
Vol. 17 - Num. 68
Original Papers
Overweight and obesity: what is our reality?, what reference do we use? The OBESGAL study
José Manuel Fernández Bustilloa, P Pereira Garcíab, María José Méndez Busteloc, Grupo Colaborativo Obesgald
aPediatra. CS Bertamiráns. Ames. A Coruña. España.
bPediatra. CS Milladoiro. Ames. A Coruña. España.
cPediatra. CS Oroso. Ames. A Coruña. España.
d4G. Antelo Rodríguez, C. Belo González, M. T. Calvo Lorenzo, M. F. Crespo Vázquez, I. Díaz-Cardama Sousa, C. A. Díaz Sánchez, J. M. Fernández Bustillo, M. Fernández Pérez, A. Fernández Pombo, S. Garabal Sánchez, C. García Cendón, C. Hernández Valencia, M.
Correspondence: JM Fernández. E-mail: josemanuel.fernandez.bustillo@sergas.es
Reference of this article: Fernández Bustillo JM, Pereira García P, Méndez Bustelo MJ, Grupo Colaborativo Obesgal. Overweight and obesity: what is our reality?, what reference do we use? The OBESGAL study. Rev Pediatr Aten Primaria. 2015;17:301-7.
Published in Internet: 23-11-2015 - Visits: 29092
Abstract
Introduction: obesity in children is a challenge for public health. Therefore, we conducted a comparative study of the results obtained in the present moment in our health area, to assess the nutritional status of children 2-15 years old who presented in different primary care centers, studying the prevalence of overweight, obesity and morbid obesity in our region and comparing them with previous studies nationwide.
Subjects and method: the study population is composed of a representative sample of 15,142 children, aged between 2 and 15 years. The medical records were reviewed and anthropometric data (weight, height and BMI) were collected from the controls in the Children's Health Program (Program do Neno San) to obtain a final sample of 12,643 individuals [6433 were collected (50.9%) boys and 6210 girls (49.1%)].
The prevalence of overweight and obesity was analyzed according to age and sex variables, establishing a cutoff corresponding to the p85 percentile (overweight) and p95 (obesity). To categorize the BMI, charts for age and sex of longitudinal growth study Orbegozo Foundation, contained in the medical record SERGAS (Galician Health), were used. Prevalence estimates were accompanied by the respective 95% confidence intervals (CI). Chi square test was used to compare qualitative variables. The data were analyzed using the statistical package SPSS for Windows, version 12.0.
We compared our results with those of previous studies: the enKid study (1988-2000), and Aladino study (2010-2011).
Results: the prevalence of overweight (9.3%) and obesity (9.7%) in our study is lower, overall, than that obtained in other studies of national reference: enKid (12.4 / 13.9%), Aladino (26.2 / 18.3%), etc., although it is difficult to make comparisons because the criteria used to define overweight and obesity are not the same, we do not use the same tables as a reference or the same cutoff.
Conclusions: the prevalence of overweight and obesity varies depending on the baseline study used, being in our case far from the "official" expected figure. It requires consensus and unified criteria (WHO, IOTF, Orbegozo, etc.) to establish the diagnosis of overweight or obesity using the BMI.
Keywords
● Growth ● Obesity ● Overweight ● PrevalenceINTRODUCTION
In recent decades, there has been a considerable increase in the prevalence of obesity in developed as well as developing countries, which led the 57th World Health Assembly to declare it “the 21st century epidemic” in May 2004 and to endorse the development of a global strategy on diet, physical activity and health.1 The Spanish Ministry of Health then began to implement its NAOS strategy for the prevention of obesity in 2005.2
Obesity is a widespread problem in the paediatric age group, a silent epidemic that poses a veritable challenge to public health, since according to estimates made by the WHO3 more than forty million children under five years of age were overweight in 2011, and the worldwide prevalence will rise to 11% by 2015 to seventy million children if current trends persist.4
Poor dietary habits, with a broad range of hypercaloric foods available for consumption, and changes in lifestyle (such as sedentary habits), combined with an increasingly evident genetic basis, seem to constitute the risk factors for the development of childhood obesity,5 which has a significant impact on future quality of life (morbidity and mortality) and health care costs. There has also been a considerable increase in severe obesity among children,6 with severe short- and long-term consequences for health (cardiovascular, metabolic, etc), and thus prevention is a global health priority, as the obese child is at high risk of obesity in adulthood.7
Our aim was to assess the current nutritional status of the population of children aged 2 to 14 years receiving services at various primary care centres and the prevalence of overweight and morbid obesity in the autonomous community of Galicia.
