
Vol. 20 - Num. 77
Original Papers
How do primary care paediatricians guide complementary feeding in Spain?
Ana Martínez Rubioa, M.ª Dolores Cantarero Vallejob, Beatriz Espín Jaimec
aPediatra. CS de Camas. Sevilla. España.
bPediatra. CS de Illescas . Toledo. España.
cSección de Gastroenterología, Hepatología y Nutrición Pediátrica. Hospital Universitario Infantil Virgen del Rocío. Sevilla. España.
Correspondence: A Martínez. E-mail: mrubiorama@gmail.com
Reference of this article: Martínez Rubio A, Cantarero Vallejo MD, Espín Jaime B. How do primary care paediatricians guide complementary feeding in Spain? Rev Pediatr Aten Primaria. 2018;20:35-44.
Published in Internet: 16-02-2017 - Visits: 37449
Abstract
Objectives: to assess the attitudes of Spanish primary care paediatricians regarding complementary feeding and review the published evidence on the baby-led-weaning approach.
Methods: a thirty-six item questionnaire about complementary feeding and baby-led-weaning was drafted and distributed through the Spanish Association of Primary Care Paediatricians mailing list.
Results: we received 579 responses. Of all respondents, 95.3% reported using an informational handout (28.6% of their own making). Paediatricians recommended introducing complementary foods at age six months (60.6%), five months (24.9%) and four months (10.7%), and cereal was the food recommended to start complementary feeding by 39.4% of respondents. Nearly 61% of physicians recommended spoon-feeding, 21.4% bottle-feeding and 17.4% no particular feeding method. Of all respondents, 54.6% recommended giving the child foods to chew as soon as the child showed interest in it, and up to 10.7% recommended delaying it under age 1 year. Seventy-nine percent knew about baby-led-weaning, 45.3% recommended it in some cases and 6.6% routinely. The main concerns of the respondents were lack of information (67.2%), lack of scientific evidence (10.6%) and the potential risk of choking (10.6%).
Conclusions: there is huge variability in the recommendations regarding complementary feeding. The approach used most frequently in Spain is the traditional one. The number of paediatricians that know about the baby-led-weaning approach is growing, but few are prepared to recommend it routinely.
Keywords
● Feeding ● InfantsINTRODUCTION
There is little scientific evidence on the impact of different approaches to the introduction of complementary feeding (CF) in the future health of children, the development of healthy dietary habits and the prevention of adult diseases such as obesity, hypertension, type 2 diabetes or cardiovascular disease.1
In recent years, the method known as baby-led-weaning (BLW), which promotes infant self-feeding of whole foods of a shape and size that the infant can grasp and put in the mouth as opposed to spoon-feeding of puréed foods by parents, has become widespread.2
The aim of our study was to assess the attitudes of primary care paediatricians in Spain regarding CF and the BLW approach in particular, and to conduct a review of the evidence published to date on the introduction of CF through BLW.
MATERIALS AND METHODS
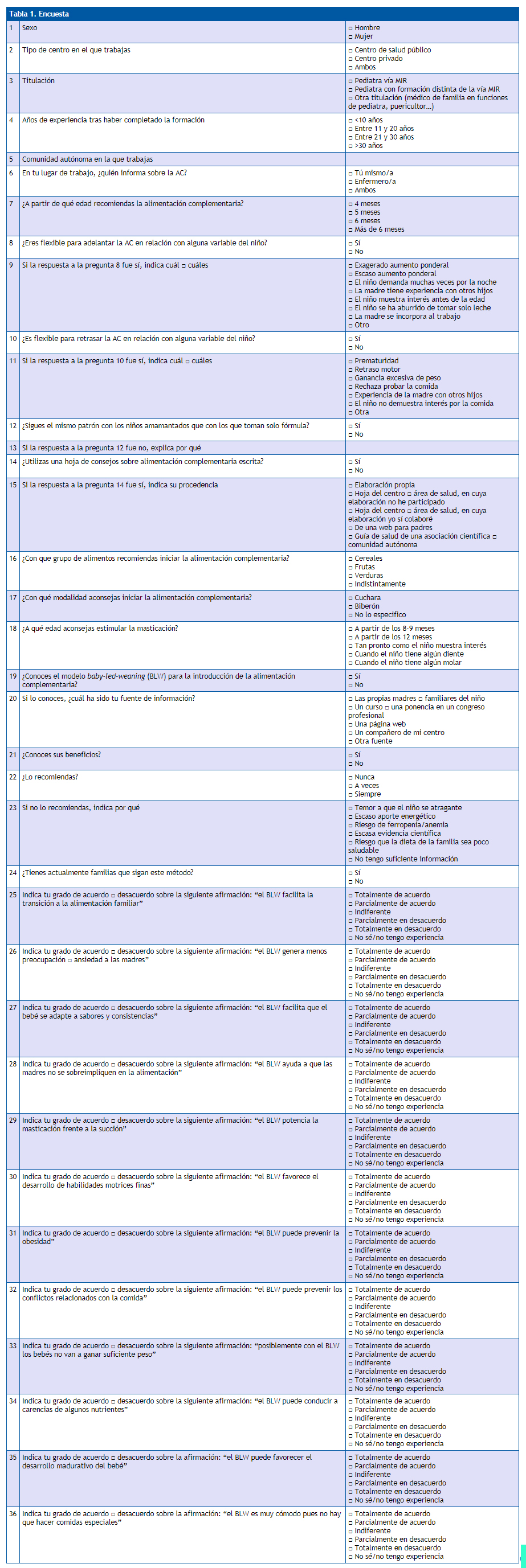
We conducted a descriptive study by developing a structured questionnaire with 36 open- and close-ended questions regarding the approach to the introduction of CF and assessing the familiarity with the BLW approach (Table 1).
| Table 1. Questionnaire | ||
|---|---|---|
| 1 | Sex | □ Male □ Female |
| 2 | Work setting | □ Public health centre □ Private clinic □ Both |
