
Vol. 20 - Num. 77
Original Papers
Review of the diagnosis and clinical features of Kawasaki disease: retrospective descriptive and analytical study
Beatriz Baleato Gómeza, Carmen González Ávilaa, Borja Souto Cainzosa, Beatriz Iglesias Gonzáleza, Cristina González Menchéna, José Tomás Ramos Amadora
aServicio de Pediatría. Hospital Clínico Universitario San Carlos. Madrid. España.
Correspondence: B Baleato. E-mail: bea_0019@hotmail.com
Reference of this article: Baleato Gómez B, González Ávila C, Souto Cainzos B, Iglesias González B, González Menchén C, Ramos Amador JT. Review of the diagnosis and clinical features of Kawasaki disease: retrospective descriptive and analytical study. Rev Pediatr Aten Primaria. 2018;20:15-24.
Published in Internet: 02-11-2017 - Visits: 26812
Abstract
Introduction: Kawasaki disease is an acute, febrile and self-limiting vasculitis that may be complicated by cardiovascular changes. Its diagnosis is based on clinical criteria. Although effective treatment is available, it is the leading cause of acquired heart disease in children in developed countries. Objectives: to assess the prevalence of coronary artery abnormalities in paediatric patients diagnosed in our area, and the demographic, clinical and laboratory characteristics of the population under study, describing the risk factors for coronary involvement in children with Kawasaki disease.
Methods: we performed a retrospective review of the medical records of children given a diagnosis of Kawasaki disease between January 1997 and December 2016 at the Hospital Clínico San Carlos (Madrid, Spain). We defined Kawasaki disease as the presence of the clinical criteria proposed for its diagnosis by the American Academy of Pediatrics in 2017.
Results: cases of Kawasaki disease were most frequent in the winter (n = 13; 56.5%), in girls (n = 12; 52.2%) and in children aged 5 years or less (n = 18; 78.3%). Patients presented with fever (n = 23; 100%) and changes in the oropharyngeal mucosa (n = 21; 91.3%), with elevation of C-reactive protein and the erythrocyte sedimentation rate (n = 20; 86.95% and n = 13; 86.6%). Treatment consisted of intravenous immunoglobulin (n = 22; 95.7%) and acetylsalicylic acid at anti-inflammatory doses (n = 22; 95.7%) or antithrombotic doses (n = 20; 87%). Three patients (13%) developed coronary artery abnormalities that eventually resolved.
Conclusions: in our cohort, the prevalence of coronary complications was similar to the prevalence reported for Spain and higher than the prevalence reported in international studies. The main risk factors for coronary artery abnormalities were delays in diagnosis or treatment, a white blood cell count greater than 12 000 cells/µl, a serum level of C-reactive protein greater than 3 mg/dl and thrombocytosis.
Keywords
● Coronary disease ● Mucocutaneous lymph node syndrome ● Risk factorsINTRODUCTION
Kawasaki disease (KD), previously known as mucocutaneous lymph node syndrome, is an acute febrile vasculitis involving small- to medium-sized vessels. It was first described in 1967 by Tomisaku Kawasaki.1 Although it is a self-limiting process occurring mainly in children, it can give rise to coronary complications associated with a significant morbidity and mortality. Thus, it is the leading cause of acquired heart disease in children in developed countries.2
Its incidence is higher in individuals of Asian descent3,4 (estimated incidence of 30.3/100 000 children aged less than 5 years) and males (1.5:1).5,6 It is less frequent in infants aged less than 6 months or children aged more than 5 years, and is usually diagnosed late, when there is a higher risk of coronary artery abnormalities (CAAs).
