
Vol. 18 - Num. 71
Original Papers
Food and exercise habits in teenagers
María Alfaro Gonzáleza, Marta Esther Vázquez Fernándezb, Ana Fierro Urturic, Luis Rodríguez Molinerod, M.ª Fe Muñoz Morenoe, B Herrero Bregónf
aServicio de Pediatría. Hospital Medina del Campo. Valladolid. España.
bPediatra. CS Arturo Eyries. Facultad de Medicina. Universidad de Valladolid. Valladolid. España.
cPediatra. CS Pisuerga. Arroyo de la Encomienda. Valladolid. España.
dServicio de Pediatría. Hospital Recoletas Campo Grande. Valladolid. España.
eUnidad de Investigación Biomédica. Hospital Clínico Universitario de Valladolid. Valladolid. España.
fMIR-MFyC. CS Arturo Eyries. (Área Oeste). Valladolid. España.
Correspondence: M Alfaro. E-mail: mariaalfaro28@hotmail.com
Reference of this article: Alfaro González M, Vázquez Fernández ME, Fierro Urturi A, Rodríguez Molinero L, Muñoz Moreno MF, Herrero Bregón B. Food and exercise habits in teenagers. Rev Pediatr Aten Primaria. 2016;18:221-9.
Published in Internet: 12-09-2016 - Visits: 26859
Abstract
Objective: to study the characteristics of diet and exercise in adolescents enrolled in school in the province of Valladolid.
Methods: a broad survey was conducted anonymously and auto filled by 2412 students from 13 to 18 years old, extracting data related to food and exercise from March to May 2012.
Results: the 79.2% of adolescents had breakfast daily in contrast to the 4% that never breakfasted. The 45.2% referred to consume fruit daily, taking cooked or raw vegetables at least twice a week, the 31.9% and the 62.6% respectively, and the 92.4% ate legume at least once a week. The 10.7% did not ever consume fish. Regarding to unhealthy foods, the 10.5% drank soft or fizzy drinks daily, the 7.2% ate snacks and sweets and the 4.5% ate chips. The 62.4% of these teenagers felt that their weight was adequate but the 30.2% had ever gone on a diet in some occasion. Inducing vomiting, taking laxatives or diuretics to lose weight was ever used by the 7.7% of them and the 1.6% used these methods once a day or frequently. Regarding to exercise, the 95.8% exercised daily and the 69.6% at school.
Conclusions: we found problems in the habits of feeding and exercise for teens. It is important to carry out promotional campaigns for healthy habits.
Keywords
● Adolescents ● Diet-therapy ● Eating disorders ● Physical exerciseINTRODUCTION
Adolescence is a stage of life with increased essential nutrient requirements (energy, proteins, vitamins and minerals) and during which a diet of high nutritional quality becomes particularly important. Healthy nutrition during childhood and adolescence promotes optimal growth and development, prevents immediate health problems, such as iron deficiency, anaemia, obesity, eating disorders and tooth decay, and may also contribute to the prevention of health problems in the long term, such as coronary heart disease, obesity, cancer, hypertension and osteoporosis.1 Furthermore, the dietary habits developed during adolescence (those that promote health as well as those that put it at risk) will become routine during adulthood.
The prevalence of overweight and obesity in childhood and adolescence has become one of the issues that most concern public health authorities. In fact, the World Health Organization (WHO)2 urges the promotion of healthy lifestyles in these developmental stages as the key to stop what it calls the rapid and progressive epidemic of obesity. More specifically, the data for the past few years of the Health Behaviour in School-Aged Children (HBSC) cross-national study has shown that Spain is among the countries with the highest prevalences of obesity in adolescents.3,4
In this context, the objectives of our study were to assess diet-related habits in adolescents and their association with other factors, and to detect associated behavioural disorders or maladaptive behaviours, with the purpose of establishing dietary and physical activity recommendations for adolescents.