| 3 | Professional title | □ Paediatrician with MIR residency □ Paediatrician with training other than MIR □ Other (family physician fulfilling the role of paediatrician, early childhood specialist…) |
| 4 | Years of work experience after completing education | □ <10 years □ 11 to 20 years □ 21 to 30 years □ > 30 years |
| 5 | Autonomous community where you are employed | |
| 6 | In your workplace, who provides information regarding CF? | □ I do □ Nurses □ Both |
| 7 | At which age would you recommend starting complementary feeding? | □ 4 months □ 5 months □ 6 months □ More than 6 months |
| 8 | Are you open to starting CF earlier in certain infants based on specific factors? | □ Yes □ No |
| 9 | If the answer to question 8 was yes, check any that apply | □ Excess weight gain □ Poor weight gain □ Infant demands night feeds too often □ Mother has experience with other children □ The child expresses an interest before that age □ The child is tired of having milk alone □ The mother is returning to work □ Other |
| 10 | Are you open to delaying CF in certain infants based on specific factors? | □ Yes □ No |
| 11 | If the answer to question 10 was yes, check any that apply | □ Preterm birth □ Motor delay □ Excess weight gain □ Refuses food □ Mother has experience with other children □ The child shows no interest □ other |
| 12 | Do you have the same approach to CF in breastfed children compared to children exclusively fed formula? | □ Yes □ No |
| 13 | If the answer to question 12 was no, explain why | |
| 14 | Do you use a written handout with recommendations on CF? | □ Yes □ No |
| 15 | If the answer to question 14 was yes, check the source of the handout | □ I made it myself □ Handout developed by my centre or health care district, without my participation □ Handout developed by my centre or health care district, with my participation □ From a parenting website □ Health care guideline of a scientific association or autonomous community |
| 16 | Which food group do you recommend for starting complementary feeding? | □ Cereals □ Fruits □ Vegetables □ Any of the above |
| 17 | Which feeding method do you recommend for starting complementary feeding? | □ Spoon feeding □ Bottle feeding □ I do not recommend a specific method |
| 18 | At which age do you recommend encouraging chewing? | □ Starting at 8-9 months □ Starting at 12 months □ As soon as the child expresses interest □ Once the child has some teeth □ Once the child has one molar |
| 19 | Do you know the baby-led-weaning (BLW) approach to introducing complementary foods? | □ Yes □ No |
| 20 | If so, which was the source of the information? | □ Mothers or relatives of the child □ A course or a presentation in a professional congress □ Webpage □ Work colleague □ Other |
| 21 | Do you know the benefits of this approach? | □ Yes □ No |
| 22 | Do you recommend this approach? | □ Never □ Sometimes □ Always |
| 23 | If you do not recommend it, explain why | □ Fear of child choking □ Low energy intake □ Risk of iron deficiency/anaemia □ Scarce scientific evidence □ Possibility that the family diet is unhealthy □ I don’t have enough information |
| 24 | Are any of the families in your caseload currently using this method? | □ Yes □ No |
| 25 | Indicate the extent to which you agree or disagree with the following statement: “BLW facilitates the transition to the family diet” | □ Completely agree □ Partly agree □ Neither agree nor disagree □ Partly disagree □ Completely disagree □ I don’t know/don’t have experience on the matter |