Although this disease has been known for 50 years, its aetiology remains unknown.4,7 It seems to involve genetic susceptibility (Asian ethnicity and positive family history), immunologic factors (it was initially hypothesised that it involved an immune response triggered by a superantigen, although recent studies have proposed a cascade response induced by a conventional antigen)6,8 and infectious factors (higher incidence in the winter, with a potential association with infection by viruses or bacteria such as parvovirus B19, retrovirus, Epstein-Barr virus, human herpesvirus, Chlamydia pneumoniae or Mycoplasma as well as staphylococcal or streptococcal toxic shock syndrome). For all of the above, it is believed that the pathophysiology of KW involves an abnormal and stereotyped immune response in a genetically susceptible host to one of a variety of infectious agents or environmental factors.4,9
Kawasaki disease is characterised by a systemic inflammation of medium-sized arteries and multiple organs and tissues during the acute phase. Its clinical presentation varies depending on the involved systems: gastrointestinal tract (abdominal pain, vomiting, diarrhoea, hepatitis, pancreatitis), lung (interstitial pneumonitis), meninges (aseptic meningitis, irritability), heart (coronary artery disease, myocarditis, pericarditis, valvulopathy), urinary tract (sterile pyuria), musculoskeletal system (arthritis, arthralgia) and lymph nodes (lymphadenopathy).4,6,10 The course of KD unfolds in three phases: a necrotising arteritis that is self-limiting (first two weeks), followed by subacute or chronic vasculitis, which in a small percentage of cases can last months or years with progression to luminal myofibroblastic proliferation.6,11
The diagnosis of KD is based on clinical criteria1,6,12 and requires fever of at least 5 days’ duration associated with 4 or more of the following: polymorphous rash, changes in distal extremities (redness and swelling in hands or feet, desquamation of periungual region starting 2 weeks after onset), changes in the oral mucosa (strawberry tongue, fissuring, erythema, dryness), bilateral non-exudative conjunctival injection or cervical lymphadenopathy at least 1.5 cm in diameter (usually unilateral). In the presence of 4 or more clinical criteria (especially redness and swelling of the hands and feet), the diagnosis of KD can be made with only 4 days of fever. These inflammatory manifestations may develop sequentially. Complete or classic KD is diagnosed in patients that meet the case definition, and incomplete KD in patients with prolonged fever and fewer than 4 clinical criteria with compatible echocardiographic or laboratory findings.6
A high degree of suspicion is required in the presence of fever associated with any of the diagnostic clinical criteria, given the nonspecificity of the main signs and symptoms of KD. Due to the absence of a specific diagnostic test, the diagnosis of KD requires ruling out other diseases with a similar presentation.6
Laboratory tests typically reveal a normal or elevated white blood cell count with neutrophil predominance, elevated acute phase reactants (C-reactive protein [CRP] and erythrocyte sedimentation rate [ESR]), normocytic normochromic anaemia, sterile pyuria, low serum sodium and albumin levels, elevated serum liver enzymes, and thrombocytosis.6 Although nonspecific, laboratory findings support the diagnosis, and are of particular importance in the diagnosis of incomplete KD.
The most significant complications in terms of severity are those involving pathological changes in the coronary arteries. These include aneurysms, dilation, impaired vasodilation, narrowing of the arterial lumen, decreased myocardial contractility, mild heart valve regurgitation and pericardial effusion, with coronary aneurisms being the most frequent sequelae of KD. Approximately 25% of patients that do not receive early treatment with high-dose intravenous immunoglobulin (IVIG) develop cardiovascular complications, an incidence that dropped to 4% with the introduction of IVIG.2 Recent studies suggest that a much higher proportion of children with KD experience subtle and often transient changes in the coronary arteries.13 The risk factors associated with the development of CAAs are not well established, although the literature has described associations with delayed diagnosis and late initiation IVIG therapy, age less than 1 year or greater than 9 years, male sex, prolonged fever, failure of initial IVIG therapy and laboratory findings suggestive of severe and persistent inflammation.14-18
The incidence of CAAs is higher in patients with incomplete KD, a finding that has been associated with greater delays in diagnosis and treatment, as the disease may go unnoticed in these patients.18
The treatment recommended for the acute phase is combined therapy with IVIG and acetylsalicylic acid (ASA) after the diagnosis is confirmed, and preferably initiated before 10 days from onset.6,19
Immunoglobulin is administered intravenously at a dose of 2 g/kg as a single infusion delivered over 10 to 12 hours. Although its mechanism of action is unknown, it appears to have a systemic anti-inflammatory effect and is considered the best treatment for the prevention of CAAs.6,19
During the acute phase, it is recommended that ASA be given at anti-inflammatory doses of 30 to 100 mg/kg/day, divided in four doses. When the patient has been afebrile for 48 to 72 hours, it is lowered to an antithrombotic dose of 3 to 5 mg/kg for 6 to 8 weeks if the patient does not have coronary involvement.20
Adjuvant treatment with corticosteroids can be considered in patients at high risk of developing CAAs. 6,21
The approach to cases refractory to initial treatment (10%-20% of the total), defined as those that do not respond by 36 hours from completion of the IVIG infusion, remains controversial.6,22 A second dose of IVIG is recommended, and treatment with corticosteroids (as an alternative to IVIG or combined with it) or infliximab may be considered. Alternative treatments may be considered for patients resistant to these drugs, such as cyclosporine or immunomodulatory monoclonal antibody therapy.6,22,23
The outcome of KD depends on the development of CAAs. In Japan, KD recurs in approximately 3% of cases; recurrence is more frequent in the first two years from the initial episode and is associated with a higher risk of coronary sequelae. The mortality is estimated at approximately 0.015% due to coronary sequelae, with a peak between 15 to 45 days after the onset of fever, and cases of sudden death occurring during the long-term followup.6
Hypothesis: the prevalence of CAAs in our patients is similar to the one reported in the literature. The risk factors for development of CAAs described in paediatric patients with a KD diagnosis will be the same in our sample.
