 |
| No | 2 | 13 | |||
| Internet on the phone | Yes | 12 | 33 | 2.75 | 0.1 |
| No | 0 | 8 | |||
| Problems with the studies | Yes | 8 | 13 | 4.81 | 0.03 |
| No | 6 | 37 | |||
| Internet at home | Yes | 14 | 49 | - | - |
| No | 0 | 0 | |||
| Computer location | Bedroom | 2 | 24 | 9.31 | 0.03 |
| Living room | 6 | 6 | |||
| Other | 6 | 18 | |||
| Foreigner | Yes | 1 | 1 | 0.96 | 0.33 |
| No | 9 | 49 | |||
| Working father | Yes | 13 | 47 | 0.05 | 0.82 |
| No | 1 | 3 | |||
| Working mother | Yes | 9 | 33 | 0.01 | 0.91
|
| No | 5 | 17 | |||
The findings of the descriptive analysis of the items included in the questionnaire pertaining to cyberbullying were the following:
- 12.5% of students reported that there was cyberbullying in their school in the past 2 months, 6.3% reported having experienced this type of bullying through the mobile phone, and 10.9% through the internet but a non-mobile device.
- 4.7% of students reported having bullied online through nonmobile devices, and 0% bullying through a mobile device.
- When it came to the impact of cyberbullying compared to traditional bullying, 37.5% stated they did not know whether there were any differences, 29.7% stated they had the same effect and 18.8% that it had a stronger effect.
- Of all students that reported being victims, 3.1% stated being bullied by a boy and 8% not knowing who was bullying them.
- When it came to their emotional response to cyberbullying, 6.3% reported feeling unwell, 3.1% sad, 6.3% angry and 3.1% worried.
- When faced with bullying, 3.1% cried or ignored it, and the rest of the possible answers all had a frequency of 1.6%: told their parents, teachers or friends, asked the bully to stop, done the same thing back or shut down the application or window.
- Cyberbullying in the internet was experienced through chatrooms by 4.7% of students, instant messaging by 3.1% and websites by 1.6%.
- The duration of cyberbullying through the internet was of 2 to 3 weeks in 3.1% and less than 1 week in 4.1%.
- Cyberbullying through the mobile phone was experienced by 1.6% of students through WhatsApp and by 6.3% of students through other mobile applications.
- 50% of the students believed that banning phone use in school would help, 31.3% that it would result in the bullying occurring after school, and 18% that despite this measure students would still use the phone when teachers were not paying attention.
The analysis of the health problems of victims and bullies only revealed differences in sadness (χ2 = 15.4; p < 0.002) between victims and non-victims.
