
Vol. 19 - Num. 73
Original Papers
Quality of life in children with attention deficit hyperactivity disorder (ADHD)
Montserrat Hernández Martíneza, Nuria Pastor Hernándezb, Xavier Pastor Duránc, Cristina Boix Lluchd, Anna Sans Fitóe
aPediatra. Centro de Asistencia Primaria Collblanc. Consorci Sanitari Integral. Hospitalet de Llobregat. Barcelona. España.
bPsicóloga general sanitaria. Centro Psicológico Iranea. Barcelona. España.
cServicio de Pediatría. Hospital Clínic. Departamento de Pediatría. Facultad de Medicina. Universidad de Barcelona. Barcelona. España.
dNeuropsicóloga. Unidad de Trastornos de Aprendizaje (UTAE). Hospital San Joan de Dèu. Esplugues de Llobregat. Barcelona. España.
eNeuropediatra. Unidad de Trastornos del Aprendizaje (UTAE). Hospital San Joan de Dèu. Esplugues de Llobregat. Barcelona. España.
Correspondence: M Hernández. E-mail: 21583mhm@comb.cat
Reference of this article: Hernández Martínez M, Pastor Hernández N, Pastor Durán X, Boix Lluch C, Sans Fitó A. Quality of life in children with attention deficit hyperactivity disorder (ADHD). Rev Pediatr Aten Primaria. 2017;19:31-9.
Published in Internet: 10-03-2017 - Visits: 25927
Abstract
Introduction: the Attention Deficit Hyperactivity Disorder (ADHD) is the most common neurodevelopmental disorder in childhood. It’s definition points toward those problems which originate discomfort in persons and their environment. ADHD has a multifactorial origin, with a neurobiological basis, strong genetic component and interaction with environmental factors. Nearly 75% of children with ADHD will be adolescents with ADHD, and 50% of them will be adults with ADHD. This disorder causes a great impact at cognitive, emotional and social levels. The objective of this study is to evaluate the impact of ADHD over the family, school and social relationships of affected children under the view of primary care, using the concept of Health Related Quality of Life (HRQoL), defined as the individual and subjective patient’s self-perception related to their own health, as well as the degree of physical, psychological and social welfare in respect to the disease and the treatment.
Material and methods: KINDL® was used in the evaluation of HRQoL. It was applied to two groups children aged from 6 to 16 years old. One group included children with a recent diagnosis of ADHD and still not treated with any therapy. The other group consisted in children without ADHD.
Results: results showed that the global score of HRQoL as well as the six dimensions which compose this measure have significant differences. The HRQoL is significantly lower in the group of ADHD children when compared with the control group.
Conclusion: as a main conclusion, ADHD impairs seriously the quality of life of children who suffer such disorder.
Keywords
● Attention deficit disorder (ADHD) ● Quality of lifeINTRODUCTION
Attention deficit hyperactivity disorder (ADHD) affects approximately one in twenty children or adolescents in Europe.1 It is a problem of considerable magnitude given its high prevalence, the psychological problems it entails, the potential associated comorbidities and its chronic nature. Consequently, it should be considered a public health problem.2
Patients with ADHD may experience symptoms of inattention, hyperactivity or impulsivity, emotional dysregulation, cognitive impairment and comorbidities. It causes functional impairment with a negative impact on quality of life. Although it may be invisible in the context of everyday life, it does have a serious impact on the psychological and social well-being and academic achievement of affected individuals.3 The primary care (PC) paediatrician plays a critical role in the early detection and management of this disorder, and must approach it as a chronic health problem.4
In recent years, the importance of health-related quality of life (HRQoL) in children has been reflected in the increasing number of scientific publications on the subject and the development of tools for its assessment. This concept derives from the definition of health by the World Health Organization (WHO)5 as “a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity.”
In 1982, Kaplan and Bush proposed the term health-related quality of (HRQoL), which construes health as a holistic, multidimensional and integral concept that for the first time takes into account how the individual perceives his wellbeing in relation to physical, psychological, cognitive and social aspects.6 The definition includes both elements intrinsic to the individual as well as external elements that interact with the individual and may impact his or her health status. Thus, the concept of quality of life cannot be in any way extricated from the cultural norms, behavioural patterns and expectations of each individual, and these aspects are particularly relevant when it comes to developing or adapting instruments to measure it. Health-related quality of life is evaluated by means of standardised questionnaires comprised of different dimensions that are assessed with items whose answers are formatted as categorical scales.
