
Vol. 19 - Num. 75
Original Papers
Factors associated with overweight and obesity in high school students
Juana Aurelia Ninatanta Ortiza, Luz Amparo Núñez Zambranoa, Segunda Aydeé García Floresa, Romaní Romaní Romaníb
aEnfermera. Facultad Ciencias de la Salud. Universidad Nacional de Cajamarca. Perú.
bMédico. Oficina General de Investigación y Transferencia Tecnológica. Instituto Nacional de Salud. Perú.
Reference of this article: Ninatanta Ortiz JA, Núñez Zambrano LA, García Flores SA, Romaní Romaní F. Factors associated with overweight and obesity in high school students. Rev Pediatr Aten Primaria. 2017;19:209-21.
Published in Internet: 11-09-2017 - Visits: 28943
Abstract
Objective: to identify the associated factors to overweight and obesity in students of high school of an Andean region of northern of Peru.
Methods: a cross sectional study was performed in a sample of 586 students, residing in two districts of Cajamarca region. We performed the anthropometric evaluation using the standards of child growth of the World Health Organization (using the score z of the body mass index). We applied a structured survey for recollect data of lifestyles, food consumption, physical activity, depressive symptoms questionnaire, bullying and weight perception. We performed a logistic regression was performed to identify associated characteristics.
Results: the proportion of overweight and obesity was 22.9% and 6.8% of adolescents, respectively. Belonging to public schools was a protective factor for overweight (adjusted OR: 0.62, CI 95%: 0.39 to 0.99) regardless of gender, physical activity and depressive symptoms. Male gender (adjusted OR 2.05, 95% CI: 1.02 to 4.11) and low physical activity (adjusted OR: 4.14, 95% CI: 1.65 to 10.35) were risk factors for obesity, while belonging to public schools was a protective factor (adjusted OR 0.43, 95% CI: 0.20 to 0.92).
Conclusions: the level of physical activity is the main factor associated with obesity; on the other hand, public school students have less chance of overweight and obesity. Schools represent environments to implement preventive interventions of overweight and obesity based on increased physical activity.
Keywords
● Adolescent ● Obesity ● Overweight ● StudentsINTRODUCTION
Obesity is a growing health problem worldwide; it is estimated that in 2025 it will affect 18% of men and 21% of women.1 Excess weight in adolescents is also a public health problem.2 In Latin America, the prevalences of overweight and obesity vary between countries; in Mexico, 40.9% of adolescents had overweight and 22.9% obesity (2002)3; in Brazil, 25.7% to 28.8% had overweight and 10.4% to 15.4% obesity;4 and in Argentina (2014) 26.4% of adolescents were found to have overweight and 14.1% obesity.5 In children and adolescents in the United States (2013-2014), the prevalence of overweight was 33.4% and the prevalence of obesity 26.1%.6
In Peru, the prevalence of excess weight in adolescents has been increasing; according to the Instituto Nacional de Salud (National Institute on Health [INS]), overweight in adolescents aged 10 to 19 years grew from 15.8% (2011) to 18.5% (2014), while obesity increased from 4.6% to 7.5%. Excess weight is not distributed uniformly: in urban areas, the prevalence of overweight doubles compared to rural areas, while the prevalence of obesity is sevenfold.7 There are districts with a high prevalence of excess weight, most of which are located along the Peruvian coastline.8 In 2014, in the northern Andes region, the prevalences of overweight and obesity were 16.1% and 2.1%, respectively, and they were on the increase, as in 2011 overweight affected 9.3% and obesity 1.8% of adolescents in this region.7 The identification of modifiable risk factors could explain this trend in Andean regions. In 2015, the population of adolescents (12 to 17 years) in the region of Cajamarca had reached 184 167 inhabitants, and this was the Andean region in Peru with the largest adolescent population.9 In this region, excess weight starts and progresses in childhood: in 2014, the prevalences of overweight and obesity in children aged less than 5 years were 5.3% and 1.5%, respectively,8 while the range in adolescents rose to 10%-20%.10
Cross-sectional studies in secondary education students from different regions in Peru have found prevalences of excess weight ranging between 6.8% and 33.7%, depending on sex and geographical area.7-12 There are also studies that have investigated the characteristics associated with overweight and obesity; a literature review found that associated factors in adolescents (aged 10 to 19 years) included lower educational attainment of the head of household, poverty, female sex and residing in an urban area.10 Another study of schoolchildren aged 6 to 17 years found that living in the coast and low cardiorespiratory fitness were associated characteristics.13 In 2007, a study in primary school students in the Lima metropolitan area and Callao found that the percentage of overweight was greater in private compared to public school students (21.6% versus 10.3%).14 At the international level, there is evidence that excess weight may be explained by risk factors unrelated to physical fitness and dietary habits; other studies have found an association with symptoms of depression,15,16 school bullying17-19 and body image perception.20,21
Reducing the prevalence of overweight and obesity in children and adolescents could reduce the extent of obesity and its complications in subsequent stages of life. The probability of obese children of being obese as adults is five times that of children who are not obese.2 There is also evidence of a strong association between a history of obesity in adolescence and increased mortality due to coronary disease and stroke in adulthood.22 In light of the above, reducing excess weight in adolescence would contribute to reducing obesity and its complications in adulthood. Our study aimed to determine the proportion of overweight and obesity in a sample of secondary school students residing in an Andean region of Peru, and to identify associated modifiable risk factors with the ultimate purpose of aiding the implementation of health promotion strategies in educational facilities in urban areas in the Andes.
MATERIALS AND METHODS
Study design and population
The region of Cajamarca is located in the northern Andes in Peru. The study was carried out in the districts of Chota and Cajamarca. Cajamarca is located in the homonymous province and has a population of 246 536 inhabitants (2015 estimate), while Chota has 48 698 inhabitants (2015) (Series Nacionales INEI).