Objectives: to analyse the prevalence of CAAs in paediatric patients diagnosed with KD in our region, describe the risk factors for CAAs in children with KD and assess the clinical, laboratory and demographic characteristics of the population under study.
MATERIALS AND METHODS
Study design
We conducted a retrospective observational analytical epidemiological study. The sample consisted of children included in the catchment area of the Hospital Clínico San Carlos (HCSC) in Madrid, Spain, that received a diagnosis of KD between January 1, 1997 and December 31, 2016.
Inclusion criteria: patients aged 0 to 18 years with a diagnosis of KD made in the period specified above. Exclusion criteria: patients with insufficient data (lack of data on the clinical criteria, laboratory tests or heart imaging tests used for diagnosis) or patients that received a working diagnosis of KD that was subsequently ruled out.
Ethical aspects
We retrieved data on test results and different variables from the electronic health records of patients after obtaining the approval and an exemption from informed consent from the Research Ethics Committee of the HCSC.
Methods
We conducted a retrospective review of the health records of children that received a diagnosis of KD between January 1997 and December 2016 at the HCSC. We entered different epidemiologic, laboratory, treatment response and cardiovascular complication variables in a multipurpose form. The variables included in the study concerned the epidemiology of KD (age at diagnosis, sex, season, and length of hospital stays), its clinical presentation (fever, polymorphous rash, changes in distal extremities, cervical lymphadenopathy, changes in oral mucosa and conjunctival injection), laboratory findings (anaemia, leukocytosis with neutrophilia, thrombocytosis, elevated CRP, elevated ESR, elevated transaminases, hypoalbuminaemia, sterile pyuria and results of blood culture), response to treatment (duration of fever, use of ASA and IVIG), and cardiovascular complications (echocardiographic abnormalities, date of diagnosis and resolution).
We collected the data used for the statistical analysis from chart notes, discharge reports and reports of echocardiographic and laboratory test findings.
We defined KD based on the presence of the clinical criteria proposed by the American Academy of Pediatrics in 2017, according to which complete or classic KD is defined as at least 4 days of fever with 4 or more clinical criteria, and incomplete KD as at least 5 days of fever combined with 2 or 3 clinical criteria and echocardiographic or laboratory findings that support the diagnosis (CRP ≥ 3 mg/dl or ESR ≥ 40 mm/h accompanied by ≥ 3 additional criteria: albumin < 3 g/dl, anaemia, high serum level of alanine aminotransferase, thrombocytosis after 7 days with ≥ 450 000/μl, white blood cells ≥ 12 000/μl or sterile pyuria). We defined KD refractory to IVIG as fever persisting more than 36 hours after completion of IVIG infusion.
The patients that received a KD diagnosis were admitted to the paediatric ward if fewer than 10 days had elapsed since onset, or if more than 10 days had elapsed but the patient remained febrile, had abnormal laboratory findings with elevation of acute phase reactants or had abnormal echocardiographic findings. Patients admitted to hospital were treated with IVIG administered as a single dose of 2g/kg or in 5 doses of 400 mg/kg, and ASA at a dose of 80-100 mg/kg/day until the patient had been afebrile for at least 48 hours, followed by ASA at a maintenance dose of 3 to 5 mg/kg/day given once daily for 4 to 8 weeks if the patient had no CAAs. Patients were assessed by means of echocardiography, laboratory tests and electrocardiography at the time of diagnosis. After discharge, patients were followed up in the cardiology clinic, including echocardiographic assessments at 4 and 8 weeks post discharge, and thereafter depending on the presence or absence of CAAs.
Statistical analysis
In the statistical analysis, we summarised qualitative variables as frequency distributions and percentages. We summarised quantitative variables using the mean and standard deviation if they were normally distributed, and otherwise the median and interquartile range. We performed the statistical analysis with the software SPSS® Statistics version 23 (IBM).
RESULTS
A total of 25 patients received a diagnosis of KD between 1997 and 2016. Data concerning the diagnosis was missing in one patient, and KD ruled out in another after development of bilateral tonsillar exudate that responded well to oral antibiotherapy, so these two patients were excluded from the study. Of the total patients in the sample (n = 23), 20 (87%) had a diagnosis of classic KD and 3 (13%) of incomplete KD. The median age at diagnosis in our sample was 2.8 years (range, 1.4-5.0).