MATERIALS AND METHODS
Sample universe
The sample universe consisted of secondary education students aged 13 to 18 years enrolled in schools or educational centres that offer years 2, 3 and 4 of the Secondary Compulsory Education (Enseñanza Secundaria Obligatoria [ESO]) and 1 and 2 of the Spanish Baccalaureate (Bachillerato) as specified in the Spanish Educational Law (Ley Orgánica General del Sistema Educativo [LOGSE]).
Sample
Students were selected by two-stage cluster sampling, selecting schools at random (n = 14) and then including all students in the selected classrooms. We estimated the sample size required for an estimated proportion of 50% and a precision of 2.5% in two-tail tests, assuming a nonresponse rate of 10%, and obtained a size of 2412 students.
Questionnaire and fieldwork
We used a questionnaire made of items validated in previous projects at the international,5,6 national,7,8 autonomous community and province9-11 levels. It consisted of 101 questions pertaining to sociodemographic variables, alcohol use, academic performance, entertainment and leisure, accidents, tobacco use, drug use, behaviour, experience of abuse, interpersonal relationships, diet and sexual activity. The questionnaires were filled on a voluntary and anonymous basis during regular school hours. The time spent completing the questionnaire ranged between 35 and 40 minutes. All questionnaires were administered between March and May of 2012. This study presents the findings pertaining to diet and physical activity.
Statistical analysis
We have expressed quantitative variables as averages and 95% confidence intervals, and qualitative variables as frequency distributions. We used Pearson’s chi square test to analyse the correlation of dietary and physical activity habits with sociodemographic characteristics. When the percentage of cells with expected frequencies of less than five exceeded 20%, we used Fisher’s exact test or the likelihood ratio for variables with more than two categories. We analysed the data using SPSS® version 19.0 for Windows®. Statistical significance was defined as P < .05.
RESULTS
Of a total of 2412 valid questionnaires, 47.3% corresponded to females and 52.7% to males. When it came to the school year, 23.5% of participants were enrolled in year 2 of the ESO, 25.8% in year 3 of the ESO, 20.2% in year 4 of the ESO, 18.9% in year 1 of Bachillerato and 11.6% in year 2 of Bachillerato.
When it came to breakfast, the number of days a week that adolescents reported having breakfast were: every day, 79.2%; four to six days a week, 4.9%; one to three times a week, 4.5%; only on weekends, 7.4%. Four percent reported never having breakfast. A higher percentage of male respondents compared to female respondents reported having breakfast (84.1% vs 73.7%; P < .001). Lastly, we found that the frequency with which respondents had breakfast decreased with increasing school year: 81.7% of adolescents in year 2 of the ESO had breakfast daily compared to 75.7% of adolescents in year 2 of the Bachillerato, although the differences we found were not statistically significant (P = .127). The foods consumed at breakfast were milk or dairy products (89.3%), cereal (45.1%), pasta, biscuits or madeleine cakes (44.6%), fruit or juice (22.9%), bread or toast (22.1%) and other foods (7.9%).
We went on to analyse the consumption of the basic food groups by sex, school year and socioeconomic status. Table 1 shows the percentages corresponding to each answer choice (none, once a week, several times a week, every day) for the consumption of foods by sex. We did not find statistically significant differences in the consumption of any type of food by school year. However, we did find an association between high socioeconomic status (determined by the Family Affluence Scale)12 and more frequent consumption of dairy products, vegetables (raw and cooked) and salads, fruit and fish, with no differences in the remaining foods.
