
Vol. 20 - Num. 77
Original Papers
Prevalence of overweight and obesity in immigrant adolescents
aPediatra. Servicios de Pediatría y Adolescencia. Instituto Aragonés de Servicios Sociales. Gobierno de Aragón. Zaragoza. España.
Correspondence: G Oliván. E-mail: golivang@aragon.es
Reference of this article: Oliván Gonzalvo G. Prevalence of overweight and obesity in immigrant adolescents. Rev Pediatr Aten Primaria. 2018;20:27-32.
Published in Internet: 29-11-2017 - Visits: 24091
Abstract
Introduction: few studies conducted in Spain have analysed the influence of ethnicity in the prevalence of overweight and obesity in adolescents. Our aim was to assess the prevalence of overweight and obesity in first-generation immigrant adolescents in Aragon, compared our results to those of the HBSC-2014 study for Spain, and discuss potential aetiological factors.
Materials and methods: cross-sectional study in 274 immigrant adolescents (11-17 years) from Latin America (n = 160) and Eastern Europe (n = 114). To assess overweight and obesity, we calculated the body mass index an applied the cut-off points proposed by the International Obesity Task Force. We used two-tailed z- and t-tests for comparisons, defining statistical significance as a p-value of less than 0.05.
Results: we found overweight or obesity in 27.5% of immigrant adolescents from Latin America (18.8% and 8.7%, respectively) and 14.9% of those from Eastern Europe (12.3% and 2.6%, respectively). In Latin American adolescents, the prevalence of obesity was significantly higher (P = .03846), as was the prevalence of overweight and obesity combined (P = .01352), mostly on account of male adolescents (P = .04036). The comparison with the HBSC-2014 study in Spain showed a higher prevalence of obesity in Latin American immigrant adolescents that was statistically significant (P = .00228).
Conclusions: the prevalence of overweight and obesity in first-generation immigrant adolescents from Latin America was significantly higher than that observed in autochthonous Spanish adolescents and Caucasian first-generation immigrant adolescents. We believe that genetic, socio-economic, cultural and behavioural factors are involved in the aetiology of obesity and overweight. This population is at high risk of developing metabolic syndrome and cardiovascular disease in adulthood.
Keywords
● Adolescent ● Emigrants and Immigrants ● Obesity ● OverweightINTRODUCTION
The prevalence of overweight and obesity has been increasing in the paediatric age group.1,2. In Spain, few studies have analysed the role of ethnicity in the prevalence of overweight and obesity in children and adolescents.3-7 The Ministry of Health, Social Services and Equality recently published a study conducted between March and December 2014 analysing the prevalence of overweight and obesity in immigrant adolescents aged 11 to 18 years in Spain (Health Behaviour in School-aged Children [HBSC] 2014, Spain).8
The aim of our study was to analyse the prevalence of overweight and obesity in first-generation adolescent immigrants from Latin America and Eastern Europe residing in Aragon, search for differences between both groups of adolescent immigrants, compare our results with those of the HBSC-2014 study in Spain8 and consider the aetiology of these conditions.
MATERIALS AND METHODS
We conducted a cross-sectional epidemiological observational study in a sample 274 first-generation immigrant adolescents aged 11-17 years from Latin America and Eastern Europe residing in Aragon. Most of the Latin American immigrant adolescents (n = 160) were from Ecuador (22.5%), Colombia (21.9%), Dominican Republic (18.1%) and Brazil (15%). The remaining 22.5% were from Venezuela, Peru, Honduras, Cuba, Nicaragua, Argentina, Paraguay, Bolivia, Panama and Chile. Most of the Eastern European immigrant adolescents (n = 114) were from Romania (81.6%). The remaining 18.4% were from Bulgaria, Moldavia, Russia, Poland and Czech Republic.