The term child health-related quality of life (CHRQoL)7 refers to how children and adolescents perceive their physical, psychological and social functioning when one or more of them have been limited or changed by disease or injury, and according to their developmental stage, individual differences and sociocultural context.
Objective
The main objective of this study was to assess the impact of ADHD on the quality of life of children with this disorder. To do so, we analysed the differences in self-perceived CHRQoL between a group of children with ADHD and a control group of children without ADHD. The tool chosen for the assessment was the KINDL® questionnaire, which assesses six dimensions: physical, psychological, self-esteem, family, friends, and school. We compared the impact of ADHD on the different dimension and on the total score by observing the difference between groups in the affected areas.
MATERIALS AND METHODS
The health care setting from which patients were recruited comprehended the PC services of the Primary Care Centre (PCC) of Collblanc and the ambulatory clinic of the Learning Disorders Unit (LDU) of the Hospital de San Joan de Dèu (Barcelona, Spain). The recruitment period lasted one calendar year (January 2014 to January 2015).
The diagnosis was made using tests that apply the DSM-IV-TR clinical criteria. Specifically, we used the ADHD Rating Scale-IV (du Paul 1998)8 completed for two different settings: one by teachers and one by the family. Inclusion required onset of symptoms prior to age 7 years that significantly interfered with the child or adolescent’s functioning in academic, social and family settings and could not be explained by a different disorder.
Criteria for inclusion in the experimental group: 1) age 6 to 18 years; 2) children with a recent ADHD diagnosis that have not initiated any type of treatment (pharmacological or psychological); 3) absence of chronic disease that may impact quality of life and d) ability to correctly complete the questionnaire.
Criteria for inclusion in the control group: 1) age 6 to 18 years; 2) failure to meet the DSM-IV-TR criteria for the clinical diagnosis of ADHD; 3) absence of chronic disease that may impact quality of life and d) ability to correctly complete the questionnaire.
We considered the following prior to approving participation in the study:
- Approval by the Ethics Committee of the Consorcio Sanitario Integral (Integral Health Care Consortium), which includes the PCC of Collblanc, where most of the study was conducted.
- Informed consent (IC) form. Children aged 12 or more years signed the consent themselves after being informed along with their parents. Parents signed the consent for children aged less than 12 years.
- Informational brochure on the study to be conducted. The patient, or the parents (or legal guardians) for children below the age of consent, were given sufficient information on the objectives of the study.
The final sample recruited for the study consisted of a total of 58 children of both sexes aged 6 to 16 years. It included 26 children with ADHD and 32 without.
Methods
We conducted an inferential case-control study. Participating children filled out the Spanish version of the German KINDL® questionnaire (Figure 1) adapted to their age. To assess the impact on affected areas of quality of life in both groups, we compared total scores and scores in the different dimensions under study.
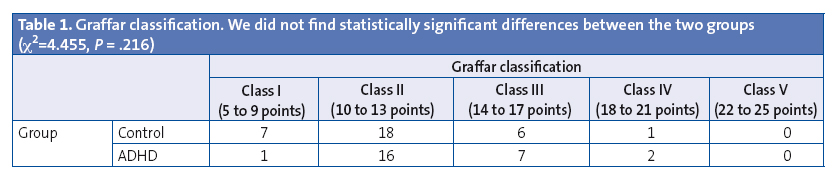
Since self-perceived quality of life is determined to a great extent by the sociocultural context of the individual, we assessed this context by means of the Graffar classification. This classification takes into account educational attainment, social class, household size, type of residence and household income to quantify socioeconomic level in a single value. The purpose of the comparative analysis of this classification between the two groups was to identify potential differences that may account for the results.