MATERIALS AND METHODS
We conducted a descriptive, retrospective and cross-sectional study between June and September of 2013. We reviewed the medical records of 15 142 children residing in the towns of Ames, A Estrada, Lousame, Lugo, Órdenes, Oroso, Santiago de Compostela and Tomiño of the Autonomous Community of Galicia, and collected data from check-up appointments corresponding to the Well Child Programme (Programa do Neno San).8 The health care system of Galicia (Servicio Galego de Saúde [SERGAS]) has an electronic medical records system implemented in all of its centres, and given the high coverage rate of the well child programme, the data we collected is representative of the current situation at the autonomous community level.
All measurements were performed by qualified personnel (paediatric nurses) in the paediatrics clinics of the aforementioned health care centres. Patients were measured in their underwear and barefoot, with the weight measured by means of calibrated scales accurate to 100 g, and the height with rigid, non-extensible wall-mounted stadiometers accurate to 0.1 cm with the patient standing on both feet and the head placed in the Frankfurt plane.
For each participant in the study, the following fields were filled out in an Excel® spreadsheet: date of birth, sex, weight, height, and date of examination. The final sample included 12 643 individuals (6433 boys [50.9%] and 6210 girls [49.1%]).
The body mass index (weight in kg/squared height in meters [BMI]) was calculated automatically in the same Excel® spreadsheet. To classify the BMI, we used the charts for the corresponding age and sex of the longitudinal growth study of the Fundación Orbegozo featured in the electronic medical records system of the SERGAS.9
Once the data were collected, the sample was stratified into three groups according to the age distribution established by the SERGAS:
- Children aged 2 to 4 years: 3726 (29.5%).
- Children aged 5 to 9 years: 5293 (41.9%).
- Children aged 10 to 14 years: 3614 (28.6%).
We analysed the prevalence of overweight and obesity by age and sex, establishing the cut-off points at the 85th percentile (overweight) and 95th percentile (obesity).
To calculate the prevalence of severe obesity we used the 99th percentile as the cut-off point, estimated as 120% of the 95th percentile (1.2 × 95th %ile) of the BMI for age,6 which gives values that approximate the data for the 99th percentile in the growth chart.
We calculated the corresponding 95% confidence intervals (CIs) for the estimated prevalences. We used the chi-squared test to compare qualitative variables. The data were analysed with the statistical software SPSS® for Windows®, version 12.0.
RESULTS
Our study (Table 1) found a prevalence of 9.7% for overall obesity and of 9.3% for overweight that rose to 19% if we calculated the combined prevalence of excess weight (overweight and obesity) , with the highest figures corresponding to the 10–14 years age group (11.2% overweight and 11.9% obesity). Analysing the groups separately we observed that excess weight increased progressively with age from 13% in the 2–4 years age group to 23.1% in the 10–14 years group.
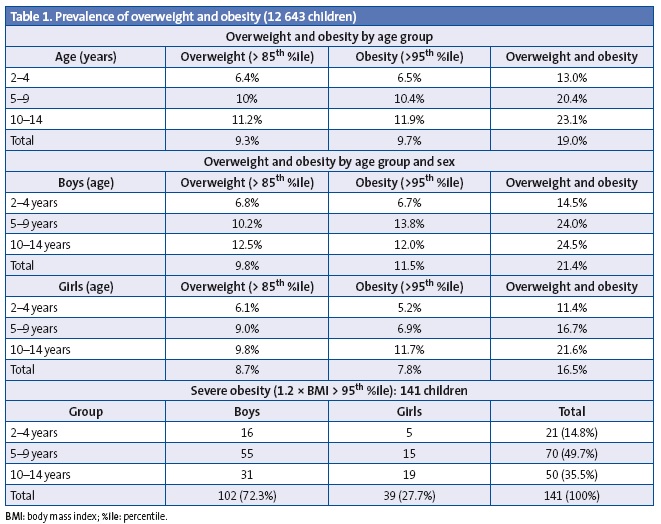
When we broke down the overall prevalences by sex and age (Table 1) we found differences between age groups both in the total and partial calculations. Thus, boys reached the highest prevalence of obesity, 13.8%, between ages 5 and 9 years; this percentage rose to 24% when obesity and overweight were combined, a trend that was sustained in the 10–14 years age group with a lower contribution from overweight. In girls, it was the 10–14 years age group that reached the highest prevalences of both overweight (9.8%) and obesity (11.7%), with the prevalence of obesity being similar to that of boys in the same age group (12%).