We collected data on the weight and height recorded during medical checkups in a social paediatrics clinic in the 2014-2016 period. Recorded weights corresponded to the mean of two measurements performed with a digital seca 799 scale accurate to 100 g, and recorded heights to the mean of two measurements made with a measuring rod attached to the digital scale accurate to 1 mm taken with the adolescent standing straight. All measurements were taken by the same individual. We assessed overweight and obesity by means of the body mass index (BMI) (weight/height2), whose value we interpreted using the cut-off points for age and sex established by Cole9 and recommended by the International Obesity Task Force (IOTF).
We entered the values for the variables under study in an Excel® spreadsheet, which we used to calculate means and standard deviations (SDs). We compared group proportions by means of the two-tailed z-test and defined statistical significance as a p-value of less than 0.05. We used the two-tailed t-test to compare the means of independent groups, with statistical significance defined as p < 0.05.
RESULTS
Table 1 presents and compares the values of demographic and anthropometric variables in the sample of first-generation immigrant adolescents from Latin America and Eastern Europe residing in Aragon. In the Latin American immigrant group, 27.5% of adolescents had overweight or obesity (18.8% and 8.7%, respectively), and we found no differences between the sexes (1:1). In the Eastern European immigrant group, 14.9% had overweight or obesity (12.3% and 2.6%, respectively), and the prevalence was greater in female adolescents (1:1.5). When we compared both ethnic groups, we found a significantly greater prevalence of obesity (P = .03846) and overweight and obesity combined (P = .01352) in Latin American adolescents, mainly on account of male adolescents (P = 0.04036).
| Table 1. Prevalence of overweight and obesity in first-generation immigrant adolescents in Aragon (Spain): comparison of adolescents from Eastern Europe versus Latin America | ||||||
|---|---|---|---|---|---|---|
| Variables | Eastern Europe | Latin America | ||||
| Male | Female | Total | Male | Female | Total | |
| Sex (n [%]) | 44 (38.6) | 70 (61.4) | 114 | 69 (43.1) | 91 (56.9) | 160 |
| Age (years; mean [SD]) | 14.6 (2.4) | 15.4 (2.1) | 15 (2.3) | 14.8 (2.2) | 15.2 (1.7) | 15 (1.9) |
| Weight (kg; mean [SD]) | 53 (13.6) | 51.9 (9.4) | 52 (11.4) | 57.8 (16.1) | 54.1 (10.8) | 55.7 (13.4) |
| Height (cm; media (DE)] | 162.5 (12.2) | 157.2 (6.4) | 158.8 (9.9) | 161.9 (12.7) | 155.1 (7) | 158 (10) |
| BMI (kg/m2; mean [SD]) | 19.8 (3.3) | 21 (3.2) | 20.5 (3.3) | 21.8 (4.8) | 22.4 (3.6) | 22.1 (4.1) |
| Overweight (IOFT cutoff; n [%]) | 4 (9.1) | 10 (14.3) | 14 (12.3) | 12 (17.4) | 18 (19.8) | 30 (18.8) |
| Obesity (IOFT cutoff; n [%]) | 1 (2.3) | 2 (2.9) | 3 (2.6) | 7 (10.1) | 7 (7.7) | 14 (8.7)* |
| Overweight + obesity (n [%]) | 5 (11.4) | 12 (17.1) | 17 (14.9) | 19 (27.5)* | 25 (27.5) | 44 (27.5)* |