When it came to sex, 11 were male (47.8%) and 12 female (52.2%). Cases were diagnosed most frequently in winter, in 13 patients (56,5%), followed by summer, in 5 patients (21.7%). The mean length of stay of the patients was 6 days (range, 4.0-12.0).
Clinical criteria
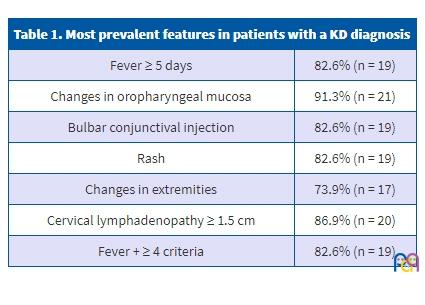
Our analysis of the clinical criteria showed that 20 patients (86.9%) presented with fever of 5 or more days’ duration. Cervical lymphadenopathies larger than 1.5 cm in diameter were found on palpation in 20 patients (86.9%). Nineteen patients had a polymorphous rash (82.6%). There were changes in the distal extremities in 17 patients (73.9%) and in the oral mucosa in 21 (91.3%). Lastly, 19 patients (82.6%) presented with bilateral non-exudative conjunctival injection. The patients presented with a mean of 4.17 ± 0.95 criteria, with a maximum of 5 criteria in 8 patients (34.7%) (Table 1).
| Table 1. Most prevalent features in patients with a KD diagnosis | |
|---|---|
| Fever ≥ 5 days | 82.6% (n = 19) |
| Changes in oropharyngeal mucosa | 91.3% (n = 21) |
| Bulbar conjunctival injection | 82.6% (n = 19) |
| Rash | 82.6% (n = 19) |
| Changes in extremities | 73.9% (n = 17) |
| Cervical lymphadenopathy ≥ 1.5 cm | 86.9% (n = 20) |
| Fever + ≥ 4 criteria | 82.6% (n = 19) |
Laboratory criteria
The results of our analysis of the data on laboratory testing were the following: 11 patients (47.8%) had leukocytosis with neutrophilia and 13 patients (59.1%) leukocytosis with more than 12 000 cells/mm3. As for changes in platelet counts, 9 patients (42.9%) had thrombocytosis, 2 (9.5%) thrombocytopenia and 10 (47.6%) counts within the normal range. Serum levels of CRP were elevated (> 3 mg/dl) in 20 patients (86.95%). The ESR was measured in 15 patients, and elevated values were found in 13 of them (86.6%). Haemoglobin levels were also recorded, with detection of anaemia in 10 patients (43.5%). Only 4 patients had sterile pyuria (18.2%). Blood cultures were performed in 10 patients and were negative in all. We also analysed the serum albumin level, which was only documented in 6 patients, and was low in half (n = 3) and within the normal range in the other half (n = 3), as well as serum transaminase levels, which were elevated in 11 patients (57.9%) and normal in 8 (42.1%).
Treatment
Of all patients in the study (n = 23), 22 (95.7%) received IVIG therapy. One patient was not treated with IVIG due to a late diagnosis (> 10 days), with normal laboratory and echocardiographic findings at the time of assessment in the emergency department. This patient received a diagnosis of classic KD and was only treated with ASA at an antithrombotic dose (3-5 mg/kg/day).
The dose administered to the patient was documented in 19 of them, of who 17 (89.5%) received a single 2 g/kg dose of IVIG, while the remaining 2 (10.5%) received 5 doses of 400 mg/kg, a low-dose scheme that been abandoned since 2004. The time elapsed from the onset of fever to initiation of IVIG therapy was 7 days (5.0-9.0), with a delay of more than 10 days in 3 of the patients.
As for treatment with ASA, 22 patients (95.7%) received it at anti-inflammatory doses (80-100 mg/kg/day), initiated 0 to 2 days from admission. The duration of treatment with ASA was only documented in 15 patients, in whom treatment lasted 2.5 to 4.0 days. On the other hand, 20 patients (87%) received ASA at antithrombotic doses (3-5 mg/kg/day), of who 1 had not previously received it at an anti-inflammatory dose. None of the patients received clopidogrel.
The response to IVIG therapy was documented in 20 patients, of who 6 (30%) had refractory KD. Five patients (22.7%) received a second IVIG dose, of who 3 had refractory KD based on the study definition.