When we analysed obesity trends we found that its prevalence was lower in girls than in boys in all age groups.
When it came to severe obesity (Table 1) we found substantial differences between age groups and sexes. It was more frequent in boys (72.3% of the total cases of severe obesity) than in girls (27.7%), and this degree of obesity was more marked in the 5–9 age group, which accounted for 49.7% of the total cases, decreasing to 35.5% in the 10-14 years group; although we found a high percentage of 14.8% at early ages (2–4 years).
DISCUSSION
Obesity, which is considered “the 21st century epidemic”, has experienced a significant increase in recent decades, which is reflected by many studies conducted in Spain. Thus, the prevalence of childhood obesity rose from 4.9% in 1984, according to the Paidós study,11 to 13.9% between 1988 and 2000, as reported by the enKid study.12
However, the national population survey carried out by the Spanish Ministry of Health and Consumer Affairs in the 2006–2007 period in children aged 2 to 15 years13 found an overall prevalence of 10.3% using the BMI cut-off points recommended by the IOTF, which had dropped to 9.6% by the survey conducted in the 2011–2012 period.
During the 2010–2011 period, the Spanish Agency of Food Safety and Nutrition (Agencia Española de Seguridad Alimentaria y Nutrición [AESAN, currently known as AECOSAN]) carried out the Aladino study on diet, child development and obesity to estimate the prevalence of childhood obesity in boys and girls aged 6 to 9.9 years. Using the WHO standards as a reference, it estimated a prevalence of obesity of 20.9% in boys and 15.5% in girls, with an overall prevalence of excess weight, including obesity, of 44.5%, figures that significantly exceed those found in our study (Table 1).
The prevalence of obesity in our study was also lower than the prevalence found in the enKid nationwide reference study, which used the 85th and 97th percentiles of the Orbegozo tables to define overweight and obesity. Thus, for the population aged 2 to 24 years in the northern region of Spain (Galicia, Asturias, Cantabria, Basque Country, Navarra and La Rioja), the enKid study reported a prevalence of 12.7% for overweight and 12.3% for obesity. When looking separately at data for the paediatric age groups, the enKid study found the highest prevalences for overweight (14.6%) and obesity (16.6%) in the 10–13 years group, and these were even higher in boys, reaching 20.0% and 21.9%, respectively, which is consistent with the trends found in our study, although the percentages we found both overall (obesity,12.2%; overweight, 11.3%) and by sex were significantly lower. We ought to note that in our study, the prevalence of obesity was higher in girls than in boys in this age group, while in other age groups it was higher in boys. This has also been observed in other studies, such as one conducted in the Canary Islands,14 while others like the one conducted in Navarra found a higher prevalence in boys at these ages.15
Recent data suggests that the increasing trend in obesity in children and adolescents is slowing down,16 while the overall prevalence may have started to stabilize in recent years.17 This is corroborated by the Aladino study of 2013, which found a decrease in the prevalences of overweight and obesity compared to those found in previous years.18 Yet an alarming trend is emerging in severe childhood obesity, which has been increasing progressively in children and adolescents, reaching a prevalence of 4% to 6% in youth aged 6 to 19 years in the United States, with a severe impact on health, as it carries a higher risk of cardiovascular disease, diabetes mellitus type 2, and premature death in adulthood.19 The prevalence of severe obesity was substantially lower in our study, as it was found in only 141 children (1.1% of the total), which is consistent with a study conducted recently in Navarra that, applying the WHO standards, found obesity and severe obesity prevalences similar to those in our study (7.9% and 1.2%), but also a significantly higher prevalence of overweight (21%).20 Nevertheless, it is important to consider that a very high percentage of severe obesity cases corresponded to boys (72.3%), while in both sexes the highest percentage (49.7%) was found in the 5–9 years age group, decreasing slightly between ages 10 and 14 years. However, this problem is already found at early ages, if only in significantly lower numbers, and 14.8% of children with severe obesity are 2 to 4 years of age.