The sample comprised 586 students enrolled in the first and second year of secondary education in four schools of the urban areas of the districts selected for participation in the study “Estudio prevalencia de síndrome metabólico en estudiantes de secundaria, universitarios y madres residentes de una región andina del Perú.”23 This study was conducted between June and October 2014. The sample size of the original study was calculated assuming a prevalence of metabolic syndrome of 19.1% for a 95% confidence level and a relative margin of error of 15%.
Outcome measurement
- Anthropometric evaluation. We defined overweight and obesity based on the 2007 World Health Organization (WHO) growth standards for children aged more than 5 years. We made the classification based on the body mass index (BMI) z-score (zBMI) adjusted for age, using a macro for SPSS® developed by the WHO (who.int/childgrowth/software/es/). Overweight was defined as a zBMI > +1 and ≤ +2, and obesity as a zBMI > +2.24
- We used a structured questionnaire to collect data on unhealthy habits: having ever smoked (Yes/No), having ever consumed alcoholic beverages (Yes/No). Dietary habits were explored based on how frequently the following foods were consumed each week (number of days/week): carbonated drinks, snacks, water, fruit, vegetables, dairy (milk/yoghourt), eggs, chicken meat, red meat, fish and cold meats. We categorised the intake of fruit and vegetables as adequate if participants reported consuming them four to seven days a week (Yes/No); water intake was considered adequate for four to eight glasses a day (Yes/No). Physical activity was measured by means of the short version of the International Physical Activity Questionnaire (IPAQ), whose criteria were used to define low, moderate and high levels of activity; these categories were regrouped into low and moderate/high for the bivariate and multivariate analyses.25 We defined optimal rest as sleeping seven to eight hours a night (Yes/No).
- Symptoms of depression. We used the Zung self-rating depression scale adapted for adolescents,26 and categorised the resulting scores into normal (score ˂ 50), mild (50-59), moderate (60-69) and severe depression (≥ 70). These categories were modified to normal, mild depression and moderate/severe depression for the bivariate and multivariate analyses.
- To identify cases of school victimization and bullying, we presented 14 different situations, following the methodology of the Comisión Nacional para el Desarrollo y Vida sin Drogas (National Committee for Drug-Free Development and Life [DEVIDA])27. These situations were the following:
- Someone threatened you with a weapon, hit you, hid your things, broke your things or stole your things were classified as forms of physical violence
- The following situations were considered verbal violence: someone insulted you, called you names or gave you a nickname, or spoke ill of you.
- The following were considered situations of social exclusion: you were ignored/they did not pay attention to you, they did not let you participate, someone discriminated against you.
- Mixed forms included: someone threatened you to intimidate others, someone blackmailed you/forced you to do things you did not want to do, and someone sexually harassed you.
- To identify cases of bullying, we formulated the question: “Since you started secondary school, have you done or participated in any of the following?” for the 14 presented situations. The answers for each situation were Yes/No. A Yes scored 1 point and a No 0 points. We considered participants with scores of 3 or higher victims or bullies.
- Body image perception. We posed the question: “For your age, do you consider your weight to be…?” The categories proposed were low, normal, and excessive.
Data collection
We used a structured questionnaire to collect data on sociodemographic characteristics, family history of disease, healthy habits (dietary habits and physical activity), unhealthy habits, features of depression, school bullying and body image perception. Anthropometric measurements (weight, height) were made by health care professionals certified by the Centro Nacional de Alimentación y Nutrición (National Centre on Diet and Nutrition) of the INS conforming to national technical guidelines for anthropometric nutritional assessment.28
Statistical analysis
We estimated the prevalence of excess weight (overweight and obesity) at the time of the assessment, with the corresponding 95% confidence interval del 95% (95 CI). We performed a descriptive analysis (frequencies and percentages) of sociodemographic characteristics, lifestyle, symptoms of depression, school bullying and body image perception. We compared proportions in lifestyle variables by sex using the χ2 test. We used box plots to compare the number of days foods were consumed by each sex. We performed bivariate analysis using the χ2 test for proportions or the Fisher exact test to identify characteristics associated with nutritional status. We fit a multivariate logistic regression model including the variables that had a statistically significant association with nutritional status in the bivariate analysis. The model included the variables “adequate water intake” and “optimal sleep” once the stratified analysis identified type of school and nutritional status as confounders. We used the statistical software applications Epi-Dat® 3.1 and SPSS® version 22 for Windows (2013, SPSS Inc, USA).
Ethical aspects
The research protocol for the original study was approved by the Committee on Research Ethics of the Instituto Nacional de Salud. All participants were informed of the objectives of the study, and procedures were performed with prior written consent/assent.
RESULTS
General characteristics
The mean age was 12.74 ± 0.94 years, and the median 13 years (interquartile range: 12-13). Boys amounted to 48.0% of the sample (n = 281). We did not find statistically significant differences between sexes in mean age (12.68 ± 0.92 years in boys versus 12.78 ± 0.95 in girls, P = .19). Of all students, 78.3% (n = 459) attended public schools. A family history of diabetes mellitus was reported by 7.2% (n = 42), a family history of arterial hypertension (HTN) by 13.7% (n = 80), a family history of cancer by 3.1% (n = 18) and a family history of stroke by 2.6% (n = 15).