| 26 | Indicate the extent to which you agree or disagree with the following statement: “BLW generates less worry or anxiety in mothers” | □ Completely agree □ Partly agree □ Neither agree nor disagree □ Partly disagree □ Completely disagree □ I don’t know/don’t have experience on the matter |
| 27 | Indicate the extent to which you agree or disagree with the following statement: “BLW helps the baby get used to new flavours and textures” | □ Completely agree □ Partly agree □ Neither agree nor disagree □ Partly disagree □ Completely disagree □ I don’t know/don’t have experience on the matter |
| 28 | Indicate the extent to which you agree or disagree with the following statement: “BLW helps mothers not be overinvolved in their child’s nutrition” | □ Completely agree □ Partly agree □ Neither agree nor disagree □ Partly disagree □ Completely disagree □ I don’t know/don’t have experience on the matter |
| 29 | Indicate the extent to which you agree or disagree with the following statement: “BLW promotes chewing over suctioning” | □ Completely agree □ Partly agree □ Neither agree nor disagree □ Partly disagree □ Completely disagree □ I don’t know/don’t have experience on the matter |
| 30 | Indicate the extent to which you agree or disagree with the following statement: “BLW promotes the development of fine motor skills” | □ Completely agree □ Partly agree □ Neither agree nor disagree □ Partly disagree □ Completely disagree □ I don’t know/don’t have experience on the matter |
| 31 | Indicate the extent to which you agree or disagree with the following statement: “BLW may prevent obesity” | □ Completely agree □ Partly agree □ Neither agree nor disagree □ Partly disagree □ Completely disagree □ I don’t know/don’t have experience on the matter |
| 32 | Indicate the extent to which you agree or disagree with the following statement: “BLW may prevent food-related conflicts” | □ Completely agree □ Partly agree □ Neither agree nor disagree □ Partly disagree □ Completely disagree □ I don’t know/don’t have experience on the matter |
| 33 | Indicate the extent to which you agree or disagree with the following statement: “babies may not gain enough weight with the BLW approach” | □ Completely agree □ Partly agree □ Neither agree nor disagree □ Partly disagree □ Completely disagree □ I don’t know/don’t have experience on the matter |
| 34 | Indicate the extent to which you agree or disagree with the following statement: “BLW may lead to deficiencies in some nutrients” | □ Completely agree □ Partly agree □ Neither agree nor disagree □ Partly disagree □ Completely disagree □ I don’t know/don’t have experience on the matter |
| 35 | Indicate the extent to which you agree or disagree with the following statement: “BLW may promote the maturational development of the baby” | □ Completely agree □ Partly agree □ Neither agree nor disagree □ Partly disagree □ Completely disagree □ I don’t know/don’t have experience on the matter |
| 36 | Indicate the extent to which you agree or disagree with the following statement: “BLW is very easy, as it does not require preparation of special meals” | □ Completely agree □ Partly agree □ Neither agree nor disagree □ Partly disagree □ Completely disagree □ I don’t know/don’t have experience on the matter |
The questionnaire targeted primary care paediatricians and was distributed in October 2015 via electronic mail through the mailing list of the Asociación Española de Pediatría de Atención Primaria (Spanish Association of Primary Care Paediatrics [AEPap]). We established a 30-day window for the submission of responses, which we then analysed safeguarding the anonymity of participants.