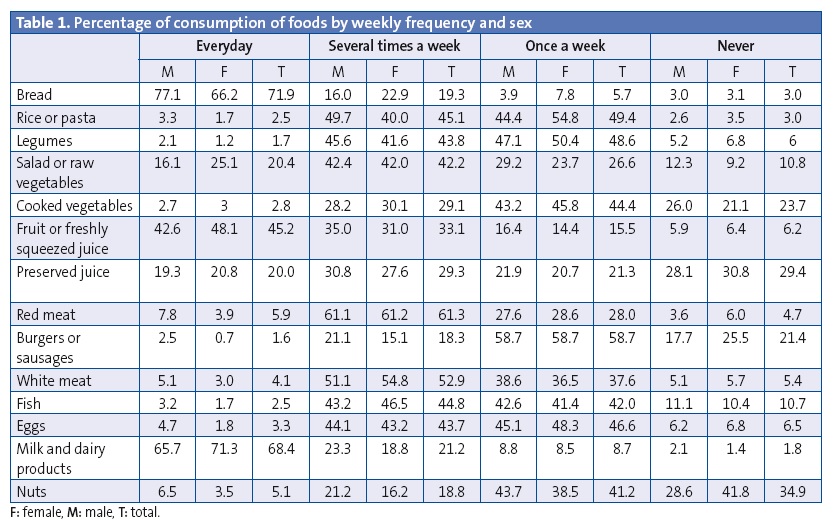
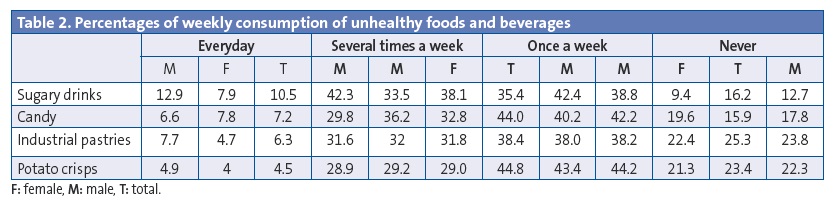
Table 2 summarises the data on unhealthy foods and beverages, showing the percentage of adolescents that consumed sugary drinks, candy, industrial pastries, sweet desserts and potato crisps by sex. We found no differences based on school year or socioeconomic level, except in the consumption of sugary drinks, which was significantly associated with low socioeconomic status.
Of all participants, 30.1% reported having been on a diet. The main reason for dieting was losing weight (77.5%), and dieting was reported more frequently by female than by male adolescents, a difference that was statistically significant (82. vs 68.6%; P < .001). We did not find significant correlations between dieting and school year or socioeconomic status. Also, 25.2% of those that dieted did it to have a healthier lifestyle, 11.7% for weight maintenance, 5.5% due to health problems or diseases, and 7.2% for other reasons.
As for symptoms of eating disorders, we found that 7.7% of the sample reported having used laxatives, diuretics or self-induced vomiting at least once in order to lose weight. This was found more frequently