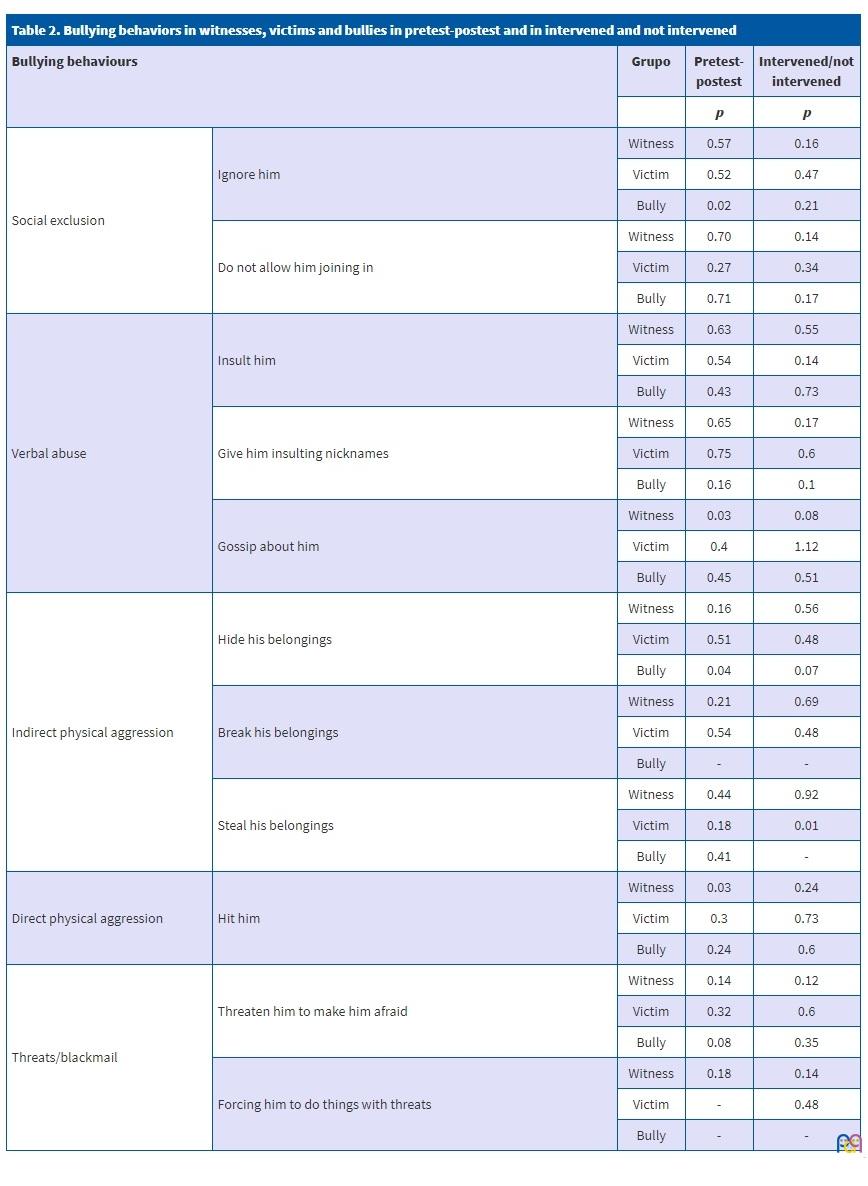
Table 2 shows the results of the analyses comparing the pre-test and post-test periods, on one hand, and the intervention and control groups, on the other, taking into account the witness, victim and bully subgroups in both.
| Table 2. Bullying behaviors in witnesses, victims and bullies in pretest-postest and in intervened and not intervened | ||||
|---|---|---|---|---|
| Bullying behaviours | Grupo | Pretest-postest | Intervened/not intervened | |
| p | p | |||
| Social exclusion | Ignore him | Witness | 0.57 | 0.16 |
| Victim | 0.52 | 0.47 | ||
| Bully | 0.02 | 0.21 | ||
| Do not allow him joining in | Witness | 0.70 | 0.14 | |
| Victim | 0.27 | 0.34 | ||
| Bully | 0.71 | 0.17 | ||
| Verbal abuse | Insult him | Witness | 0.63 | 0.55 |
| Victim | 0.54 | 0.14 | ||
| Bully | 0.43 | 0.73 | ||
| Give him insulting nicknames | Witness | 0.65 | 0.17 | |
| Victim | 0.75 | 0.6 | ||
| Bully | 0.16 | 0.1 | ||
| Gossip about him | Witness | 0.03 | 0.08 | |
| Victim | 0.4 | 1.12 | ||
| Bully | 0.45 | 0.51 | ||
| Indirect physical aggression | Hide his belongings | Witness | 0.16 | 0.56 |
| Victim | 0.51 | 0.48 | ||
| Bully | 0.04 | 0.07 | ||
| Break his belongings | Witness | 0.21 | 0.69 | |
| Victim | 0.54 | 0.48 | ||
| Bully | - | - | ||
| Steal his belongings | Witness | 0.44 | 0.92 | |
| Victim | 0.18 | 0.01 | ||
| Bully | 0.41 | - | ||
| Direct physical aggression | Hit him | Witness | 0.03 | 0.24 |
| Victim | 0.3 | 0.73 | ||
| Bully | 0.24 | 0.6 | ||
| Threats/blackmail | Threaten him to make him afraid | Witness | 0.14 | 0.12 |
| Victim | 0.32 | 0.6 | ||
| Bully | 0.08 | 0.35 | ||
| Forcing him to do things with threats | Witness | 0.18 | 0.14 | |
| Victim | - | 0.48 | ||
| Bully | - | - | ||
DISCUSSION
Our study found a proportion of victims of 21.9% and a proportion of bullies of 17.2%. The proportion of victims was higher compared to other studies conducted in children of similar ages in the Netherlands.4 This difference may be due to a lesser frequency of bullying in the Netherlands compared to other countries such as the United States.4 The prevalence found in our study also exceeded the average prevalence found in the past 15 years in Spain,4 although in the latter case the children were older and the sample larger, which may explain the discrepancy. The proportion of bullies was practically identical to the proportion found by the aforementioned study.