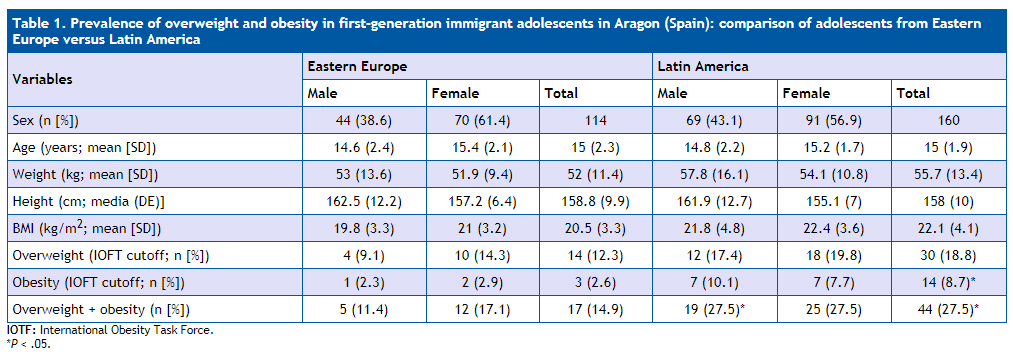
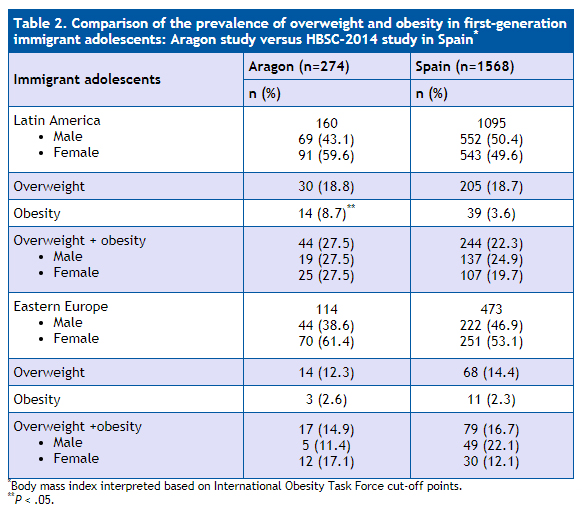
Table 2 compares the prevalence of overweight and obesity in this sample of first-generation immigrant adolescents from Latin America and Southern Europe with the prevalence found in the Spanish sample of the HBSC-2014 study.8 We found a significantly higher prevalence of obesity (P = .00228) and a higher prevalence of overweight and obesity combined—although this difference was not statistically significant—in the Latin American adolescents in our study in Aragon. We did not find statistically significant differences in the prevalence of overweight and obesity between the Eastern European adolescent immigrants of either study.
| Table 2. Comparison of the prevalence of overweight and obesity in first-generation immigrant adolescents: Aragon study versus HBSC-2014 study in Spain* |
||
|---|---|---|
| Immigrant adolescents | Aragon (n=274) | Spain (n=1568) |
| n (%) | n (%) | |
Latin America
|
160 69 (43.1) 91 (59.6) |
1095 552 (50.4) 543 (49.6) |
| Overweight | 30 (18.8) | 205 (18.7) |
| Obesity | 14 (8.7)** | 39 (3.6) |
Overweight + obesity
|
44 (27.5) 19 (27.5) 25 (27.5) |
244 (22.3) 137 (24.9) 107 (19.7) |
Eastern Europe
|
114 44 (38.6) 70 (61.4) |
473 222 (46.9) 251 (53.1) |
| Overweight | 14 (12.3) | 68 (14.4) |
| Obesity | 3 (2.6) | 11 (2.3) |
Overweight +obesity
|
17 (14.9) 5 (11.4) 12 (17.1) |
79 (16.7) 49 (22.1) 30 (12.1) |
DISCUSSION
The prevalence of overweight and obesity in first-generation immigrant adolescents from Latin America and Eastern Europe residing in Aragon was very similar to the prevalence found in the HBSC-2014 study in Spain.8 The results obtained in both studies show that 22.9% of immigrant adolescents from Latin America have overweight or obesity (18.7% and 4.2%, respectively), with a higher prevalence in males; and that 16.4% of immigrant adolescents from Eastern Europe have overweight or obesity (14% and 2.4%, respectively). The HBSC-2014 study in Spain8 also assessed the prevalence of overweight and obesity in 19 425 autochthonous Spanish children, and estimated it at 16.9% overall (14.5% for overweight and 2.4% for obesity). Based on these data, it is fair to conclude that the prevalence of overweight and obesity in first-generation immigrant adolescents from Eastern Europe is similar to that in adolescents of Spanish origin. Conversely, the prevalence of overweight and obesity in first-generation immigrant adolescents from Latin America is 6% greater than the prevalence in autochthonous Spanish and Eastern European immigrant adolescents. In the United States, a study conducted by the National Health and Nutrition Survey (NHANES) conducted between 2001-200610, and 2007-200811 found similar results, with a higher prevalence of overweight and obesity in adolescents of Latin American origin aged 12-13 years, more frequent in males, compared to non-Hispanic black and white adolescents.