RESULTS
Of the total of 3700 paediatricians of the AEPap to whom we sent the questionnaire, 579 submitted responses (16% of the members), with representation of nearly every autonomous community in Spain (Table 2). Of all respondents, 88.1% were physicians that had completed a medical residency (MIR), and most (85.8%) were employed exclusively in the public health system.
| Table 2. Distribution of analysed responses by autonomous community | ||
|---|---|---|
| Autonomous community | N | % |
| Andalusia | 92 | 15.9 |
| Aragon | 22 | 3.8 |
| Asturias | 9 | 1.6 |
| Baleares | 11 | 1.9 |
| Canarias | 12 | 2.1 |
| Cantabria | 9 | 1.6 |
| Castilla y Leon | 36 | 6.2 |
| Castilla La Mancha | 31 | 5.4 |
| Catalonia | 29 | 5 |
| Autonomous Community of Valencia | 51 | 8.8 |
| Extremadura | 12 | 2.1 |
| Galicia | 30 | 5.2 |
| Madrid | 135 | 23.3 |
| Murcia | 16 | 2.8 |
| Navarre | 21 | 3.6 |
| Basque Country | 56 | 9.7 |
| Rioja | 7 | 1.2 |
| Ceuta | 0 | 0 |
| Melilla | 0 | 0 |
| Total | 579 | 100.0 |

Information on the introduction of CF is usually provided by the paediatrician together with the nursing staff (71.8% of cases), with printed handouts used for this purpose in 95.3% of cases.
Of all participants, 60.6% recommended starting to introduce complementary foods at age 6 months, 24.9% at 5 months and 10.7% at 4 months. Although those are their initial recommendations, 95.5% of paediatricians reported being open to introducing CF earlier, especially in patients with poor weight gain (87.6%) or whose mothers were going back to work (79.9%). Other reasons given for earlier introduction were: excessive weight gain (19.8%), frequent demand of night feeds (51.8%), child expressing interest in foods (49.7%), maternal experience (39.8%) and the child “being tired of milk” (44%).
Similarly, 63.4% were open to delaying the start of CF, especially in children born preterm (71.7%), and less frequently for other reasons such as motor delays (55.9%), excessive weight gain (48.3%), rejection of new foods (46.4%), maternal experience (48.2%) and the child’s lack of interest in CF (37.5%).
Of all respondents, 45.1% reported that they recommend the same schedule for starting CF whether or not the child is currently breastfeeding; 39.4% of paediatricians recommend introducing cereals first, while 44% reported having no preference and recommending starting with vegetables, cereals or fruits. In addition, 54.6% recommend offering the child foods for chewing as soon as the child expresses interest, while 10.7% recommend delaying chewing until age 1 year.
As for the way in which new foods should be introduced, more than half of respondents (61.1%) recommended starting with spoon-feeding, 21.4% with bottle-feeding, and 17.4% not recommending any particular mode.
A large proportion of respondents (79.4%) knew of the approach to starting CF known as BLW, which they had become acquainted with by attending congresses or conferences or through mothers themselves, which were the most frequent sources of information (29.2% and 21.2%, respectively).
Of all respondents, 45.3% recommend BLW in some cases and 6.6% routinely, and up to 49.9% of physicians reported that at least one family in their caseloads was using the BLW approach at the time of the survey. The main reasons why they did not recommend this approach were lack of information (67.2%), the scarcity of scientific evidence (10.6%) and fear of children choking (10.6%), while only 5.2% reported having concerns that BLW may result in a low energy intake and 1.4% concerns that it may increase the risk of iron deficiency.
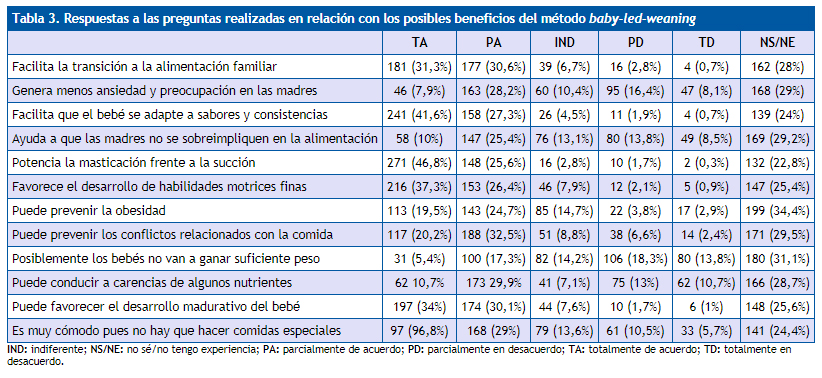
Between 20% and 35% of respondents did not have experience or a clear stance in relation to the questions asked about the potential benefits of BLW (Table 3).