To select the instrument used for the assessment of quality of life, we made a systematic review of the literature on the instruments available for measuring general HRQoL.9,10
We chose the KINDL® tool for the study. First, it is validated in the Spanish language for the Spanish population. It has good psychometric properties.11 It has a good internal consistency (α coefficient range, 0.40–0.88) and test-retest reliability (ICC range, 0.52–0.80) in most dimensions. Research on the Spanish version of the KINDL® has found acceptable reliability and validity coefficients, which affords us a new instrument for application in paediatric clinical practice and public health. It is a self-report tool to measure general HRQoL that is completed by children and adolescents themselves, so it reflects the perceptions of the individual. It was developed in Germany by Bullinger in 1994 and revised by Ravens-Sieberer and Bullinger in 1998. The Spanish version was developed by Rajmil et al in Barcelona in 2004.12 The questionnaire was designed based on the concept of health defined by the WHO, taking into account expert opinions as to the most important dimensions to be measured in children and adolescents with chronic illnesses. It consists of 24 items distributed into six dimensions of four items each: physical well-being (items 1, 2, 3 and 4); psychological well-being (items 5, 6, 7 and 8); self-esteem (items 9, 10, 11 and 12); family (items 13, 14, 15 and 16); friends (items 17, 18, 19 and 20); and school (items 21, 22, 23 and 24).
It can be used in children aged 4 to 16 years. To correctly cover this age range, there are three versions: Kiddy-KINDL® for children aged 4 to 7 years, Kid-KINDL® for children aged 8 to 12 years and Kiddo-KINDL® for ages 13 to 16 years. There are also proxy versions for parents that were not used in our study.
The answer choices for each item of the KINDL® are given as five-category Likert scales that range from 1 (never) to 5 (always). All questions refer to the week prior to the interview, and the scores obtained in each dimension are transformed to a standardised scale that allows their comparison. A higher score represents a better HRQoL. A single total or global HRQoL score can be obtained from the scores of the six dimensions. The Kiddy® version for younger children reduces the answer choices to three, and while the items are organised in the same dimensions, its results are only validated for the global HRQoL score.
The questionnaires were self-administered and participation was voluntary. The same research team members explained how to complete the questionnaires and addressed any concerns or questions, documenting the comments made by the children, who filled out the forms themselves and separately at the clinic.
For the purpose of recording and analysing the scores of the questionnaires, we created an electronic form into which we transcribed the answers on an anonymous basis. After completing data collection, we downloaded and adapted the algorithm used to calculate the total score and the scores for the different dimensions. This algorithm is provided by BiblioPRO (www.bibliopro.org) for the Kid-KINDL and the Kiddo-KINDL in the form of a syntax file for the Statistical Package for the Social Sciences® (SPSS®). For the Kiddy-KINDL, we adapted it for the reduction in the number of answer categories and to calculate only the total score. We analysed the data using IBM’s SPSS® version 23. We compared the scores for each dimension and the total scores by means of Student’s t test after analysing the homogeneity of variances in the groups to ensure the assumptions for the test were met. We used the KINDL® after requesting the authorization from the virtual library of international scientific reference virtual library on Spanish-language questionnaires on patient-reported outcomes (BiblioPRO, www.bibliopro.org)13. BiblioPRO is an online resource developed by the Health Services Research Unit of the Institut Municipal d´Investigació Mèdica (Municipal Institute of Medical Research [IMIM-IMAS]) in the framework of the Red de Investigación cooperativa para la Investigación en Resultados de Salud y Servicios Sanitarios (Network for Cooperative Research of Outcomes in Health and Health Services [IRYSS]), funded by the Instituto de Salud Carlos III (G03/202).
The timeline included an initial preparation phase for organising the documentation and the recruitment procedures, and to obtain the approval of the research ethics committee. Then, we started including participants in the study who, following verification of the inclusion criteria and completion of IC, filled out the questionnaire. The questionnaire did not include any identifiable demographic information, so that the data from the questionnaire were anonymised. Once we had a sufficient sample size, we proceeded to entering the responses in the electronic database, followed by a descriptive and inferential statistical analysis and the generation of charts to represent the results.
RESULTS
The sex distribution in our sample was of 11 boys and 20 girls in the control group, while there were 14 boys and 12 girls in the ADHD group. The comparison of the proportions in the two groups by means of the chi-square test did not find statistically significant differences (χ2 = 1.936; P = .164). We also found similar distributions in the Graffar classification used to assess socioeconomic level and educational attainment in the environment of the participants (Table 1), and found no significant differences between groups (χ2 = 4.455; P = .216).