At the individual level, overweight and obesity have an undeniable genetic component. However, genetic predisposition cannot account for the differences in their prevalence within and between populations. Many modifiable factors play a role in the development of overweight and obesity in adolescents. Chief among them are cultural, environmental and socioeconomic factors (low maternal educational attainment, migration, poverty, accelerated urbanization etc) that promote a positive energy balance. Several studies have demonstrated that children of immigrants or families of low socioeconomic status are at higher risk of developing overweight and obesity compared to other children.7,12-14 There are also behavioural factors associated with higher energy intakes (greater consumption of sugary drinks and sandwiches, larger food portions, parental dietary habits that promote overeating, etc) and lower levels of physical activity. Ethnicity is associated with differences in food-related beliefs, preferences and behaviours, and cultural factors can contribute to increase the risk of obesity in children and adolescents of ethnic minorities. Furthermore, the diet of individuals in low-income populations is frequently high in calories and fat, while vegetables, fruits and whole grains, which tend to be pricier, are usually consumed in smaller amounts.4,12,15,16 Lastly, there are developmental factors mainly related to early nutrition (maternal obesity during gestation, gestational diabetes, low birth weight, absence or short duration of breastfeeding, etc).13,16
More specifically, there is evidence of a higher prevalence of risk factors associated with the development of overweight and obesity in Latin American children and adolescents compared to their Caucasian peers. Chief among these risk factors are the consumption of sugary drinks and fast food, sedentary lifestyles, the presence of a television set in the bedroom, maternal depression, maternal obesity at the beginning of pregnancy, greater maternal weight increase during pregnancy with a higher incidence of gestational diabetes, rapid weight gain in the first months of life, a lower prevalence of breastfeeding and the early introduction of solid foods.16 The HBSC-2014 study in Spain8 analysed the lifestyle habits and family characteristics of autochthonous versus immigrant adolescents. The study found that adolescents from Latin America were less likely to have breakfast, eat appropriate amounts of fruit or engage in physical activity and most likely to have sedentary habits, while their families had lower incomes. In our study in Aragon we did not analyse the lifestyle habits of immigrant adolescents, but we did find that most of them belonged to low-income families.
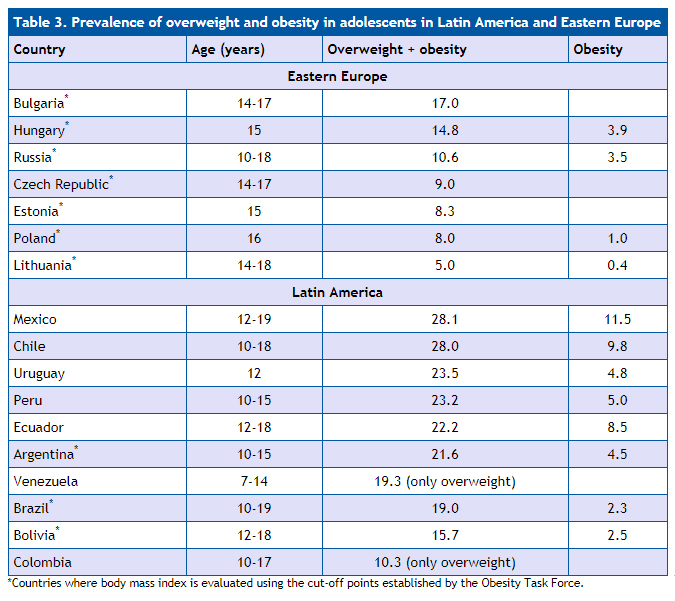