Lifestyle
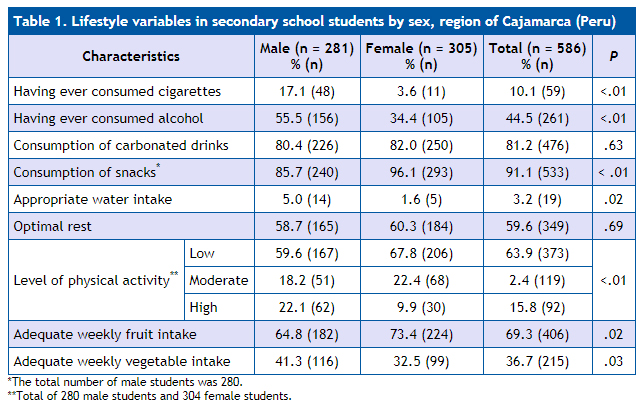
Table 1 summarises the results of the lifestyle questionnaire administered to the students.
| Table 1. Lifestyle variables in secondary school students by sex, region of Cajamarca (Peru) | |||||
|---|---|---|---|---|---|
| Characteristics | Male (n = 281) % (n) |
Female (n = 305) % (n) |
Total (n = 586) % (n) |
P | |
| Having ever consumed cigarettes | 17.1 (48) | 3.6 (11) | 10.1 (59) | <.01 | |
| Having ever consumed alcohol | 55.5 (156) | 34.4 (105) | 44.5 (261) | <.01 | |
| Consumption of carbonated drinks | 80.4 (226) | 82.0 (250) | 81.2 (476) | .63 | |
| Consumption of snacks* | 85.7 (240) | 96.1 (293) | 91.1 (533) | < .01 | |
| Appropriate water intake | 5.0 (14) | 1.6 (5) | 3.2 (19) | .02 | |
| Optimal rest | 58.7 (165) | 60.3 (184) | 59.6 (349) | .69 | |
| Level of physical activity** | Low | 59.6 (167) | 67.8 (206) | 63.9 (373) | <.01 |
| Moderate | 18.2 (51) | 22.4 (68) | 2.4 (119) | ||
| High | 22.1 (62) | 9.9 (30) | 15.8 (92) | ||
| Adequate weekly fruit intake | 64.8 (182) | 73.4 (224) | 69.3 (406) | .02 | |
| Adequate weekly vegetable intake | 41.3 (116) | 32.5 (99) | 36.7 (215) | .03 | |
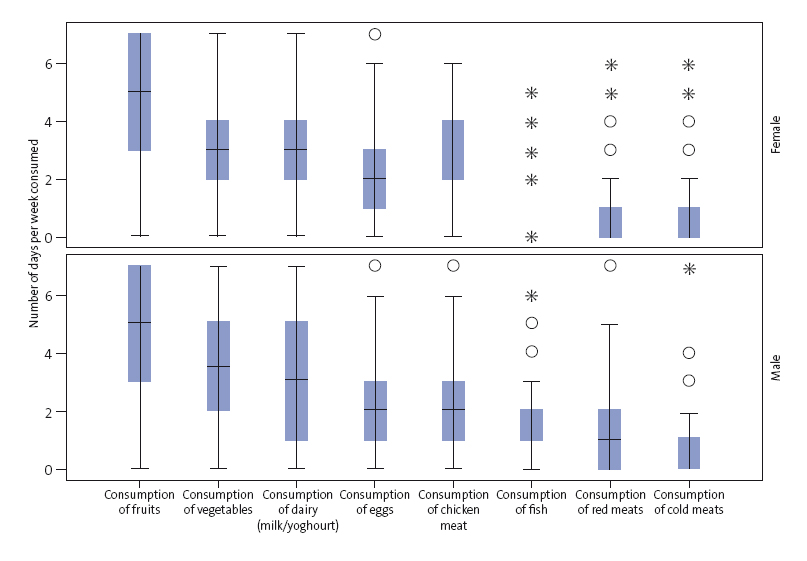
When it came to the weekly frequency of consumption of certain foods, we observed that the foods consumed most often in both sexes were fruits, vegetables, dairy and eggs (Figure 1). As for the least consumed foods, 11.0% (31/281) of male and 18.4% (56/305) of female participants reported not consuming fish during the week, while 52.7% (148/281) of male and 59.7% (182/305) of female participants reported consuming it once a week. Red meat was not consumed by 28.2% of students, a percentage that was higher among female participants (30.5% compared to 25.6%); 43.4% (122/281) of male and 53.4% (163/305) of female students reported eating red meat only once a week. As for cold meats, 63.8% of students reported not eating them (60.5% of male vs 66.9% of female students); 26.0% (73/281) of male and 23.6% (72/305) of female participants ate cold meats once a week, while 9.3% (26/281) of male and 6.2% (19/305) of female participants consumed them two days a week.
| Figure 1. Frequency of food consumption (days per week) in secondary school students in the region of Cajamarca (Peru, 2014), by sex |
|---|
 |

Features of depression
Of all students, 8.9% (52/586) scored in the “mildly depressed” category, 0.5% (3/586) in the “moderately depressed” category and 0.3% (2/586) in the “severely depressed” category. In the male subset, 11% (31/281), 0.7% (2/281) and 0.4% (1/281) had symptoms of depression of mild, moderate and severe intensity, respectively; in female students, the corresponding proportions were 6.9% (21/305), 0.3% (1/305) and 0.3% (1/305), respectively. We did not find a statistically significant association between sex and the presence of symptoms of depression (odds ratio [OR]: 1.68; 95 CI: 0.97 to 2.94, P = .06).
Body image perception
In our sample, 82.4% (483/586) of students perceived themselves as having adequate weight for their age, 9.2% (54/586) as overweight, and 0.5% (3/586) as obese. On the other hand, 7.8% (46/586) perceived their weight as low. We did not find an association between body image perception and sex (P = .85).
Victimization and bullying in school
Of all the students, 74.2% (435/586) reported being subject to bullying. In terms of degree, 31.4% (184/586) reported mild victimization, 26.8% (157/586) moderate victimization and 16.0% (94/586) severe victimization. As to the proportion of bullying, 61.4% (360/586) reported having engaged in violent acts against their schoolmates. Of them, 27.1% (159/586) reported mild aggression, 14.2% (83/586) moderate aggression and 20.1% (118/586) severe aggression. Among the aggressors, 90% reported having been bullied; while 49.1% of non-aggressors reported having been victimised, and there was an association between bullying and victimization (OR: 9.32; 95 CI: 6.05 to 14.36; P < .01). We did not find an association between sex and bullying (63.3% of male vs 59.7% of female students, P = .36) or victimization (74.7% of male vs 73.8% of female students; P = .79).