in female than in male adolescents (11.7% vs 4.2%; P < .001). These measures were used daily or frequently by 1.6%. We found no differences based on school year or socioeconomic level.
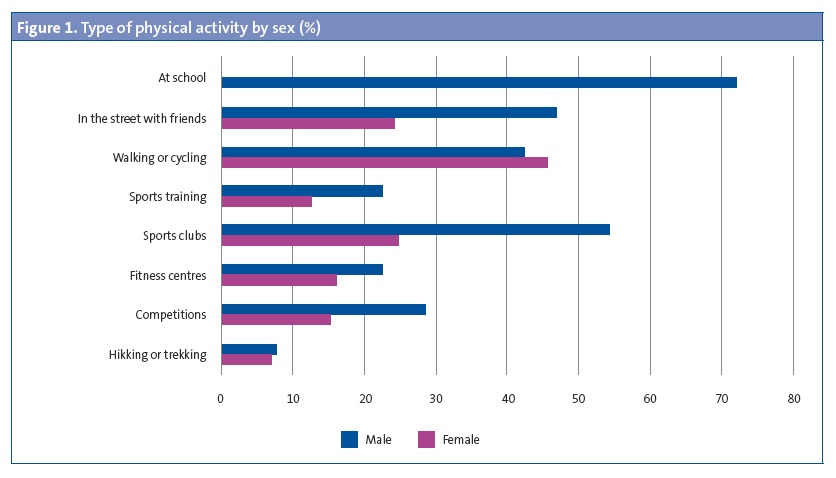
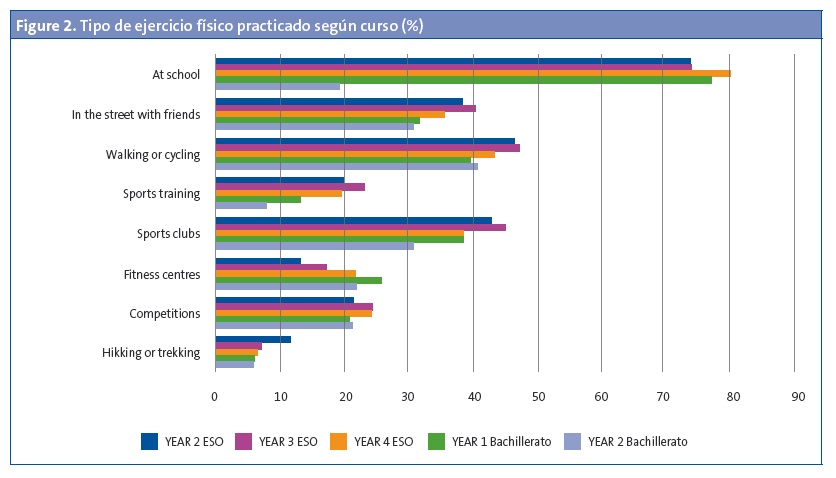
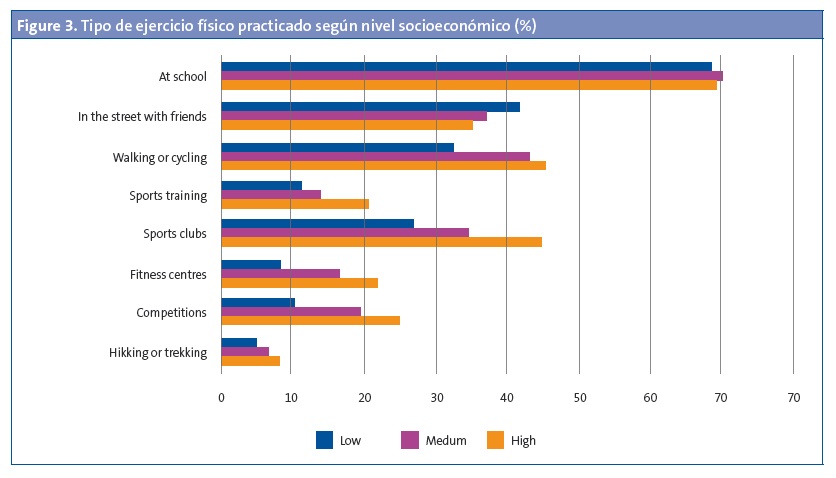
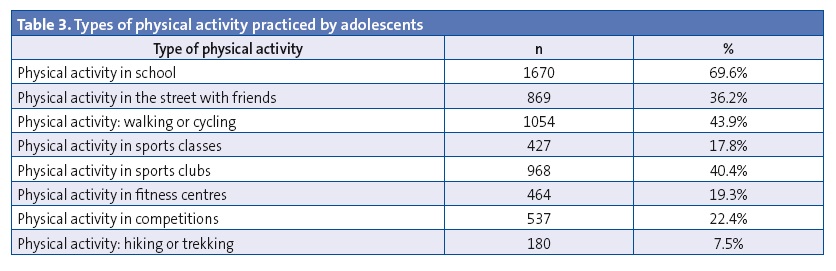
Last of all, we analysed physical activity, and found that 95.8% of participants were active daily. A higher percentage of female adolescents reported not exercising compared to male adolescents (5.8% vs 2.8%; P < .001). We observed a decrease in physical activity in students enrolled in higher years (15.5% of students in year 2 of Bachillerato reported not exercising compared to 3% of students in year 2 of the ESO). Lack of physical activity was also more frequent in adolescents of lower socioeconomic status (9.3% vs 3.7%; P = .02). Figures 1, 2 and 3 and Table 3 summarise the types of physical activity and the settings in which it took place. The practice of competitive sports was more frequent in male than in female adolescents (28.7% vs 15.4%; P < .001) and in adolescents of higher socioeconomic status (24.9% vs 10.2%, P < .001).
