
Vol. 18 - Num. 70
Original Papers
The active search of patients improves vaccination coverage
Laia Bort Llorcaa, Laura Pérez Ollerob, Javier Soriano Faurab
aMIR-Medicina de Familia. CS Fuensanta. Valencia. España.
bPediatra. CS Fuensanta. Valencia. España.
Published in Internet: 16-06-2016 - Visits: 15362
Abstract
Objective: improve vaccination coverage in the health center Fuensanta by actively seeking improperly vaccinated patients.
Material and methods: design: single-blind clinical trial. Location: pediatric patients of health center Fuensanta. Participants: 736 patients, 401 in the intervention group and 335 in the control group. 28 patients who did not attend the CS in 24 months prior to the study and 2 refused to be vaccinated. Interventions: search active involvement of patients incorrectly vaccinated by telephone, letter and alarms in Computerized Medical Record and observation of vaccination status in the control group.
Main measurements: variables: immunization status at the end of the study period; age; control group or the intervention group. Relative risk (RR), absolute risk reduction (ARR) and number needed to treat (NNT) was calculated. Results: overall improvement in the intervention group of 3.59 RR (95% CI: 2.07 to 6.22); RR 6.30 (95% CI: 1.72 to 23.10) at 3 years and RR 6.44 (95% CI: 1.38 to 29.96) at 6, with improvement, statistically not significant, at 14 (p 0.07), RR 2.22 (95 % CI: 0.90 to 5.43). Effect of active search at 3, 6 and 14: RRA 89.3% (95% CI 71.99 to 97.1) and NNT 1.11, RRA 81.1% (95% CI: 51.15 to 96, 01) and NNT 1.22; RRA 74.29% (95% CI 57.75 to 86.02) and NNT 1.33 respectively.
Conclusions: The active search was effective at 3 and 6 years. At 14, the active search, not being statistically significant, improved immunization status significantly.
Keywords
● Active search ● Vaccination ● Vaccination coverageINTRODUCTION
Vaccination is one of the public health primary care preventive measures that are most beneficial to the population: it prevents premature deaths and sequelae from vaccine-preventable diseases and epidemic outbreaks, and produces herd immunity in the population.1
Containing the socioeconomic burden of vaccine-preventable diseases depends directly on ensuring an adequate vaccination coverage.1
Vaccination rates are high in the paediatric population of Spain, as these patients require regular medical checkups in the early years of life that facilitate adherence to the immunization schedule, although it is also true that vaccine coverage rates decrease with increasing age.1-3
Our primary care health care centre (HCC) is located in the outskirts of the city of Valencia (Spain), and has two paediatrics offices that serve children from families of low-to-middle socioeconomic status. Our aim in this study was to improve vaccination coverage by actively seeking out patients of our HCC that were incorrectly vaccinated, and the main tools used for this purpose were electronic health records (EHRs), phone calls and postal mail.
MATERIALS AND METHODS
We conducted a single-blind study in patients of our HCC divided into five age groups (12 months, 18 months, 3 years, 6 years and 14 years) enrolled between October 2013 and October 2014 for a followup period of control or intervention of 12 to 24 months (ending in October 2015). We enrolled patients in the study after obtaining informed consent from them and/or their legal guardians.
The variables under study were correct or incorrect vaccination status based on the patient’s age group and the group to which they had been assigned at the time of enrolment in the study (intervention or control group), and the outcome variable of whether incorrect vaccination status was corrected by the end of the study period (24 months).
Twenty-eight patients were excluded from the study (twenty-six because they had not visited the HCC in the 24 months prior to the study, and two for refusing vaccination), and twenty dropped out of the study due to a change in address or transfer to a different HCC.
The caseloads of each of the Paediatrics offices constituted the intervention and control groups. The patients included in the two caseloads have similar characteristics.
In the intervention group (n = 401), incorrectly vaccinated patients were sought ought by phone, letters, and alerts in the EHR. The first step was to attempt a phone call to the parents or legal guardians. If they could not be reached by phone, a letter was sent by post, and an alert activated in the patient’s EHR to remind the paediatrician of this issue when the patient next visited the HCC.
In the control group (n = 335), we only observed the vaccination status of the patients until the end of the study, so that patients were only vaccinated if they attended the scheduled checkups or their families requested it.
We performed the statistical analysis with Excel® and SPSS® version 15.0, analysing contingency tables to determine the benefit, or risk ratio (RR), and the absolute risk reduction (ARR), and calculating the number needed to treat (NNT).
RESULTS
Our analysis included a total of 736 patients, of whom 388 (53%) were male. The percentage of correctly vaccinated patients was similar in both groups before the study started (no statistically significant difference).