Coronary artery abnormalities
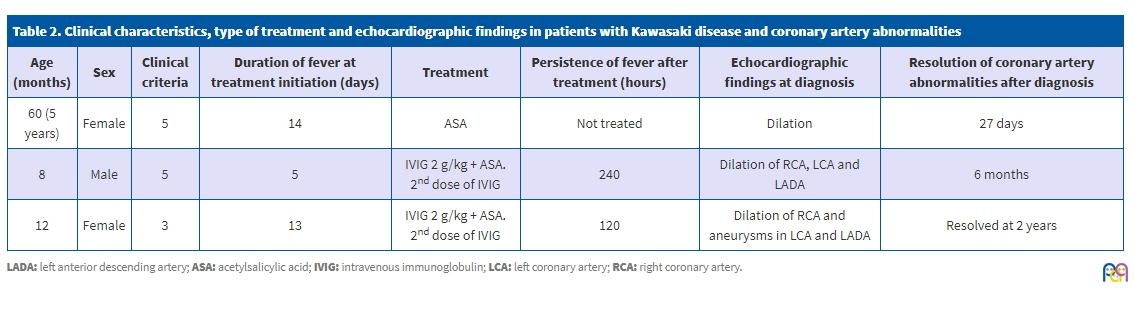
Of the 23 patients in the sample, 3 developed CAAs (13%): one, coronary artery dilation (patient A), another aneurysm (patient B) and the last one dilation and aneurysms (patient C).
Patient A was a girl aged 5 years who received a diagnosis of classic KD during the winter. Patient B was a boy aged 8 months who received a diagnosis of classic KD in the winter. Lastly, patient C was a girl aged 12 months who received a diagnosis of incomplete KD in the winter.
The laboratory abnormalities found in patient A were leukocytosis with a left shift (white blood cells 25 300/μl with 68.3% neutrophils), thrombocytosis (714 000/μl), sterile pyuria (25 white blood cells per high-power field) and elevation of CRP (11.6 mg/dl) and ESR (116 mg/dl). Patient B had leukocytosis (14 460/μl), elevation of CRP (8.3 mg/dl) and ESR, thrombocytosis (992 000/μl), anaemia (12,6 g/dl), a negative blood culture and hypoalbuminaemia. Patient C presented with leukocytosis with neutrophilia (19 600/μl with 57.7% neutrophils), thrombocytosis (527 000/μl), elevated CRP (10.8 mg/dl), anaemia (10.7 g/dl), sterile pyuria, hypoalbuminaemia and mild elevation of liver transaminases.
When it came to treatment, patient A did not receive IVIG, but was treated with ASA alone at an antithrombotic dose for 3 months. Patient B was treated with a 2g/kg dose of IVIG 5 days after the onset of fever and ASA at an anti-inflammatory dose for 23 days and then at an anti-thrombotic dose for 6.5 months. His fever persisted 240 hours after initiation of treatment, so he needed an additional dose of IVIG. Last of all, patient C was treated with a 2 g/kg dose of IVIG 13 days after the onset of fever and ASA at an anti-inflammatory dose for 3 days and at an anti-thrombotic dose for 36 months. The patient continued to have fever 120 hours after initiation of treatment, so she required retreatment with IVIG.
As for the echocardiographic findings, patient A received a diagnosis of coronary artery dilation from the third follow-up echocardiographic assessment performed 1 month and 25 days after diagnosis of KD, following normal first and second follow-up assessments 13 and 32 days after diagnosis, respectively. The fourth follow-up examination, performed 27 days after detection of the abnormality, revealed that it had resolved. In patient B, the second follow-up echocardiographic examination 17 days after the diagnosis of KD detected aneurysms, after a normal initial follow-up examination 2 days after diagnosis. The abnormality had resolved by the fourth follow-up examination, performed 6 months and 20 days after detection of the aneurysms. Patient C received a diagnosis of KD, dilation and aneurysms on the day of admission. We did not find data on the followup of CAAs in this patient, save for one follow-up assessment 2 years later that found no abnormalities in the coronary arteries (Table 2).
| Table 2. Clinical characteristics, type of treatment and echocardiographic findings in patients with Kawasaki disease and coronary artery abnormalities | |||||||
|---|---|---|---|---|---|---|---|
| Age (months) | Sex | Clinical criteria | Duration of fever at treatment initiation (days) | Treatment | Persistence of fever after treatment (hours) | Echocardiographic findings at diagnosis | Resolution of coronary artery abnormalities after diagnosis |
| 60 (5 years) | Female | 5 | 14 | ASA | Not treated | Dilation | 27 days |
| 8 | Male | 5 | 5 | IVIG 2 g/kg + ASA. 2nd dose of IVIG | 240 | Dilation of RCA, LCA and LADA | 6 months |
| 12 | Female | 3 | 13 | IVIG 2 g/kg + ASA. 2nd dose of IVIG | 120 | Dilation of RCA and aneurysms in LCA and LADA | Resolved at 2 years |
There were also 2 patients with other cardiovascular complications: a girl aged 12 years with a diagnosis of incomplete KD in whom the first echocardiographic examination performed 2 days after diagnosis revealed mild ventricular dysfunction, which resolved by 16 days of followup, and lastly 1 boy aged 20 months with incomplete KD in whom the first follow-up examination 2 days after diagnosis revealed mild pericardial effusion at the level of the right atrium and ventricle, which had resolved at 1 month.