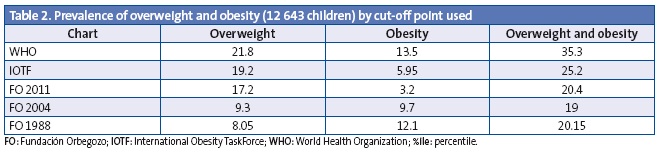
The assessment of obesity poses significant methodological challenges, as there is no consensus on the cut-off points to be used in its definition; since different tables are being used as a reference, the prevalence values also differ. To compare the results we obtained with those of previous studies we assessed the status of the patients according to the growth charts of the Fundación Orbegozo (FO),21 the criteria of the International Obesity Task Force (IOTF)22 and the WHO standards23 (Table 2).
The prevalence of obesity and overweight in Galicia is lower than in other regions; however, we observed that severe obesity was more prevalent in boys in all age groups.
It is essential to promote awareness of childhood obesity in the general population to prevent its prevalence from increasing, as only changes in lifestyle can lead to improvement. Primary care services play an essential role in the diagnosis and prevention of nutrition disorders. The Well Child Programme monitors children from birth to age 14 years, which allows for the early detection of childhood obesity and for early intervention. Thus, there is previous evidence that the most successful approach to obesity before adolescence may be to intervene on preschool-aged children by means of programmes with frequent visits.24
The prevention of obesity is a key aspect of health promotion, so it is essential that uniform, consensus-based diagnostic criteria be applied to facilitate regional, international and temporal comparisons of childhood overweight rates.25
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
Partial results of this study were presented as an oral communication at the LXIV Congreso de la Sociedad de Pediatría de Galicia 2013 and the LXV Congreso de la Sociedad de Pediatría de Galicia 2014. The study was awarded the third prize for Best Oral Communication on Paediatric Medicine at the LXIV Congreso de la Sociedad de Pediatría de Galicia (SOPEGA), held on October 25 and 26, 2013 in Vigo, Spain.
ABBREVIATIONS: FO: Fundación Orbegozo • 95% CI: 95% confidence interval • BMI: body mass index • IOTF: International Obesity Task Force • WHO: World Health Organization • SERGAS: Servicio Galego de Saúde.
ACKNOWLEDGMENTS
We want to thank the nursing staff of the health care centres in which the study was conducted for their contribution in the performance of the health checkups established by the Well Child Programme (Programa do Neno San).
REFERENCES
- Estrategia Mundial sobre Régimen Alimentario, Actividad Física y Salud. Ginebra: OMS; 2004.
- Agencia Española de Seguridad Alimentaria. Estrategia NAOS. Estrategia para la nutrición, actividad física y prevención de la obesidad. Madrid: Ministerio de Sanidad y Consumo; 2005.
- Childhood overweight and obesity, 2011. In: Organización Mundial de la Salud [online] [consulted on 16/11/2015]. Available inwho.int/dietphysicalactivity/childhood/en/
- WHO-led Commission on Ending Childhood Obesity meets o develop global responses to obesity epidemic. Second meeting of the Commission on Ending Childhood Obesity (ECHO), 13-14 January 2015. In: Organización Mundial de la Salud [online] [consulted on 16/11/2015]. Available in who.int/end-chidhood-obesity/news/echo-second-meeting/en/
- Moreno LA, Rodríguez G. Dietary risk factors for development of childhood obesity. Curr Opin Clin Nutr Metab Care. 2007;10:336-41.
- Kelly AS, Barlow SE, Rao G. Severe obesity in children and adolescents: identification, associated health risks, and treatment approaches. 2013;128:1689-712.