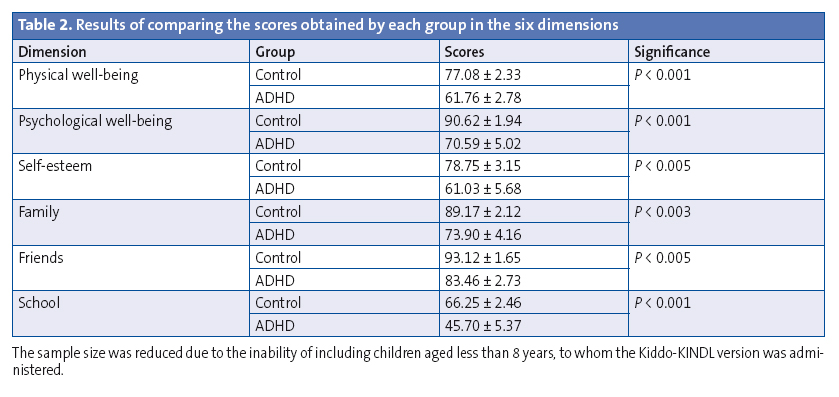
We found highly significant differences between both groups (P < .02) in each of the six dimensions and the overall score, with a poorer quality of life in children with ADHD compared to the control group.
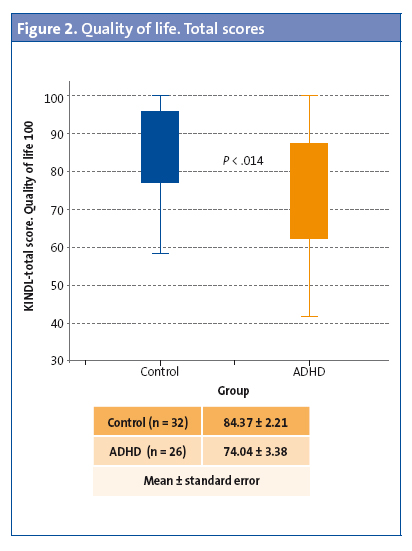
The algorithm for calculating the results from the Likert scale values entered in the questionnaires offers three equivalent formats: a cumulative result, an average and a transformed score on a scale from 0 to 100. To make things simple, we preferred to use the format that results from re-expression on a scale from 0 to 100, with 100 being the highest possible score. We have represented the results graphically by means of box plots, which provide information on the minimum and maximum values and the distributions of the results in the sample. The rectangles are the boxes, and the arms are the whiskers. They are based on quartiles. The bottom side of the box marks the first quartile (Q1, 25th percentile), the horizontal like within the box is the second quartile or median (50th percentile), and the top side marks the third quartile (Q3, 75th percentile). The lines that extend from the top and bottom sides represent the range from the maximum to the minimum values, respectively. Thus, the plot is a visual representation of the distribution of the dataset, its outliers and its symmetry. Fifty percent of the sample under analysis is contained within the limits of the box, while the bounds of the whiskers include the values for the entire sample. Both the results of the three ways in which the total HRQoL score was computed (Figure 2) re-expressed on a scale of 1 to 100, and the results for the six dimensions under analysis in those participants in whom they could be assessed (Table 2), exhibited highly significant differences between both groups, with poorer outcomes in the ADHD group in every instance. The dimensions perceived most unfavourably in this group were physical well-being and self-esteem (mean scores of 61 points) and especially school (mean score of 45 points). The largest differences between the means obtained in either group were found in the dimensions of psychological well-being (20 points) and school (21 points).
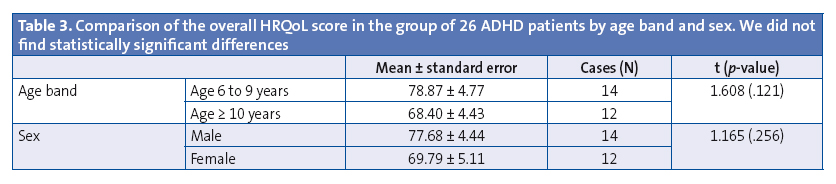
We also took the opportunity to analyse the possible influence of sex and age on the total score on HRQoL in the group of patients with ADHD (Table 3). When it came to sex, the comparison of HRQoL scores between both groups did not find significant differences (t = 1.165, P = .256). As for age, we divided the group in two age bands. The younger age band comprised children with an ADHD diagnosis aged 6 to 9 years. The older age band included children aged 10 or more years. The comparison of the mean HRQoL scores of the two groups also found no significant differences between them (t = 1.608, P = .121).