DISCUSSION
Kawasaki disease is an acute, self-limiting, febrile systemic vasculitis of unknown aetiology.7 In Spain, its incidence is of 15.1 per 100 000 children aged 5 or more years,24 somewhat lower to that reported in the United States, estimated at 25 cases per 100 000 children aged 5 or more years.5
To date, there are no known pathognomonic clinical findings or specific diagnostic tests for KD, so the diagnosis is based on a series of clinical criteria6 that are also of limited usefulness, as they are not completely sensitive.25 Based on these criteria, patients may receive a diagnosis of complete or incomplete KD.
The patients with KD included in our sample had demographic, clinical and laboratory characteristics consistent with previous descriptions in the medical literature.
Most of the cases were diagnosed in children aged less than 5 years (78.3%; n = 18), during winter or summer (78.3%; n = 18). These data were similar to those found by other case series, such as the one published by Prieto Tato et al.,26 where the case distribution by sex was 11 male (47.8%) and 12 female (52.2%). Since the remaining demographic characteristics of our sample were consistent with the literature, we believe that the predominance of the female sex found in our study could be due to our sample being too small for the assessment of a dichotomous variable with a very small margin of difference (1.5 male: 1 female).5
In our patients, KD manifested with fever (100%; n = 23) accompanied by changes in the oropharyngeal mucosa (91.3%, n = 21), bilateral non-exudative conjunctival injection (86.9%, n = 20), cervical lymphadenopathy on palpation (86.9%, n = 20) and polymorphous rash (82.6%; n = 19), while changes in distal extremities were the least prevalent feature in our sample (73.9%, n = 17). The clinical presentation was similar in the patients analysed by Prieto Tato,26 with a predominance of fever and oropharyngeal involvement (100%) and extremity involvement being the least frequent manifestation (67%).26 This is also consistent with the sample described by Kawasaki,27 who reported fever with a temperature greater than 38 °C lasting more than 6 days as the most frequent presenting symptom (100%, n = 50), followed by bilateral non-exudative conjunctival injection (98%, n = 49) and changes in the oral mucosa (96%, n = 48), with changes in the extremities being once again the least frequent manifestation (44%, n = 22).27 We believe that a high correlation in clinical features is to be expected in a disease whose diagnosis is based on the presence of such manifestations.
At present, abnormal blood test results are not among the criteria used to diagnose KD, but they are suggestive of the disease and used to support the diagnosis of KD. The most frequent abnormalities found in our study were elevation of CRP levels and the ESR (86.95% and 86.6%, respectively), the parameters that are considered most suggestive of KD by the American Heart Association (AHA).6 Other relevant abnormalities include leukocytosis, neutrophilia, thrombocytosis, anaemia and elevation of liver transaminases, which were found in approximately half of our sample. This was consistent with the findings of other studies conducted in Spain.28,29
Coronary artery abnormalities constitute the most frequent cardiovascular complication in KD, with a prevalence of 25% that drops to approximately 4% in patients treated with a single dose of IVIG. In most cases, they are dilations that resolve within 4 to 8 weeks, but some patients develop large aneurysms that pose a risk of myocardial infarction and sudden death.6
In the sample under study, 3 patients (13%) developed CAAs, but only 2 were treated with IVIG. Based on these data, 9% of the total patients treated with IVIG developed CAAs, an incidence that in any case was above the one described by the AHA.6 However, our data were similar to those of the studies by Caballero-Mora28 and Prieto,26 which reported a prevalence of CAAs in Spain of 15.7% and 13%, respectively. All of our 3 patients experienced echocardiographic resolution, which was also consistent with those studies.
Although the prognosis of KD is good, its outcome depends on the development of CAAs. For this reason, numerous studies have analysed the association between clinical or laboratory features and the development of CAAs, which may be useful for the identification of patients at high risk of CAAs.