| Table 3. Answers to items concerning the potential benefits of baby-led-weaning | ||||||
|---|---|---|---|---|---|---|
| TA | PA | IND | PD | TD | NK/NE | |
| It facilitates transition to family foods | 181 (31.3%) | 177 (30.6%) | 39 (6.7%) | 16 (2.8%) | 4 (0.7%) | 162 (28%) |
| Generates less anxiety and worry in mothers | 46 (7.9%) | 163 (28.2%) | 60 (10.4%) | 95 (16.4%) | 47 (8.1%) | 168 (29%) |
| Helps the baby get used to different flavours and textures | 241 (41.6%) | 158 (27.3%) | 26 (4.5%) | 11 (1.9%) | 4 (0.7%) | 139 (24%) |
| Helps mothers not become overinvolved in their child’s feeding | 58 (10%) | 147 (25.4%) | 76 (13.1%) | 80 (13.8%) | 49 (8.5%) | 169 (29.2%) |
| Promotes chewing over sucking | 271 (46.8%) | 148 (25.6%) | 16 (2.8%) | 10 (1.7%) | 2 (0.3%) | 132 (22.8%) |
| Promotes development of fine motor skills | 216 (37.3%) | 153 (26.4%) | 46 (7.9%) | 12 (2.1%) | 5 (0.9%) | 147 (25.4%) |
| May prevent obesity | 113 (19.5%) | 143 (24.7%) | 85 (14.7%) | 22 (3.8%) | 17 (2.9%) | 199 (34.4%) |
| May prevent food-related conflicts | 117 (20.2%) | 188 (32.5%) | 51 (8.8%) | 38 (6.6%) | 14 (2.4%) | 171 (29.5%) |
| Babies may not gain enough weight | 31 (5.4%) | 100 (17.3%) | 82 (14.2%) | 106 (18.3%) | 80 (13.8%) | 180 (31.1%) |
| May lead to nutritional deficiencies | 62 10.7% | 173 29.9% | 41 (7.1%) | 75 (13%) | 62 (10.7%) | 166 (28.7%) |
| May promote the growth and development of the baby | 197 (34%) | 174 (30.1%) | 44 (7.6%) | 10 (1.7%) | 6 (1%) | 148 (25.6%) |
| It is very convenient, as it does not require preparation of special foods | 97 (96.8%) | 168 (29%) | 79 (13.6%) | 61 (10.5%) | 33 (5.7%) | 141 (24.4%) |
DISCUSSION
The introduction of CF is considered a particularly important period in the nutrition of the child, as it involves significant changes in diet with exposure to new foods, flavours and textures that will culminate with assimilation into the dietary habits of the family. There is broad variability as to the timing and approach to its introduction due to the vagueness of the recommendations of scientific societies, the cultural diversity worldwide, and the scarcity of the scientific evidence on the subject.1,3,4
In recent years, the approach known as BLW has gained significant momentum. It proposes offering infants whole foods instead of pureed foods, cut in narrow and long shapes (“finger foods”) so that infants can grasp them and place them in their mouths.2 It is an approach to CF where the infant plays a more active role, for while the parents decide which foods to offer, it is the child that decides which of the offered foods to eat, in which amount, and at what pace. The timing of its introduction does not depend on the infant reaching a specific age as much as having developed certain skills, such as the ability to sit up unassisted, the coordinated use of hands to explore and manipulate objects, and the necessary oral motor skills to handle bits of food, that is, the ability to chew to break down soft foods and push them to the back of the mouth for subsequent swallowing. Giving infants a more active role in their own nutrition and having them know and partake of family foods as soon as possible is the underlying principle in this approach, which eliminates spoon-feeding by parents altogether or relegates it to a very small part of nutrition (< 10% of the total intake). In addition to the potential advantages highlighted by its proponents (more active participation of the child, improved satiety responsiveness and an easier transition to the consumption of solid textures), concerns have also been raised that it may increase the risk of choking and of nutritional deficiencies.5 In an attempt to mitigate potential nutritional imbalances, a modified version of the BLW known as Baby-Led Introduction to SolidS (BLISS) was proposed in 2015. This approach includes advice on how to ensure intake of high-energy foods and encourage the incorporation of iron-rich foods to the diet from an early stage, along with specific recommendations on the prevention of choking.6
In Spain, a high percentage of physicians (79.4%) are familiar with the BLW approach, and the most frequent source of information on this modality is attendance to courses or congresses and mothers themselves (29.2% and 21.2%, respectively). Few publications have echoed the growing popularity of this approach to CF in recent years. Brown and Lee7 found that out of 604 British mothers that participated in a survey about the approach to CF they were using with their babies, 58.1% practiced BLW, while Cameron8 found that out of 199 mothers surveyed in New Zealand, 29% reported using this approach, although only 8% were strict in its application. As for the attitudes of health care professionals, Cameron et al. found that of the 31 surveyed professionals, less than half had heard of this approach to CF, and that professionals felt they had limited knowledge on the details of this approach. The potential risk of choking was the greatest concern that prevented them from recommending BLW.9
Our survey is the first of its kind in Spain, and it shows that a large percentage of the physicians that responded (79.4%) knew what BLW was, and that 49.9% had families in their caseloads that were practicing this approach at the time of the survey. Although only 6.6% of paediatricians recommended BLW routinely as the best approach to CF, 45.3% reported recommending it in some cases, and lack of information was the main reason why they would not recommend it (67.2%), with a considerable lead over other reasons such as the scarcity of scientific evidence (10. 6%) or fear of the child developing complications like choking (10.6%), low energy intake (5.2%) or iron deficiency (1.4%).