Table 3 shows the prevalence of overweight and obesity in adolescents in different countries in Latin America and Eastern Europe.17 We can see that in all Latin American countries the prevalence of overweight and obesity is high, and considerably higher compared to Eastern European countries. These data suggest that genetic predisposition may be a key factor in Latin American immigrant adolescents. In regard to potential genetic factors, we ought to highlight the “thrifty genotype” hypothesis proposed by Neel,18 according to which certain polymorphisms in genes encoding proteins involved in lipid and carbohydrate metabolism would have undergone natural selection over many generations. These polymorphisms would have been an advantage for survival under conditions of scarcity, as they allowed a more efficient use of food through insulin resistance and fat accumulation, but when environmental conditions improved, this thriftiness was rendered detrimental, a situation that is more evident in certain populations, including Latin American youth.19-21
| Table 3. Prevalence of overweight and obesity in adolescents in Latin America and Eastern Europe | |||
|---|---|---|---|
| Country | Age (years) | Overweight + obesity | Obesity |
| Eastern Europe | |||
| Bulgaria* | 14-17 | 17.0 | |
| Hungary* | 15 | 14.8 | 3.9 |
| Russia* | 10-18 | 10.6 | 3.5 |
| Czech Republic* | 14-17 | 9.0 | |
| Estonia* | 15 | 8.3 | |
| Poland* | 16 | 8.0 | 1.0 |
| Lithuania* | 14-18 | 5.0 | 0.4 |
| Latin America | |||
| Mexico | 12-19 | 28.1 | 11.5 |
| Chile | 10-18 | 28.0 | 9.8 |
| Uruguay | 12 | 23.5 | 4.8 |
| Peru | 10-15 | 23.2 | 5.0 |
| Ecuador | 12-18 | 22.2 | 8.5 |
| Argentina* | 10-15 | 21.6 | 4.5 |
| Venezuela | 7-14 | 19.3 (only overweight) | |
| Brazil* | 10-19 | 19.0 | 2.3 |
| Bolivia* | 12-18 | 15.7 | 2.5 |
| Colombia | 10-17 | 10.3 (only overweight) | |
In conclusion, the epidemiological studies conducted in Spain show that the prevalence of overweight and obesity in first-generation immigrant adolescents from Latin America is significantly higher compared to that of autochthonous Spanish children and first-generation immigrant children of Caucasian origin. There are also studies in the literature that show that in Spain, the frequency of metabolic syndrome in obese children and adolescents of Latin American origin is greater compared to obese Caucasian children, and that Latin American children exhibit poorer adherence to dietary and physical activity treatment strategies. This is associated with an increased risk of future cardiovascular disease in these patients
CONFLICTS OF INTEREST
The author has no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS
BMI: body mass index • IOTF: International Obesity Task Force • SD: standard deviation.
REFERENCES
- Wang Y, Lobstein T. Worldwide trends in childhood overweight and obesity. Int J Pediatr Obes. 2006;1:11-25.
- De Onis M, Blössner M, Borghi E. Global prevalence and trends of overweight and obesity among preschool children. Am J Clin Nutr. 2010;92:1257-64.
- Díez López I, Rodríguez Estévez A. Resultados de una intervención nutricional en población infantil con obesidad: diferencias entre la población inmigrante y la española. Rev Esp Obes. 2008;6:280-5.
- González García G, Rodríguez Martínez G, Romero Noreña A, Fuertes Fernández-Espinar J, Lorente Aznar T, Álvarez Sauras MT, et al. Influencia de la etnia y el sexo en la ingesta de alimentos como factores de riesgo de malnutrición en escolares. Acta Pediatr Esp. 2009;67:493-7.