Although numerous studies have been published in the medical literature, there is no overall consensus. The following associated factors have been described: male sex, age < 12-24 months and > 9 years, delayed diagnosis and treatment (> 10 days since onset of fever without IVIG therapy), refractory disease, prolonged fever, CRP elevation, white blood cell count > 12 000/mm3, thrombocytosis, hypoalbuminaemia and anaemia.13-18,26,28,30
The study by Beiser et al.14 found a correlation between development of CAAs and male sex, as CAAs were found in 8.3% of female patients compared to 17% of male patients. The study by Caballero-Mora et al.28 that analysed possible risk factors in Spain found statistically significant differences for male sex, elevated CRP levels and anaemia. In our sample, the 3 patients that developed CAAs had CRP levels greater than 8 mg/dl, with a mean level of 10.23 mg/dl, while the mean level found in patients without CAAs and elevated CRP levels was 8.1 mg/dl. In addition, 2 of these 3 patients had anaemia. However, only one of them was male.
As for age, the results of the study by Honkanen et al.15 showed echocardiographic changes in 10 out of the 14 patients that received a diagnosis of KD before age 1 year. Of the 5 patients with echocardiographic abnormalities in our sample, 3 were aged less than 12 months and 1 more than 9 years.
The study published by Maric17 identified leukocytosis, thrombocytosis and hypoalbuminaemia as risk factors, which was consistent with the findings in the patients that developed CAAs in our study.
Berdej-Szczot18 analysed 73 patients with cases diagnosed between 2003 and 2016, and concluded that the independent risk factors were prolonged duration of fever, refractory disease, delayed diagnosis, mild presentation and thrombocytosis. In our sample, we found that 2 of the patients with CAAs received the diagnosis and initial treatment more than 10 days after the onset of fever, on days 13 and 14, specifically, of who 1 did not respond to treatment. The third such patient continued to have fever for 10 more days despite early diagnosis and treatment, and was therefore also nonresponsive to IVIG.
Limitations
This study is limited by its retrospective design and the small sample size, which reduced the power of the statistical analysis. Furthermore, it includes cases diagnosed over the course of 20 years, which means that the management of the disease was heterogeneous and may have been a source of bias. Further studies with larger samples are required to improve our knowledge of this disease in Spain.
CONCLUSIONS
In our cohort, the prevalence of CAAs was similar to the one reported in Spain and higher than the prevalence described in international studies.
The risk factors for CAAs found in our patients were similar to those described in the medical literature, as they mainly occurred in patients with delayed diagnosis and treatment, a white blood cell count greater than >12 000 cells/µl, a CRP level of less than 3 mg/dl and thrombocytosis.
In our region, KD cases occurred most frequently during the winter, in girls and in children aged 5 years or fewer, and presented with fever, changes in the oropharyngeal mucosa and elevation of CRP and the ESR.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS
ASA: acetylsalicylic acid • AHA: American Heart Association • CAA: coronary artery abnormality • CRP: C-reactive protein • ESR: erythrocyte sedimentation rate • IVIG: intravenous immunoglobulin • KD: Kawasaki disease.
REFERENCES
- Kawasaki T. Acute febrile mucocutaneous syndrome with lymphoid involvement with specific desquamation of the fingers and toes in children. Arerugi. 1967;16:178-222.
- Rowley AH, Shulman ST. Kawasaki syndrome. Pediatr Cardiol. 1999;46:313-29.
- Kao AS, Getis A, Brodine S, Burns JC. Spatial and temporal clustering of Kawasaki syndrome cases. Pediatr Infect Dis J. 2008;27:981.
- Sundel R. Kawasaki disease: epidemiology and etiology. In: UpToDate [online] [accessed 27/10/2017]. Available at www.uptodate.com/contents/kawasaki-disease-epidemiology-and-etiology
- Holman RC, Belay ED, Christensen KY, Folkema AM, Steiner CA, Schonberger LB. Hospitalizations for Kawasaki syndrome among children in the United States, 1997-2007. Pediatr Infect Dis J. 2010;29:483-8.
- McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, et al. Diagnosis, treatment and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation. 2017;135:927-99.
- Takahashi K, Oharaseki T, Yokouchi Y. Pathogenesis of Kawasaki disease. Clin Exp Immunol. 2011;164:20-22.
- Matsubara T, Ichiyama T, Furukawa S. Immunological profile of peripheral blood lymphocytes and monocytes/macrophages in Kawasaki disease. Clin Exp Immunol. 2005;141:381-7.
- Burgner D, Harnden A. Kawasaki disease: what is the epidemiology telling us about the etiology? Int J Infect Dis. 2005;9:185-94.
- Amano S, Hazama F, Kubagawa H, Tasaka K, Haebara H, Hamashima Y. General pathology of Kawasaki disease: on the morphological alterations corresponding to the clinical manifestations. Acta Pathol Jpn. 1980;30:681-94.