Prevalence of excess weight
Excess weight was found in 29.69% of students (95 CI: 25.91 to 33.48) (174/586). The prevalence of overweight was 22.86% (95 CI: 19.38 to 26.35) (134/586) and the prevalence of obesity was 6.83% (95 CI: 4.69 to 8.95) (40/586). We did not find an association between sex and nutritional status determined on the basis of anthropometric measurements (Table 2). The proportion of excess weight was 21.7% in students aged 11 years, 32.1% in those aged 12 years, 31.0% in those aged 13 years, 26.4% in those aged 14 years, and 16.7% in those aged 15 years; no cases were identified in students aged 16 or 17 years.
| Table 2. Characteristics of secondary school students by nutritional status, region of Cajamarca (Peru) | |||||
|---|---|---|---|---|---|
| Variables | Nutritional status | ||||
| No overweight or obesity % (n) | Overweight % (n) | Obesity % (n) | P | ||
| Type of school | Public (459) | 72.8 | 21.1 | 6.1 | .044 |
| Private (127) | 61.4 | 29.1 | 9.4 | ||
| Sex | Male (281) | 69.8 | 21.4 | 8.9 | .138 |
| Female (305) | 70.8 | 24.3 | 4.9 | ||
| Family history of DM | No (544) | 71.1 | 22.4 | 6.4 | .212 |
| Yes (42) | 59.5 | 28.6 | 11.9 | ||
| Family history of HTN | No (506) | 70.6 | 22.9 | 6.5 | .763 |
| Yes (80) | 68.8 | 22.5 | 8.8 | ||
| Family history of stroke | No (571) | 70.4 | 23.1 | 6.5 | .103* |
| Yes (15) | 66.7 | 13.3 | 20.0 | ||
| Cigarette use | No (527) | 70.6 | 22.6 | 6.8 | .884 |
| Yes (59) | 67.8 | 25.4 | 6.8 | ||
| Alcohol use | No (325) | 69.5 | 23.1 | 7.4 | .815 |
| Yes (261) | 71.3 | 22.6 | 6.1 | ||
| Consumption | No (110) | 60.9 | 30.0 | 9.1 | .057 |
| Yes (476) | 72.5 | 21.2 | 6.3 | ||
| Consumption of snacks | No (52) | 63.5 | 25.0 | 11.5 | .312 |
| Yes (533) | 70.9 | 22.7 | 6.4 | ||
| Optimal water intake | No (567) | 71.4 | 22.0 | 6.5 | .005 |
| Yes (19) | 36.8 | 47.4 | 15.8 | ||
| Hours of sleep | Risk (237) | 75.5 | 20.3 | 4.2 | .035 |
| Optimal (349) | 66.8 | 24.6 | 8.6 | ||
| Physical activity | Baja (373) | 68.1 | 22.8 | 9.1 | .015 |
| Moderate / high (211) | 73.9 | 23.2 | 2.8 | ||
| Adequate consumption of fruit | No (180) | 68.9 | 22.8 | 8.3 | .625 |
| Yes (406) | 70.9 | 22.9 | 6.2 | ||
| Adequate consumption of vegetables | No (371) | 69.8 | 23.7 | 6.5 | .761 |
| Yes (215) | 71.2 | 21.4 | 7.4 | ||
| Body image | Low weight (46) | 95.7 | 2.2 | 2.2 | <.01 |
| Normal (483) | 74.1 | 22.2 | 3.7 | ||
| Excess weight (57) | 17.5 | 45.6 | 36.8 | ||
| Symptoms of depression | Normal (519) | 71.5 | 22.5 | 6.0 | .018* |
| Mild (49) | 61.5 | 26.9 | 11.5 | ||
| Moderate / grave (5) | 40.0 | 20.0 | 40.0 | ||
| School bullying | No (226) | 67.3 | 23.9 | 8.8 | .239 |
| Yes (360) | 72.2 | 22.2 | 5.6 | ||
| School victimization | No (151) | 69.5 | 21.2 | 9.3 | .359 |
| Yes (435) | 70.6 | 23.4 | 6.0 | ||
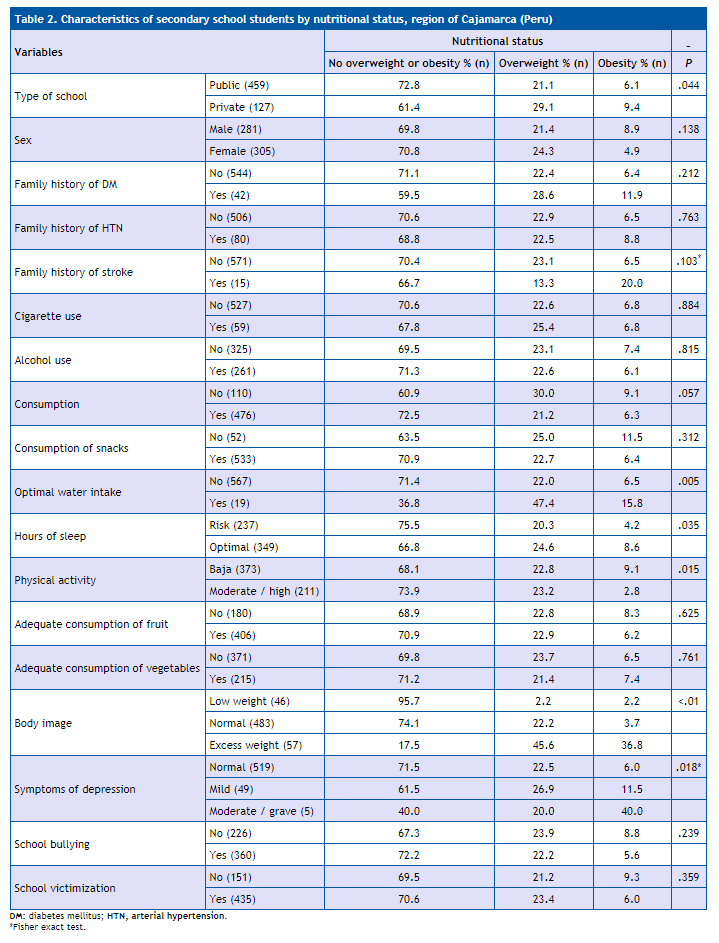
Characteristics associated with excess weight
They are summarised in Table 2. In the multinomial logistic regression analysis, “No overweight/obesity” was considered the reference level. We included in the model those variables that were significantly associated in the bivariate analysis (P < .05). We identified the variables “optimal water intake” and “optimal rest” as confounders. In the bivariate analysis, we found an association between type of school and excess weight (crude OR: 1.67; 95 CI: 1.11 to 2.53), however, we found that adequate water intake was strongly associated with attending a private school (crude OR: 5.32; 95 CI: 2.1 to 13.6) as well as with excess weight (crude OR: 4.28; 95 CI: 1.65 to 11.08). Optimal rest behaved similarly, as it was associated with both attending a private school (crude OR: 1.56; 95 CI: 1.03 to 2.37) and excess weight (crude OR: 1.53; 95 CI: 1.06 to 2.22).