- Bibiloni MM, Martínez E, Llull R, Juarez MD, Pons A, Tur JA. Prevalence and risk factors for obesity in Balearic Islands adolescents. Br J Nutr. 2010;103:99-106.
- Enes Romero P, Cano Gutiérrez B, Álvarez Gil N, Martín-Frías M, Alonso Blanco M, Barrio Castellanos R. Influencia étnica en la prevalencia de síndrome metabólico en población pediátrica obesa. An Pediatr (Barc). 2013;78:75-80.
- Esteban-Gonzalo L, Veiga OL, Regidor E, Martínez D, Marcos A, Calle ME. Immigrant status, acculturation and risk of overweight and obesity in adolescents living in Madrid (Spain): the AFINOS study. J Immigr Minor Health. 2015;17:367-74.
- Moreno C, Jiménez-Iglesias A, Sánchez-Queija I, Ramos P, Rivera F, García-Moya I, et al. Adolescentes inmigrantes en España: análisis de sus estilos de vida, salud, ajuste psicológico y relaciones en sus contextos de desarrollo. Resultados del Estudio HBSC-2014 en España. Madrid: Ministerio de Sanidad, Servicios Sociales e Igualdad; 2016.
- Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000;320:1240-3.
- Johnson WD, Kroon JJ, Greenway FL, Bouchard C, Ryan D, Katzmarzyk PT. Prevalence of risk factors for metabolic syndrome in adolescents: National Health and Nutrition Examination Survey (NHANES), 2001-2006. Arch Pediatr Adolesc Med. 2009;163:371-7.
- Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in US children and adolescents, 2007-2008. JAMA. 2010;303:242-9.
- Freedman DS, Khan LK, Serdula MK, Ogden CL, Dietz WH. Racial and ethnic differences in secular trends for childhood BMI, weight, and height. Obesity (Silver Spring). 2006;14:301-8.
- Moreno LA, Pigeot I, Ahrens W. Childhood obesity: etiology - synthesis part II. Etiological factors. In: Moreno LA, Pigeot I, Ahrens W (eds.). Epidemiology of obesity in children and adolescents. Prevalence and etiology. New York: Springer; 2011. p. 483-92.
- Wang Y, Lim H. The global childhood obesity epidemic and the association between socio-economic status and childhood obesity. Int Rev Psychiatry. 2012;24:176-88.
- Cheikh Moussa K, Sanz-Valero J, Wanden-Berghe C. The social determinants of health of the child-adolescent immigration and its influence on the nutritional status: systematic review. Nutr Hosp. 2014;30:1008-19.
- Albala C, Corvalan C. Epidemiology of Obesity in Children in South America. In: Moreno LA, Pigeot I, Ahrens W (eds.). Epidemiology of obesity in children and adolescents. Prevalence and etiology. New York: Springer; 2011. p. 95-110.
- Ahrens W, Moreno LA, Pigeot I. Childhood obesity: prevalence worldwide - synthesis part I. Descriptive Epidemiology. In: Moreno LA, Pigeot I, Ahrens W (eds.). Epidemiology of obesity in children and adolescents. Prevalence and etiology. New York: Springer; 2011. p. 219-38.
- Neel JV. Diabetes mellitus: a thrifty genotype rendered detrimental by progress. Am J Hum Genet. 1962;14:353-62.
- Goran MI, Walker R, Le KA, Mahurkar S, Vikman S, Davis JN, et al. Effects of PNPLA3 on liver fat and metabolic profile in Hispanic children and adolescents. Diabetes. 2010;59:3127-30.
- Casazza K, Willig AL, Gower BA, Nagy TR, Hunter GR, Wallace S, et al. The role of European genetic admixture in the etiology of the insulin resistance syndrome in children: are the effects mediated by fat accumulation. J Pediatr. 2010;157:50-6.
- Butte NF, Comuzzie AG, Cole SA, Mehta NR, Cai G, Tejero M, et al. Quantitative genetic analysis of the metabolic syndrome in Hispanic children. Pediatr Res. 2005;58:1243-8.