One of the potential beneficial effects of BLW over the traditional approach to CF with pureed foods is that it hypothetically promotes acceptance of foods with a variety of textures and flavours, resulting in an increased intake of foods considered healthy, such as vegetables and non-processed foods. Most of the surveyed paediatricians (68.9%) agreed with this claim despite the scarcity of the evidence published to date. The most comprehensive study that has attempted to assess this assumption is the one published by Townsend.10 In this study, 155 parents of children aged 20 to 78 months filled out a questionnaire that explored their approach to weaning and subsequent nutrition-related outcomes. Ninety-two respondents reported having used a BLW approach compared to 63 that used a traditional approach with spoon-feeding of puréed foods, and while the spoon-fed group later liked sweet foods most, the BLW group developed a preference for carbohydrates, even though there had been no difference in the exposure to these foods between the two groups. This finding suggests that we ought to consider not only the frequency of exposure to foods, but also their texture and appearance, which are important factors in promoting the development of specific preferences.
One of the goals of BLW is for children to feed on demand, refraining from ever forcing them to eat, thus giving them the opportunity to regulate on their own the amounts of food they consume and to develop a sense of satiety, as has been proposed for breastfeeding on demand. Only one third of the surveyed paediatricians agreed totally or partially that BLW is associated with decreased anxiety in mothers, who would theoretically have a more relaxed approach to their children’s nutrition, while half of the paediatricians believed that BLW may help prevent conflicts regarding food (52.7%) and obesity (44.2%). Although maternal attitudes have in fact been associated with long-term nutritional outcomes in children, few studies have addressed the potential impact of specific approaches to the introduction of CF. The studies conducted by Brown and Lee7,11 showed that mothers that adopted the BLW approach were less likely to pressure their children to eat and limit consumption of specific foods compared to mothers that adopted a traditional CF approach, and that at age 18-24 months, children of the former had greater control of their appetite (less interest in food in the absence of hunger and a greater ability to self-regulate intake based on satiety). Furthermore, while few children had a body mass index (BMI) above the 85th percentile, the proportion of these children was higher in the group fed with purees. Townsend10 found similar results in comparing the nutritional status of 92 children that had been weaned with the BLW approach and 63 weaned with the traditional CF approach. While most of the children had an adequate BMI, children in the BLW group had lower BMIs, a difference that could not be attributed to differences in birth weight, parental BMI or socioeconomic status, while the proportion of children with a BMI above the 85th percentile was higher in the group of children that had been fed purées. Still, the interpretation of the results of both studies may be limited by potential biases, such as the weight of children being reported by the mothers, and the fact that the mothers that chose the BLW method tended to have a higher educational attainment, breastfeed longer, and return to work later, all of them factors that may affect the growth of the child.
The results of a prospective trial whose main purpose was to determine whether a modified BLW approach (the BLISS method) led to differences in BMI z-score at 12 and 24 months compared to introduction of CF with pureed foods have been published recently. This study also assessed potential differences in energy intake and eating behaviours between both groups.12 At one year of age, of the 166 children in the sample (78 in the traditional CF group and 88 in the BLISS group), children that had been weaned with the modified BLW approach were less fussy eaters and enjoyed food more, but contrary to previous data, they were less responsive to satiety at age 2 years. There were no statistically significant differences in total energy intake or BMI z-score, although more children in the BLISS group had a BMI above the 85th percentile at age 24 months (10.3%) compared to the control group (6.4%). The authors concluded that the BLISS method provides adequate nutrition for growth and is associated with different eating behaviours in children weaned with the approach, but not with a lower risk of overweight at age 2 years.