- Orenstein JM, Shulman ST, Fox LM, Baker SC, Takahashi M, Bhatti TR, et al. Three linked vasculopathic processes characterize Kawasaki disease: a light and transmission electronmicroscopic study. PloS One. 2012;7:e38998.
- Council on Cardiovascular Disease in the Young; Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease; American Heart Association. Diagnostic guidelines for Kawasaki disease. Circulation. 2001;103:335-6.
- Sundel R, Klein-Gitelman M, Kaplan S, TePas E. Kawasaki disease: complications. In: UpToDate [online] [accessed 27/10/2017]. Available at www.uptodate.com/contents/kawasaki-disease-complications
- Beiser AS, Takahashi M, Baker AL, Sundel RP, Newburger JW, US Multicenter Kawasaki Disease Study Group. A predictive instrument for coronary artery aneurysms in Kawasaki disease. Am J Cardiol. 1998;81:1116-20.
- Honkanen VE, McCrindle BW, Laxer RM, Feldman BM, Schneider R, Silverma ED. Clinical relevance of the risk factors for coronary artery inflammation in Kawasaki disease. Pediatr Cardiol. 2003;24:122-6.
- Koren G, Lavi S, Rose V, Rowe R. Kawasaki disease: review of risk factors for coronary aneurysms. J Pediatr. 1986;108:388-92.
- Maric LS, Knezovic I, Papic N, Mise B, Roglic S, Markovinovic L, et al. Risk factors for coronary artery abnormalities in children with Kawasaki disease: a 10‑year experience. Rheumatol Int. 2015;35:1053-8.
- Berdej-Szczot E, Małecka-Tendera E, Gawlik T, Firek-Pędras M, Szydłowski L, Gawlik A. Risk factors of immunoglobulin resistance and coronary complications in children with Kawasaki disease. Kardiol Pol. 2017;75:261-6.
- Shulman ST. Intravenous immunoglobulin for the treatment of Kawasaki disease. Pediatr Ann. 2017;46:e25-e28.
- Sundel R. Kawasaki disease: initial treatment and prognosis. In: UpToDate [online] [accessed 27/10/2017]. Available at www.uptodate.com/contents/kawasaki-disease-initial-treatment-and-prognosis
- Chen S, Dong Y, Yin Y, Krucoff MW. Intravenous immunoglobulin plus corticosteroid to prevent coronary artery abnormalities in Kawasaki disease: a meta-analysis. Heart. 2013;99:76-82.
- Campbell AJ, Burns JC. Adjunctive therapies for Kawasaki disease. J Infect. 2016;72:1-5.
- Kimura M, Harazaki M, Fukuoka T, Asakura I, Sakai H, Kamimaki T, et al. Targeted use of prednisolone with the second IVIG dose for refractory Kawasaki disease. Pediatr Int. 2017;59:397-403.
- Martínez Ruiz M, del Castillo Martín F, Borque Andrés C, García Miguel MJ, de José Gómez MI, Martínez Cortés F, et al. Incidencia y características clínicas de la enfermedad de Kawasaki. An Pediatr (Barc). 2003;59:323-7.
- Witt MT, Minich LL, Bohnsack JF, Young PC. Kawasaki disease: more patients are being diagnosed who do not meet American Heart Association criteria. Pediatrics. 1999;104:10.
- Prieto Tato LM, Cuesta Rubio MT, Guillén Martín S, Ruiz Jiménez M, Cortés Coto MT, Rubio Gribble B, et al. Enfermedad de Kawasaki: diagnóstico y tratamiento. An Pediatr (Barc). 2010;73:25-30.
- Kawasaki T. Pediatric acute febrile mucocutaneous lymph node syndrome with characteristic desquamation of fingers and toes: my clinical observation of fifty cases. Pediatr Infect Dis J. 2002;21:1-38.
- Caballero-Mora FJ, Alonso-Martín B, Tamariz-Martel-Moreno A, Cano-Fernández J, Sánchez-Bayle M. Enfermedad de Kawasaki en 76 pacientes. Factores de riesgo de aparición de aneurismas coronarios. An Pediatr (Barc). 2011;74:232-8.
- González Pascual E, Villanueva Lamas J, Ros Viladoms J, Pons Odena M, Ruiz García-Diego S. Enfermedad de Kawasaki. Presentación de cincuenta casos. An Pediatr Esp. 1999;50(1):39-43.
- Galeotti C, Kaveri SV, Cimaz R, Koné-Paut I, Bayry J. Predisposing factors, pathogenesis and therapeutic intervention of Kawasaki disease. Drug Discov Today. 2016;21:1850-7.