| Table 3. Factors associated with overweight and obesity in secondary school students, region of Cajamarca (Peru | ||||||
|---|---|---|---|---|---|---|
| Overweight aOR (95 CI) |
P | Obesity aOR (95 CI) |
P | |||
| Model 1* | Sex | Female | 1 | 1 | ||
| Male | 0.84 (0.56-1.26) | .408 | 2.05 (1.02-4.11) | .044 | ||
| Type of school | Private | 1 | 1 | |||
| Public | 0.62 (0.39-0.99) | .043 | 0.43 (0.20-0.92) | .030 | ||
| Physical activity | Moderate/high | 1 | 1 | |||
| Low | 1.12 (0.73-1.70) | .604 | 4.14 (1.65-10.35) | .002 | ||
| Depression symptoms | Moderate/severe | 1 | 1 | |||
| Mild | 1.05 (0.09-13.08) | .969 | 0.42 (0.04-3.69) | .431 | ||
| Normal | 0.71 (0.06-8.11) | .783 | 0.15 (0.02-1.07) | .059 | ||
| Model 2** | Sex | Female | 1 | 1 | ||
| Male | 0.80 (0.53-1.21) | .287 | 1.91 (0.95-3.86) | .071 | ||
| Type of school | Private | 1 | 1 | |||
| Public | 0.69 (0.43-1.13) | .147 | 0.51 (0.23-1.10) | .085 | ||
| Physical activity | Moderate/high | 1 | 1 | |||
| Low | 1.14 (0.74-1.74) | .552 | 4.20 (1.66-10.61) | .002 | ||
| Depression symptoms | Moderate/severe | 1 | 1 | |||
| Mild | 0.91 (0.07-11.26) | .942 | 0.36 (0.04-3.27) | .362 | ||
| Normal | 0.66 (0.06-7.44) | .736 | 0.13 (0.02-1.01) | .051 | ||
| Adequate water intake | Yes | 1 | 1 | |||
| No | 0.22 (0.07-0.65) | .006 | 0.24 (0.05-1.12) | .068 | ||
| Optimal rest | Yes | 1 | 1 | |||
| No | 0.73 (0.48-1.11) | .138 | 0.47 (0.22-0.99) | .049 | ||
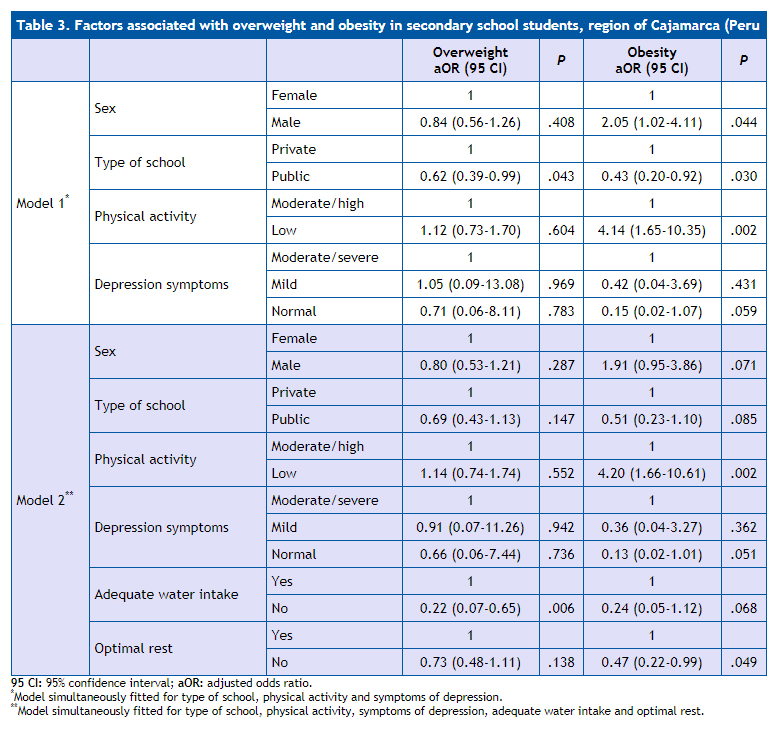
Table 3 presents two models. In the first model, the type of school was independently associated with overweight (adjusted OR: 0.62; 95 CI: 0.39 to 0.99; P = .043). Obesity, in turn, was associated with low physical activity (adjusted OR: 4.14; 95 CI: 1.65 to 10.35; P = .002) and with male sex (adjusted OR: 2.05; 95 CI: 1.02 to 4.1; P = .044); attending a public school was a protective factor against obesity (adjusted OR: 0.43; 95 CI: 0.20 to 0.92; P = .030). The second model included confounding variables, and the variable that was independently associated with overweight as a protective factor was “inadequate water intake” (adjusted OR: 0.22; 95 CI: 0.07 to 0.65; P = .06); attending a public school was not associated with overweight, although it maintained its tendency to behave as a protective factor (adjusted OR: 0.69; 95 CI: 0.43 to 1.13; P = .147). The risk factor associated independently with obesity was low level of physical activity (adjusted OR: 4.20; 95 CI: 1.66 to 10.61; P = .002), while lack of optimal sleep was a protective factor (adjusted OR: 0.47; 95 CI: 0.22 to 0.99; P = .049).