DISCUSSION
The type of foods consumed by adolescents is critical to their development. Breakfast is the main meal of the day, as it recharges the energy stores and helps adolescents face the day. Extensive research suggests that skipping breakfast or inadequate intake during breakfast contribute to an inadequate diet. This is supported by the findings of the Healthy Lifestyle in Europe by Nutrition in Adolescence project (HELENA)13 and the Dortmund Nutritional and Anthropometric Longitudinally Designed study (DONALD), the Ghent group and the Spanish AVENA study. In our study, 79.2% of adolescents reported having breakfast every day, compared to 53.4% in the nationwide HBSC study, and the proportion was larger in males than in females in both studies.
Dairy products are a good source of minerals due to their high calcium, phosphorus and magnesium content. The recommended daily calcium intake requires consumption of at least three servings of dairy products a day. In our study, only three out of four adolescents consumed these amounts daily, and the proportion was higher in females and in adolescents of higher socioeconomic status. It is important that these data are taken into account so that health education targets the subsets of the population that show poorer compliance.
Fruits constitute a particularly significant food group due to their high content of antioxidants, phytochemicals and dietary fibre, and consumption of these substances has been associated with lower incidences of health problems such as cancer, cardiovascular disease, diabetes, diverticulitis etc. When it came to fruit intake in adolescents, our results showed optimal intake with fruit consumed daily in nearly half of respondents, a percentage that was higher than those reported in other studies, such as the HBSC study, in which only 36% reported consuming fruit daily. The percentage of adolescents that reported never eating fruit was 6.2%. We did not find an inverse correlation between age and optimal consumption of fruit, as has been reported by the HBSC study. However, our results were consistent in that we found a higher consumption of fruit in female adolescents. When it came to family affluence, we observed that adolescents in families of higher socioeconomic status consumed more fruit, and the lack of consumption was found more frequently in families of lower socioeconomic status, which is probably not only due to a lower purchasing power, but also to a lack of knowledge of healthy habits.
Vegetables are usually not a food favoured by adolescents, and if adequate nutrition has not been taught from an early age, they are likely to prefer other types of foods, usually in the carbohydrate group. Their choices are influenced by packaging, flavours and advertising. The data in our study showed that consumption of vegetables was more frequent in adolescents of higher socioeconomic status and females, which is consistent with the findings of the HBSC study.
Nearly half of the surveyed adolescents consumed fish several times a week, and this was more frequent in adolescents with higher socioeconomic status and similar in both sexes. However, we found that one in ten adolescents did not eat fish. While fish is one of the food groups associated most frequently with allergic reactions, this factor does not seem to justify the high proportion of adolescents that did not eat fish in our sample. In the HBSC study, fish intake has been increasing in recent years.
The consumption of sweets, sugary drinks and salty foods should be occasional and in moderate amounts, since in general they are superfluous foods whose intake is not necessary and that carry a risk, when consumed in excess, of developing excess weight and tooth decay. However, it is common for adolescents in our population to consume them several times a week and even daily, as demonstrated by the results of our study. Slightly more than 10% consumed sugary drinks every day. The HBSC study14 shows that most adolescents consume sweets several times a week (although the frequency of daily consumption has been decreasing), something that is more frequent in adolescents that are female or of low socioeconomic status. We did not find differences between sexes or adolescents of different socioeconomic status, except in the consumption of industrial pastries, which was more frequent in males, and of sugary drinks, which was more frequent in adolescents of low socioeconomic status.