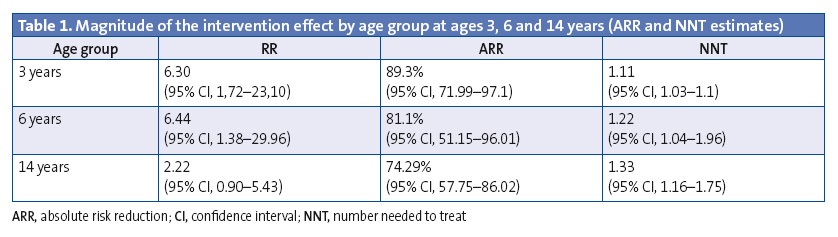
There was an overall improvement in vaccination coverage in the entire intervention group, with the benefit corresponding to a risk ratio (RR) of 3.59 (95% confidence interval [IC], 2.07–6.22); the RR was 6.30 in the 3-year-old group (95% CI, 1.72–23.10) and 6.44 in the 6-year-old group (95% CI, 1.38–29.96).
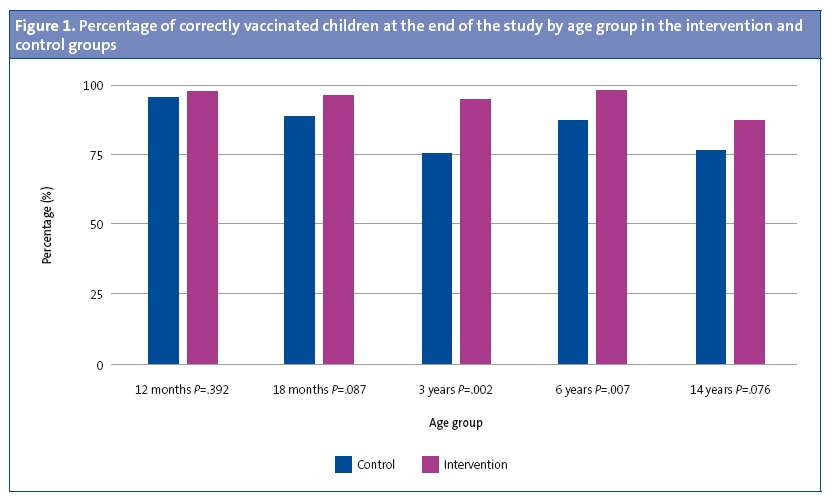
In the 14-year-old group the RR was 2.22 (95% CI, 0.90–5.43), which was not statistically significant (P = .076).
We did not find statistically significant differences between the intervention and the control group at ages 12 and 18 months.
Figure 1 shows the vaccination coverage percentages for each age group in the intervention and control groups.
In the groups of patients aged 3, 6, and 14 years, the active search for those that were incorrectly vaccinated had a considerable effect. For instance, in the 3-year-old group the ARR was 89.3% (95% CI, 71.99–97.1), that is, out of every 100 incorrectly vaccinated children that we actively sought out, we succeeded in having 89 correctly vaccinated by the end of the study. The NNT for this group was 1.11 (95% CI, 1.03–1.1).
The magnitude of the effect of the intervention was substantial in the 3, 6, and 14 year old groups (Table 1).
DISCUSSION
In our study, the initiative of seeking out incorrectly vaccinated children achieved an improvement in vaccination coverage in children aged 3, 6 and 14 years.
An active search does not seem necessary in the first 18 months of life, as we observed high vaccination rates without any intervention. This can be explained by visits to the paediatric offices for well-child checkups. Other studies have found results similar to ours in children aged less than 24 months, and attributed to the same reason.4
Active searching is effective in the 3- and 6-year age groups. The magnitude of the effect of this intervention was highly significant, achieving an improvement in vaccination coverage. There was evidence of improvement in coverage in the 14-year age group, but the difference was not statistically significant.
We must maintain and further improve the vaccination coverage achieved in this study. One possible strategy is to promote the implementation of nationwide health education programmes.2,5-10. Another tool that has yet to be integrated in the Spanish National Health System is the use of emerging technologies,11-14 such as getting in touch with parents through email, developing new mobile applications relating to the immunisation schedule,15 or setting up individual alerts in the EHRs that would get activated in case of incorrect vaccination, bringing it to the attention of paediatricians, nurses and the administrative staff.16,17 The creation of a diagnosis of “incorrect vaccination status” would also be helpful, so it could be entered in EHRs when it is detected in a patient and quickly attract the attention of paediatricians and nurses.
Along with these strategies to improve vaccination coverage, some studies have proposed establishing objectives for health care providers at the beginning of each vaccination year to assess the outcomes achieved at the end of the year, a method that has proven to be effective in improving vaccination coverage rates.11
In this regard, something that is as important as measuring the magnitude of the impact of these interventions for improving patient recruitment and thus vaccination coverage is to attempt to identify factors interfering with the correct adherence to these objectives.3,12,14,17,18
The intervention analysed in this study could be an easily available tool in primary care settings and feasible in this type of facility, and can achieve a higher vaccination coverage.4,17,19 Its correct implementation requires commitment, motivation and organisation on the part of health care providers.12,17 There is evidence that health care professionals have an influence on parents as pertains the decisions to vaccinate their children1,2,5,17,18.