In addition to concerns regarding the ability of infants to consume enough calories with the BLW method, there are concerns regarding potential inadequacies in the intake of certain nutrients. Thus, 40.6% of the paediatricians surveyed in our study believed that BLW may lead to nutritional deficiencies, although it is worth noting that only 5.2% and 1.4% identified low energy intake and the risk of iron deficiency, respectively, as concerns that prevented them from recommending this approach to the introduction of complementary foods.
Two studies published recently tried to clarify these issues. Morison et al.13 compared the intake of macronutrients and micronutrients in a small sample of infants aged 6 to 8 months and found no statistically significant differences in total energy intake. However, they found that children in the BLW group tended to consume more fats (48% versus 42% of the total energy intake, P < .001), especially saturated fat (22% versus 18% of energy, P < .001), as well as substantial differences in the intake of micronutrients, with lower intakes of iron (1.6 versus 3.6 mg, P < .001), zinc (3.0 versus 3.7 mg, P = .001) and vitamin B12 (0.2 versus 0.5 μg, P < .001) in infants in the BLW group compared to infants in the traditional CF group.
On the other hand, in an initial pilot study in 10 infants aged 6 months to assess the effectiveness of the BLISS approach in increasing iron intake, Daniels et al. found that the intake of iron-rich foods was double in the 5 infants in the BLISS group compared to the 5 infants in the traditional BLW group. Later, in the analysis of a larger sample, 15 they found no statistically significant differences between children in the BLISS group and children in the traditional CF group in total energy intake, consumption of nutrients at age 7 months, iron intake, serum concentration of ferritin or prevalence of anaemia. They also found no differences in the consumption of fruits, vegetables or cereals, and infants in both groups consumed 10% of their total energy in the form of proteins, 45% in the form of fats and 45% in the form of carbohydrates.
In recent years, there seems to be an increasing number of parents that experience difficulties with the transition from milk or formula feeding to CF, which leads to delays in the introduction of non-puréed foods. In many instances, this is due to a fear that the child will not eat enough or to misinterpretation of the difficulties that children may experience when handling pieces of whole foods. While 54.6% of the surveyed paediatricians recommended giving the child foods to chew as soon as the child expresses interest in them, 10.7% recommended delaying chewing until age 1 year, even though it is believed that there is a critical window for the introduction of non-pureed foods and that failure to introduce them during this period may lead to greater difficulties introducing new textures and developing chewing skills. This window occurs at around 7 to 9 months of age, the period when the BLW approach is most dynamic and involved. This is one of the aspects that physicians considered most beneficial in BLW, as 63.7% of them believed that the manipulation of foods by the infant in this approach facilitates the development of motor skills, and 72.4% that BLW promotes chewing over sucking. In addition to perceiving these benefits, respondents also feared the potential risk of choking, which was the main reason why 10.6% of them did not recommend BLW.
The assessment of this risk was the main aim of the study conducted by Fangupo et al.16 They assessed the frequency of choking in 206 infants (101 with traditional introduction of CF and 105 with introduction by the BLISS method) through a questionnaire administered at ages 6, 7, 8, 9 and 12 months, and assessed the exposure to foods considered choking hazards at 7 and 12 months through a 3-day diet record. While 35% of infants experienced at least one episode of choking between 6 and 8 months of age, there were no significant differences between the two groups at any of the ages under study. Infants in the BLISS group experienced nausea more frequently at 6 months compared to the traditional CF group, but they experienced it less frequently than infants in the traditional CF group at age 8 months, which could reflect that infants in whom CF are introduced by the BLISS approach learn how to handle foods with a solid consistency earlier without a significant increase in the risk of choking.
A salient finding of the study was that despite performance of frequent check-up visits during which parents were informed of the hazardous foods that should be avoided and how to act in the event of choking, half of the parents had offered at least one of these foods to their children by age 7 months, a proportion that increased to 94% by age 12 months, with no significant differences between both groups.