Body image matters greatly to adolescents, and therefore maintaining an adequate weight is particularly important to them. In our study, 22.4% of participants believed that their weight exceeded the normal range, compared to 30% in the HBSC study, and this belief was more frequent in females in both studies. However, the percentage of adolescents that reported having been on a diet was 30%, which indicates that there was a high proportion (especially in female adolescents) that dieted despite not having excess weight. The most frequent reason for dieting was weight loss, and disease or health problems were much less frequent.
In our sample, 7.7% of adolescents had symptoms of eating disorders, as they reported having induced vomiting or used laxatives at least once, with 1.6% reporting doing it daily or frequently. The SIVFRENT study,15 conducted in 2009 in adolescents residing in Madrid, found lower percentages (3.7%), although these disorders were also more frequent in the female sex. The female beauty standards promoted by the mass media probably contribute to the development of these eating disorders.
Physical activity during childhood and adolescence has physical benefits, but also provides opportunities for social interaction and for developing self-esteem and mental health.16 Most adolescents in our study engaged in physical activity, with a significantly higher proportion of males and a significant decrease in higher school years. Our findings are consistent with those of previous research.7,8 As adolescents grow older, and especially after puberty, they start to go out more and to devote more time to studying and entertainment; some of them may quit sports that they used to practice in school or at sports facilities, especially when the habit of exercising was not fully established. On the other hand, lower socioeconomic status was associated with lower physical activity, which may be due not only to the financial factor, which should not necessarily influence the practice of at least some sports, but also to parents not playing sports or being unaware of the benefits provided by healthy lifestyles and, in any case, not having been able to establish the habit of exercise in their children.17 At present, there is widespread consensus that increasing physical activity and decreasing sedentary habits should be the main goals of health promotion strategies that target children and adolescents.18-20
CONCLUSIONS
Dietary habits in a significant proportion of adolescents were inadequate, mostly due to skipping breakfast and not adhering to nutritional recommendations (failure to consume dairy products, fruits and vegetables on a daily basis, and nearly daily consumption of unhealthy foods and beverages). We also found eating disorders and decreased physical activity, mainly in older adolescents and female adolescents. In order to minimise these risks, we need to promote healthy dietary habits in adolescents and their families.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article. This study was funded by the AEPap.
ABBREVIATIONS: DONALD: Dortmund Nutritional and Anthropometric Longitudinally Designed · ESO: Enseñanza Secundaria Obligatoria · HBSC: Health Behaviour in School-aged Children · HELENA: Healthy Lifestyle in Europe by Nutrition in Adolescence · LOGSE: Ley Orgánica General del Sistema Educativo · WHO: World Health Organization.
REFERENCES
- Guidelines for school health programs to promote lifelong healthy eating. J Sch Health. 1997;67:9-26.
- World Health Organization. Which health problems affect adolescents and what can be done to prevent and respond to them? Child and adolescent health and development. Copenhague: WHO Regional Office for Europe; 2009.
- Haug E, Rasmussen M, Samdal O, Iannotti R, Kelly C, Borraccino A, et al. Overweight in school-aged children and its relationship with demographic and lifestyle factors: results from the WHO-Collaborative Health Behaviour in School-aged Children (HBSC) study. Int J Public Health. 2009;54:167-79.
- Agencia Española de Seguridad Alimentaria. La seguridad alimentaria en la Educación Secundaria Obligatoria. Guía didáctica. Madrid: Ministerio de Sanidad y Consumo; 2003.
- Brooks F, Van der Sluijs W, Klemera E, Morgan A, Magnusson J, Gabhainn SC, et al. Young people’s health in Great Britain and Ireland. Findings from the Health Behaviour in School-Aged Children Study 2006. HBSC International Coordinating Centre, University of Edinburgh. 2006.