The ongoing economic crisis has changed public health policies, and the optimisation of resources is being prioritised. This study demonstrates a type of inexpensive primary care intervention that prevents the development, transmission and complications of infectious diseases.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
We conducted this study after obtaining the informed consent of all participants, and adhering to the protocols established by the Fuensanta HCC for accessing health records and for publications for the purposes of scientific research and divulgation.
ABBREVIATIONS: ARR: absolute risk reduction · CI: confidence interval · EHR: electronic health record · HCC: health care centre · NNT: number needed to treat· RR: relative risk.
ACKNOWLEDGMENTS
We want to thank the entire team of the Fuensanta health care centre in Valencia.
REFERENCES
- Borràs E, Domínguez A, Oviedo M, Batalla J, Salleras L. The influence of public or private paediatric health care on vaccination coverages in children in Catalonia (Spain). Eur J Public Health. 2008;19:69-72.
- Fierro A, Sanz M, Valverde D, López E, Mata M. Cobertura de vacunas no sistemáticas en Pediatría de un consultorio semiurbano de Valladolid. Acta Pediatr Esp. 2014;72:87-93.
- González R, Campins M, Rodrigo JA, Uriona S, Vilca LM. Cobertura de vacunación antigripal en niños con condiciones de riesgo en Cataluña. Enferm Infecc Microbiol Clin. 2015;33:22-6.
- Arrazola MP, de Juanes JR, García de Codes A. Conceptos generales. Calendarios de Vacunación sistemática del niño y del adulto en España. Impacto de los programas de vacunación. Enferm Infecc Microbiol Clin. 2015;33:58-65.
- Goncalves G, Frutuoso M, Ferreira M, Freitas M. A strategy to increase and assess vaccine coverage in the north of Portugal. Eurosurveillance. 2005;10:98-102.
- Vilella A, Bayas JM, Díaz MT, Guinovart C, Díez C, Simó D, et al. The role of mobile phones in improving vaccination rates in travelers. J Prev Med. 2004;38:503-9.
- Kreuter MW, Caburnay CA, Chen JJ, Donlin MJ. Effectiveness of invidually tailored calendars in promoting childhood inmmunization in urban public health centers. Am J Public Health. 2004;94:122-7.
- Wood DL; American Academy of Pediatrics Committee on Community Health Services; American Academy of Pediatrics Committee on Practice and Ambulatory Medicine. Increasing immunization coverage. American Academy of Pediatrics Committee on Community Health Services. American Academy of Pediatrics Committee on Practice and Ambulatory Medicine. Pediatrics. 2003;112:993-6.
- Cotter S, Ryan F, Hegarty H, McCabe T, Keane E. Immunisation: the views of parents and health professional in Ireland. Eurosurveillance. 2003;6:145-50.
- Roberts K, Dixon-Woods M, Fitzpatrick R, Abrams K, Jones D. Factors affecting uptake of childhood immunization: a Bayesian synthesis of qualitative and quantitative evidence. 2002;360:1596-9.
- Álvarez MJ. Estrategias para mejorar las coberturas vacunales en los Centros de Salud. In: Asociación Española de Vacunología [online] [consulted on 14/06/2016]. Available in www.vacunas.org/estrategias-para-mejorar-las-coberturas-vacunales-en-centros-de-salud
- Leandro SV, Hernández M, Cebrián I, Elizalde C, Orrico MA, Abeti MA. Vacunación infantil: Cobertura, conocimientos y actitudes de la población. Estudio en un Área de Salud. An Esp Pediatr. 1996;44:464-8.
- Martínez-Campillo F, Maura da Fonseca A, Santiago J, Verdú M, Serramia del Prisco A, Ibáñez Molina M, et al. Estudio de la cobertura vacunal e intervención con agentes de salud comunitarios en población infantil marginal gitana de Alicante. Aten Primaria. 2003;3:234-8.
- Martín S, Álvarez MJ, Sesmero MA, Martínez N, Gómez JJ. Aumento de cobertura de vacuna antigripal en pacientes menores de 65 años con factores de riesgo. Vacunas. 2006;7:4-10.
- Averhoff F, Linton L, Peddecord KM, Edwards CH, Wang W, Fishbein D. A middle school immunization law rapidly and substantially increases immunization coverage among adolescents. Am J Public Health. 2004;94:978-84.
- Glauber JH. The immunization delivery effectiveness assessment score: a better immunization mesure. Pediatrics. 2003;112:39-45.
- Findley SE, Irigoyen M, See D, Sanchez M, Chen S, Sternfels P, et al. Community-provider partnerships to reduce immunization disparities: field report from Northern Manhattan. Am J Public Health. 2003;93:1041-4.
- Kharbanda EO, Stockwell MS, Fox HW, Rickert VI. Text4Health: a qualitative evaluation of parental readiness for text message immunization reminders. Am J Public Health. 2009;99:2176-8.
- Antón F, Richart MJ, Serrano S, Martínez AM. Estrategias para mejorar la cobertura de la vacunación antigripal en Atención Primaria. Semergen. 2015;42:147-51.