DISCUSSION
We found that one out of three secondary school students in an Andean region of Peru had excess weight. The proportion of overweight was 22.9%, while obesity affected 6.8% of the adolescents. Based on our findings, in 2014 there would have been between 47 000 and 62 000 adolescents with excess weight in the region of Cajamarca (Peru). Our findings are consistent with calculations for the northern region of the Peruvian Andes (year 2014), where the prevalences of overweight and obesity in adolescents were estimated at 18.5% and 7.5%, respectively.7 However, our data corroborated the increasing trend in excess weight, exceeding the 20% prevalence reported for this region in the 2009-2010 period.10
The figures found in our study were lower than those reported for a district in the Lima Metropolitan Area (year 2012), where the prevalences of overweight and obesity in a sample of 1743 students were 33.7% and 14.4% respectively.12 Other studies conducted in Peru have estimated lower figures: a study conducted in schools in four regions of Peru found a prevalence of excess weight of 11.3%11; in 2010, overweight was found in 6.8% of male students and 3.6% of female students in a city in the Peruvian highlands, while in cities located in the jungle, the prevalence of overweight was 16.6% in female students and 13.7% in male students, while the prevalence of obesity was 2.4% in female students and 2.7% in male students.13
The most prevalent lifestyle factors included consumption of alcoholic beverages (44.5%), and a high consumption of carbonated drinks (81.2%) and snacks (91.1%). Some lifestyle habits were associated with sex: in male students, there was a higher consumption of cigarettes, alcohol and vegetables, in addition to a greater level of physical activity, while female students consumed more snacks and fruit. The diet was characterised by a large weekly consumption of fruits, vegetables and dairy in both male and female students; the frequency of consumption of cold meats was low. The most frequently consumed meat was chicken, with consumption of fish and red meat being lower. The observed diet reveals a decreased frequency of the traditional homemade diet with an increase in the consumption of processed foods, fast food and foods prepared outside the home. Water intake was generally below the recommended amount, and consumption of sugary carbonated drinks accounted for most of the fluid intake. This could be explained by the fact that healthy food options in school settings, where adolescents spend most of their time, are scarce or nonexistent, while low-quality foods abound.29
Our findings show that adolescents in public schools are less likely to be overweight or obese; similar findings have been reported for developed30 as well as developing countries.31,32 The type of school (private vs public) may behave as a proxy for parental income level: greater incomes would facilitate family spending on goods and services associated with a greater risk of excess weight in adolescents, such as videogames, foods prepared outside the home (including fast food) and increased consumption of sweets, snacks and carbonated drinks.
We found that male students were more likely to be obese compared to female students, a difference previously reported in studies on adolescents conducted in Puerto Rico, 32 Brazil,32 Saudi Arabia30 and the Asian-American population of the United States.33 However, the differences in prevalence observed between sexes were small, so our study was not consistent with the predominance of the male or female sex in the distribution of excess weight.34
Another modifiable risk factor that was independently associated with obesity was low level of physical activity. This finding was consistent with a growing body of evidence demonstrating that physical inactivity is an important risk factor in the development of obesity during adolescece.35-37 A meta-analysis of randomised controlled trials38 in which the intervention was a programme of aerobic exercise lasting at least four weeks in children and adolescents aged 2 to 18 years with overweight or obesity found a reduction in BMI of 1.08 kg/m2. A cross-sectional study conducted between 2001 and 2002 in adolescents aged 10 to 16 years in 34 countries found that a low level of physical activity and a large number of hours of television viewing were associated with overweight, independently of dietary variables.39 A review that assessed risk factors for overweight and obesity in adolescents in Asian countries found that six out of eight studies reported that physical inactivity was associated with excess weight.40
As occurred in other studies, we did not find an association between nutritional status and modifiable risk factors such as consumption of carbonated drinks, snacks or fruits and vegetables. A study conducted in Canada in children aged 11 to 16 years did not find a clear association between weight and patterns of consumption of fruits, vegetables and snacks36; and an association between overweight/obesity and consumption of fresh fruit, vegetables, carbonated drinks and fast food 4 or more days a week was also not found in children and adolescents aged 5 to 18 years in northern China.41 A possible explanation for the absence of an association would be the increased probability of recall bias in relation to food consumption in individuals with overweight and obesity compared to individuals with normal weight42; on the other hand, in our study we only obtained data for the frequency of food consumption, without considering portion sizes for unhealthy foods, which may have been larger in adolescents with excess weight.
We found that the probability of overweight and obesity decreased when symptoms of depression were mild or absent. Since this was a cross-sectional study, we could not establish a temporal relationship as a criterion to determine causality. A study in a representative sample of adolescents in Canada reported that obesity between ages 6 and 12 years increased the risk of depression at age 13 years.16 Another study analysed the association between depression symptoms and increases in BMI in adolescents aged 11 to 16 years, and concluded that symptoms of depression were not a predictor of excessive weight gain in adolescence.15 In our study, we found that the perception of excess weight was associated with the presence of overweight and obesity; however, a study conducted in Spanish adults and adolescents found that despite the increase in the prevalence of excess weight between 1987 and 2007, the parents of children of either sex increasingly perceived as normal the weight of their children with objective excess weight.43
Our study did not find an association between nutritional status and any form of school bullying (aggression and victimization). Our findings are similar to those reported in studies on adolescents in the United States18 and Finland,20 in which the presence of overweight or obesity were not associated with bullying or victimization. However, a meta-analysis published in 2014 found that the probability of being victimised was 19% greater in adolescents with overweight, and 51% greater in obese adolescents17; furthermore, a study of Italian adolescents found that involvement in bullying depended on the degree of excess weight, with severely obese male adolescents being at higher risk of being victimised and being aggressors; the same study found that obese adolescents were more often involved as aggressors compared to adolescents with normal weight or overweight.19
The results of this study must be interpreted taking its weaknesses into account. The first weakness is that the study sample was obtained from a study that was originally designed to estimate the prevalence of metabolic syndrome, and thus, the overweight and obesity estimates may not be extrapolated to the population under study; second, the potential for recall bias in the assessment of physical activity, the family history, dietary habits and school victimization/bullying, which could be a reason for the absence of an association with excess weight; last of all, the cross-sectional design did not allow us to establish causal relationships between the several factors analysed in relation to excess weight.