DISCUSSION
One singularity of this study is that we administered the questionnaire to the children rather than their parents or caregivers. It is important to highlight that the concept of HRQoL is based in the subjective and the individual. Although it is reasonable to wonder whether the concentration difficulties and changes in executive functioning experienced by children with ADHD could pose a challenge to introspection in the context of completing questionnaires, we thought it was important for children to complete the questionnaire themselves rather than inferring their responses from the perspective of an adult, since HRQoL is what is perceived by the individual him or herself, and as we noted above there are several validated instruments for its measurement in the paediatric age group.
Previous studies have highlighted differences in perceived HRQoL in ADHD between affected children and their parents. One study14 found that children with ADHD rated their HRQoL less favourably than their parents. Another one15 demonstrated that there was little agreement between parents and children in their perception of the impact of ADHD in HRQoL.
There are published studies that assess child quality of life in which children themselves completed the KINDL® questionnaire.16
Another aspect to consider is the impact of ADHD on the quality of life of affected children. The LIS study17 assessed the repercussions of ADHD and how it could negatively and profoundly impact social and family relationships in the day-to-day life of affected children. The study was conducted in six European countries (United Kingdom, France, Germany, Italy, Netherlands and Spain) by means of an extensive online survey. In this study, questionnaires were filled out by parents and caregivers of children with and without ADHD, and by adults with and without ADHD. Sixty percent of caregivers considered that ADHD had a direct impact on the self-esteem of children. In the LIS study, school was the most frequently impaired area.
The results of our study corroborate these findings. Psychological well-being, family and school were the three dimensions that patients perceived as being most affected. Quality of life was rated lowest for the school dimension in both groups, while still being rated significantly lower by children with ADHD, constituting one of the largest differences in comparison to children in the control group.
We ruled out potential bias from the sociocultural context and family educational attainment by verifying that the distribution of the Graffar classifications was equivalent in both groups. Sex also did not seem to influence the answers to the questionnaire in the group of children with ADHD, and neither did age group, which indirectly demonstrates the validity of the KINDL® questionnaire.
There is an electronic version of the KINDL® known as the CAT-SCREEN. It is designed for younger children. The psychometric properties of this electronic version have not been assessed in full, which is why we could not use it in this study.
In conclusion, quality of life is impaired in patients with ADHD, as has been suggested and reported by other authors.
CONCLUSIONS
Children with a new diagnosis of ADHD have a less favourable perception of their quality of life compared to children without ADHD. We found significant differences between the two groups in all the dimensions analysed. We can conclude that overall, patients with ADHD perceive their life quality as significantly impaired compared to children without ADHD. Physical well-being, self-esteem and school are the aspects perceived most negatively.
We found the largest differences between the two groups in the psychological well-being, family and school dimensions. Therefore, the alertness of PC paediatricians to family dynamics and academic difficulties is of great importance in suspecting the presence of ADHD through these effects in the context of the patient’s immediate relational environment.
New tools that take into account the perspective of the patient are needed in primary care paediatrics. Measures of HRQoL have proven to be very useful for the purpose of diagnosis and to assess patient needs. It is important that the assessment of HRQoL is included in the management of children with ADHD to evaluate its impact and analyse the dimensions of everyday life that are most affected, in order to develop more specific interventions and improve their well-being. Any intervention in children, be it in the school, family or health care setting, should take into account the areas which children consider important in everyday satisfaction and consider whether those needs and goals are being addressed.
The presence of ADHD has a direct impact on the lives of patients and influences how children perceive life.
Considering the evidence obtained from our study and the medical literature, the challenge facing PC paediatricians is to attempt the early and effective detection and treatment of ADHD with the purpose of minimising the impact that this disorder has on the quality of life of the patients that suffer it and their environment. Improving quality of life in children with ADHD sets a solid foundation for future well-being.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation with the preparation and publication of this study
This study was presented as a poster at the 22 Congress of the International Society of Quality of Life Research (ISOQOL) held in Vancouver (Canada) in October 2015.