When it came to the first objective of our study, which was to compare the personal and household characteristics of victims and non-victims of school bullying, we found significant differences between these two groups, as victims had more problems in these areas. Involvement in bullying situations is associated with increased absenteeism and poorer academic performance,5,10 which was reflected in our findings. We also found significant differences in the location of the computer at home. These differences may be due to differences in the monitoring by parents or legal guardians of computer use by children. However, we did not find any differences in other variables (low socioeconomic level, single-parent household, etc) that had been identified as significant in other studies;4 we believe this may be due to the small sample size in our study.
As for our second objective, which was to compare the different personal and household characteristics of potential bullies and non-bullies, we did not find any significant differences between the 2 groups. Students from non-traditional, dysfunctional and low socioeconomic status households are more often involved as bullies,4 as do students with poor academic performance.12 The discrepancy of our findings on this aspect with the previous literature may be due to the fact that our sample was homogeneous in terms of socioeconomic status.
Our third objective was to establish the frequency and characteristics of cyberbullying in the sample of students. We found a prevalence of 12.5%. In Spain, the prevalence of cyberbullying is of approximately 7.6%.4 This prevalence is lower compared to the one found in our study, but when we sought prevalence data for each autonomous community in Spain, we found that the prevalence in Andalusia was of 9.5%.2 Although this value was closer to our findings, the difference is still far from negligible. In any case, the frequency of cyberbullying has been increasing in recent years in North America, Asia and Europe.1 In our sample, 100% of the victims of cyberbullying were girls. In Andalusia overall, the corresponding percentage is 67.2%.2 This difference is probably due to the small sample size in our study, although it could also result from selection bias.
The fourth objective was to compare the frequency of health problems in students identified as possible victims or possible bullies, and we found significant differences between the victim and non-victim groups in the presence of sadness: victims were more likely to experience this symptom. Victims of school bullying experience health problems such as sleep disturbances, enuresis, abdominal pain, headache, sadness and other depressive symptoms more frequently than children that are not bullied.5,11 We did not find significant differences in any other of the health problems under study, which we attribute to the small sample size.
Our fifth goal was to assess the effectiveness of the implementation of different interventions for preventing school bullying and raising awareness in different types of students (bullies, victims and witnesses). We found significant differences in the pre-test and post-test assessment of the witness subgroup in the gossip and hitting variables. We also found significant differences between the intervention and control groups within the victim subgroup in regard to the stealing of belongings. However, we did not find statistically significant differences in any of the variables under study in the rest of the subgroups, either in the pre-test/post-test comparison or between the intervention and control groups. Future studies need to implement broader and longer interventions to determine whether they have a stronger effect on the different groups of students. On the other hand, the use of school-based educational interventions similar to the one implemented in our study in other countries has also proven ineffective for reducing the frequency of bullying.6 Only one study found significant differences in one of the variables under study, but it was due to exposure to an intervention outside the school.13. Longer interventions (lasting several months) involving both students and teachers and including training in social skills have achieved better outcomes in terms of a reduction in the incidence of bullying in the samples under study.6
A study conducted by Ellen Sánchez et al. found that 1 year after implementation of a multidisciplinary antibullying programme (involving teachers, parents, students and police) in 6 schools, the students were less reluctant to denounce bullying, although there was no impact on the prevalence of this problem.14
CONCLUSIONS
- School bullying and cyberbullying are very common phenomena in childhood that are highly relevant to stakeholders and agents in the fields of education and clinical practice.
- Their prevalence is increasing and is greater in Andalusia compared to the mean prevalence in Spain, which makes the problem all the more alarming in our region.
- There are personal and family circumstances that are more frequent in victims of school bullying, which could help identify collectives at risk.