To conclude, we found that three out of every ten adolescent students that resided in urban areas in the Peruvian Andes had excess weight, and that overweight was the most frequent abnormality. A low level of physical activity was the main independent risk factor for the development of obesity. Adolescents attending private schools were at higher risk of overweight and obesity; however, this association was influenced by lifestyles such as adequate water intake and optimal rest, which behaved as confounders. The results of our study support the need to implementing strategies to increase the level of physical activity in the educational environment and for this healthy habit to be then transferred to the home. While we did not find an association with specific dietary habits, the high consumption of alcoholic and carbonated beverages and snacks was alarming.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
FUNDING
The study was funded by the Universidad Nacional de Cajamarca, according to Rectoral Decision No 038-2013-UNC of February 27, 2013, which stated the decision to “approve the research projects presented by the educators of the Universidad Nacional de Cajamarca to be funded with Competitive Grants from the Canon Minero, Sobrecanon y Regalías Mineras, corresponding to the 2012 Financiamiento de Investigación Docente Canon Minero.
ABBREVIATIONS
BMI: body mass index • CVA: cardiovascular arrest • HTN: arterial hypertension • INS: Instituto Nacional de Salud • OR: odds ratio • WHO: World Health Organization • zBMI: body mass index z-score for age• 95 CI: 95% confidence interval.
REFERENCES
- NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet. 2016;387:1377-96.
- Simmonds M, Burch J, Llewellyn A, Griffiths C, Yang H, Owen C, et al. The use of measures of obesity in childhood for predicting obesity and the development of obesity-related diseases in adulthood: a systematic review and meta-analysis. Health Technol Assess. 2015;19:1-336.
- Forrest KYZ, Leeds MJ. Prevalence and associated factors of overweight among Mexican-American adolescents. J Am Diet Assoc. 2007;107:1797-800.
- Niehues JR, Gonzales AI, Lemos RR, Bezerra PP, Haas P. Prevalence of overweight and obesity in children and adolescents from the age range of 2 to 19 years old in Brazil. Int J Pediatr. 2014;2014:583207.
- Catalani F, Fraire J, Pérez N, Mazzola M, Martínez AM, Mayer MA. Prevalencia de bajo peso, sobrepeso y obesidad en adolescentes escolarizados de la provincia de La Pampa. Arch Argent Pediatría. 2016;114:2-3.
- Skinner AC, Perrin EM, Skelton JA. Prevalence of obesity and severe obesity in US children, 1999-2014. Obesity. 2016;24:1116-23.
- Instituto Nacional de Salud, Centro Nacional de Alimentación y Nutrición. Observatorio de nutrición y estudio del sobrepeso y obesidad. Situación del sobrepeso y obesidad en la población peruana. In: Observa-T Perú [online] [accessed 07/09/2017]. Available at www.observateperu.ins.gob.pe/sala-situacional/situacion-nutricional
- Hernández-Vásquez A, Bendezú-Quispe G, Díaz-Seijas D, Santero M, Minckas N, Azañedo D, et al.Análisis espacial del sobrepeso y la obesidad infantil en el Perú, 2014. Rev Peru Med Exp Salud Pública. 2016;33:489.
- Día Mundial de la Población 2015. In: Instituto Nacional de Estadística e Informática de Perú [online] [accessed 07/09/2017]. Available at www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1251/Libro.pdf
- Álvarez-Dongo D, Sánchez-Abanto J, Gómez-Guizado G, Tarqui-Mamani C. Sobrepeso y obesidad: prevalencia y determinantes sociales del exceso de peso en la población peruana (2009-2010). Rev Peru Med Exp Salud Pública. 2012;29:303-13.
- Núñez-Robles E, Huapaya-Pizarro C, Torres-Lao R, Esquivel-León S, Suarez-Moreno V, Yasuda-Espinoza M, et al. Prevalence of cardiovascular and metabolic risk factors in school students, university students, and women from community-based organizations in the districts of Lima, Callao, la Libertad and Arequipa, Peru 2011. Rev Peru Med Exp Salud Pública. 2014;31:652-9.
- Lozano-Rojas G, Cabello-Morales E, Hernández-Diaz H, Loza-Munarriz C. Prevalencia de sobrepeso y obesidad en adolescentes de un distrito urbano de Lima, Perú 2012. Rev Peru Med Exp Salud Pública. 2014;31:494-500.
- Bustamante A, Maia J. Weight status and cardiorespiratory fitness in school students in the central region of Peru. Rev Peru Med Exp Salud Pública. 2013;30:399-407.
- Liria M, Mispireta M, Lanata C, Creed-Kanashiro H. Perfil nutricional en escolares de Lima y Callao. 1st Lima, Peru: Instituto de Investigación Nutricional (ISIL); 2008.
- Larsen JK, Otten R, Fisher JO, Engels RC. Depressive symptoms in adolescence: a poor indicator of increases in body mass index. J Adolesc Health. 2014;54:94-9.
- Ames ME, Wintre MG, Flora DB. Trajectories of BMI and internalizing symptoms: Associations across adolescence. J Adolesc. 2015;45:80-8.