ABBREVIATIONS: ADHD: attention deficit hyperactivity disorder · HRQoL: health-related quality of life · IC: informed consent · PC: Primary Care · PCC: Primary Care Centre · QoL: Quality of Life · Red IRYSS: Red de Investigación cooperativa para la Investigación en Resultados de Salud y Servicios Sanitarios WHO: World Health Organization.
ACKNOWLEDGMENTS
We thank all the children and families that were willing to participate in this study.
REFERENCES
- Polanczyk G, Silva M, Lessa B, Biederman J, Rohde LA. The worldwide prevalence of ADHD: a systematic review and meta-regression analyses. Am J Psychiatry. 2007;164:942-8.
- Fernández M, Eddy LS, Rodríguez L, Txakartegi X. El trastorno por déficit de atención e hiperactividad y la Atención Primaria: pasado y perspectivas. Rev Pediatr Aten Primaria. 2007;9:S101-12.
- Young S, Fitzgerlad M, Postma MJ. ADHD: making the invisible visible. En: Russell A. Barkley, Ph.D. [en línea] [consultado el 06/03/2017]. Disponible en org/factsheets/ADHD_MakingTheInvisibleVisible.pdf
- Lora A. El tratamiento del niño y adolescente con TDAH en Atención Primaria desde el punto de vista de la evidencia. Rev Pediatr Aten Primaria. 2006;8:S69-114.
- Organización mundial dela Salud. Basic documents. Ginebra: OMS; 1948.
- Kaplan RM, Bush JW. Health related quality of life measurement for evaluation research and policy analysis. Health Psychol. 1982;1:61-80.
- Quiceno JM, Vinaccia S. Calidad de vida relacionada con la salud infantil: una aproximación desde la enfermedad crónica. Avances de la disciplina. 2013;7 69-86.
- Servera M, Cardo E. ADHD rating scale-iv en una muestra escolar española: datos normativos y consistencia interna para maestros, padres y madres. Rev Neurol. 2007;45:393-9.
- Pane S, Solans M, Gaite L, Serra-Sutton V, Estrada MD, Rajmil L. Revisión sistemática de la literatura: actualización sobre Instrumentos de calidad de vida relacionada con la salud en la edad pediátrica. Barcelona: Agència d’Avaluació de Tecnologia i Recerca Mèdiques; 2006.
- Rajmil L, Estrada MD, Herdman M, Serra-Sutton V, Alonso J. Calidad de vida relacionada con la salud (CVRS) en la infancia y la adolescencia: revisión de la bibliografía y de los instrumentos adaptados en España. Gac Sanit. 2001;15:S34-43.
- Fernández-López JA, Fernández M, Cieza A, Ravens-Sieber U. Medición de la calidad de vida en niños y adolescentes: comprobación preliminar de la validez y fiabilidad de la versión española del cuestionario KINDL. Aten Primaria. 2004;33:434-42.
- Rajmil L, Serra Sutton V, Fernández-López JA, Berra S, Aymerich M, Cieza A, et al. Versión española del cuestionario alemán de calidad de vida relacionada con la salud en población infantil y de adolescentes: el Kindl. An Pediatr (Barc). 2004;60:514-21.
- IMIM-IMAS. BiblioPRO [en línea] [consultado el 06/03/2017]. Disponible en www.bibliopro.org
- Danckaerts M, Sonuga-Barke EJ, Banaschewski T, Buitelaar J, Döpfner M, Hollis C, et al. The quality of life of children with attention deficit/hyperactivity disorder: a systematic review. Eur Child Adolesc Psychiatry. 2010;19:83-105.
- Rajmil L, Estrada MD, Herdman M, Serra-Sutton V, Tebé C, Izaguirre J, et al. Concordancia entre padres e hijos en la calidad de vida relacionada con la salud en niños con trastorno por déficit de atención con hiperactividad: estudio longitudinal. An Pediatr (Barc). 2009;70:553-61.
- Verdugo MA, Sabeh EN. Evaluación de la percepción de calidad de vida en la infancia. 2002;14:86-91.
- Caci H, Doepfner M, Asherson P, Donfrancesco R, Faraone SV, Hervas A, et al. Daily life impairments associated with self-reported childhood/adolescent attention-deficit/hyperactivity disorder and experiences of diagnosis and treatment: results from the European Lifetime Impairment Survey. Eur Psychiatry. 2014;29:316-23.