- California Health Interview Survey (CHIS). Adolescent Questionnaire 2009. In: Universidad de California [online] [consulted on 07/09/2016]. Available in http://healthpolicy.ucla.edu/chis/design/Documents/CHIS2009teenquestionnaire.pdf
- Moreno-Rodríguez C, Muñoz Tinoco V, Pérez Moreno PJ, Sánchez Queija I, Granado Alcon MC, Ramos Valverde P, et al. Desarrollo adolescente y salud. Resultados del estudio HBSC 2006 con chicos y chicas españoles de 11-17 años. In: HBSC España [online] [consulted on 07/09/2016]. Available in http://grupo.us.es/estudiohbsc/index.php/es/
- Nebot M, Pérez A, García-Continente X, Ariza C, Espelt A, Pasarín M, et al. Informe FRESC 2008. Resultats principals. Barcelona: Agència de Salut Pública de Barcelona; 2010.
- Consejería de Salud y Servicios Sanitarios. Encuesta de Salud Infantil en Asturias 2009. Oviedo: Consejería de Salud y Servicios Sanitarios del Principado de Asturias; 2010.
- Schiaffino A, Moncada A, Martín A. Estudi EMCSAT 2008. Conductes de salut de la població adolescent de Terrassa, 1993-2008. Terrassa: Ajuntament de Terrassa; 2009.
- Departamento de Salud, Gobierno Vasco. Encuesta de Salud del País Vasco 2013. Vitoria: Departamento de Salud, Gobierno Vasco; 2014.
- Boyce W, Torsheim T, Currie C, Zambon A. The Family Affluence Scale as a measure of national wealth: validation of an adolescent self-report measure. Soc Indic Res. 2006;78:473-87.
- Moreno LA, Kersting M, De Henauw S, González-Gross M, Sichert-Hellert W, Matthys C, et al. How to measure dietary intake and food habits in adolescence: the European perspective. Int J Obes (Lond). 2005;29:S66-77.
- Moreno C, Ramos P, Rivera F, Jiménez-Iglesias A, García I. Las conductas relacionadas con la salud y el desarrollo de los adolescentes españoles. Resultados del estudio HBSC-2010 con chicos y chicas españoles de 11 a 18 años. in: Ministerio de Sanidad, Servicios Sociales e Igualdad [online] [consulted on 07/09/2016]. Available in www.msssi.gob.es/profesionales/saludPublica/prevPromocion/promocion/saludJovenes/docs/HBSC2010_Resumen.pdf
- Díez-Gañán L. Hábitos de salud en la población juvenil de la Comunidad de Madrid 2013. Resultados del Sistema de Vigilancia de Factores de Riesgo asociados a Enfermedades No Transmisibles en población juvenil (SIVFRENT-J). Año 2013. Boletín Epidemiológico de la Comunidad de Madrid. Madrid: Consejería de Sanidad; 2014.
- Santaularia A. Actividad física y salud. Beneficios de la práctica de ejercicio. Aten Primaria. 1995;15:574-9.
- Ministerio de Sanidad, Servicios Sociales e Igualdad. Informe Juventud en España 2012. INJUVE. In: Instituto de la Juventud online] [consulted on 07/09/2016]. Available in www.injuve.es/sites/default/files/2013/26/publicaciones/IJE2012_0.pdf
- Healthy People 2010 final review. In: National Center for Health Statistics [online] [consulted on 07/09/2016]. Available in www.cdc.gov/nchs/data/hpdata2010/hp2010_final_review.pdf
- Tammelin T, Näyhä S, Laitinen J, Rintamäki H, Järvelin MR. Physical activity and social status in adolescence as predictors of physical inactivity in adulthood. Prev Med. 2003;37:375-81.
- Ortega F, Ruiz J, Castillo MJ, Moreno LA, González-GrosS M, Wärnberg J, et al. Bajo nivel de forma física en los adolescentes españoles. Importancia para la salud cardiovascular futura (Estudio Avena). Rev Esp Cardiol. 2005;58:898-909.