- Some health problems are more prevalent in victims of bullying, which can help primary care paediatricians in the diagnosis of school bullying.
- The delivery of interventions targeting the students did not prove useful in the prevention of school bullying under the circumstances that applied in our study. In light of this, it would be interesting to develop longer interventions involving students and teachers to develop interpersonal skills with the aim of reducing the prevalence of school bullying and raise awareness of this problem in children.
- Future studies should be conducted with larger samples and including different age groups, as bullying is starting at increasingly young ages.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS
SD: standard deviation · CEE: compulsory elementary education.
SUPPLEMENTAL MATERIALS
REFERENCES
- Caravaca Sánchez F, Falcón Romero M, Navarro-Zaragoza J, Luna Ruiz-Cabello A, Rodriges Frantzisko O, Luna Maldonado A. Prevalence and patterns of traditional bullying victimization and cyber-teasing among college population in Spain. BMC Public Health. 2016;16:176.
- Sastre A, Calmaestra J, Escorial A, García P, del Moral C, Perazzo C, et al. Yo a eso no juego: bullying y ciberbullying en la infancia. 1st edition. In: Save The Children [online] [accessed 04/04/2019]. Available at www.savethechildren.es/sites/default/files/imce/docs/yo_a_eso_no_juego.pdf
- Pérez P, de la Fuente S, García L, Guijarro J, Blas ME; INTECO. Estudio sobre seguridad y privacidad en el uso de servicios móviles por los menores españoles. In: Pantallas Amigas [online] [accessed 04/04/2019]. Available at www.pantallasamigas.net/pdf/estudio_sobre_seguridad_y_privacidad_en_el_uso_de_los_servicios_moviles_por_los_menores_espanoles.pdf
- Jansen P, Verlinden M, Berkel A, Mieloo C, van der Ende J, Veenstra R, et al. Prevalence of bullying and victimization among children in early elementary school: do family and school neighbourhood socioeconomic status matter? BMC Public Health. 2012;12:494.
- Schreier A, Wolke D, Thomas K, Horwood J, Hollis C, Gunnell D, et al. Prospective study of peer victimization in childhood and psychotic symptoms in a nonclinical population at age 12 years. Arch Gen Psychiatry. 2009;66:527-36.
- Vreeman RC, Carroll AE. A systematic review of school-based interventions to prevent bullying. Arch Pediatr Adolesc Med. 2007;161:78-88.
- Bogart LM, Elliot MN, Klein DJ, Tortolero SR, Mrug S, Peskin MF, et al. Peer victimization in fifth grade and health in tenth grade. Pediatrics. 2014;133:440-7.
- Wang J, Nansel TR, Iannotti R. Cyber and traditional bullying: differential association with depression. J Adolesc Health. 2011;48:415-7.
- García-García J, Ortega E, De la Fuente L, Zaldivar F, Gil Fenory, MJ. Systematic review of the prevalence of school violence in Spain. Procedia - Soc Behavioral Sci. 2017;237:125-9.
- Violencia escolar: el maltrato entre iguales en la Educación Secundaria Obligatoria 1999-2006. In: Defensor del Pueblo [online] [accessed 04/04/2019]. Available at www.defensordelpueblo.es/wp-content/uploads/2015/05/2007-01-Violencia-escolar-el-maltrato-entre-iguales-en-la-Educaci%C3%B3n-Secundaria-Obligatoria-1999-2006.pdf
- Elgar FJ, Craig W, Boyce W, Morgan A, Vella-Zarb R. Income inequality and school bullying: multilevel study of adolescents in 37 countries. J Adolesc Health. 2009;45:351-9.
- Glew GM, Fan MY, Katon W, Rivara FP, Kernic MA. Bullying, psychosocial adjustment, and academic performance in elementary school. Arch Pediatr Adolesc Med. 2005;159:1026-31.
- Ramya SG, Kulkarni ML. Bullying among school children: prevalence and association with common symptoms in childhood. Indian J Pediatr. 2011;78:307-10.
- Sánchez E, Robertson TR, Lewis CM, Rosenbluth B, Bohman T, Casey DM. Preventing bullying and sexual harassment in elementary schools. J Emot Abus. 2001;2:157-80.