- Van Geel M, Vedder P, Tanilon J. Are overweight and obese youths more often bullied by their peers? A meta-analysis on the correlation between weight status and bullying. Int J Obes (Lond). 2014;38:1263-7.
- Odar Stough C, Merianos A, Nabors L, Peugh J. Prevalence and predictors of bullying behavior among overweight and obese youth in a nationally representative sample. Child Obes. 2016;12:263-71.
- Bacchini D, Licenziati MR, Garrasi A, Corciulo N, Driul D, Tanas R, et al. Bullying and victimization in overweight and obese outpatient children and adolescents: an italian multicentric study. PloS One. 2015;10:e0142715.
- Kaltiala-Heino R, Lankinen V, Marttunen M, Lindberg N, Fröjd S. Overweight, perceived overweight and involvement in bullying in middle adolescence. Child Abuse Negl. 2016;54:33-42.
- Brixval CS, Rayce SLB, Rasmussen M, Holstein BE, Due P. Overweight, body image and bullying--an epidemiological study of 11- to 15-years olds. Eur J Public Health. 2012;22:126-30.
- Twig G, Yaniv G, Levine H, Leiba A, Goldberger N, Derazne E, et al. Body-mass index in 2.3 million adolescents and cardiovascular death in adulthood. N Engl J Med. 2016;374:2430-40.
- Ninantanta J, Núñez L, García S, Romaní F. Frecuencia de síndrome metabólico en estudiantes de secundaria, universitarios y madres residentes de una región andina del Perú. Rev Peru Med Exp Salud Pública. 2016;33:640-50.
- De Onís M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. 2007;85:660-7.
- Universidad de Granada. Traducción de las guías para el procesamiento de datos y análisis del Cuestionario Internacional de Actividad Física (IPAQ). Versiones corta y larga. In: Junta de Andalucía [online] [accessed 07/09/2017]. Available at www.juntadeandalucia.es/salud/sites/csalud/galerias/documentos/p_4_p_2_promocion_de_la_salud/actividad_fisica_alimentacion_equilibrada/IPAQ_Guia_Traducida.pdf
- Cogollo Z, Díaz C, Campo A. Exploración de la validez de constructo de la escala de Zung para depresión en adolescentes escolarizados. Colom Med. 2006;37:102-6.
- Observatorio Peruano de Drogas. Informe Ejecutivo: IV Estudio nacional de prevención y consumo de drogas en estudiantes de secundaria, 2012. Lima: DEVIDA; 2013.
- Aguilar L, Contreras M, Calle M del C. Guía técnica para la valoración nutricional antropométrica de las personas adolescentes. In: Ministerio de Salud, Instituto Nacional de Salud [online] [accessed 07/09/2017]. Available at http://repositorio.ins.gob.pe/bitstream/INS/214/1/CENAN-0056.pdf
- Aceves-Martins M, Llauradó E, Tarro L, Solà R, Giralt M. Obesity-promoting factors in Mexican children and adolescents: challenges and opportunities. Glob Health Action. 2016;9:29625.
- Al-Hazzaa HM, Abahussain NA, Al-Sobayel HI, Qahwaji DM, Musaiger AO. Lifestyle factors associated with overweight and obesity among Saudi adolescents. BMC Public Health. 2012;12:354.
- Elías-Boneta AR, Toro MJ, García O, Torres R, Palacios C. High prevalence of overweight and obesity among a representative sample of Puerto Rican children. BMC Public Health. 2015;15:219.
- Rosaneli CF, Auler F, Manfrinato CB, Rosaneli CF, Sganzerla C, Bonatto MG, et al. Evaluation of the prevalence and nutritional and social determinants of overweight in a population of schoolchildren: a cross-sectional analysis of 5037 children. Rev Assoc Medica Bras (1992). 2012;58:472-6.
- Cook WK, Tseng W, Bautista R, John I. Ethnicity, socioeconomic status, and overweight in Asian American adolescents. Prev Med Rep. 2016; 4:233-7.
- Sweeting HN. Gendered dimensions of obesity in childhood and adolescence. Nutr J. 2008;7:1.
- Leatherdale ST. A cross-sectional examination of school characteristics associated with overweight and obesity among grade 1 to 4 students. BMC Public Health. 2013;13:982.
- Janssen I, Katzmarzyk PT, Boyce WF, King MA, Pickett W. Overweight and obesity in Canadian adolescents and their associations with dietary habits and physical activity patterns. J Adolesc Health. 2004;35:360-7.
- Saikia D, Ahmed SJ, Saikia H, Sarma R. Overweight and obesity in early adolescents and its relation to dietary habit and physical activity: a study in Dibrugarh town. Clin Epidemiol Glob Health. 2016;4:S22-28.
- Kelley GA, Kelley KS, Pate RR. Exercise and BMI in overweight and obese children and adolescents: a systematic review and trial sequential meta-analysis. Biomed Res Int. 2015;2015:704539.
- Janssen I, Katzmarzyk PT, Boyce WF, Vereecken C, Mulvihill C, Roberts C, et al. Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationships with physical activity and dietary patterns. Obes Rev. 2005;6:123-32.
- Mistry SK, Puthussery S. Risk factors of overweight and obesity in childhood and adolescence in South Asian countries: a systematic review of the evidence. Public Health. 2015;129:200-9.
- Guo X, Zheng L, Li Y, Yu S, Sun G, Yang H, et al. Differences in lifestyle behaviors, dietary habits, and familial factors among normal-weight, overweight, and obese Chinese children and adolescents. Int J Behav Nutr Phys Act. 2012;9:120.
- Vance VA, Woodruff SJ, McCargar LJ, Husted J, Hanning RM. Self-reported dietary energy intake of normal weight, overweight and obese adolescents. Public Health Nutr. 2009;12:222-7.
- Salcedo V, Gutiérrez-Fisac JL, Guallar-Castillón P, Rodríguez-Artalejo F. Trends in overweight and misperceived overweight in Spain from 1987 to 2007. Int J Obes (Lond). 2010;34:1759-65.