- Wang LY, Chyen D, Lee S, Lowry R. The association between body mass index in adolescence and obesity in adulthood. J Adolesc Health. 2008;42:512-8.
- Actividades preventivas en Pediatría. Guía de apoio para o programa do Neno San. División de Asistencia Sanitaria. Consellería de Sanidade (SERGAS). Xunta de Galicia; 2004.
- Sobradillo B, Aguirre A, Aresti U, Bilbao A, Fernández-Ramos C, Lizárraga A, et al. Curvas y tablas de crecimiento. Estudios longitudinal y transversal. Fundación Orbegozo. In: Patrones de crecimiento y desarrollo en España. Atlas de gráficas y tablas. Madrid: Ergón; 2004. pp. 1465-68.
- Aranceta Bartrina J, Serra Majem L, Foz Sala M, Moreno Esteban B. Prevalencia de obesidad en España. Med Clin (Barc). 2005;125:460-6.
- Bueno M, Grupo PAIDOS 84. Estudio epidemiológico sobre nutrición y obesidad infantil. Proyecto universitario. Madrid: DANONE; 1985.
- Serra Majem L, Ribas Barba L, Aranceta Bartrina J. Obesidad infantil y juvenil en España. Resultados del Estudio enKid (1988-2000). Med Clin (Barc). 2003;121:725-32.
- Valdés Pizarro J, Royo-Bordonada MA. Prevalence of childhood obesity in Spain: National Health Survery 2006-2007. Nutr Hosp. 2012;27:154-60.
- Henríquez P, Doreste J, Laínez P, Estévez MD, Iglesias M. Prevalencia de obesidad y sobrepeso en adolescentes canarios. Relación con el desayuno y la actividad física. Med Clin (Barc). 2008;130:606-10.
- Durá Trave T, Hualde Olascoaga J, Garralda Torres I. Exceso de peso corporal infantil en Navarra y su relación con la adolescencia. Med Clin (Barc). 2012;138:52-6.
- Posso M, Brugulat Guiteras P, Puig T, Mompart Penina A. Prevalencia y condicionantes de la obesidad en la población infantojuvenil de Cataluña, 2006-2012. Med Clin (Barc). 2014;143:475-83.
- Sánchez Cruz J, Jiménez Moleón J, Fernández Quesada M, Sánchez M. Prevalencia de obesidad infantil y juvenil en España en 2012. Rev Esp Cardiol. 2013;66:371-6.
- Estudio Aladino 2013. Estudio de Vigilancia del Crecimiento, Alimentación, Actividad Física, Desarrollo Infantil y Obesidad 2013. Agencia Española de Consumo, Seguridad Alimentaria y Nutrición. Madrid: Ministerio de Sanidad, Servicios Sociales e Igualdad; 2014.
- Park MH, Falconer C, Viner RM, Kinra S. The impact of childhood obesity on morbidity and mortality in adulthood: a systematic review. Obes Rev. 2012;13:985-1000.
- Sánchez M. Aspectos epidemiológicos de la obesidad infantil. Rev Pediatr Aten Primaria. Supl. 2012;(21):9-14.
- Fundación Faustino Orbegozo Eizaguirre-Instituto de Investigación sobre Crecimiento y Desarrollo [online] [consulted on 16/11/2015]. Available in http://www.aepap.org/pdf/f_orbegozo_04.pdf
- Cole TJ, Bellizzi MC, Flegal KM, Diez WH. Body mass index cut offs to define thinness in children and adolescents: international survey. 2007;335:194-7.
- Child growth standards: methods and development. In: Organización Mundial de la Salud [online] [consulted on 16/11/2015]. Available inwho.int/childgrowth/standards/technical_report/en/
- Barroso Espadero D. ¿Cuál es la mejor evidencia disponible para recomendar el tratamiento de la obesidad en niños por debajo de los cinco años de edad? Evid Pediatr. 2009;5:74.
- Martínez Álvarez JR, Villarino Marín A, García Alcón RM, Calle Purón ME, Marrodán Serrano MD. Obesidad infantil en España: hasta qué punto es un problema de salud pública o sobre la fiabilidad de las encuestas. Nutr Clín Diet Hosp. 2013;33:80-8.