CONCLUSIONS
We found considerable variability between the surveyed paediatricians in their recommendations regarding CF. The most common approach continues to be spoon- or even bottle-feeding of pureed foods. An increasing number of paediatricians are aware of the BWL approach, but few feel prepared enough to recommend it routinely. Paediatricians need to learn more about this approach, its basis, benefits and risks to be better prepared to recommend BWL or a different approach to CF. For this to happen, more evidence is required on the safety and risks of this method and the impact it may have on child growth and development.
Paediatricians use different handouts with recommendations for CF, which may be confusing to parents. Thus, a single handout with evidence-based recommendations on CF should be created for use in all primary care paediatrics settings.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS
AEPap: Asociación Española de Pediatría de Atención Primaria • BLISS: baby-led introduction to solids • BLW: baby-led-weaning • BMI: body mass index •CF: complementary foods • MIR: Medical Intern.
ACKNOWLEDGMENTS
We thank all the colleagues that have collaborated by participating in the survey.
REFERENCES
- Fewtrell M, Bronsky J, Campoy C, Domellöf M, Embleton N, et al. Complementary feeding: a position paper by the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) Committee on Nutrition. J Pediatr Gastroenterol Nutr. 2017;64:119-32.
- Cameron SL, Heath AM, Taylor RW. How feasible is baby-led weaning as an approach to infant feeding? A review of the evidence. Nutrients. 2012;4:1575-609.
- Shiess S, Grote V, Scaglioni S, Luque V, Martin F, Stolarczyk A, et al. Introduction of complementary feeding in 5 european countries. J Pediatr Gastroenterol Nutr. 2010;50:92-8.
- Alvisi P, Brusa S, Alboresi S, Amarri S, Bottau P, et al. Recommendations on complementary feeding for healthy, full term infants. Italian J Pediatr. 2015;41:36.
- Brown A, Jones SW, Rowan H. Baby-led weaning: the evidence to date. Curr Nutr Rep. 2017;6:148-56.
- Cameron SL, Taylor RW, Heath A-LM. Development and pilot testing of Baby-Led Introduction to SolidS (BLISS) - a version of baby-led weaning modified to address concerns about iron deficiency, growth faltering and choking. BMC Pediatr. 2015;15:99.
- Brown A, Lee M. Maternal control of child feeding during the weaning period: differences between mothers following a baby-led or standard weaning approach. Matern Child Nutr. 2011;15:1265-71.
- Cameron SL, Taylor RW, Heath A-LM. Parent-led or baby-led? Associations between complementary feeding practices and health-related behaviours in a survey of New Zealand families. BMJ Open. 2013;3:e003946.
- Cameron SL, Heath A-LM, Taylor RW. Healthcare professionals’ and mothers’ knowledge of attitudes to and experiences with baby-led weaning: a content analysis study. BMJ Open. 2012;2:e001542.
- Townsend E, Pitchford NJ. Baby knows best? The impact of weaning style on food preferences and body mass index in early childhood in a case controlled sample. BMJ Open. 2012;2:e000298.
- Brown A, Lee MD. Early influences on child satiety-responsiveness: the role of weaning style. Pediatr Obes. 2013;10:57-66.
- Taylor RW, Williams SM, Fangupo LJ, Wheeler BJ, Taylor BJ, Daniels L, et al. Effect of a baby-led approach to complementary feeding on infant growth and overweight. A randomized clinical trial. JAMA Pediatr. 2017;171:838-46.
- Morison BJ, Taylor RW, Haszard JJ, SchrammCJ, Erickson LW, Fangupo LJ, et al. How different are baby-led weaning and conventional complementary feeding? A cross-sectional study of infants aged 6-8 months. BMJ Open. 2016;6:e010665.
- Daniels L, Heath A-LM, Williams SM, Cameron SL, Fleming EA, et al. Baby-Led Introduction to SolidS (BLISS) study: a randomised controlled trial of a baby-led approach to complementary feeding. BMC Pediatr. 2015;15:179.
- Daniels L, Taylor RW, Williams SM, Fleming LA, Wheeler BJ, et al. Impact of a baby-led approach to complementary feeding on iron status at 12 months of age: a randomised controlled trial. EAPS Congress 2016: October 21-25, 2016. Eur J Pediatr. 2016;175:1393-880.
- Fangupo LJ, Heath AM, Williams SM, Williams LWE, Morison BJ, Fleming EA, et al. A baby-led approach to eating solids and risk of choking. Pediatrics. 2016;138:e20160772.